
Bacterial Urinary Tract Infection and Early Asymptomatic Bacteriuria in Kidney Transplantation Still Negatively Affect Kidney Transplant Outcomes in the Era of Modern Immunosuppression and Cotrimoxazole Prophylaxis
 , , and
, , and
Abstract
1. Introduction
2. Methods
2.1. Study Design and Study Population
2.2. Outcomes and Definitions
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
3.1. Baseline Characteristics of Kidney Transplant Recipients
3.2. Risk Factors for Developing UTI
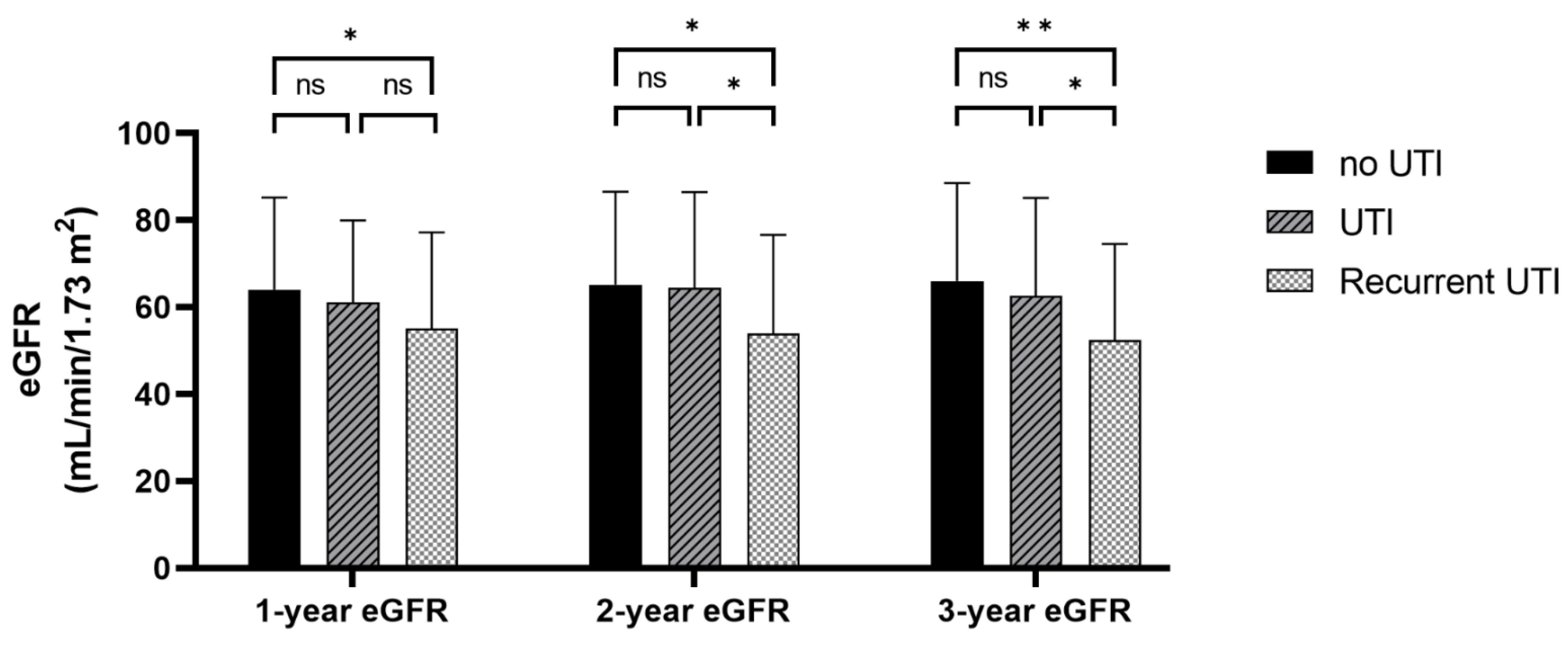
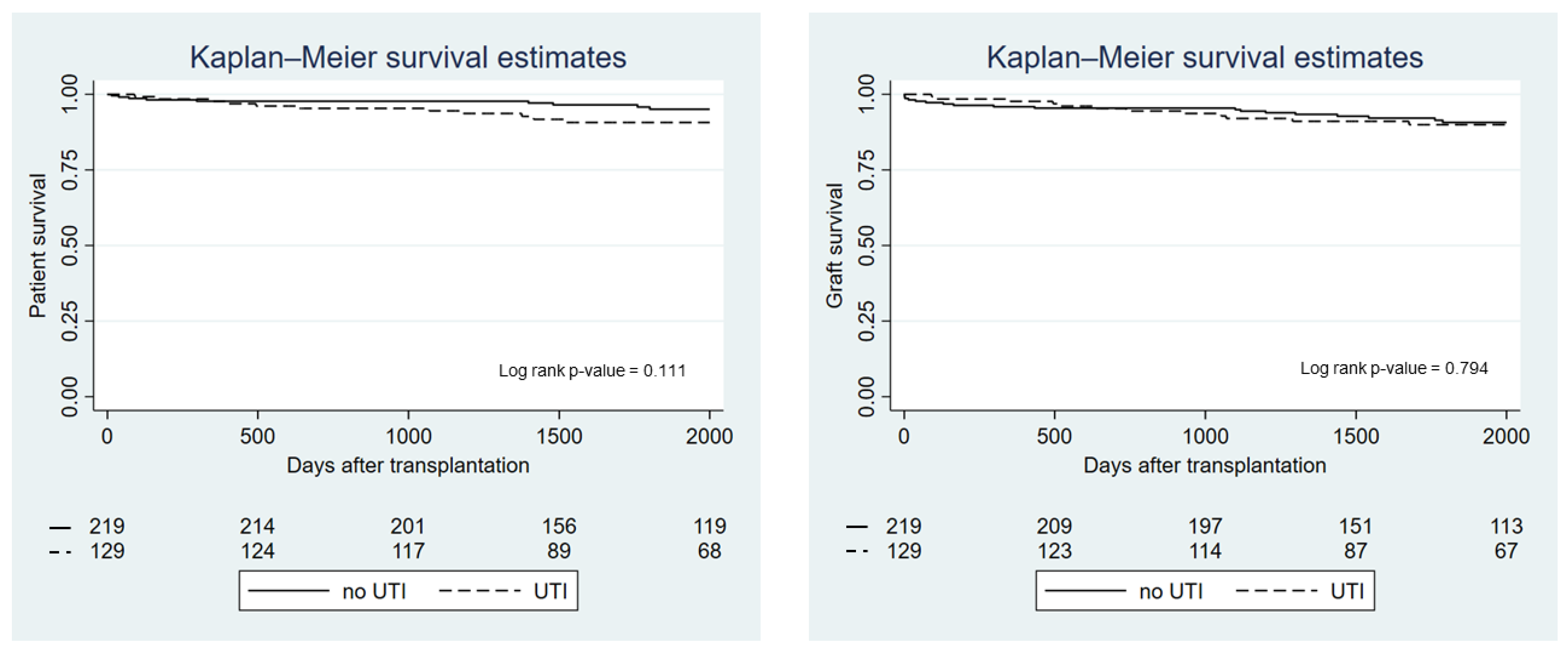
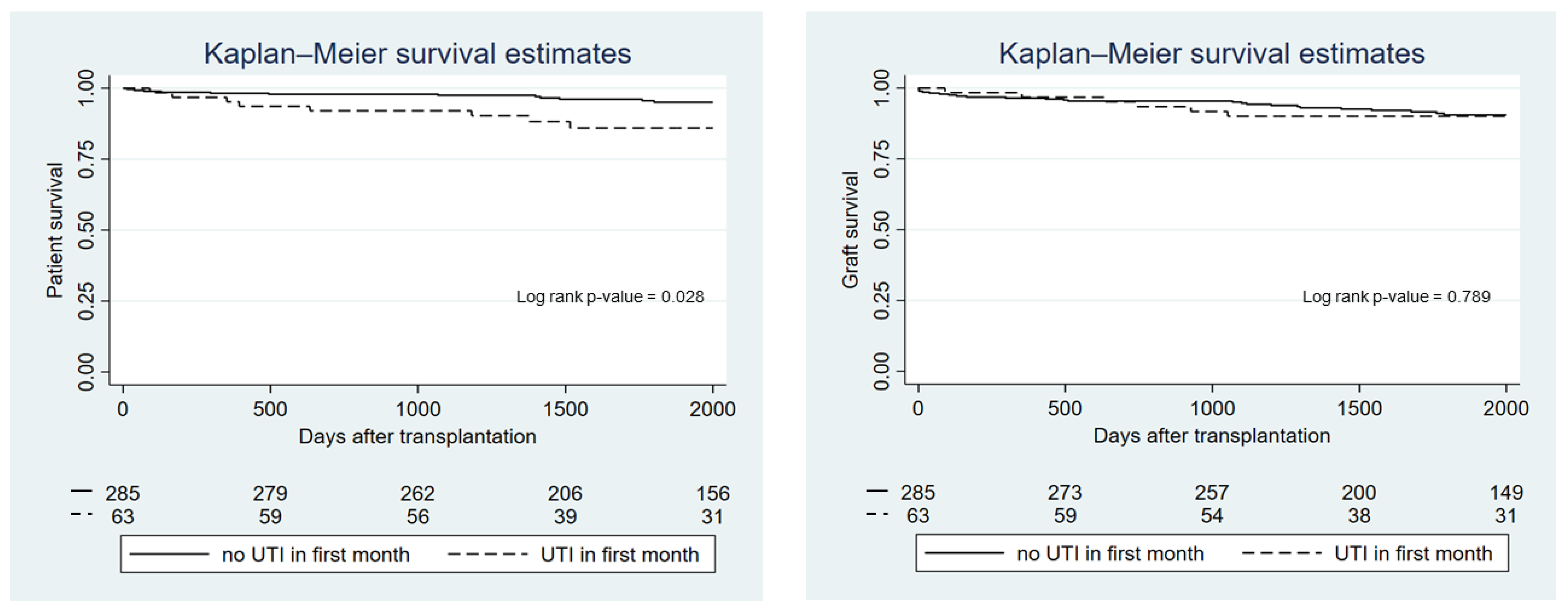
3.3. Association between UTI and Kidney Transplant Outcomes
3.4. Type of Causative Organisms
3.5. Association between Immunosuppressive Medications and UTI
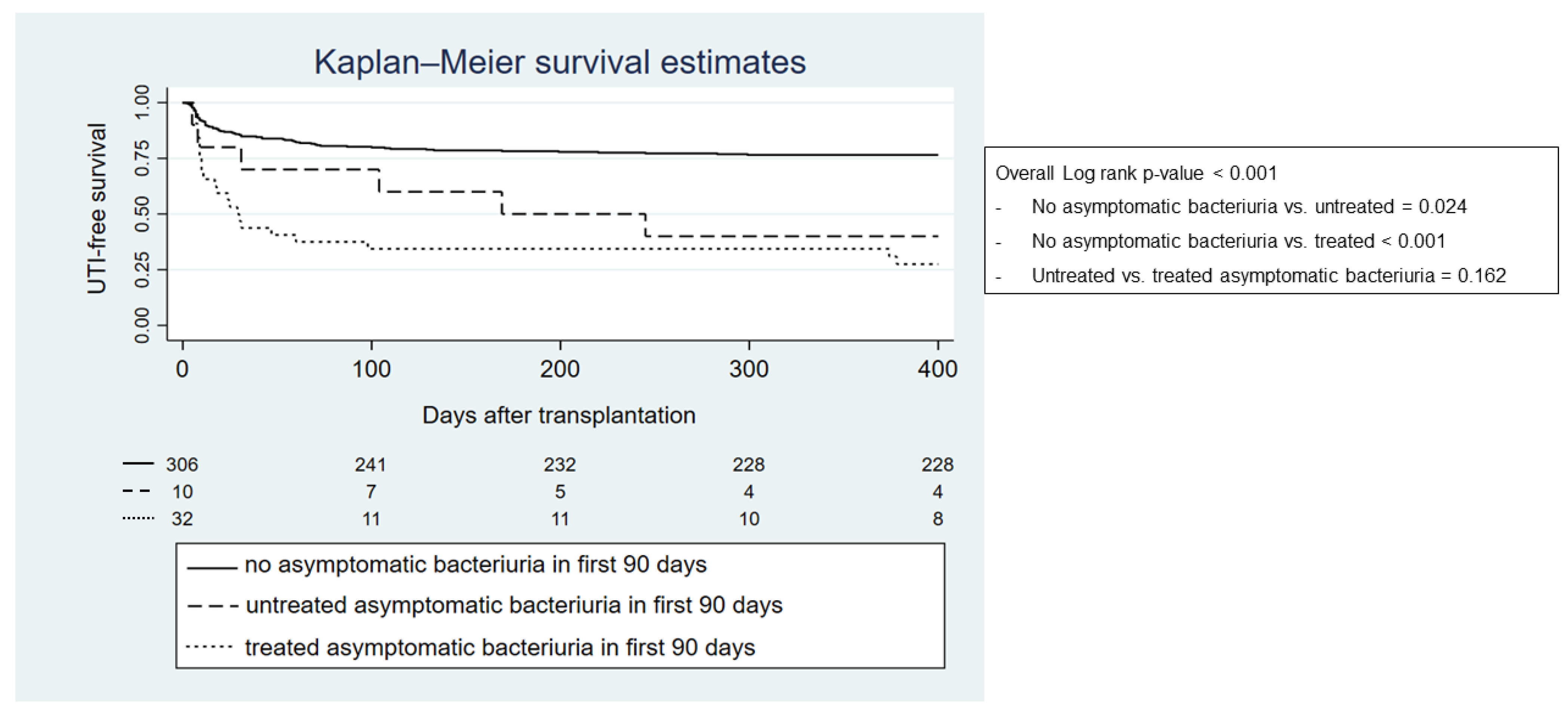
3.6. Risk Factors and Consequences of ASB within the First 90 Days after Transplantation
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Souza, R.M.; Olsburgh, J. Urinary tract infection in the renal transplant patient. Nat. Clin. Pract. Nephrol. 2008, 4, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Säemann, M.; Hörl, W.H. Urinary tract infection in renal transplant recipients. Eur. J. Clin. Investig. 2008, 38 (Suppl. S2), 58–65. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.D.; Julian, K. Urinary tract infections in solid organ transplant recipients: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transpl. 2019, 33, e13507. [Google Scholar] [CrossRef] [PubMed]
- Rice, J.C.; Safdar, N. Urinary tract infections in solid organ transplant recipients. Am. J. Transpl. 2009, 9 (Suppl. S4), S267–S272. [Google Scholar] [CrossRef] [PubMed]
- Karuthu, S.; Blumberg, E.A. Common Infections in Kidney Transplant Recipients. Clin. J. Am. Soc. Nephrol. 2012, 7, 2058–2070. [Google Scholar] [CrossRef] [PubMed]
- Fiorentino, M.; Pesce, F.; Schena, A.; Simone, S.; Castellano, G.; Gesualdo, L. Updates on urinary tract infections in kidney transplantation. J. Nephrol. 2019, 32, 751–761. [Google Scholar] [CrossRef] [PubMed]
- Fernández, M.L.S.; Cano, N.R.; Santamarta, L.; Fraile, M.G.; Blake, O.; Corte, C.D. A Current Review of the Etiology, Clinical Features, and Diagnosis of Urinary Tract Infection in Renal Transplant Patients. Diagnostics 2021, 11, 1456. [Google Scholar] [CrossRef]
- Gao, H.; Zhang, X.; Fu, J.; Lin, F.; Khaledi, A. Overview on urinary tract infection, bacterial agents, and antibiotic resistance pattern in renal transplant recipients. J. Res. Med. Sci. 2021, 26, 26. [Google Scholar] [CrossRef]
- Hollyer, I.; Ison, M.G. The challenge of urinary tract infections in renal transplant recipients. Transpl. Infect. Dis. 2018, 20, e12828. [Google Scholar] [CrossRef]
- Olenski, S.; Scuderi, C.; Choo, A.; Singh, A.K.B.; Way, M.; Jeyaseelan, L.; John, G. Urinary tract infections in renal transplant recipients at a quaternary care centre in Australia. BMC Nephrol. 2019, 20, 479. [Google Scholar] [CrossRef]
- Lyerová, L.; Lácha, J.; Skibová, J.; Teplan, V.; Vítko, S.; Schück, O. Urinary tract infection in patients with urological complications after renal transplantation with respect to long-term function and allograft survival. Ann. Transpl. 2001, 6, 19–20. [Google Scholar]
