Abstract
Elderly people are sensitive to loneliness, which may contribute to mental and physical health, serious illness, and increased mortality. This study investigates the development trend of information communication technology (ICT) interventions designed for the elderly to reduce loneliness and synthesize its effect. We searched relevant articles on 23 May 2020 using three databases: Ovid-Medline, Ovid-EMBASE, and the Cochrane library. Data extraction and quality assessment were independently performed by two authors. The development is changing from animal robots to online social platforms and from simple emotional support to a multifaceted system that promotes social participation, cognition, physical activity, and nutrition. Our systematic review reported that ICT interventions are being developed to alleviate loneliness and increase social participation. Our study revealed an increase in the use of ICT interventions among the elderly and a positive change in their attitude toward ICT interventions. ICT interventions in the field of nursing should continue to be developed in the future to meet social, health, and safety needs. In the context of coronavirus disease 2019 (COVID-19), ICT interventions are needed to respond effectively to the needs of the elderly. This study is expected to provide basic knowledge for the development of ICT interventions for the elderly.
1. Introduction
According to the current population trend, the proportion of the elderly is expected to rise significantly [1]. Elderly people are sensitive to social isolation and loneliness, which may contribute to mental and physical health, serious illness, and increased mortality [2,3,4,5]. Consequently, reducing social isolation and loneliness in the elderly is an important topic in many countries [6,7]. To prevent the potential risks of social isolation and loneliness, it is crucial to develop social interventions for the age group [8].
The belief that face-to-face interaction is the standard of social participation has been challenged [9], and there is evidence that communication technology can establish feelings of connectivity [10]. Information communication technology (ICT) has emerged to improve the social participation and health conditions of the elderly by reducing social isolation and loneliness [11]. Specifically, there are general ICT interventions, such as the use of the Internet and computer training, and ICT interventions designed for the elderly. ICT interventions designed for the elderly have been developed to help them overcome technical barriers [12], while taking into consideration the interests and preferences of the elderly [12,13,14]. Many recent studies have also been developing ICT interventions, particularly those that follow a senior-centered design [15,16,17].
One study reported that the enjoyment of an ICT intervention designed for the elderly is higher than that of existing ICT interventions for everyone in the market, including traditional groups [12]. In previous studies, ICT interventions designed for the elderly have been reported to be effective in reducing social isolation and loneliness [18,19,20,21,22] by promoting social communication [23,24,25,26,27] and improving participation in physical activities [23,26] among the elderly. ICT interventions have also been accepted by the elderly [22,26] who have a positive attitude toward them, and are intended for daily use [25,28].
Several systematic reviews have examined the effects of ICT interventions on social isolation and loneliness in the elderly [11,29,30,31]. However, these studies reported general ICT interventions, such as the use of the Internet and computer training, not ICT interventions designed specifically for the elderly. Although several studies partially included ICT interventions designed for the elderly, they did not systematically examine the development trends. Moreover, these studies have not comprehensively summarized either the effect of reducing social isolation and loneliness or the satisfaction of using ICT interventions.
Therefore, a comprehensive systematic review including recently published literature needs to be performed to investigate the development trends of and summarize the effects of ICT interventions designed for the elderly to reduce social isolation and loneliness.
2. Materials and Methods
This systematic review was conducted to confirm the development trends and effectiveness of ICT interventions designed for the elderly according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
2.1. Search Strategy
We searched relevant articles on 23 May 2020 using three databases: Ovid-Medline, Ovid-EMBASE, and the Cochrane library. To retrieve eligible articles, the following keywords were used: ((elderly OR older OR seniors OR aging), (information communication technology OR ICT OR social media OR robot OR virtual reality OR application OR online platform OR game OR computer system), and (social isolation OR loneliness OR social support OR social connect OR social interaction OR well-being OR social ties OR the quality of elderly life OR physical and cognitive training OR health care)). All of the search terms and Medical Subject Headings (MeSH) are presented in Appendix A.
2.2. Eligibility Criteria and Study Selection
Two authors of the current study (LSH and CHK) independently selected relevant studies based on predefined inclusion criteria: (a) Studies involving elderly people aged 60 or older; (b) Studies conducting ICT interventions designed for the elderly to reduce loneliness and social isolation; and (c) Studies including protocols and reviews to consider the latest ICT interventions. We excluded studies if they met the following criteria: (a) Posters, abstracts, animal studies, articles not published in English, and duplicated studies; and (b) Studies performing general ICT interventions such as general Internet use, SNS, video games, and others not designed for the elderly. Two reviewers independently screened the titles and abstracts based on the inclusion and exclusion criteria. Full texts of affiliated studies were examined by the same reviewers. The reliability was checked by two authors using Cohen’s kappa coefficient.
2.3. Data Items and Data Collection Process
Data extraction was performed independently and checked by two reviewers using a data collection form predefined by mutual agreement. We extracted some components of the population for ICT interventions, such as sample size, age, sex, subject criteria, and others. We also investigated the development trends and outcome measurements.
