
Rod Angulation Relationship with Thoracic Kyphosis after Adolescent Idiopathic Scoliosis Posterior Instrumentation
 , , , , , , , , and
on behalf of the European Spine Study Group
, , , , , , , , and
on behalf of the European Spine Study Group
Abstract
:1. Introduction
2. Material and Methods
2.1. Design
2.2. Surgery Technique
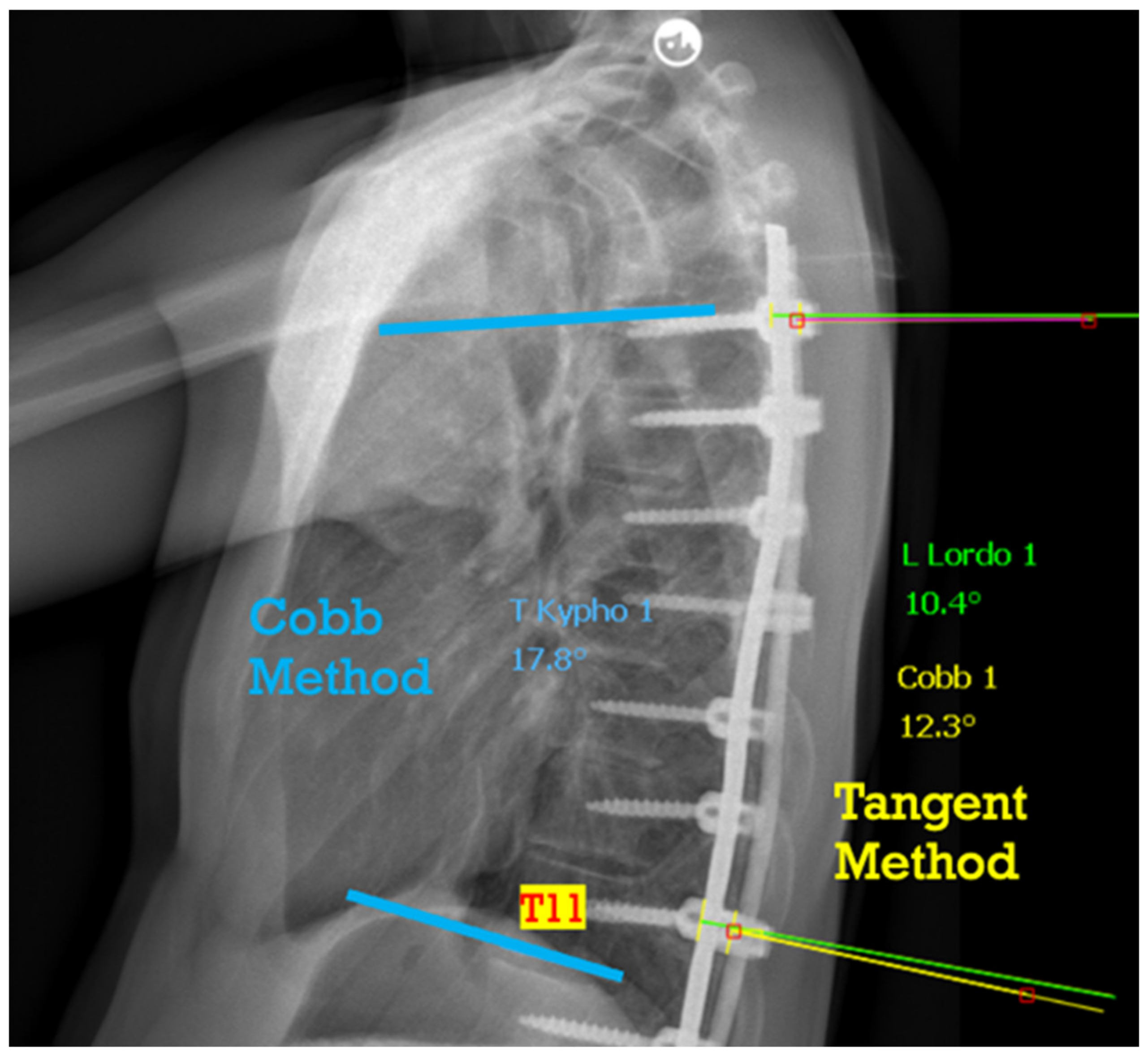
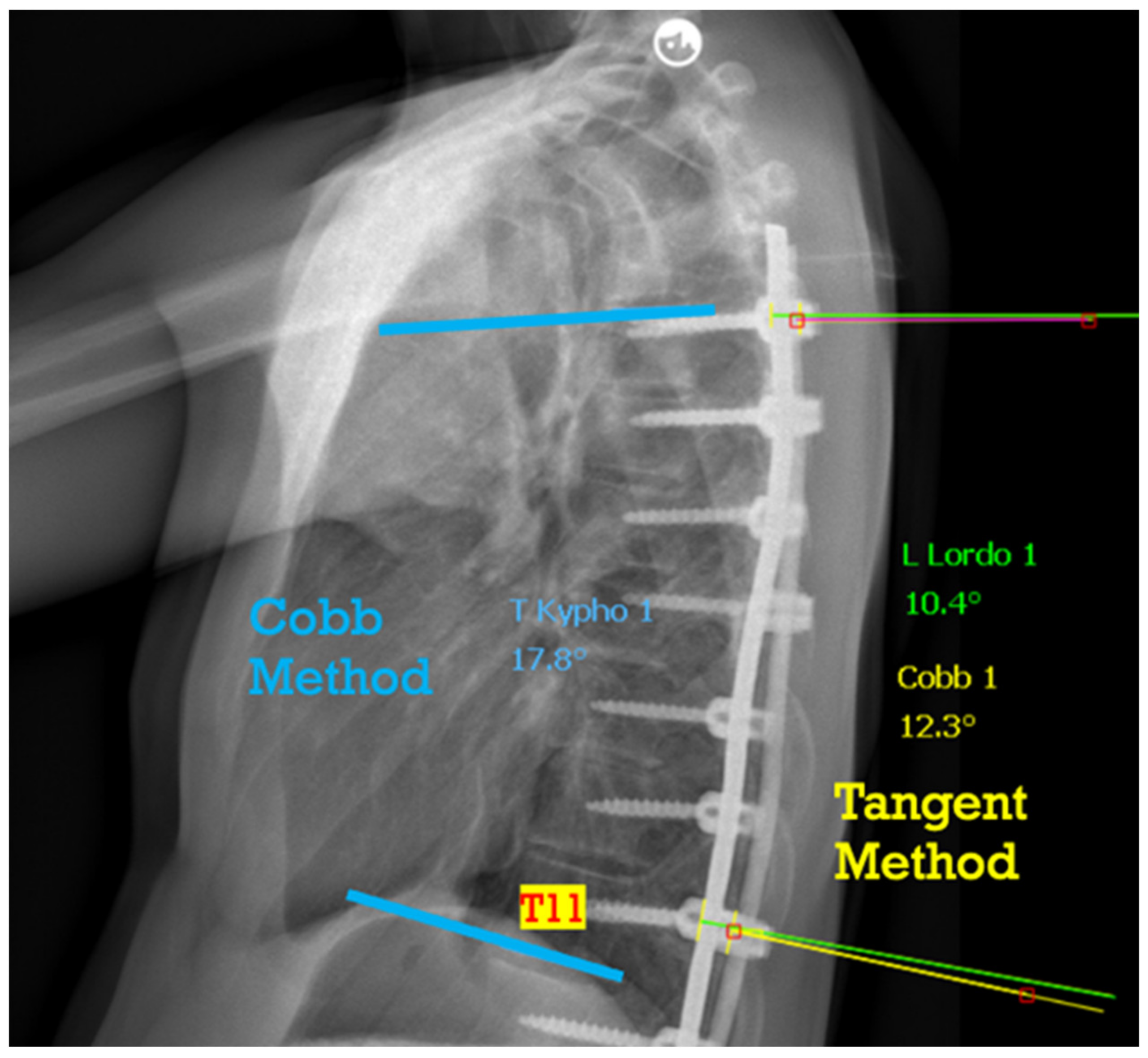
2.3. Data Collection and Radiographic Measurement
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, Z.; Rong, L. Comparison of combined anterior–posterior approach versus posterior-only approach in treating adolescent idiopathic scoliosis: A meta-analysis. Eur. Spine J. 2016, 25, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Berlin, C.; Tielemann, S.; Quante, M.; Halm, H. Correlation of radiographic parameters and patient satisfaction in adolescent idiopathic scoliosis treated with posterior screw-dual-rod instrumentation. Eur. Spine J. 2023, 32, 3140–3148. [Google Scholar] [CrossRef] [PubMed]
- King, H.A.; Moe, J.H.; Bradford, D.S.; Winter, R.B. The selection of fusion levels in thoracic idiopathic scoliosis. J. Bone Jt. Surg. Am. 1983, 65, 1302–1313. [Google Scholar] [CrossRef]
- Bao, H.; Shu, S.; Yan, P.; Liu, S.; Liu, Z.; Zhu, Z.; Qian, B.; Qiu, Y. Fifteen Years and 2530 Patients: The Evolution of Instrumentation, Surgical Strategies, and Outcomes in Adolescent Idiopathic Scoliosis in a Single Institution. World Neurosurg. 2018, 120, e24–e32. [Google Scholar] [CrossRef] [PubMed]