- Chuang, P.; Parikh, C.; Langone, A. Urinary tract infections after renal transplantation: A retrospective review at two US transplant centers. Clin. Transpl. 2005, 19, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Bodro, M.; Sanclemente, G.; Lipperheide, I.; Allali, M.; Marco, F.; Bosch, J.; Cofan, F.; Ricart, M.; Esforzado, N.; Oppenheimer, F.; et al. Impact of urinary tract infections on short-term kidney graft outcome. Clin. Microbiol. Infect. 2015, 21, 1104.e1–1104.e8. [Google Scholar] [CrossRef] [PubMed]
- Brune, J.E.; Dickenmann, M.; Wehmeier, C.; Sidler, D.; Walti, L.; Golshayan, D.; Manuel, O.; Hadaya, K.; Neofytos, D.; Schnyder, A.; et al. Impact of different urinary tract infection phenotypes within the first year post-transplant on renal allograft outcomes. Am. J. Transpl. 2022, 22, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes KDIGO. Clinical Practice Guideline for the Care of Kidney Transplant Recipients. Am. J. Transpl. 2009, 9 (Suppl. S3), S1–S155. [CrossRef] [PubMed]
- Green, H.; Rahamimov, R.; Gafter, U.; Leibovitci, L.; Paul, M. Antibiotic prophylaxis for urinary tract infections in renal transplant recipients: A systematic review and meta-analysis. Transpl. Infect. Dis. 2011, 13, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Sabé, N.; Oriol, I.; Melilli, E.; Manonelles, A.; Bestard, O.; Polo, C.; Arcos, I.L.; Perelló, M.; Garcia, D.; Riera, L.; et al. Antibiotic Treatment Versus No Treatment for Asymptomatic Bacteriuria in Kidney Transplant Recipients: A Multicenter Randomized Trial. Open Forum Infect. Dis. 2019, 6, ofz243. [Google Scholar] [CrossRef]
- Coussement, J.; Kaminski, H.; Scemla, A.; Manuel, O. Asymptomatic bacteriuria and urinary tract infections in kidney transplant recipients. Curr. Opin. Infect. Dis. 2020, 33, 419–425. [Google Scholar] [CrossRef]
- Coussement, J.; Kamar, N.; Matignon, M.; Weekers, L.; Scemla, A.; Giral, M.; Racapé, J.; Alamartine, E.; Mesnard, L.; Kianda, M.; et al. Antibiotics versus no therapy in kidney transplant recipients with asymptomatic bacteriuria (BiRT): A pragmatic, multicentre, randomized, controlled trial. Clin. Microbiol. Infect. 2021, 27, 398–405. [Google Scholar] [CrossRef]
- Udomkarnjananun, S.; Townamchai, N.; Kerr, S.J.; Tasanarong, A.; Noppakun, K.; Lumpaopong, A.; Prommool, S.; Supaporn, T.; Avihingsanon, Y.; Praditpornsilpa, K.; et al. The First Asian Kidney Transplantation Prediction Models for Long-term Patient and Allograft Survival. Transplantation 2020, 104, 1048–1057. [Google Scholar] [CrossRef]
- Wojciechowski, D.; Wiseman, A. Long-Term Immunosuppression Management: Opportunities and Uncertainties. Clin. J. Am. Soc. Nephrol. 2021, 16, 1264–1271. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.; Ison, M.G.; Danziger-Isakov, L. Long-Term Infectious Complications of Kidney Transplantation. Clin. J. Am. Soc. Nephrol. 2022, 17, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Parasuraman, R.; Julian, K. Urinary tract infections in solid organ transplantation. Am. J. Transpl. 2013, 13 (Suppl. S4), 327–336. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Origüen, J.; López-Medrano, F.; Fernández-Ruiz, M.; Polanco, N.; Gutiérrez, E.; González, E.; Mérida, E.; Ruiz-Merlo, T.; Morales-Cartagena, A.; Asín, M.A.P.-J.; et al. Should Asymptomatic Bacteriuria Be Systematically Treated in Kidney Transplant Recipients? Results From a Randomized Controlled Trial. Am. J. Transpl. 2016, 16, 2943–2953. [Google Scholar] [CrossRef]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed]