We extracted outcomes such as loneliness, social isolation, life satisfaction, social support, quality of life, other emotional responses, usage and usability, and attitudes toward ICT interventions. In case of loneliness indicators (University of California-Los Angeles Loneliness Scale, 20 to 80; Ando, Osada, and Kodama Loneliness Scale, 0 to 10; Short Form of University of California-Los Angeles Loneliness Scale; De Jong Gierveld Loneliness Scale, 0 to 6), lower scores of the social isolation tools (Friendship Scale, 0 to 24) represent a decreasing level of loneliness, while higher scores indicate alleviated levels of social isolation.
Regarding indicators such as life satisfaction (Satisfaction with Life Scale), social support (Duke Social Support Scale; Interpersonal Support Evaluation List, 6 to 36), and health-related quality of life (MOS 36-Item Short-form Health Survey, 0 to 100), higher scores represent a greater level of life satisfaction, social support, and health-related quality of life.
Concerning other affective responses, which are facial expressions (face scale, 1 to 20), moods (The Profile of Mood States, 0 to 4), well-being (Satisfaction with Life Scale; World Health Organization-Five Well-Being Index), comport, satisfaction, and happiness (1 to 5), exercise enjoyment (Physical Activity Enjoyment Scale), and self-efficacy (General Self-Efficacy Scale), higher scores indicated a more positive emotional status of the elderly. Additionally, indicators of salivary chromogranin A, 17-ketosteroid sulfate (17-KS-S) values, and the ratio of 17-ketosteroid sulfate/17-hydroxycorticosteroids (17-KS-S/17-OHCS) were examined, and lower scores indicated a lower level of stress.
As for usability indicators such as usefulness and usability (Technology Acceptance Questionnaire), higher scores and values meant that the ICT interventions were easy to use. For perceptions of ICT interventions and attitudes toward technology (5 to 25), higher scores meant more positive perceptions. Additionally, social cognition (Young Schema Questionnaire) and perceived vulnerability (Perceived Vulnerability Scale, 1 to 6) were examined, and lower scores of the indicators indicated more positive attitude toward ICT interventions.
2.4. Risk of Bias in Individual Studies
Quality assessment of the studies was performed by two authors using the Cochrane Risk of Bias tool (RoB) for randomized controlled trials (RCTs). The assessment consists of seven domains: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and others (other bias). Each domain of the RoB was evaluated with “low,” “high,” or “unclear” risk of bias. In case of disagreement, the two reviewers discussed and agreed on the outcome.
The quality of non-randomized studies was evaluated using the RoB for Nonrandomized Studies (ROBANS). The assessment tool involves six domains: the selection of participants, confounding variables, measurement of intervention (exposure), blinding for outcome assessment, incomplete outcome data, and selective outcome reporting. Further, each domain was scored as 2 (reported and adequate), 1 (reported but inadequate), or 0 (not reported).
3. Results
3.1. Study Selection
After full-text reviews, 14 articles were identified as appropriate for this study. Nine additional articles were found by hand search, and 23 studies were included in the final review process through discussion. Figure 1 illustrates the flowchart of the selection procedure. We checked the reliability using Cohen’s kappa coefficient (k = 0.98).
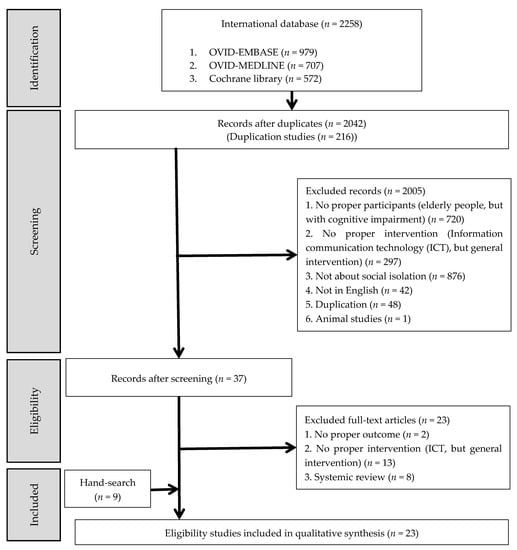
Figure 1.
Flow chart of the study selection.
3.2. Characteristics of Included Studies
Table 1 summarizes the characteristics of the 23 studies, which included four randomized controlled trials, two non-randomized controlled trials, five before studies, three mixed methods, four in-depth interviews, one observational and qualitative study, two reviews, and two randomized controlled trial protocols. These studies searched on 23 May 2020 had been published between 2003 and 2019. The ICT interventions in the included studies were developed via seven studies from Europe, one from North America, five from South America, five from Asia, one from Africa, and two from multiple continents.

Table 1.
General characteristics of selected articles.
3.3. Quality Assessment
Of the 23 selected studies, four were RCTs, and two were non-RCTs. For the four RCTs assessed using the RoB tool, the risk of attrition bias and reporting bias was low. Three of the four studies had a high risk of performance and detection biases. In selection bias, random sequence generation was high, and the allocation concealment was unclear in two of the four studies. The results of the quality assessment using the RoB tool are shown in Figure 2. For the two non-RCTs assessed using the ROBANS tool, the risk of selection of participants, confounding variables, measurement of intervention (exposure), incomplete outcome data, and selective outcome reporting was low. However, the risk of blinding for outcome assessment was high.
