Abstract
Background/Objectives: Micropulse laser trabeculoplasty (MLT) is gaining attention as a non-invasive treatment option for primary open-angle glaucoma (POAG), offering an alternative to traditional surgeries and medications. This systematic review evaluates the effectiveness, safety, and potential of MLT in glaucoma management. Methods: This review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The strength of evidence was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology, following the 2011 Oxford Centre for Evidence-Based Medicine (OCEBM) recommendations. Results: We identified 79 articles, and after removing duplicates and screening abstracts, 56 articles were eligible for further review. A detailed full-text analysis was conducted on 26 articles, of which 15 met the predefined inclusion criteria. Conclusions: MLT shows promise as a primary or adjunctive treatment for reducing intraocular pressure (IOP) in glaucoma and ocular hypertension patients. Current evidence supports its efficacy and safety; however, additional long-term studies are needed to confirm its durability and compare its effectiveness with traditional surgical and pharmacological approaches. Standardizing treatment protocols and refining patient selection criteria could enhance MLT’s clinical value and support its broader adoption in glaucoma care.
Keywords:
glaucoma; micropulse laser trabeculoplasty (MLT); minimally invasive glaucoma surgery; minimally invasive bleb surgery; non-plate; bleb-forming glaucoma devices; trabeculectomy; glaucoma-therapy-related ocular surface disease; glaucoma drainage devices; non-penetrating glaucoma surgery; ciliary body function modulation; selective laser trabeculoplasty 1. Introduction
Glaucoma is a leading cause of irreversible blindness worldwide, characterized by progressive optic nerve damage and visual field loss [1]. Elevated intraocular pressure (IOP) is a major modifiable risk factor in glaucoma pathogenesis. While pharmacotherapy remains the cornerstone of glaucoma management, surgical interventions such as trabeculectomy and minimally invasive glaucoma surgeries (MIGSs) are often pursued in cases of inadequate IOP control or intolerance to medications.
Micropulse laser trabeculoplasty (MLT) has emerged as a non-invasive, repeatable treatment option for reducing IOP by enhancing aqueous outflow through the trabecular meshwork. Unlike traditional continuous-wave lasers, MLT delivers energy in short, repetitive pulses interspersed with cooling intervals. This approach minimizes thermal damage to the trabecular meshwork while promoting aqueous humor outflow.
The mechanisms of MLT involve several principles. First, MLT stimulates trabecular meshwork endothelial cells, enhancing aqueous humor outflow [2]. Second, the cooling intervals between pulses reduce collateral thermal damage to adjacent tissues [3]. Third, MLT induces biological modulation, including cytokine release and extracellular matrix remodeling, which contributes to sustained IOP reduction [4].
Selective laser trabeculoplasty (SLT) is another established laser treatment for IOP control. It employs a Q-switched frequency-doubled 532 nm Nd:YAG laser that targets pigmented trabecular cells with short bursts of energy [5]. In contrast, MLT uses a 532 nm green, a 577 nm yellow, or an 810 nm diode laser in a micropulse delivery mode. The cooling intervals in MLT minimize thermal damage, reducing inflammation and the risk of complications. Conversely, SLT produces microthermal effects at the cellular level, which can result in pigment dispersion and mild inflammation within trabecular meshwork cells, occasionally leading to intraocular pressure spikes [6,7,8].
This systematic review aims to consolidate the current evidence regarding the efficacy, safety, and future directions of MLT in glaucoma management.
2. Materials and Methods
A systematic search of the literature was conducted across PubMed, Embase, Scopus, and Cochrane Library databases to identify studies published up to 15 February 2024. The search strategy incorporated keywords such as “micropulse laser trabeculoplasty”, “MLT”, “glaucoma”, “intraocular pressure”, and “ocular hypertension”. Eligible study types included randomized controlled trials (RCTs), prospective cohort studies, retrospective analyses, and systematic reviews.
Studies were selected based on predefined eligibility criteria, focusing on interventions involving MLT for glaucoma treatment, outcomes related to intraocular pressure (IOP) reduction, safety profiles, and follow-up duration. Inclusion criteria required studies to link the micropulse laser trabeculoplasty (MLT) technique with IOP reduction in primary open-angle glaucoma (POAG). Studies reporting outcomes unrelated to IOP reduction with MLT, as well as review articles, pilot studies, case series, case reports, photo essays, and studies written in languages other than English, were excluded. Additionally, studies involving animal eyes, cadaveric eyes, and pediatric patients were excluded.