- Wolfensberger, A.; Kuster, S.P.; Marchesi, M.; Zbinden, R.; Hombach, M. The effect of varying multidrug-resistence (MDR) definitions on rates of MDR gram-negative rods. Antimicrob. Resist. Infect. Control 2019, 8, 193. [Google Scholar] [CrossRef]
- Glover, M.; Moreira, C.G.; Sperandio, V.; Zimmern, P. Recurrent urinary tract infections in healthy and nonpregnant women. Urol. Sci. 2014, 25, 1–8. [Google Scholar] [CrossRef]
- Czajkowski, K.; Broś-Konopielko, M.; Teliga-Czajkowska, J. Urinary tract infection in women. Menopausal Rev. 2021, 20, 40–47. [Google Scholar] [CrossRef]
- Semins, M.J.; Shore, A.D.; Makary, M.A.; Weiner, J.; Matlaga, B.R. The Impact of Obesity on Urinary Tract Infection Risk. Urology 2012, 79, 266–269. [Google Scholar] [CrossRef]
- Dobner, J.; Kaser, S. Body mass index and the risk of infection—From underweight to obesity. Clin. Microbiol. Infect. 2018, 24, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.-S.; Chang, Y.-C.; Chang, C.-H.; Wu, L.-C.; Wang, J.-L.; Lin, H.-H. The Association Between Body Mass Index and the Risk of Hospitalization and Mortality due to Infection: A Prospective Cohort Study. Open Forum Infect. Dis. 2021, 8, ofaa545. [Google Scholar] [CrossRef] [PubMed]
- Saltiel, A.R.; Olefsky, J.M. Inflammatory mechanisms linking obesity and metabolic disease. J. Clin. Investig. 2017, 127, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Solt, C.M.; Hill, J.L.; Vanderpool, K.; Foster, M.T. Obesity-induced immune dysfunction and immunosuppression: TEM observation of visceral and subcutaneous lymph node microarchitecture and immune cell interactions. Horm. Mol. Biol. Clin. Investig. 2019, 39. [Google Scholar] [CrossRef] [PubMed]
- Magnuson, A.M.; Regan, D.; Booth, A.D.; Fouts, J.K.; Solt, C.M.; Hill, J.L.; Dow, S.W.; Foster, M.T. High-fat diet induced central adiposity (visceral fat) is associated with increased fibrosis and decreased immune cellularity of the mesenteric lymph node in mice. Eur. J. Nutr. 2020, 59, 1641–1654. [Google Scholar] [CrossRef]
- Chadban, S.J.; Ahn, C.; Axelrod, D.A.; Foster, B.J.; Kasiske, B.L.; Kher, V.; Kumar, D.; Oberbauer, R.; Pascual, J.; Pilmore, H.L.; et al. KDIGO Clinical Practice Guideline on the Evaluation and Management of Candidates for Kidney Transplantation. Transplantation 2020, 104, S11–S103. [Google Scholar] [CrossRef] [PubMed]
- Britt, N.S.; Hagopian, J.C.; Brennan, D.C.; Pottebaum, A.A.; Santos, C.A.; Gharabagi, A.; Horwedel, T.A. Effects of recurrent urinary tract infections on graft and patient outcomes after kidney transplantation. Nephrol. Dial. Transpl. 2017, 32, 1758–1766. [Google Scholar] [CrossRef]
- Kotagiri, P.; Chembolli, D.; Ryan, J.; Hughes, P.; Toussaint, N. Urinary Tract Infections in the First Year Post–Kidney Transplantation: Potential Benefits of Treating Asymptomatic Bacteriuria. Transpl. Proc. 2017, 49, 2070–2075. [Google Scholar] [CrossRef]