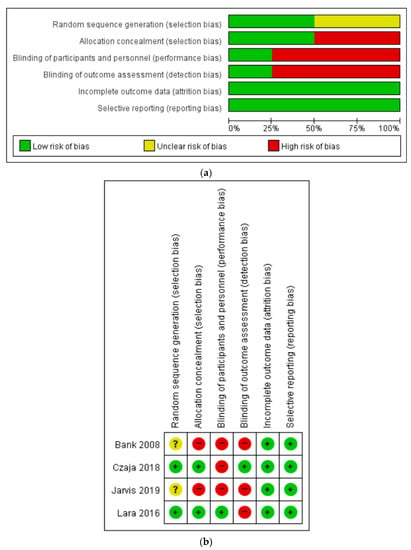
Figure 2.
Quality assessment (a) Risk of bias graph, (b) Risk of bias summary.
3.4. Development Trend
Table 2 provides a summary of the development trends of the included papers in the review. The types of ICT interventions designed for the elderly varied, so the trends in the papers were identified by categorizing them in order of time.
Table 2.
Development trend.
3.4.1. Animal Robot
Five studies targeted animal robots that look like dogs or seals. The robot has a variety of sensors that can react to stimuli. Additionally, the robot has several needs, based on a diurnal rhythm [18,21]. Another robot expresses emotions and recognizes language through communication. Consequently, interaction with the robot has psychosocial effects on the elderly [27,32,33].
3.4.2. Humanoid Agent
Two studies reported software humanoid animated agents that assess the elderly’s affective state and the number of steps per day. Daily conversations with them ease the sense of social isolation, and appropriate healthy feedback motivates the elderly to engage in physical activities. The agents present a graph of their progress, discuss obstacles, and negotiate a goal for the following day [22,23].
3.4.3. Mobile Robot
Four studies presented assistive mobile robots that allows users to control navigation and facilitate social interaction by providing video communication with other people [34]. Therefore, the elderly can reduce loneliness, and caregivers can remotely control the robot and observe the daily life of the elderly. Additionally, some robots carry small objects, measure vital parameters [25,28], detect danger, and help carry out daily activities at home [13].
3.4.4. Exercise Game
Three studies presented an exercise game that is a combination of videogames and exercise. The games allow communication with others, which helps to reduce loneliness during exercise [12,15,35]. Considering the interests and physical conditions of the elderly, an exercise game was designed to achieve motivation and enjoyment.
3.4.5. Interpersonal Communication
Two studies targeted social applications [24,36]. One app allows interaction through photos, audio, videos, and messages using iPads. The interface offers large touch icons for the elderly [36]. These apps enable the elderly to have contact with each other in their homes and reduce loneliness.
3.4.6. Online Social Platform
Seven studies targeted online social platforms that provide easy access to information sources and opportunities to communicate. These platforms promote a lifestyle for the elderly, including physical activities, cognitive function, a safe environment, and emotion. These platforms also include various functions such as self-monitoring, calendars, photos, games, and online help [14,19,20,26,37]. Reflecting the opinions of the elderly, two of seven studies are currently underway [16,17].
3.5. Effectiveness of ICT Interventions Designed for the Elderly
Of 23 selected articles, 14 measured the effectiveness of the ICT interventions designed for the elderly. The results are presented in Table 3. Eight reported the effectiveness of loneliness and social isolation. One examined life satisfaction, two measured social support, one reported quality of life, and eight examined other affective responses. Six reported use and usability, three showed attitudes toward ICT interventions, and two reported others including nutrition and physical activity.
Table 3.
Effectiveness of information communication technology (ICT) intervention for the elderly.
3.5.1. Loneliness and Social Isolation
Eight studies included loneliness and social isolation. There was a decrease in loneliness in the intervention group (3.33 ± 2.16 to 1.00 ± 1.26; p = 0.07) [21] as compared to the passive group (3.57 ± 6.10 vs.−0.8 ± 2.77; p = 0.13) [22]. Additionally, there was a significant decrease in loneliness among those in the intervention group (3.53 ± 1.3 to 1.38 ± 1.33; p < 0.001) as compared to those in the usual care group (3.59 ± 1.23 to 4.00 ± 1.32; p = 0.064) [20], and there was a significant decrease in loneliness and social isolation (p < 0.01) [19]. There were no statistically significant differences in loneliness among those in the intervention group (p > 0.05), but the outcomes were similar to those of the usual care group [12,18,23]. However, there were no significant changes in loneliness before and after the study (p > 0.05) [36].
3.5.2. Life Satisfaction
One study included life satisfaction. It significantly differed between the three groups (p = 0.234) because of the small sample size, family conflicts, and activities provided to control groups [12].
3.5.3. Social Support
Two studies included social support. It was improved and maintained after intervention (p < 0.01) [19]. However, there were no significant changes (p > 0.05), but the elderly answered in an interview that the intervention increased positive mood and self-efficacy [36].