Data extraction and synthesis were independently performed by two reviewers (T.V. and F.S.), with discrepancies resolved through the consensus of a third senior consultant (F.C.). The search was limited to studies published in English but was not restricted by publication type, study design, or publication date. The complete search strategy is provided in Appendix A.
The strength of the evidence was evaluated using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach, following the 2011 Oxford Centre for Evidence-Based Medicine (OCEBM) recommendations (Table 1).

Table 1.
Characteristics, quality, and level of evidence of the included studies.
3. Results
A total of 79 articles were identified. Following the removal of duplicates and screening of abstracts, 56 articles remained. Subsequently, a comprehensive full-text review of 26 articles was conducted. Ultimately, 15 articles met the predefined inclusion criteria (Appendix B). All the studies evaluated the efficacy of MLT in primary open-angle glaucoma (POAG), pseudoexfoliative glaucoma (PXG), and ocular hypertension (OHT). Across various study designs, MLT consistently demonstrated a significant reduction in IOP. Adverse events associated with MLT were generally mild and transient, including intraocular inflammation, transient IOP spikes, and corneal epithelial defects. Long-term follow-up data on the durability of IOP reduction post-MLT are limited but suggest sustained efficacy over months to years. Figure 1 summarizes the research approach applied in this systematic review within a flowchart.
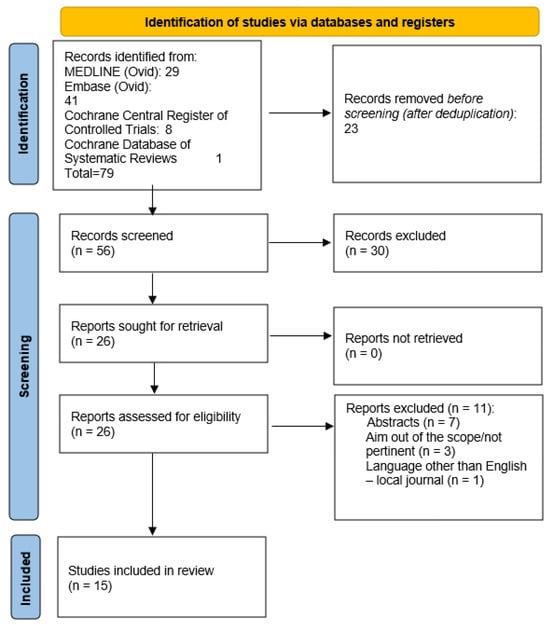
Figure 1.
Flowchart of the literature search and selection according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA).
The specific papers with determining reasons for inclusion or exclusion of the full-text reviewed articles are reported in Appendix B.
4. Discussion
Laser trabeculoplasty techniques have long been recognized as safe, non-invasive, and repeatable methods for reducing intraocular pressure (IOP) in glaucoma patients. Micropulse laser trabeculoplasty (MLT), introduced in 2005, employs a 15% duty cycle targeting the anterior trabecular meshwork. This technique minimizes thermal tissue damage, postoperative inflammation, and peripheral anterior synechiae (PAS) formation compared to conventional laser trabeculoplasty (CLT) [21].
Several studies have assessed the efficacy and safety of MLT. In 2015, Lee et al. conducted a prospective cohort study on 48 eyes with primary open-angle glaucoma (POAG), including normal tension glaucoma (IOP < 21 mm Hg). A single session of 360° MLT significantly reduced IOP at all follow-up intervals up to six months and decreased glaucoma medication use. At the six-month follow-up, 20% of patients achieved IOP lowering and 21% reduced their medication use. No significant side effects were observed [16].
In a retrospective review by Valera-Cornejo et al., in 2018, 30 eyes treated with 360° MLT showed a ≥ 20% IOP reduction in 35% and 41% of cases at three and six months, respectively. A trend toward greater IOP reduction with higher baseline IOP was observed, although this was not statistically significant due to the small sample size [13].
In 2019, Hong et al. evaluated the outcomes of MLT in 72 eyes, reporting a 20% IOP decrease from baseline across a 24-week follow-up. The study also found reduced medication use and no significant inflammation [10]. Another study by Phan et al. in 2019 stratified outcomes based on baseline IOP and glaucoma severity. Patients with higher initial IOP and early-stage glaucoma experienced significant IOP reductions, while those with advanced glaucoma did not [18].