- Tawab, K.A.; Gheith, O.; Al Otaibi, T.; Nampoory, N.; Mansour, H.; A Halim, M.; Nair, P.; Said, T.; Abdelmonem, M.; El-Sayed, A.; et al. Recurrent Urinary Tract Infection Among Renal Transplant Recipients: Risk Factors and Long-Term Outcome. Exp. Clin. Transpl. 2017, 15, 157–163. [Google Scholar] [CrossRef][Green Version]
- Ciszek, M.; Pączek, L.; Bartłomiejczyk, I.; Mucha, K. Urine Cytokines Profile in Renal Transplant Patients with Asymptomatic Bacteriuria. Transplantation 2006, 81, 1653–1657. [Google Scholar] [CrossRef]
- Lorenz, E.C.; Cosio, F.G. The impact of urinary tract infections in renal transplant recipients. Kidney Int. 2010, 78, 719–721. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-X.; Li, R.; Gu, L.; Xu, K.-Y.; Liu, Y.-Z.; Zhang, R.-W. Risk factors and etiology of repeat infection in kidney transplant recipients. Medicine 2019, 98, e17312. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.; Meyrick, J.; Bath, J.; Dunham, O.; McNulty, C. Effectiveness of behavioural interventions to reduce urinary tract infections and Escherichia coli bacteraemia for older adults across all care settings: A systematic review. J. Hosp. Infect. 2019, 102, 200–218. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Wang, S.; Zhu, Y.; Wang, Z.; Zhao, M.; Chen, D.; Zhou, C. Behavioral and dietary risk factors of recurrent urinary tract infection in Chinese postmenopausal women: A case–control study. J. Int. Med. Res. 2020, 48, 300060519889448. [Google Scholar] [CrossRef] [PubMed]
- Sihra, N.; Goodman, A.; Zakri, R.; Sahai, A.; Malde, S. Nonantibiotic prevention and management of recurrent urinary tract infection. Nat. Rev. Urol. 2018, 15, 750–776. [Google Scholar] [CrossRef] [PubMed]
- Abbott, K.C.; Swanson, S.; Richter, E.R.; Bohen, E.M.; Agodoa, L.Y.; Peters, T.G.; Barbour, G.; Lipnick, R.; Cruess, D.F. Late urinary tract infection after renal transplantation in the United States. Am. J. Kidney Dis. 2004, 44, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Pellé, G.; Vimont, S.; Levy, P.P.; Hertig, A.; Ouali, N.; Chassin, C.; Arlet, G.; Rondeau, E.; Vandewalle, A. Acute Pyelonephritis Represents a Risk Factor Impairing Long-Term Kidney Graft Function. Am. J. Transpl. 2007, 7, 899–907. [Google Scholar] [CrossRef]
- Ghojogh, M.G.; Salarilak, S.; Afshari, A.T.; Khalkhali, H.R.; Mohammadi-Fallah, M.R.; Makhdoomi, K. The effect of urinary tract infection on patient and graft survival rate in a group of kidney transplanted patients. J. Ren. Inj. Prev. 2018, 7, 292–296. [Google Scholar] [CrossRef]
- O’Brien, W.J.; Gupta, K.; Itani, K.M.F. Association of Postoperative Infection with Risk of Long-term Infection and Mortality. JAMA Surg. 2020, 155, 61–68. [Google Scholar] [CrossRef]
- Kim, J.S.; the Korean Organ Transplantation Registry Study Group; Jeong, K.H.; Lee, D.W.; Lee, S.Y.; Lee, S.H.; Yang, J.; Ahn, C.; Hwang, H.S. Epidemiology, risk factors, and clinical impact of early post-transplant infection in older kidney transplant recipients: The Korean organ transplantation registry study. BMC Geriatr. 2020, 20, 519. [Google Scholar] [CrossRef] [PubMed]