3.5.4. Quality of Life
One study included quality of life. The intervention served to maintain and improve the quality of life after the intervention (38.63 ± 38.86 to 75.00 ± 41.83; p = 0.03). In the activity evaluation, the scores of the last activity significantly increased compared to that of the initial activity [21].
3.5.5. Other Affective Responses
Eight studies included other affective responses. There were positive emotional responses. Scores on the face scale and moods increased after the intervention (p < 0.05) [33]. Comfort (4.59 ± 0.80 vs. 4.33 ± 0.85), satisfaction (3.95 ± 1.08 vs. 3.14 ± 1.26), and happiness (3.89 ± 0.90 vs. 3.26 ± 1.26) improved compared to the passive group (p < 0.05) [22]. Scores of exercise enjoyment were higher than those in other groups (24.4 ± 0.65 vs. 22.0 ± 0.65; p > 0.05) [12]. Emotional words (1.40 ± 0.55 to 2.40 ± 0.55; p = 0.03), amount of speech (1.20 ± 0.45 to 2.50 ± 0.55; p = 0.04), and satisfaction (1.60 ± 0.55 to 3.00 ± 0.00; p = 0.04) increased after the intervention. Moreover, the reaction to stress eased after the activity. Salivary chromogranin A (CgA) decreased after intervention (1.14 ± 0.63 to 0.94 ± 0.74; p < 0.01) [21]. The hormone values of 17-KS-S (1.00 ± 0.51 to 1.41 ± 1.09) and the 17-KS-S/17-OHCS ratio (0.18 ± 0.08 to 0.26 ± 0.09) improved after the activity (p < 0.05) [32,33]. However, self-efficacy was lower than other groups (p > 0.05) [12], and well-being was not significantly different between the intervention and usual care groups (p > 0.05) [20,23]. In contrast, well-being increased significantly (p < 0.05) [19]. Since the elderly performed the intervention alone, limited social interaction occurred [12,23].
3.5.6. Usage and Usability
Six studies included usage and usability. The use of ICT interventions has increased [20,23]. Attachment to intervention increased [18], and the density of objective social networks and average time spent increased [27]. Moreover, the interviewed elderly responded that ICT interventions were easy to use and helpful [19,23,28].
3.5.7. Attitude toward ICT Interventions
Three studies included attitudes toward ICT interventions. Perceptions of ICT interventions were mostly positive [23]. Social cognition about abandonment, defectiveness, emotional deprivation, mistrust, and social isolation of the intervention group (83.53 ± 19.3 to 52.62 ± 15.99; p = 0.008) significantly decreased compared to the usual care group (73.82 ± 29.05 to 78.00 ± 14.77; p = 0.275) [20]. Attitudes toward technology changed positively (p < 0.01) and perceived vulnerability decreased in the intervention group (p < 0.001) [19].
3.5.8. Others: Diet Management, Weight Control, and Physical Activity
Two studies included other interventions such as diet management, weight control, and physical activity. The Mediterranean diet score (4.7 to 4.6) was relatively higher than that of the usual care group (3.8 to 3.8). The body weight (−0.6 vs. −0.3 kg) and waist circumference (−0.9 vs. −0.4 cm) had a smaller reduction than the usual care group. Regarding physical activity, all physical outcomes were similar to those of the usual care group [26]. The increase per week in mean steps walked (411.1 vs. 83.9) was more than that in the standard care group (p = 0.004) [23].
4. Discussion
In our systematic review, we examined 23 studies related to ICT interventions designed for the elderly to reduce loneliness and social isolation. To the best of our knowledge, our study is the most updated and comprehensive systematic review conducted so far and the only one that analyzes the development trends and effects of ICT interventions designed for the elderly. The principal finding of this systematic review is that the trend of development is changing from animal robots to online social platforms and from simple emotional support to a multifaceted system that promotes social participation, cognition, physical activity, nutrition, and sleep. Secondly, our results showed that ICT interventions for the elderly are being developed to alleviate loneliness among the elderly and increase social participation. Thirdly, our systematic review revealed that the elderly increased their use of ICT interventions, and have a positive attitude towards it.
In our study, we examined the development trends of ICT interventions, which is shifting from animal robots to online social platforms especially developed for the elderly. Initially, animal robots were designed for entertainment, communication, and mental therapy [27]. However, the form was evolving from an animal robot that soothes loneliness to online social platforms with more comprehensive functions. Another type of humanoid agent, which appeared as a person on the screen, provided an effective interface modality for the elderly and became a conversational partner and an exercise advisor [23]. Mobile robots assist the elderly in activities of daily living and social interaction, and offer multiple functionalities, such as navigation; fetching, and carrying small objects; measuring vital parameters, providing reminders, a calendar, and interpersonal communication [25]. Others are ICT interventions in exercise games and interpersonal communication technology. The exercise game form allows the elderly to overcome barriers to low exercise adherence by increasing the players’ enjoyment [12] and reducing the risk of social isolation [15]. Interpersonal communication technology can create social connections, helping alleviate social isolation and loneliness [36]. The next step was to create online social platforms. Recently developed online social platforms promoted healthy eating, physical activity, and meaningful social roles [14,17,19]. These services can also support more comprehensive support than previous types of ICT interventions. They can improve the quality of life and help maintain their independence, including improving loneliness and isolation, preventing falling, and managing medications, driving, and transportation [14]. Additionally, they can facilitate active and healthy aging, and prevent cognitive impairment, frailty, depression, anxiety, social isolation, poor sleep quality, and falls [17].
