Abstract
Background: The purpose of this review is to explore the evidence and efficacy of two trends in early childhood intervention services: the family-centered model and the use of tele-intervention. Methods: A systematic review was carried out following the PRISMA methodology and using three databases: Web of Science, PubMed and Scopus. The studies included were those aimed at children from 0 to 6 years of age, focused on early intervention, and which alluded to the family-centered model and/or tele-intervention. Results: a total of 33 studies were included. Five main themes were identified: (1) The participation of children and family is facilitated and improved by the family-centered model of care; (2) the feeling of competence, self-efficacy, satisfaction and empowerment in professionals and families have a positive impact on quality of life; (3) the use of tele-intervention as a tool for prevention and intervention; (4) preparation for telepractice can improve the development of commitment; (5) tele-intervention as a possible solution to contextual barriers. Conclusions: Tele-intervention in pediatrics is presented as a tool inherent to the family-centered model since its implementation involves several common strategies. Future lines of research should explore the use of this tool as a possible solution to contextual barriers.
1. Introduction
Infant maturational development is the name given to a series of physiological processes that enable the maturation, organization and function of the different apparatuses and systems that together make up the human organism [1,2,3]. Children, through their performance and participation in different activities, experience and interact with the environment by developing the necessary and expected motor, cognitive and sensory-perceptual skills, in order to face increasingly complex challenges, according to their culture, society and age [2]. This suggests that there is a relationship between the number and type of experiences gained and the need for support in different aspects of life. The scientific literature provides descriptive information about children with neurodevelopmental disorders and the appearance of difficulties in the acquisition and deployment of specific intellectual, motor or social functions. This will negatively impact the participation in, and performance of, daily life activities [4,5,6], resulting in their restriction and limitation, respectively [7].
Early intervention means identifying and providing effective early support to children who are at risk of poor outcomes [8]. In these children, it has been shown to improve school performance [9,10,11], as well as skill development and acquisition [12]. Therefore, it is essential to identify and address those who present some alteration in their development or who are at biological, social or environmental risk. This care is offered between the ages of 0 and 6 years in order to improve these capacities and skills, as well as to prevent or reduce the impact of possible difficulties that may arise throughout their lives [2,13,14]. There is also evidence that children who are developmentally delayed or have a diagnosis that affects their development, and who live in small rural municipalities, face unique challenges due to limited access to specialized resources and services [15]. Therefore, there is a pressing need to analyze and research new trends in Early Intervention for these environments and this type of population [12,14,16,17].
Within contemporary trends in Early Intervention, one of the tendencies is based on the involvement of families in supporting the early development of the child, which is essential to overcome the negative consequences associated with disability or developmental delays [18]. With a purely ecological and transactional model, working with the family must be one of the pillars in any system working with early childhood [19,20,21]. This trend is known as family-centered care, the key principles of which are empowerment in decision-making [22]; increased levels of competence and involvement of the family, and the strengthening of the family’s bonds with the practitioners involved in the process [20,23]. The practical application of these principles is positively related to the development of children with disabilities [24]. Therefore, families are considered central elements during the intervention process, who must be guided and trained by the team of professionals who intervene from the family-centered care model.
The introduction of this model into childcare practices is incorporated as the possibility for families to use their specific circumstances to optimize developmental opportunities and thereby increase the child’s quality of life [22]. It differs from the previously established expert model, in which the family is relegated to a secondary role [19]. In fact, in the more classic scientific literature, it is already shown that families play a fundamental role in the field of early intervention because of the time that the family shares with the child [25]. For this reason, they are considered to be fundamental in identifying and responding to the communicative signals of their children [26]. The fundamental principle underpinning intervention based on the family-centered model is to build on the needs, concerns, wishes and expectations of the caregivers themselves, working in natural settings and contexts, not just in a specialized intervention room. The aim is to facilitate real experience-based learning and provide the opportunity to generalize skills into the routines that make up the day-to-day life of families [20,23,27]. Components such as motivation are of vital importance, as an indication of commitment or a feeling of capability [28,29].
Traditionally, family-centered interventions have been carried out face to face, where the practitioner and the family are in the same room [20]. Despite having suggested a practice based on the family-centered model of care, certain factors may hinder access to specialized services. The variables mentioned in the scientific literature and considered to be the most limiting are based on the shortage of specialized professionals, problems accessing transport and the overload of services with long waiting lists [15,18,30]. Such variables are exacerbated in more remote settings. Again, the conditions of rural–urban disparity become notable and bring to light accessibility barriers that directly and negatively affect the response to the care needs required by families. Sanz Tolosana et al. [31] conclude that it is necessary to consider inclusive policies that truly take into consideration the different particularities of the rural population and their territories. Recent studies refer to the use of alternative tools or methods to conventional actions that take advantage of the development of technological resources, something which is currently in constant growth. In the healthcare context, this is known as tele-intervention.
In response to these challenges, and with the advent of the global health emergency caused by COVID-19, the need to find alternative solutions to the existing ones has become apparent in order to ensure continuity and proper development of care services. In this sense, the use of Information and Communication Technologies (ICT) has provided a feasible option to guarantee access to different intervention services in the sphere of healthcare [32,33]. The application of this technology in the provision of healthcare services is known as tele-intervention, including interactive services for both remote consultation and remote diagnosis [34]. Superficially, tele-intervention does not differ much from expert model’s methodology, with the interaction between the child, family, practitioner and support staff being the common thread of the intervention [18]. In the study by Olsen et al. [35], they compared the interactions between different participants during both telematic and face-to-face sessions. On the one hand, family coaching was conducted simultaneously with the session with the child, in order to discuss and select strategies to facilitate the child’s development and acquisition of skills. On the other hand, a direct interaction with the family and the child took place. This second procedure allowed for continuity in the sessions while the family received information and comments in situ from the practitioner, making it possible to generalize learning to the real environment. Statistically significant differences were found between the intervention-defining behaviors in the different groups.