- Pesenti, S.; Clément, J.-L.; Ilharreborde, B.; Morin, C.; Charles, Y.P.; Parent, H.F.; Violas, P.; Szadkowski, M.; Boissière, L.; Jouve, J.-L.; et al. Comparison of four correction techniques for posterior spinal fusion in adolescent idiopathic scoliosis. Eur. Spine J. 2022, 31, 1028–1035. [Google Scholar] [CrossRef] [PubMed]
- Pesenti, S.; Charles, Y.P.; Prost, S.; Solla, F.; Blondel, B.; Ilharreborde, B.; on behalf of the French Spine Surgery Society (SFCR). Spinal Sagittal Alignment Changes during Childhood: Results of a National Cohort Analysis of 1,059 Healthy Children. J. Bone Jt. Surg. 2023, 105, 676–686. [Google Scholar] [CrossRef] [PubMed]
- Clément, J.-L.; Geoffray, A.; Yagoubi, F.; Chau, E.; Solla, F.; Oborocianu, I.; Rampal, V. Relationship between thoracic hypokyphosis, lumbar lordosis and sagittal pelvic parameters in adolescent idiopathic scoliosis. Eur. Spine J. 2013, 22, 2414–2420. [Google Scholar] [CrossRef]
- Thomas, E.S.; Boyer, N.; Meyers, A.; Aziz, H.; Aminian, A. Restoration of thoracic kyphosis in adolescent idiopathic scoliosis with patient-specific rods: Did the preoperative plan match postoperative sagittal alignment? Eur. Spine J. 2023, 32, 190–201. [Google Scholar] [CrossRef]
- Schlager, B.; Großkinsky, M.; Ruf, M.; Wiedenhöfer, B.; Akbar, M.; Wilke, H.-J. Range of surgical strategies for individual adolescent idiopathic scoliosis cases: Evaluation of a multi-centre survey. Spine Deform. 2023. Ahead of print. [Google Scholar] [CrossRef]