Looking at the research results included in this review, the needs of the elderly have been identified, and efforts have been made to satisfy them. The fundamental needs of the elderly were health needs such as cognitive function or chronic disease management, safety needs such as fall prevention, and social needs such as social participation to reduce loneliness. Therefore, future developments should be proposed not only in emotional care, including loneliness and social isolation but also in a multifaceted way. The results of other systematic reviews [8,11,29,30,31,38,39,40] do not systematically organize the development trend as in our study. However, they suggest that the ICT interventions should be developed to promote affection, health, and safety of the elderly, as shown in our results. The roles of technology should meet the various needs of the elderly. In conclusion, ICT interventions designed for the elderly in the field of nursing should continue to be developed to meet social, health, and safety needs.
Secondly, considering the effects of ICT interventions designed for the elderly, most studies have examined the general effectiveness in improving loneliness, life satisfaction, social support, quality of life, health outcome, and other affective responses compared to real animals or usual care. Some systematic reviews have also identified the effectiveness of reducing social isolation and loneliness and increasing social networks as in our study [8,11,30,40]. Other systematic reviews that reported the social support result also showed a good effect, consistent with our results [38,39]. Another systematic review reported health outcomes that were consistent with our study [31].
However, several studies reported no statistically significant difference between the intervention and control groups regarding loneliness. In those studies, the elderly performed the intervention alone with no supervision, so limited social interaction occurred [12,23]. It determined that to increase the effectiveness of the intervention, compliance should be increased through continuous monitoring. In other cases, although there was no statistical difference in social support, the elderly answered in an interview that the intervention increased positive mood and self-efficacy [36]. The reason previous studies were not statistically significant is because of the small sample size, other life events such as family conflicts, and activities provided to the control group [12]. In terms of the effectiveness of ICT interventions on affect, most studies reported positive emotional responses, such as mood, facial expression, emotional words, amount of speech, comfort, happiness, satisfaction, exercise enjoyment, well-being, and stress reduction [12,19,21,22,27,32,33]. However, some studies using small samples reported that well-being did not significantly change after intervention [20,23]. Although we comprehensively analyzed papers worldwide, because studies had a short intervention interval and a small number of participants who lived alone, further studies designed with a large sample size are required.
The elderly increased their use of ICT interventions, and there was a general increase in positive attitudes toward computers. Most studies reported that the elderly would like to continue using the system, and a significant increase in the frequency of usage demonstrated that elderly use the system comfortably and with minimal training. The majority of users indicated that the intervention was easy to use. To satisfy the needs of the elderly for healthy social participation, administrative care, and safety using ICT, the following conditions were met: affordability, usability, and accessibility. According to other previous study results, it is reported that affordability, usability, and accessibility are the main elements of non-face-to-face services for the elderly [41,42,43]. In our systematic review, there was substantial evidence that the usability of non-face-to-face interventions for the elderly, despite many concerns, has improved. In the future, additional studies that can deal with not only the usability of online interventions but also their affordability and accessibility should be conducted.
In the context of coronavirus disease 2019 (COVID-19), which has become another barrier for face-to-face interaction, it is increasingly difficult to implement offline social services for the elderly through the community care system. With the lack of offline services, the physical condition of the elderly is in greater danger of worsening, which can cause high levels of stress, anxiety, depression, loneliness, and social isolation. Thus, to respond effectively to the needs of the elderly during the COVID-19 crisis, innovative online solutions based on ICTs are needed for personalized interventions [44]. In the future, as the importance of non-face-to-face service increases, this study is expected to provide basic knowledge for the development of such interventions for the elderly.
We identified the development trend and effectiveness of ICT interventions designed for the elderly. However, this study has several limitations. First, most studies in this systematic review varied widely in the methodology regarding the ICT interventions conducted. However, we included reviews or protocols to consider the latest ICT interventions. Second, heterogeneous interventions make comparisons difficult, and it is challenging to draw conclusions. Therefore, the results should be interpreted with caution. Third, more studies are needed to examine the effectiveness of ICT interventions. Therefore, evaluating the effectiveness of ICT interventions requires more randomized clinical trials with large-scale samples and comparative studies. Finally, the outcome measurements were often reported in different ways, which made meta-analysis impossible for selected studies.
5. Conclusions
The development trend of ICT interventions for the elderly is gradually changing from animal robots that provide emotional support to the online social platforms that can promote social participation, cognition, physical activity, nutrition, and sleep. Our research showed that ICT interventions designed for the elderly, compared to real animals or usual care, have proved to be effective in improving loneliness, life satisfaction, social support, quality of life, and other affective responses. Based on this study, ICT interventions designed for the elderly should continue to be developed in the nursing field to meet social, health, and safety needs.