Yang et al., in 2022, documented sustained IOP reductions at one day, three months, and six months post-treatment in 39 eyes. However, at 36 months, only 21.88% of patients achieved a ≥ 20% reduction, indicating MLT’s diminishing efficacy over time [20].
The role of operator expertise has also been highlighted. In a study by Kakihara et al., MLT efficacy was greater when performed by experienced glaucoma specialists. This underscores the need for further investigation into the impact of operator expertise on treatment outcomes [11].
MLT has also been evaluated in pseudoexfoliation glaucoma (PEXG). In 2019, Makri et al. treated 27 PEXG eyes with inadequate IOP control using prostaglandin analogs, reporting significant IOP reductions up to 12 months, with 52.17% of cases achieving a ≥20% reduction [17]. Similarly, Aydin Kurna et al. assessed 180° MLT in 51 eyes with uncontrolled POAG or PEXG, achieving IOP reduction in 34–42% of cases during follow-ups of up to 48 months. A significant correlation was observed between baseline IOP and treatment success, while age and laser power showed no correlation [14].
Comparisons between MLT and selective laser trabeculoplasty (SLT) reveal distinct advantages and limitations. Hirabayashi et al. reported similar success rates for MLT (44%) and SLT (40%) in a cohort of 100 eyes. MLT showed consistent efficacy regardless of age or baseline IOP and did not induce IOP spikes, unlike SLT [9,22]. Pimentel et al. found SLT to be slightly more effective at 12 months in achieving an IOP ≤ 21 mm Hg with ≥20% reduction, although MLT demonstrated comparable overall efficacy [6]. Sun et al. observed greater IOP reductions with SLT at early follow-ups, but similar long-term outcomes between the two techniques [19]. Table 2 summarizes the differences between MLT and SLT in POAG treatment.
Table 2.
Advantages of MLT in comparison to SLT.
Studies suggest that MLT may cause less inflammation and fewer IOP spikes post-treatment compared to SLT, making it a safer option for some patients [5,8].
In conclusion, MLT presents a promising, less invasive alternative to traditional methods for managing glaucoma and ocular hypertension, particularly in patients at risk of post-treatment complications. However, further research is needed to optimize treatment protocols, assess long-term efficacy, and clarify inter-operator variability.
Although there is now sufficient evidence to consider MLT a safe and effective treatment for glaucoma patients, several areas remain worthy of further investigation. These include determining optimal treatment parameters such as laser energy settings, the number of laser applications, and retreatment intervals. Additionally, many studies conducted to date have limitations that may affect their results. These include retrospective designs that may introduce selection bias, small sample sizes, short follow-up periods, a lack of randomization, and the absence of control groups in some cases.
Patient selection criteria, including baseline IOP, glaucoma subtype, and prior treatment history, may also influence the likelihood of treatment success. Therefore, future studies should aim to include more homogeneous cohorts to enhance the reliability of findings.
Future research directions should focus on prospective, comparative studies to elucidate the mechanisms underlying MLT’s IOP-lowering effects, explore combination therapy approaches, and assess the cost-effectiveness of MLT compared to standard treatments.
5. Conclusions
MLT represents a valuable adjunctive or primary treatment option for lowering IOP in patients with glaucoma or ocular hypertension. While existing evidence supports its efficacy and safety profile, further long-term studies are warranted to establish its durability and comparative effectiveness relative to traditional surgical and pharmacological interventions. The standardization of treatment protocols and refinement of patient selection criteria may enhance the clinical utility of MLT and pave the way for its widespread adoption in glaucoma management.
One key area of future research is the identification of patient profiles most likely to benefit from MLT. While current evidence supports its use across various glaucoma subtypes, differences in individual responses suggest that factors such as baseline intraocular pressure, angle anatomy, and disease progression rates may influence outcomes. Longitudinal studies with diverse patient populations are needed to develop predictive models for tailoring MLT to individual needs.
Another promising avenue for investigation is the integration of MLT with pharmacological and surgical interventions. Understanding the synergistic effects of MLT with medications such as prostaglandin analogues or its role as a bridge therapy before more invasive procedures could optimize treatment algorithms. Randomized controlled trials should evaluate the efficacy and safety of such combination approaches, particularly in patients with advanced or refractory glaucoma.