- Emal, D.; Rampanelli, E.; Claessen, N.; Bemelman, F.J.; Leemans, J.C.; Florquin, S.; Dessing, M.C. Calcineurin inhibitor Tacrolimus impairs host immune response against urinary tract infection. Sci. Rep. 2019, 9, 106. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.B.; A Fishman, J. Immunosuppressive Agents and Infectious Risk in Transplantation: Managing the “Net State of Immunosuppression”. Clin. Infect. Dis. 2021, 73, e1302–e1317. [Google Scholar] [CrossRef] [PubMed]
- Gołębiewska, J.E.; Dębska-Ślizień, M.A.; Rutkowski, B. Treated asymptomatic bacteriuria during first year after renal transplantation. Transpl. Infect. Dis. 2014, 16, 605–615. [Google Scholar] [CrossRef] [PubMed]
- Antonio, M.E.E.; Cassandra, B.G.C.; Emiliano, R.J.D.; Guadalupe, O.L.M.; Lilian, R.E.A.; Teresa, T.G.M.; Mario, G.G.; Ivan, R.C.G.; Mercedes, R.V.; Alfredo, C.W.; et al. Treatment of asymptomatic bacteriuria in the first 2 months after kidney transplant: A controlled clinical trial. Transpl. Infect. Dis. 2022, e13934. [Google Scholar] [CrossRef]
- Zhou, X.J.; Rakheja, D.; Yu, X.; Saxena, R.; Vaziri, N.D.; Silva, F.G. The aging kidney. Kidney Int. 2008, 74, 710–720. [Google Scholar] [CrossRef] [PubMed]
- Denic, A.; Glassock, R.J.; Rule, A.D. Structural and Functional Changes with the Aging Kidney. Adv. Chronic Kidney Dis. 2016, 23, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Hommos, M.; Glassock, R.J.; Rule, A.D. Structural and Functional Changes in Human Kidneys with Healthy Aging. J. Am. Soc. Nephrol. 2017, 28, 2838–2844. [Google Scholar] [CrossRef]
- Flenker, K.S.; Burghardt, E.L.; Dutta, N.; Burns, W.J.; Grover, J.M.; Kenkel, E.J.; Weaver, T.M.; Mills, J.; Kim, H.; Huang, L.; et al. Rapid Detection of Urinary Tract Infections via Bacterial Nuclease Activity. Mol. Ther. 2017, 25, 1353–1362. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Xu, Y.; Yan, H.; Zhu, Y.; Wang, L.; Zhang, Y.; Lu, Y.; Xing, W. Sensitive and rapid detection of pathogenic bacteria from urine samples using multiplex recombinase polymerase amplification. Lab. Chip. 2018, 18, 2441–2452. [Google Scholar] [CrossRef]
- Greenleaf, E.; Farooq, U.; Jain, A.; DiCristina, R.; Kadry, Z.; Sharma, R. Native kidney pyelonephritis as the cause of recurrent urinary tract infections in a kidney transplant recipient. Kidney Int. 2018, 93, 762. [Google Scholar] [CrossRef]
- Thompson, E.R.; A Hosgood, S.; Nicholson, M.L.; Wilson, C.H. Early versus late ureteric stent removal after kidney transplantation. Cochrane Database Syst. Rev. 2018, 2018, CD011455. [Google Scholar] [CrossRef] [PubMed]
- Visser, I.J.; van der Staaij, J.P.T.; Muthusamy, A.; Willicombe, M.; Lafranca, J.A.; Dor, F.J.M.F. Timing of Ureteric Stent Removal and Occurrence of Urological Complications after Kidney Transplantation: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 689. [Google Scholar] [CrossRef] [PubMed]
- Arabi, Z.; Al Thiab, K.; Altheaby, A.; Tawhari, M.; Aboalsamh, G.; Almarastani, M.; Kashkoush, S.; Shaheen, M.F.; Altamimi, A.; Alnajjar, L.; et al. The Impact of Timing of Stent Removal on the Incidence of UTI, Recurrence, Symptomatology, Resistance, and Hospitalization in Renal Transplant Recipients. J. Transpl. 2021, 2021, 3428260. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables at the Time of Transplantation | Non-UTI Group (n = 219) | UTI Group (n = 129) | p-Value |
|---|---|---|---|
| Age, years (mean ± SD) | 44.2 ± 12.1 | 44.9 ± 11.9 | 0.631 |