- Aubin, C.-E.; Labelle, H.; Ciolofan, O.C. Variability of spinal instrumentation configurations in adolescent idiopathic scoliosis. Eur. Spine J. 2007, 16, 57–64. [Google Scholar] [CrossRef]
- Solla, F.; Barrey, C.Y.; Burger, E.; Kleck, C.J.; Fière, V. Patient-specific Rods for Surgical Correction of Sagittal Imbalance in Adults: Technical Aspects and Preliminary Results. Clin. Spine Surg. Spine Publ. 2019, 32, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Moufid, A.Y.; Cloche, T.; Ghailane, S.; Ounajim, A.; Vendeuvre, T.; Gille, O. Mismatch between rod bending and actual post-operative lordosis in lumbar arthrodesis with poly axial screws. Orthop. Traumatol. Surg. Res. 2019, 105, 1143–1148. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.; Wang, G.; Jin, Z.; Wu, T.; Wang, H.; Sun, J.; Nicolas, Y.S.M.; Rupesh, K.C.; Yang, K.; Liu, J. Use of the sagittal Cobb* angle to guide the rod bending in the treatment of thoracolumbar fractures: A retrospective clinical study. J. Orthop. Surg. Res. 2020, 15, 574. [Google Scholar] [CrossRef] [PubMed]
- Boissiere, L.; Guevara-villazón, F.; Bourghli, A.; Abdallah, R.; Pellise, F.; Pizones, J.; Alanay, A.; Kleinstueck, F.; Larrieu, D.; Obeid, I. Rod angulation does not reflect sagittal curvature in adult spinal deformity surgery: Comparison of lumbar lordosis and rod contouring. Eur. Spine J. 2023, 32, 3666–3672. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Boyer, L.; Le Naveaux, F.; Schwend, R.M.; Aubin, C.-E. How does differential rod contouring contribute to 3-dimensional correction and affect the bone-screw forces in adolescent idiopathic scoliosis instrumentation? Clin. Biomech. 2016, 39, 115–121. [Google Scholar] [CrossRef]