Previous studies have reported that the key elements of ICT interventions for the elderly are affordability, usability, and accessibility [41,42,43]. Our study revealed the improved usability of ICT interventions for the elderly. In the future, studies should be conducted to address the usability of ICT interventions as well as their affordability and accessibility. With the increasing importance of non-face-to-face services in the context of COVID-19, we expect our systematic review to be fundamental knowledge for the development of ICT interventions for the elderly.
Author Contributions
Both authors designed the study: H.K.C., analyzed the extracted data and wrote the initial version of the manuscript. S.H.L., contributed to discussions about data, and critically reviewed the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Gachon University research fund of 2020 (GCU-202002510001).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Gachon University (protocol code 1044396-202005-HR-102-01).
Acknowledgments
The authors would like to express their gratitude to the G University.
Conflicts of Interest
The authors have no conflict of interest to declare.
Appendix A. Search Term
| Population | Intervention | Outcome |
| “The elderly” OR “elderly people” OR “older people” OR “elderly” OR “elderly person” OR “older frail adults” OR “seniors” OR “older adults” OR “aging population” OR “elderly population” OR “aging” OR “exp. aging/” AND | “information communication technology” OR “ICT” OR “social media” OR “exp. social media/” OR “telepresence robot” OR “robotic assistants” OR “assistive robotics” OR “rehabilitation robots” OR “exp. rehabilitation robot/” OR “mobile robotic systems” OR “robotic assistive technologies” OR “service robot” OR “virtual reality and social media OR virtual reality-based application” OR “rehabilitative applications” OR “VR-based social application” OR “virtual reality cognitive training programs” OR “video conference application” OR “social application” OR “technology applications” OR “mobile instant messaging” OR “online platforms” OR “social platform” OR “online service platform” OR “online social support tool” OR “social media platforms” OR “active video game” OR “persuasive video gaming” OR “video game role-play” OR “persuasive social impact game” OR “computer system” OR “exp. computer system/” OR “living in network connected communities” OR “exergames” OR “the Personal Reminder Information and Social Management system (PRISM)” OR “PRISM Buddy” OR “mHealth-supported intervention” OR “WhatsApp” OR “Social Bike application” OR “Will Sports game package” AND | “social isolation” OR “exp. social isolation/” OR “social support” OR “exp. social support/” OR “social connection” OR “social connectedness” OR “loneliness” OR “exp. loneliness/” OR “social interaction” OR “exp. social interaction/” OR “well-being” OR “exp. wellbeing/” OR “social ties” OR “social connectivity” OR “the quality of elderly life” OR “physical and cognitive training” OR “health care” |
References
- Ammar, A.; Bouaziz, B.; Trabelsi, K.; Glenn, J.; Zmijewski, P.; Müller, P.; Chtourou, H.; Jmaiel, M.; Chamari, K.; Driss, T.; et al. Applying digital technology to promote active and healthy confinement lifestyle during pandemics in the elderly. Biol. Sport 2021, 38, 391–396. [Google Scholar] [CrossRef]
- Bartlett, H.; Warburton, J.; Lui, C.-W.; Peach, L.; Carroll, M. Preventing social isolation in later life: Findings and insights from a pilot Queensland intervention study. Ageing Soc. 2013, 33, 1167. [Google Scholar] [CrossRef]
- Cornwell, E.Y.; Waite, L.J. Social disconnectedness, perceived isolation, and health among older adults. J. Health Soc. Behav. 2009, 50, 31–48. [Google Scholar] [CrossRef]
- Eng, P.M.; Rimm, E.B.; Fitzmaurice, G.; Kawachi, I. Social ties and change in social ties in relation to subsequent total and cause-specific mortality and coronary heart disease incidence in men. Am. J. Epidemiol. 2002, 155, 700–709. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, N.R., Jr. Social isolation in older adults: An evolutionary concept analysis. J. Adv. Nurs. 2009, 65, 1342–1352. [Google Scholar] [CrossRef] [PubMed]
- Dickens, A.P.; Richards, S.H.; Greaves, C.J.; Campbell, J.L. Interventions targeting social isolation in older people: A systematic review. BMC Public Health 2011, 11, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Sum, S.; Mathews, M.R.; Pourghasem, M.; Hughes, I. Internet technology and social capital: How the Internet affects seniors’ social capital and wellbeing. J. Comput. Mediat. Commun. 2008, 14, 202–220. [Google Scholar] [CrossRef]