| Female, n (%) | 68 (31.1) | 77 (59.7) | <0.001 |
| BMI, kg/m2 (mean ± SD) | 21.4 ± 3.2 | 21.9 ± 3.7 | 0.199 |
| Mode of RRT, n (%) | 0.104 | ||
| Preemptive | 11 (5.0) | 3 (2.3) | |
| Hemodialysis | 197 (90.0) | 113 (87.6) | |
| Peritoneal dialysis | 11 (5.0) | 13 (10.1) | |
| Dialysis vintage, years (median, Q1–Q3) | 2.9 (1.2–5.2) | 3.8 (1.5–6.3) | 0.099 |
| Previous kidney transplantation, n (%) | 9 (4.1) | 7 (5.4) | 0.571 |
| Recipient diabetes mellitus, n (%) | 29 (13.2) | 22 (17.1) | 0.331 |
| Cause of kidney disease, n (%) | 0.876 | ||
| Glomerulonephritis | 70 (32.0) | 46 (35.7) | |
| Diabetic kidney disease | 21 (9.5) | 16 (12.4) | |
| Hypertensive nephrosclerosis | 24 (11.0) | 13 (10.1) | |
| Cystic kidney disease | 10 (4.6) | 5 (3.8) | |
| Urinary tract obstruction/reflux nephropathy | 4 (1.8) | 3 (2.3) | |
| Unknown | 90 (41.1) | 46 (35.7) | |
| Donor age, years (mean ± SD) | 37.6 ± 12.1 | 38.0 ± 11.9 | 0.743 |
| Deceased donor, n (%) | 110 (50.5) | 78 (61.4) | 0.049 |
| Donor serum Cr, mg/dL (mean ± SD) | 1.55 ± 1.47 | 1.46 ± 1.16 | 0.593 |
| HLA mismatch (mean ± SD) | 2.7 ± 1.5 | 3.0 ± 1.6 | 0.084 |
| PRA >50%, n (%) | 15 (6.9) | 24 (18.6) | 0.001 |
| ABO incompatible transplantation, n (%) | 23 (10.5) | 18 (14.0) | 0.335 |
| Total ischemic time >12 h, % | 97 (45.1) | 72 (56.7) | 0.039 |
| Delayed graft function, n (%) | 51 (23.5) | 35 (27.3) | 0.426 |
| Anti-thymocyte globulin induction, n (%) | 25 (11.9) | 22 (17.3) | 0.164 |
| Time to remove Foley catheter, days (median, Q1–Q3) | 7 (7–7) | 7 (7–7) | 0.618 |
| Time to remove drainage tube, days (median, Q1–Q3) | 8 (8–9) | 8 (8–9) | 0.969 |
| Time to remove double J stent, days (median, Q1–Q3) | 26 (19–39) | 28 (20–42) | 0.345 |
| Variable | Univariable Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95%-CI | p-Value * | Adjusted HR | 95%-CI | p-Value | |
| Age (years) | 1.00 | 0.99–1.02 | 0.667 | - | - | - |
| Female (vs. male) | 2.47 | 1.74–3.51 | <0.001 | 2.25 | 1.56–3.24 | <0.001 |
| BMI ≥ 25 kg/m2 | 1.60 | 1.05–2.44 | 0.028 | 1.57 | 1.01–2.44 | 0.044 |
| Hemodialysis (vs. preemptive) | 2.07 | 0.66–6.50 | 0.215 | - | - | - |
| Peritoneal dialysis (vs. preemptive) | 3.77 | 1.07–13.24 | 0.038 | 2.92 | 0.81–10.55 | 0.103 |
| Dialysis vintage (years) | 1.05 | 0.99–1.10 | 0.093 | 0.99 | 0.93–1.07 | 0.879 |
| Previous kidney transplantation | 1.27 | 0.59–2.73 | 0.534 | - | - | - |
| Recipient diabetes mellitus | 1.29 | 0.81–2.04 | 0.281 | - | - | - |
| Cystic kidney disease (vs. other causes of ESRD) | 0.91 | 0.37–2.23 | 0.838 | - | - | - |
| Obstructive/reflux nephropathy (vs. other causes of ESRD) | 1.19 | 0.38–3.74 | 0.769 | - | - | - |
| Deceased donor (vs. living donor) | 1.47 | 1.03–2.10 | 0.035 | 1.00 | 0.46–2.19 | 0.991 |
| Donor age (per 1 year increased) | 1.00 | 0.99–1.02 | 0.697 | |||
| Donor serum creatinine (per 1 mg/dL) | 0.97 | 0.84–1.11 | 0.649 | - | - | - |
| HLA mismatch (per 1 mismatch) | 1.12 | 0.99–1.26 | 0.067 | 1.14 | 1.01–1.29 | 0.041 |
| PRA > 50% (vs. PRA ≤ 50%) | 2.16 | 1.39–3.37 | 0.001 | 1.67 | 1.03–2.72 | 0.038 |
| ABO incompatible transplantation | 1.21 | 0.74–2.00 | 0.445 | - | - | - |
| Total ischemic time >12 h | 1.52 | 1.07–2.16 | 0.020 | 1.52 | 0.74–3.09 | 0.252 |