Finally, economic considerations are critical for the widespread adoption of MLT. Comprehensive cost-effectiveness analyses comparing MLT with other treatment modalities, including traditional laser trabeculoplasty and newer surgical options, are essential. These studies should consider not only direct costs but also the long-term economic impact of reduced medication use and delayed progression to invasive surgeries.
Author Contributions
Conceptualization, F.C. and T.V.; methodology, F.C., B.C., A.P., F.S., R.P., L.D., G.P. and T.V.; software, F.C., B.C., A.P., F.S., R.P., L.D., G.P. and T.V.; validation, F.C. and T.V.; formal analysis, F.C., B.C., A.P., F.S., R.P., L.D., G.P. and T.V.; investigation, F.C., B.C., A.P., F.S., R.P., L.D., G.P. and T.V.; resources, F.C., G.P. and T.V.; data curation, F.C.; writing—original draft preparation, F.C., B.C., A.P., F.S., R.P., L.D., G.P. and T.V.; writing—review and editing, F.C., B.C., A.P., F.S., R.P., L.D., G.P. and T.V.; visualization, F.C., B.C., A.P., F.S., R.P., L.D., G.P. and T.V.; supervision, T.V.; project administration, F.C.; funding acquisition, F.C., B.C., A.P., F.S., R.P., L.D., G.P. and T.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study did not require ethical approval.
Data Availability Statement
All the data are available on reasonable request from the corresponding author.
Acknowledgments
Oslo University Hospital library service.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
Documentation on the literature search
Micropulse laser trabeculoplasty (MLT) was used for primary open-angle glaucoma (POAG).
The following databases were searched:
| Database | Number of Retrieved References |
| MEDLINE (Ovid) | 29 |
| Embase (Ovid) | 41 |
| Cochrane Central Register of Controlled Trials | 8 |
| Cochrane Database of Systematic Reviews | 1 |
| Number of references before deduplication | 79 |
| Number of references after deduplication | 56 |
All searches were conducted on 15 February 2024 by Sølvi Biedilæ, a senior librarian, at the Library of Medicine and Science, University of Oslo.
| Ovid Databases | |
| exp/ | Exploded index term |
| / | After an index, the term indicates that a subject heading is selected |
| .tw,kf. | This searches for a term in the title, abstract, and author keywords |
| * | This truncates the end of a term; for example, diet * retrieves both diet, diets, and dietary |
| Adj3 | This searches for two terms next to each other, in any order, with up to three words in between |
| Cochrane Library | |
| NEAR/3 | This searches for two terms next to each other, in any order, with up to three words in between |
Ovid MEDLINE(R) ALL <1946 to 14 February 2024>
| 1. | exp Glaucoma/ | 60,993 |
| 2. | glaucoma*.tw,kf. | 73,555 |
| 3. | 1 or 2 | 84,174 |
| 4. | ((micropulse* or micro pulse*) adj3 laser* adj3 trabecul*).tw,kf. | 29 |
| 5. | mlt.tw,kf. | 1444 |
| 6. | 4 or 5 | 1457 |
| 7. | 3 and 6 | 29 |
Embase Classic+Embase <1947 to 2024 February 14>
| 1. | exp Glaucoma/ | 116,701 |
| 2. | glaucoma*.tw,kf. | 99,413 |
| 3. | 1 or 2 | 130,841 |
| 4. | ((micropulse* or micro pulse*) adj3 laser* adj3 trabecul*).tw,kf. | 38 |
| 5. | mlt.tw,kf. | 1889 |
| 6. | 4 or 5 | 1904 |
| 7. | 3 and 6 | 41 |
Cochrane Library
| ID | Search | Hits |
| #1 | MeSH descriptor: [Glaucoma] explode all trees | 4180 |
| #2 | (glaucoma*) | 9377 |
| #3 | #1 or #2 | 9377 |
| #4 | ((micropulse* or micro pulse*) near/3 laser* near/3 trabecul*) | 9 |
| #5 | (mlt) | 169 |
| #6 | #4 or #5 | 173 |
| #7 | #3 and #6 in Cochrane Reviews | 1 |
| #8 | #3 and #6 in Trials | 8 |
Appendix B
Table A1.