- Li, J.; Erdt, M.; Chen, L.; Cao, Y.; Lee, S.Q.; Theng, Y.L. The Social Effects of Exergames on Older Adults: Systematic Review and Metric Analysis. J. Med. Internet Res. 2018, 20, e10486. [Google Scholar] [CrossRef]
- Van Bel, D.T.; Smolders, K.; IJsselsteijn, W.A.; de Kort, Y. Social connectedness: Concept and measurement. Intell. Environ. 2009, 2, 67–74. [Google Scholar]
- Drageset, J.; Kirkevold, M.; Espehaug, B. Loneliness and social support among nursing home residents without cognitive impairment: A questionnaire survey. Int. J. Nurs. Stud. 2011, 48, 611–619. [Google Scholar] [CrossRef]
- Baker, S.; Warburton, J.; Waycott, J.; Batchelor, F.; Hoang, T.; Dow, B.; Ozanne, E.; Vetere, F. Combatting social isolation and increasing social participation of older adults through the use of technology: A systematic review of existing evidence. Australas. J. Ageing 2018, 37, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Xu, X.; Pham, T.P.; Theng, Y.L.; Katajapuu, N.; Luimula, M. Exergames Designed for Older Adults: A Pilot Evaluation on Psychosocial Well-Being. Games Health J. 2017, 6, 371–378. [Google Scholar] [CrossRef]
- D’Onofrio, G.; Fiorini, L.; de Mul, M.; Fabbricotti, I.; Okabe, Y.; Hoshino, H.; Limosani, R.; Vitanza, A.; Greco, F.; Giuliani, F.; et al. Agile Co-Creation for Robots and Aging (ACCRA) Project: New technological solutions for older people. Eur. Geriatr. Med. 2018, 9, 795–800. [Google Scholar] [CrossRef]
- McTavish, F.; Gustafson, D.H.; Mahoney, J.E.; Johnson, R.A.; Lee, J.D.; Quanbeck, A.; Atwood, A.K.; Isham, A.; Veeramani, R.; Clemson, L.; et al. The effect of an information and communication technology (ICT) on older adults’ quality of life: Study protocol for a randomized control trial. Trials 2015, 16, 191. [Google Scholar]
- Arlati, S.; Colombo, V.; Spoladore, D.; Greci, L.; Pedroli, E.; Serino, S.; Cipresso, P.; Goulene, K.; Stramba-Badiale, M.; Riva, G.; et al. A Social Virtual Reality-Based Application for the Physical and Cognitive Training of the Elderly at Home. Sensors 2019, 19, 261. [Google Scholar] [CrossRef]
- Rochat, J.; Nap, H.H.; Ricci, A.; Cornelisse, L.; Lukkien, D.; Lovis, C.; Ehrler, F. Designing an Online Social Support Platform Through Co-Creation with Seniors. Stud. Health Technol. Inform. 2018, 247, 760–764. [Google Scholar]
- Vercelli, A.; Rainero, I. My-AHA, an ICT platform to detect frailty risk and propose personalized intervention. Syst. Med. 2019, 2, A32–A33. [Google Scholar]
- Banks, M.R.; Willoughby, L.M.; Banks, W.A. Animal-assisted therapy and loneliness in nursing homes: Use of robotic versus living dogs. J. Am. Med. Dir. Assoc. 2008, 9, 173–177. [Google Scholar] [CrossRef]
- Czaja, S.J.; Boot, W.R.; Charness, N.; Rogers, W.A.; Sharit, J. Improving Social Support for Older Adults Through Technology: Findings From the PRISM Randomized Controlled Trial. Gerontologist 2018, 58, 467–477. [Google Scholar] [CrossRef]
- Jarvis, M.A.; Padmanabhanunni, A.; Chipps, J. An Evaluation of a Low-Intensity Cognitive Behavioral Therapy mHealth-Supported Intervention to Reduce Loneliness in Older People. Int. J. Environ. Res. Public Health 2019, 16, 1305. [Google Scholar] [CrossRef] [PubMed]
- Kanamori, M.; Suzuki, M.; Oshiro, H.; Tanaka, M.; Inoguchi, T.; Takasugi, H.; Saito, Y.; Yokoyama, T. Pilot study on improvement of quality of life among elderly using a pet-type robot. In Proceedings of the 2003 IEEE International Symposium on Computational Intelligence in Robotics and Automation. Computational Intelligence in Robotics and Automation for the New Millennium (Cat. No. 03EX694), Kobe, Japan, 16–20 July 2003; pp. 107–112. [Google Scholar]
- Ring, L.; Barry, B.; Totzke, K.; Bickmore, T. Addressing loneliness and isolation in older adults: Proactive affective agents provide better support. In Proceedings of the 2013 Humaine Association Conference on Affective Computing and Intelligent Interaction, Geneva, Switzerland, 2–5 September 2013; pp. 61–66. [Google Scholar]
- Bickmore, T.W.; Caruso, L.; Clough-Gorr, K.; Heeren, T. ‘It’s just like you talk to a friend’ relational agents for older adults. Interact. Comput. 2005, 17, 711–735. [Google Scholar] [CrossRef]
- Hemberg, J.; Santamaki Fischer, R. A Window Toward the World: Older Adults’ Experiences of Becoming in Health and Developing as Human Beings Through Interacting with Others Using Real Video Communication. Holist. Nurs. Pract. 2018, 32, 90–97. [Google Scholar] [CrossRef]
- Koceska, N.; Koceski, S.; Beomonte Zobel, P.; Trajkovik, V.; Garcia, N. A Telemedicine Robot System for Assisted and Independent Living. Sensors 2019, 19, 834. [Google Scholar] [CrossRef]