| Delayed graft function | 1.27 | 0.86–1.87 | 0.235 | - | - | - |
| Anti-thymocyte globulin induction | 1.28 | 0.81–2.03 | 0.294 | - | - | - |
| Time to remove Foley catheter (per 1 day increased) | 0.99 | 0.93–1.06 | 0.780 | - | - | - |
| Time to remove drainage tube, days (per 1 day increased) | 1.02 | 0.99–1.05 | 0.161 | - | - | - |
| Time to remove double J stent (per 1 day increased) | 1.01 | 0.99–1.01 | 0.152 | - | - | - |
| UTI within the First Month (n = 63) | UTI in 2–12 Months (n = 35) | UTI after 12 Months (n = 31) | |||
|---|---|---|---|---|---|
| Organism | % | Organism | % | Organism | % |
| Escherichia coli | 63.4 | Escherichia coli | 54.3 | Escherichia coli | 54.8 |
| Klebsiella spp. | 22.2 | Klebsiella spp. | 14.3 | Klebsiella spp. | 19.3 |
| Enterococcus faecalis | 6.4 | Enterococcus faecalis | 8.6 | Enterococcus faecalis | 12.9 |
| Negative culture | 3.2 | Pseudomonas aeruginosa | 8.6 | Proteus spp. | 6.5 |
| Citrobacter spp. | 1.6 | Proteus spp. | 5.7 | Negative culture | 6.5 |
| Acinetobacter baumannii | 1.6 | Negative culture | 5.7 | ||
| Serratia spp. | 1.6 | Citrobacter spp. | 2.8 | ||
| MDR Organisms | Univariable Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| OR | 95%-CI | p-Value * | Adjusted OR | 95%-CI | p-Value | |
| Tacrolimus dose (per 1 mg/day increase) | 1.20 | 1.04–1.39 | 0.012 | 1.12 | 0.95–1.33 | 0.181 |
| Tacrolimus C0 (per 1 ng/mL increase) | 1.17 | 1.02–1.35 | 0.030 | 1.20 | 1.02–1.42 | 0.032 |
| MPA dose (per 250 mg/day of MMF or 180 mg/day of MPS increase) | 1.43 | 1.05–1.94 | 0.024 | 1.16 | 0.78–1.72 | 0.459 |
| Prednisolone dose (per 1 mg/day increase) | 1.04 | 1.02–1.06 | 0.001 | 1.04 | 1.01–1.07 | 0.007 |
| Recurrent UTI | Univariable analysis | Multivariable analysis | ||||
| OR | 95%-CI | p-value * | aOR | 95%-CI | p-value | |
| Tacrolimus dose (per 1 mg/day increase) | 1.20 | 1.04–1.38 | 0.012 | 1.26 | 1.07–1.50 | 0.007 |
| Tacrolimus C0 (per 1 ng/mL increase) | 1.26 | 1.09–1.47 | 0.002 | 1.28 | 1.10–1.50 | 0.002 |
| MPA dose (per 250 mg/day of MMF or 180 mg/day of MPS increase) | 1.14 | 0.84–1.53 | 0.405 | - | - | - |
| Prednisolone dose (per 1 mg/day increase) | 0.99 | 0.97–1.01 | 0.363 | - | - | - |
| Variable | Univariable Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| OR | 95%-CI | p-Value * | Adjusted OR | 95%-CI | p-Value | |
| Age (years) | 1.00 | 0.97–1.02 | 0.786 | - | - | - |
| Female (vs. male) | 4.15 | 2.04–8.43 | <0.001 | 4.60 | 2.11–10.04 | <0.001 |
| BMI ≥ 25 kg/m2 | 0.99 | 0.42–2.35 | 0.979 | - | - | - |
| Hemodialysis (vs. preemptive) | 1.76 | 0.22–13.86 | 0.590 | - | - | - |
| Peritoneal dialysis (vs. preemptive) | 2.60 | 0.26–25.93 | 0.415 | - | - | - |
| Dialysis vintage (years) | 1.04 | 0.94–1.15 | 0.411 | - | - | - |
| Previous kidney transplantation | 1.04 | 0.23–4.76 | 0.957 | - | - | - |
| Recipient diabetes mellitus | 1.44 | 0.62–3.32 | 0.393 | - | - | - |
| Cystic kidney disease (vs. other causes of ESRD) | 0.51 | 0.07–3.97 | 0.519 | |||
| Obstructive/reflux nephropathy (vs. other causes of ESRD) | 1.22 | 0.14–10.39 | 0.856 | |||
| Deceased donor (vs. living donor) | 1.79 | 0.91–3.53 | 0.094 | 0.46 | 0.08–2.45 | 0.359 |
| Donor age (per 1 year increase) | 1.04 | 1.01–1.07 | 0.014 | 1.05 | 1.01–1.08 | 0.006 |