- Solla, F.; Barrey, C.Y.; Rampal, V.; Fière, V. Comments to “Utility of Patient-Specific Rod Instrumentation in Deformity Correction: Single Institution Experience” by Sadrameli et al. Spine Surg. Relat. Res. 2021, 5, 450–451. [Google Scholar] [CrossRef]
- Le Navéaux, F.; Aubin, C.-E.; Parent, S.; Newton, P.O.; Labelle, H. 3D rod shape changes in adolescent idiopathic scoliosis instrumentation: How much does it impact correction? Eur. Spine J. 2017, 26, 1676–1683. [Google Scholar] [CrossRef]
- Sabah, Y.; Clément, J.-L.; Solla, F.; Rosello, O.; Rampal, V. Cobalt-chrome and titanium alloy rods provide similar coronal and sagittal correction in adolescent idiopathic scoliosis. Orthop. Traumatol. Surg. Res. 2018, 104, 1073–1077. [Google Scholar] [CrossRef]
- Pasha, S.; Shah, S.; Newton, P. Machine Learning Predicts the 3D Outcomes of Adolescent Idiopathic Scoliosis Surgery Using Patient–Surgeon Specific Parameters. Spine 2021, 46, 579–587. [Google Scholar] [CrossRef]
- Terai, H.; Toyoda, H.; Suzuki, A.; Dozono, S.; Yasuda, H.; Tamai, K.; Nakamura, H. A new corrective technique for adolescent idiopathic scoliosis: Convex manipulation using 6.35 mm diameter pure titanium rod followed by concave fixation using 6.35 mm diameter titanium alloy. Scoliosis 2015, 10, S14. [Google Scholar] [CrossRef]