- Lara, J.; O’Brien, N.; Godfrey, A.; Heaven, B.; Evans, E.H.; Lloyd, S.; Moffatt, S.; Moynihan, P.J.; Meyer, T.D.; Rochester, L.; et al. Pilot Randomised Controlled Trial of a Web-Based Intervention to Promote Healthy Eating, Physical Activity and Meaningful Social Connections Compared with Usual Care Control in People of Retirement Age Recruited from Workplaces. PLoS ONE 2016, 11, e0159703. [Google Scholar] [CrossRef]
- Wada, K.; Shibata, T. Social effects of robot therapy in a care house-change of social network of the residents for two months. In Proceedings of the 2007 IEEE International Conference on Robotics and Automation, Rome, Italy, 10–14 April 2007; pp. 1250–1255. [Google Scholar]
- Koceski, S.; Koceska, N. Evaluation of an Assistive Telepresence Robot for Elderly Healthcare. J. Med. Syst. 2016, 40, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.R.; Schulz, P.J. The Effect of Information Communication Technology Interventions on Reducing Social Isolation in the Elderly: A Systematic Review. J. Med. Internet Res. 2016, 18, e18. [Google Scholar] [CrossRef]
- Chipps, J.; Jarvis, M.A.; Ramlall, S. The effectiveness of e-Interventions on reducing social isolation in older persons: A systematic review of systematic reviews. J. Telemed. Telecare 2017, 23, 817–827. [Google Scholar] [CrossRef] [PubMed]
- Khosravi, P.; Ghapanchi, A.H. Investigating the effectiveness of technologies applied to assist seniors: A systematic literature review. Int. J. Med. Inform. 2016, 85, 17–26. [Google Scholar] [CrossRef]
- Wada, K.; Shibata, T. Living with seal robots—its sociopsychological and physiological influences on the elderly at a care house. IEEE Trans. Robot. 2007, 23, 972–980. [Google Scholar] [CrossRef]
- Wada, K.; Shibata, T.; Saito, T.; Tanie, K. Effects of robot-assisted activity for elderly people and nurses at a day service center. Proc. IEEE 2004, 92, 1780–1788. [Google Scholar] [CrossRef]
- Beer, J.M.; Takayama, L. Mobile remote presence systems for older adults: Acceptance, benefits, and concerns. In Proceedings of the 6th International Conference on Human-Robot Interaction, Lausanne, Switzerland, 8–11 March 2011; pp. 19–26. [Google Scholar]
- Khoo, E.T.; Cheok, A.D.; Nguyen, T.H.D.; Pan, Z. Age invaders: Social and physical inter-generational mixed reality family entertainment. Virtual Real. 2008, 12, 3–16. [Google Scholar] [CrossRef]
- Barbosa Neves, B.; Franz, R.; Judges, R.; Beermann, C.; Baecker, R. Can Digital Technology Enhance Social Connectedness Among Older Adults? A Feasibility Study. J. Appl. Gerontol. 2019, 38, 49–72. [Google Scholar] [CrossRef]
- Czaja, S.J.; Boot, W.R.; Charness, N.; Wendy, R.; Sharit, J.; Fisk, A.D.; Lee, C.C.; Nair, S.N. The personalized reminder information and social management system (PRISM) trial: Rationale, methods and baseline characteristics. Contemp. Clin. Trials 2015, 40, 35–46. [Google Scholar] [CrossRef]
- Forsman, A.K.; Nordmyr, J.; Matosevic, T.; Park, A.L.; Wahlbeck, K.; McDaid, D. Promoting mental wellbeing among older people: Technology-based interventions. Health Promot. Int. 2018, 33, 1042–1054. [Google Scholar] [CrossRef]
- Fuss, B.G.; Dorstyn, D.; Ward, L. Computer-mediated communication and social support among community-dwelling older adults: A systematic review of cross-sectional data. Australas. J. Ageing 2019, 38, e103–e113. [Google Scholar] [CrossRef]
- Morris, M.E.; Adair, B.; Ozanne, E.; Kurowski, W.; Miller, K.J.; Pearce, A.J.; Santamaria, N.; Long, M.; Ventura, C.; Said, C.M. Smart technologies to enhance social connectedness in older people who live at home. Australas. J. Ageing 2014, 33, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Carr, K.; Weir, P.L.; Azar, D.; Azar, N.R. Universal design: A step meet toward successful aging. J. Aging Res. 2013, 2013, 324624. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Coughlin, J.F. PERSPECTIVE: Older adults’ adoption of technology: An integrated approach to identifying determinants and barriers. J. Prod. Innov. Manag. 2015, 32, 747–759. [Google Scholar] [CrossRef]
- Portet, F.; Vacher, M.; Golanski, C.; Roux, C.; Meillon, B. Design and evaluation of a smart home voice interface for the elderly: Acceptability and objection aspects. Pers. Ubiquitous Comput. 2013, 17, 127–144. [Google Scholar] [CrossRef]
- Alexander, G.L.; Wakefield, B.J.; Rantz, M.; Skubic, M.; Aud, M.A.; Erdelez, S.; Al Ghenaimi, S. Passive sensor technology interface to assess elder activity in independent living. Nurs. Res. 2011, 60, 318. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).