Second round of papers inclusion with reasons behind the choices.
Table A1.
Second round of papers inclusion with reasons behind the choices.
| Paper (Total 26; 15 Included; 11 Excluded) | Included (Comment) | Excluded (Reason) |
| A comparison of efficacy between SLT and MLT is provided. | |
| MLT is effective and safe for POAG patients. No patient experienced IOP spikes after MLT. The IOP 6 mo after treatment decreased significantly with less glaucoma medication. | |
| The 6-month effectiveness of MLT for controlling IOP is relatively limited in eyes with OAG using maximal tolerable glaucoma eyedrops. However, its effectiveness may be improved if performed by a glaucoma specialist with sufficient MLT experience. | |
| Both the original article (retrospective comparative study) and review are included. | |
| The results suggest that 180° MDLT is a safe but ineffective treatment in patients with open-angle glaucoma. | |
| MLT has a significantly lower incidence of pressure spikes and a similar treatment failure rate at 1-year post-procedure, demonstrating that it is a reasonable alternative compared to SLT. | |
| MLT slightly reduces the IOP in a few patients with uncontrolled OAG for a very short time and may not be suitable for these patients. | |
| Enyr Saran Arcieri, Rafael Saran Arcieri; MICROPULSE DIODE LASER TRABECULOPLASTY RESULTS IN TREATMENT OF PRIMARY OPEN-ANGLE GLAUCOMA PATIENTS. Invest. Ophthalmol. Vis. Sci. 2014;55(13):6165. | ARVO abstract | |
| antonella clemente, Caterina Toma, Stela Vujosevic, chiara padovan, stefano de cillà; Efficacy of Micropulse Laser Trabeculoplasty in Open Angle Glaucoma. Invest. Ophthalmol. Vis. Sci. 2019;60(9):696. | ARVO abstract | |
| Peter Coombs, Nathan M Radcliffe; Outcomes of Micropulse Laser Trabeculoplasty vs. Selective Laser Trabeculoplasty. Invest. Ophthalmol. Vis. Sci. 2014;55(13):6155. | ARVO abstract | |
| Robert G Dionisio, Olga Lekakh German, Thomas Patrianakos, Michael Giovingo; MLT vs. SLT in the Hispanic and African American Population for Treatment of Open-Angle Glaucoma. Invest. Ophthalmol. Vis. Sci. 2018;59(9):6097. | ARVO abstract | |
| Briana C. Gapsis, Matthew Bickford, Robert Allan Sharpe, Sudeep Das, Leah Kammerdeiner, Matthew J. Nutaitis; Analysis of the Relative Efficacy of Micropulse Laser Trabeculoplasty and Selective Laser Trabeculoplasty. Invest. Ophthalmol. Vis. Sci. 2018;59(9):6090. | ARVO abstract; outcome is out of the scope of the review | |
| Kunjal K Modi, Scott M Walsman; Effect of Increasing Shot Number in Micropulse Laser Trabeculoplasty (MLT) for Open Angle Glaucoma. Invest. Ophthalmol. Vis. Sci. 2017;58(8):4976. | ARVO abstract; outcome is out of the scope of the review | |
| Marcelle Morcos, Jack Klenda, Patricia Fortin, Andrew Pansick, Christian Draper; Impact of Micropulse Laser Trabeculoplasty: A 2-Year Retrospective Analysis. Invest. Ophthalmol. Vis. Sci. 2022;63(7):170–A0363. | ARVO abstract | |
| D.D. Ingvoldstad, R. Krishna, L. Willoughby; MicroPulse Diode Laser Trabeculoplasty versus Argon Laser Trabeculoplasty in the Treatment of Open Angle Glaucoma. Invest. Ophthalmol. Vis. Sci. 2005;46(13):123. | ARVO abstract | |
| Micropulse trabeculoplasty has demonstrated similar efficacy to SLT over a 52-week follow-up period with less discomfort experienced both during and after the procedure. | |
| The reduction in intraocular pressure shows a significant correlation with baseline intraocular pressure, while age and laser power show no correlation (p > 0.05). MLT is a novel treatment option for patients with glaucoma with favorable long-term outcomes and a good safety profile. | |