- McAlister, W.H.; Shackelford, G.D. Measurement of spinal curvatures. Radiol. Clin. N. Am. 1975, 13, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Burke, C.A.; Speirs, J.N.; Nelson, S.C. Maximizing mechanical advantage: Surgical technique increases stiffness in spinal instrumentation. Spine Deform. 2022, 10, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Clement, J.-L.; Chau, E.; Kimkpe, C.; Vallade, M.-J. Restoration of Thoracic Kyphosis by Posterior Instrumentation in Adolescent Idiopathic Scoliosis: Comparative Radiographic Analysis of Two Methods of Reduction. Spine 2008, 33, 1579–1587. [Google Scholar] [CrossRef] [PubMed]
- Lenke, L.G.; Betz, R.R.; Harms, J.; Bridwell, K.H.; Clements, D.H.; Lowe, T.G.; Blanke, K. Adolescent idiopathic scoliosis: A new classification to determine extent of spinal arthrodesis. J. Bone Jt. Surg. Am. 2001, 83, 1169–1181. [Google Scholar] [CrossRef]
- Pesenti, S.; Lafage, R.; Henry, B.; Kim, H.J.; Bolzinger, M.; Elysée, J.; Cunningham, M.; Choufani, E.; Lafage, V.; Blanco, J.; et al. Deformity correction in thoracic adolescent idiopathic scoliosis: A comparison of posteromedial translation using sublaminar bands and cantilever with pedicle screws. Bone Jt. J. 2020, 102-B, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Kluck, D.; Newton, P.O.; Sullivan, T.B.; Yaszay, B.; Jeffords, M.; Bastrom, T.P.; Bartley, C.E. A 3D Parameter Can Guide Concave Rod Contour for the Correction of Hypokyphosis in Adolescent Idiopathic Scoliosis. Spine 2020, 45, E1264–E1271. [Google Scholar] [CrossRef] [PubMed]