| Donor serum creatinine (per 1 mg/dL) | 1.06 | 0.83–1.34 | 0.656 | - | - | - |
| HLA mismatch (per 1 mismatch) | 1.07 | 0.86–1.32 | 0.562 | - | - | - |
| PRA > 50% (vs. PRA ≤ 50%) | 2.51 | 1.09–5.74 | 0.029 | 2.00 | 0.78–5.15 | 0.151 |
| ABO incompatible transplantation | 0.77 | 0.26–2.27 | 0.629 | - | - | - |
| Total ischemic time >12 h | 2.66 | 1.31–5.44 | 0.007 | 4.36 | 0.88–21.63 | 0.071 |
| Delayed graft function | 1.82 | 0.92–3.60 | 0.088 | 1.59 | 0.68–3.67 | 0.283 |
| Anti-thymocyte globulin induction | 1.07 | 0.42–2.69 | 0.892 | - | - | - |
| Time to remove Foley catheter (per 1 day increased) | 1.01 | 0.91–1.12 | 0.870 | - | - | - |
| Time to remove drainage tube, days (per 1 day increased) | 1.00 | 0.94–1.06 | 0.945 | - | - | - |
| Time to remove double J stent (per 1 day increased) | 1.00 | 0.98–1.02 | 0.865 | - | - | - |
| Asymptomatic Bacteriuria in the First 90 Days | No UTI in the First Year, n (%) | Non-MDR UTI in the First Year, n (%) | MDR UTI in the First Year, n (%) | Total |
|---|---|---|---|---|
| No asymptomatic bacteriuria | 235 (76.8%) | 31 (10.1%) | 40 (13.1%) | 306 |
| Untreated asymptomatic bacteriuria | 4 (40.0%) | 2 (20.0%) | 4 (40.0%) | 10 |
| Treated asymptomatic bacteriuria | 11 (34.4%) | 4 (12.5%) | 17 (53.1%) | 32 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santithanmakorn, C.; Vanichanan, J.; Townamchai, N.; Jutivorakool, K.; Wattanatorn, S.; Sutherasan, M.; Opanuruk, J.; Kerr, S.J.; Praditpornsilpa, K.; Avihingsanon, Y.; et al. Bacterial Urinary Tract Infection and Early Asymptomatic Bacteriuria in Kidney Transplantation Still Negatively Affect Kidney Transplant Outcomes in the Era of Modern Immunosuppression and Cotrimoxazole Prophylaxis. Biomedicines 2022, 10, 2984. https://doi.org/10.3390/biomedicines10112984
Santithanmakorn C, Vanichanan J, Townamchai N, Jutivorakool K, Wattanatorn S, Sutherasan M, Opanuruk J, Kerr SJ, Praditpornsilpa K, Avihingsanon Y, et al. Bacterial Urinary Tract Infection and Early Asymptomatic Bacteriuria in Kidney Transplantation Still Negatively Affect Kidney Transplant Outcomes in the Era of Modern Immunosuppression and Cotrimoxazole Prophylaxis. Biomedicines. 2022; 10(11):2984. https://doi.org/10.3390/biomedicines10112984
Chicago/Turabian StyleSantithanmakorn, Chayanan, Jakapat Vanichanan, Natavudh Townamchai, Kamonwan Jutivorakool, Salin Wattanatorn, Methee Sutherasan, Julin Opanuruk, Stephen J. Kerr, Kearkiat Praditpornsilpa, Yingyos Avihingsanon, and et al. 2022. "Bacterial Urinary Tract Infection and Early Asymptomatic Bacteriuria in Kidney Transplantation Still Negatively Affect Kidney Transplant Outcomes in the Era of Modern Immunosuppression and Cotrimoxazole Prophylaxis" Biomedicines 10, no. 11: 2984. https://doi.org/10.3390/biomedicines10112984
APA StyleSantithanmakorn, C., Vanichanan, J., Townamchai, N., Jutivorakool, K., Wattanatorn, S., Sutherasan, M., Opanuruk, J., Kerr, S. J., Praditpornsilpa, K., Avihingsanon, Y., & Udomkarnjananun, S. (2022). Bacterial Urinary Tract Infection and Early Asymptomatic Bacteriuria in Kidney Transplantation Still Negatively Affect Kidney Transplant Outcomes in the Era of Modern Immunosuppression and Cotrimoxazole Prophylaxis. Biomedicines, 10(11), 2984. https://doi.org/10.3390/biomedicines10112984