| Micropulse diode laser trabeculoplasty is a useful adjunct in the management of open-angle glaucoma in Nigerians. This corroborates the findings of other researchers in western populations. | |
| Detry-Morel M, Muschart F, Pourjavan S. Micropulse diode laser (810 nm) versus argon laser trabeculoplasty in the treatment of open-angle glaucoma: comparative short-term safety and efficacy profile. Bull Soc Belge Ophtalmol. 2008;(308):21-8. PMID: 18700451. | Language other than English and a local journal | |
| MLT is effective in reducing IOP and medications in OAG with minimal post-laser inflammation and low failure rates at 6 months following laser trabeculoplasty. | |
| Makri OE, Pagoulatos D, Kagkelaris K, Plotas P, Georgakopoulos CD. Evaluation of intraocular pressure in the first 24hours after micropulse laser trabeculoplasty in eyes with pseudoexfoliation glaucoma. J Fr Ophtalmol. 2019 Nov;42(9):983-986. doi: 10.1016/j.jfo.2019.05.008. Epub 2019 Jun 6. PMID: 31178072. | Studies with outcomes other than IOP lower the effect of MLT | |
| Micropulse laser trabeculoplasty appears to be an effective method in lowering IOP in patients with PEXG up to 12 month of the follow-up period. | |
| Patients with a higher initial IOP and in the early stages of glaucoma are more likely to benefit from MLT in lowering IOP. A randomized clinical trial is necessary to confirm these preliminary findings. We recommend that clinicians should consider MLT in the management of early glaucoma and among those with IOP >16 mm Hg. | |
| Eyes have similar success after MLT compared to SLT at 1 year. Laser trabeculoplasty with either method can be offered as a treatment with consideration of MLT in those eyes where IOP spikes should be avoided. | |
| Catherine Q Sun, Yvonne Ou; Comparison of Outcomes of Micropulse Laser Trabeculoplasty versus Selective Laser Trabeculoplasty. Invest. Ophthalmol. Vis. Sci. 2018;59(9):6089. | ARVO abstract | |
| Micropulse laser trabeculoplasty reduce IOP in patients with glaucoma or ocular hypertension for a short period, but its lowering efficiency is limited up to 6 months of the follow-up period. |
References
- Dietze, J.; Blair, K.; Zeppieri, M.; Havens, S.J. Glaucoma. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Ma, A.; Yu, S.W.Y.; Wong, J.K.W. Micropulse Laser for the Treatment of Glaucoma: A Literature Review. Surv. Ophthalmol. 2019, 64, 486–497. [Google Scholar] [CrossRef] [PubMed]
- Micropulse Laser Therapy as an Integral Part of Eye Disease Management. Available online: https://www.mdpi.com/1648-9144/59/8/1388 (accessed on 2 January 2025).
- Chen, Y.-F.; Zeng, W. Mechanism of Selective Laser Trabeculoplasty: A Systemic Review. Int. J. Ophthalmol. 2024, 17, 963–968. [Google Scholar] [CrossRef] [PubMed]
- Abramowitz, B.; Chadha, N.; Kouchouk, A.; Alhabshan, R.; Belyea, D.A.; Lamba, T. Selective Laser Trabeculoplasty vs Micropulse Laser Trabeculoplasty in Open-Angle Glaucoma. Clin. Ophthalmol. 2018, 12, 1599–1604. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, R.L.; Alves Júnior, R.R.; Lima, W.M.M.L.; Dantas, L.O.R.; Costa, V.P. Selective Laser Trabeculoplasty versus Micropulse Laser Trabeculoplasty for Intraocular Pressure Control in Patients with Primary Open Angle Glaucoma: A 12-Month Retrospective Comparative Study. Lasers Med. Sci. 2023, 38, 102. [Google Scholar] [CrossRef] [PubMed]
- Barkana, Y.; Belkin, M. Selective Laser Trabeculoplasty. Surv. Ophthalmol. 2007, 52, 634–654. [Google Scholar] [CrossRef] [PubMed]