- Wan, S.H.-T.; Wong, D.L.-L.; To, S.C.-H.; Meng, N.; Zhang, T.; Cheung, J.P.-Y. Patient and surgical predictors of 3D correction in posterior spinal fusion: A systematic review. Eur. Spine J. 2023, 32, 1927–1946. [Google Scholar] [CrossRef]
- Ilharreborde, B.; Simon, A.L.; Ferrero, E.; Mazda, K. How to Optimize Axial Correction without Altering Thoracic Sagittal Alignment in Hybrid Constructs with Sublaminar Bands: Description of the “Frame” Technique. Spine Deform. 2019, 7, 245–253. [Google Scholar] [CrossRef]
- Stagnara, P.; Claude De Mauroy, J.; Dran, G.; Gonon, G.P.; Costanzo, G.; Dimnet, J.; Pasquet, A. Reciprocal Angulation of Vertebral Bodies in a Sagittal Plane: Approach to References for the Evaluation of Kyphosis and Lordosis. Spine 1982, 7, 335–342. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean (Standard Deviation) | Cases |
|---|---|---|
| Gender | 86 F, 13 M | |
| Age | 14 (1.6) | |
| Posterior Instrumented Levels | 11 (2.6) | |
| Number of Implants | 17 (5.1) | |
| Posterior Column Osteotomy | 15 (14.1%) | |
| Preoperative Major Cobb Angle | 62.6° (12.8) | |
| Postoperative Major Cobb Angle | 26.6° (9.4) | |
| Preoperative T5–T11 Kyphosis | 25.1° (16.4) | |
| Postoperative T5–T11 Kyphosis | 23.7° (8.6) | |
| Mean Rod Curvature (T5–T11) | 20.9° (8.9) | |
| Preoperative Lumbar Lordosis | 59.4° (23.1) | |
| Postoperative Lumbar Lordosis | 58.3° (10.4) | |
| T5–T11 ΔK | 2.7° (6) | |
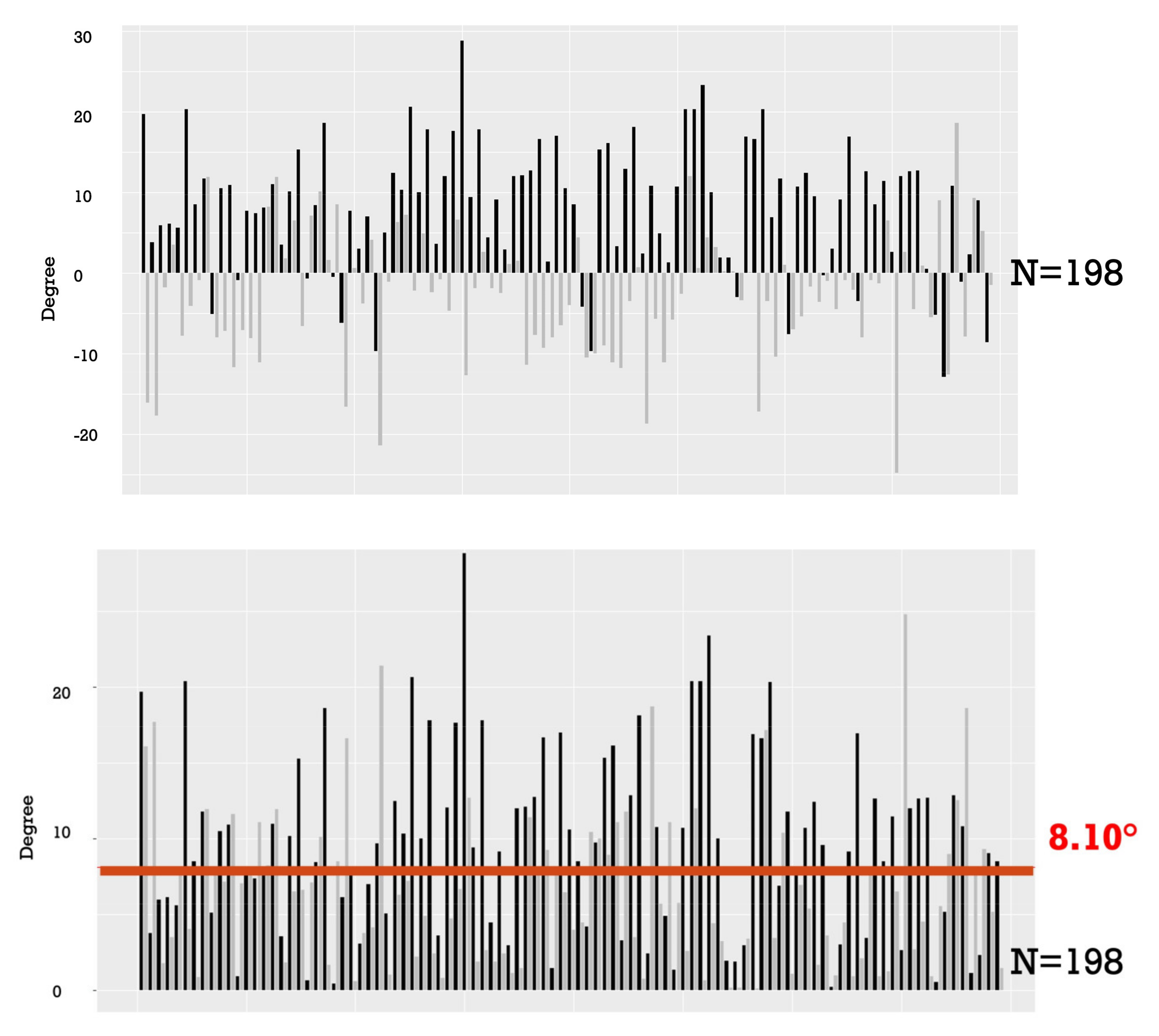
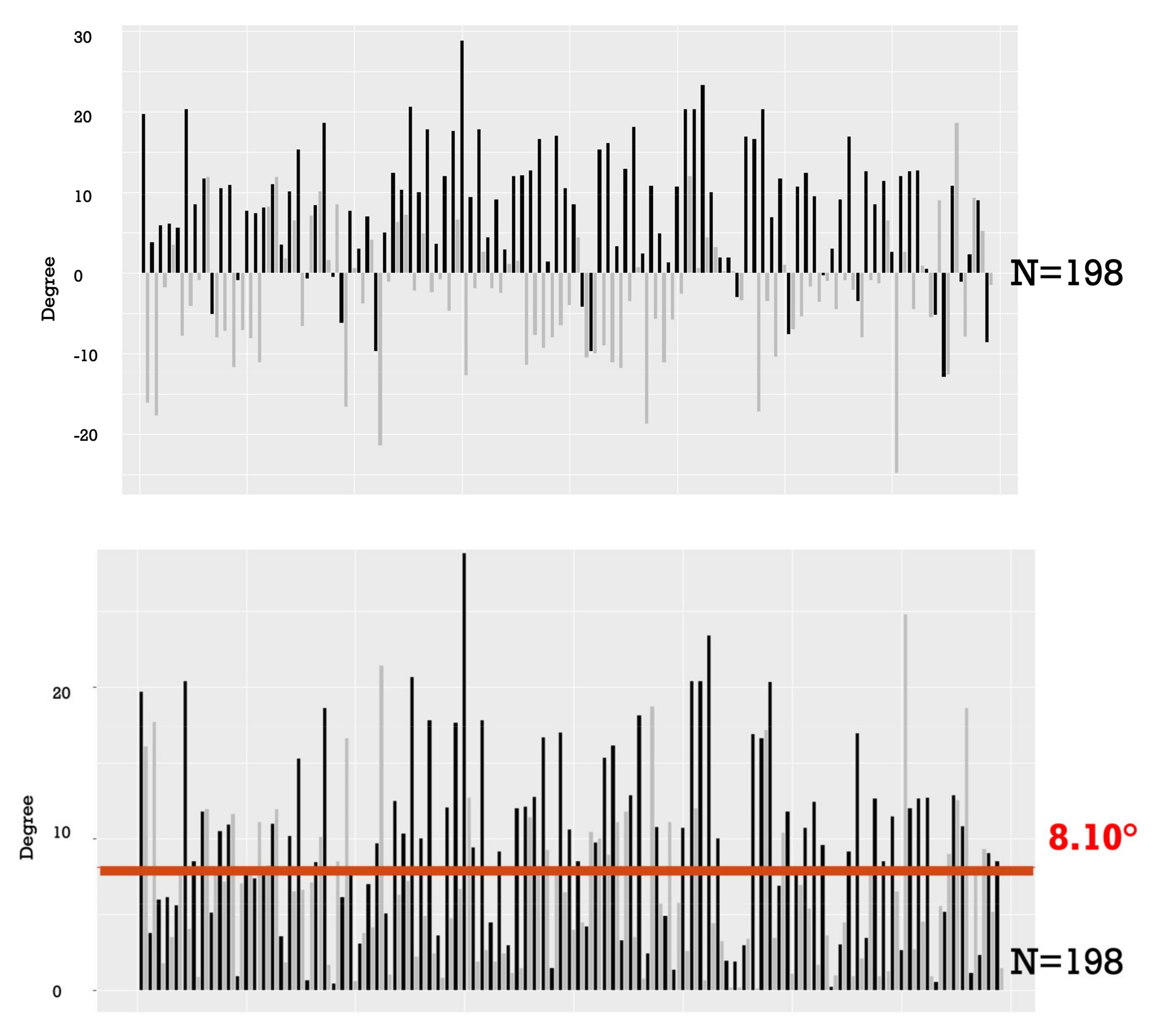