- Robin, A.Z.; Syar, P.; Darwish, D.; Thomas, C.; Pfahler, N.M.; Kakouri, A.; Patrianakos, T.; Giovingo, M. Comparison of Success Rate and Intraocular Pressure Spikes between Selective Laser Trabeculoplasty and Micropulse Laser Trabeculoplasty in African American and Hispanic Patients. Int. J. Ophthalmol. 2023, 16, 75–80. [Google Scholar] [CrossRef]
- Hirabayashi, M.T.; Rosenlof, T.L.; An, J.A. Comparison of Successful Outcome Predictors for MicroPulse® Laser Trabeculoplasty and Selective Laser Trabeculoplasty at 6 Months. Clin. Ophthalmol. 2019, 13, 1001–1009. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.; Song, S.J.; Liu, B.; Hassanpour, K.; Zhang, C.; Loewen, N. Efficacy and Safety of Micropulse Laser Trabeculoplasty for Primary Open Angle Glaucoma. Int. J. Ophthalmol. 2019, 12, 784. [Google Scholar] [CrossRef] [PubMed]
- Kakihara, S.; Hirano, T.; Imai, A.; Kurenuma, T.; Chiku, Y.; Murata, T. Micropulse Laser Trabeculoplasty under Maximal Tolerable Glaucoma Eyedrops: Treatment Effectiveness and Impact of Surgical Expertise. Int. J. Ophthalmol. 2021, 14, 388–392. [Google Scholar] [CrossRef]
- Rantala, E.; Välimäki, J. Micropulse Diode Laser Trabeculoplasty—180-degree Treatment. Acta Ophthalmol. 2012, 90, 441–444. [Google Scholar] [CrossRef] [PubMed]
- Valera-Cornejo, D.; Loayza-Gamboa, W.; Herrera-Quiroz, J.; Alvarado-Vlllacorta, R.; Cordova-Crisanto, L.; Valderrama-Albino, V.; Davalos, N. Micropulse Trabeculoplasty in Open Angle Glaucoma. Adv. Biomed. Res. 2018, 7, 156. [Google Scholar] [CrossRef] [PubMed]
- Aydin Kurna, S.; Sonmez, A.D.; Yamic, M.; Altun, A. Long-Term Results of Micropulse Laser Trabeculoplasty with 577-Nm Yellow Wavelength in Patients with Uncontrolled Primary Open-Angle Glaucoma and Pseudoexfoliation Glaucoma. Lasers Med. Sci. 2022, 37, 2745–2752. [Google Scholar] [CrossRef] [PubMed]
- Babalola, O.E. Micropulse Diode Laser Trabeculoplasty in Nigerian Patients. Clin. Ophthalmol. 2015, 9, 1347–1351. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.Y.; Yau, G.S.K.; Yick, D.W.F.; Yuen, C.Y.F. MicroPulse Laser Trabeculoplasty for the Treatment of Open-Angle Glaucoma. Medicine 2015, 94, e2075. [Google Scholar] [CrossRef]
- Makri, O.E.; Pallikari, A.; Pagoulatos, D.; Kagkelaris, K.; Kostopoulou, E.V.; Georgakopoulos, C.D. Micropulse Laser Trabeculoplasty on Pseuodexfoliation Glaucoma Patients under Topical Prostaglandin Analogue Monotherapy: 1-Year Results. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Phan, R.; Bubel, K.; Fogel, J.; Brown, A.; Perry, H.; Morcos, M. Micropulse Laser Trabeculoplasty and Reduction of Intraocular Pressure: A Preliminary Study. Saudi J. Ophthalmol. 2021, 35, 122. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.Q.; Chen, T.A.; Deiner, M.S.; Ou, Y. Clinical Outcomes of Micropulse Laser Trabeculoplasty Compared to Selective Laser Trabeculoplasty at One Year in Open-Angle Glaucoma. Clin. Ophthalmol. 2021, 15, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Huang, X.; Liao, S.; Zhang, F.; Shi, J.; Duan, X.; Liu, K. Micropulse Laser Trabeculoplasty on Chinese Patients with Glaucoma or Ocular Hypertension: Average 35 Months Follow-up Results. BMC Ophthalmol. 2022, 22, 249. [Google Scholar] [CrossRef] [PubMed]
- Kumar, H.; Mansoori, T.; Warjri, G.; Somarajan, B.; Bandil, S.; Gupta, V. Lasers in Glaucoma. Indian J. Ophthalmol. 2018, 66, 1539. [Google Scholar] [CrossRef][Green Version]
- Kramer, T.R.; Noecker, R.J. Comparison of the Morphologic Changes after Selective Laser Trabeculoplasty and Argon Laser Trabeculoplasty in Human Eye Bank Eyes. Ophthalmology 2001, 108, 773–779. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).