| Mean Absolute T5–T11 ΔK | 5.5° (3.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boissiere, L.; Bourghli, A.; Guevara-Villazon, F.; Pellisé, F.; Alanay, A.; Kleinstück, F.; Pizones, J.; Roscop, C.; Larrieu, D.; Obeid, I., on behalf of the European Spine Study Group. Rod Angulation Relationship with Thoracic Kyphosis after Adolescent Idiopathic Scoliosis Posterior Instrumentation. Children 2024, 11, 29. https://doi.org/10.3390/children11010029
Boissiere L, Bourghli A, Guevara-Villazon F, Pellisé F, Alanay A, Kleinstück F, Pizones J, Roscop C, Larrieu D, Obeid I on behalf of the European Spine Study Group. Rod Angulation Relationship with Thoracic Kyphosis after Adolescent Idiopathic Scoliosis Posterior Instrumentation. Children. 2024; 11(1):29. https://doi.org/10.3390/children11010029
Chicago/Turabian StyleBoissiere, Louis, Anouar Bourghli, Fernando Guevara-Villazon, Ferran Pellisé, Ahmet Alanay, Frank Kleinstück, Javier Pizones, Cécile Roscop, Daniel Larrieu, and Ibrahim Obeid on behalf of the European Spine Study Group. 2024. "Rod Angulation Relationship with Thoracic Kyphosis after Adolescent Idiopathic Scoliosis Posterior Instrumentation" Children 11, no. 1: 29. https://doi.org/10.3390/children11010029
APA StyleBoissiere, L., Bourghli, A., Guevara-Villazon, F., Pellisé, F., Alanay, A., Kleinstück, F., Pizones, J., Roscop, C., Larrieu, D., & Obeid, I., on behalf of the European Spine Study Group. (2024). Rod Angulation Relationship with Thoracic Kyphosis after Adolescent Idiopathic Scoliosis Posterior Instrumentation. Children, 11(1), 29. https://doi.org/10.3390/children11010029