Given the imminent paradigm shift in early childhood care in recent years, compounded by the global pandemic of 2020, there is a need for continued research in this area.
This Study
This study aims to explore and synthesize the existing scientific evidence surrounding two types of interventions implemented in the field of Early Childhood Intervention: one based on the Family-Centered Model and the other on tele-intervention, both targeting pediatric populations with developmental issues or at risk of experiencing them. It focuses on exploring studies involving individuals aged between 0 and 6 years old, aiming to enhance levels of independence and functional autonomy. Additionally, it emphasizes the search of disparities in the form of intervention between rural and urban environments. The two types of intervention have been chosen for the same study due to their complementary nature of bringing Early Intervention closer to families. In addition, they are having a growing interest at a professional and a research level. Therefore, the question arises as to whether the models that bring Early Intervention closer to the family show scientific evidence and what benefits they bring to the intervention.
The main objective is to understand the scientific evidence regarding the efficacy of tele-intervention and the Family-Centered Model in Early Childhood Intervention. To achieve this, two specific objectives are presented: explore the effectiveness evidenced in the use of the Family-Centered Model in early childhood care practices and examine the effectiveness and effects of interventions that use tele-intervention.
2. Materials and Methods
2.1. Study Design
A systematic review was conducted to explore the degree of effectiveness of early interventions based on the family-centered model and tele-intervention. To this end, we worked on the basis of the updated Preferred Reporting Items for Systematic Review and Meta-analyses (PRISMA) 2020 guidelines [36]. Use is made of the International Classification of Functioning, Disability and Health (ICF) [7,37] nomenclature to express the results obtained in the search. In an initial phase, and with the aim of offering a contemporary view of the topic, the last complete decade was taken as a reference for the search for studies, that is, from 2012 to 2023.
2.2. Search Strategy
A combined strategy of electronic searches was carried out in order to identify target studies for the research. These studies had to have been published between 2012 and the date of the search in the following databases: Web of Science, PubMed and Scopus. The search terms were differentiated into two distinct phases under the same central axis that coincides with the main theme of the study: the Early Childhood Care resource. The first search phase corresponded to early intervention and the family-centered intervention model. The second search phase consisted of linking the concept of early intervention with tele-intervention. In both phases, the Boolean operators AND, NOT and OR are combined to identify potential articles that integrate the aforementioned topics in the same study. The searches carried out in each of the databases are described in detail in Appendix A. Subsequently, the different titles and abstracts were reviewed to determine whether the studies were related to the main objective of this research and the inclusion and exclusion criteria described below.
2.3. Selection Criteria
The catalogue of services and benefits varies according to the different territorial contexts. This also affects the definition of the main focus of this research. For the purposes of this systematic review and possible future lines of research, early intervention will be understood as the set of interventions aimed at the child population aged 0–6 years, the family and the environment, responding as early as possible to the temporary or permanent needs of children with developmental disorders or at risk of suffering from them.
All studies included in this review are subject to meeting the following criteria: (1) the interventions carried out are framed within the framework of early childhood care; (2) variables related to the effectiveness of interventions based on the family-centered model and/or tele-intervention were investigated; (3) the different perspectives of one or more of the following possible groups involved were explored: family, infants, professionals; (4) a sample given by any number of infant individuals was described; regardless of cause, gender, ethnic group or geographical location with an age between 0 and 6 years; (5) the study is available in English and/or Spanish; (6) studies that dealt only with purely biomedical interventions that did not consider psychosocial aspects, such as the different perspectives of the groups that could be involved in the process, were excluded; (7) studies that were developed in contexts of high specificity (e.g., Neonatal Units) were excluded; (8) documents whose development and ultimate aim consisted of the creation of protocols or good practice manuals; and (9) conference proceedings, as they were not certain to have been peer-reviewed, were excluded.
2.4. Selection of Studies
The search results were imported into the Zotero bibliographic manager [38] version 6.0.26 for the removal of duplicates and then screened by title/abstract. The full texts of all the studies that passed the first selection stage were reviewed to assess their eligibility according to the inclusion and exclusion criteria. In parallel, in order to extract the relevant information for the study, a content analysis (i.e., an in-depth reading of the studies) was performed to obtain a list of the most decisive and defining data.
2.5. Quality Assessment and Risk of Bias
A classification of the levels of evidence and grades of recommendation of the selected articles based on the Scottish Intercollegiate Guidelines Network (SIGN) has been included to assess the quality of the studies [39]. This guide classifies the level of evidence according to the type of study design in an interval from 1 to 4, with the symbols “++”, “+” and “−” in scores 1 and 2, in order to further detail this level of evidence. In addition, based on this first classification, this guide allows the establishment of grades of recommendation in the interval A–D, with the study classified as “A” resulting from a direct recommendation.
This tool makes it possible to reduce different types of bias, as its authors indicate, having been used in previous systematic reviews [40]. Likewise, to specifically avoid the risk of individual bias, two members of the team separately made the final choice of studies to include. Those in which there was no consensus were discussed with a third reviewer. Subsequently, parallel processes were also carried out to decide the relevant variables to record from the articles, with subsequent discussion of cases where there was no consensus. For all these processes, Microsoft Excel version 16.74 software was used.
3. Results
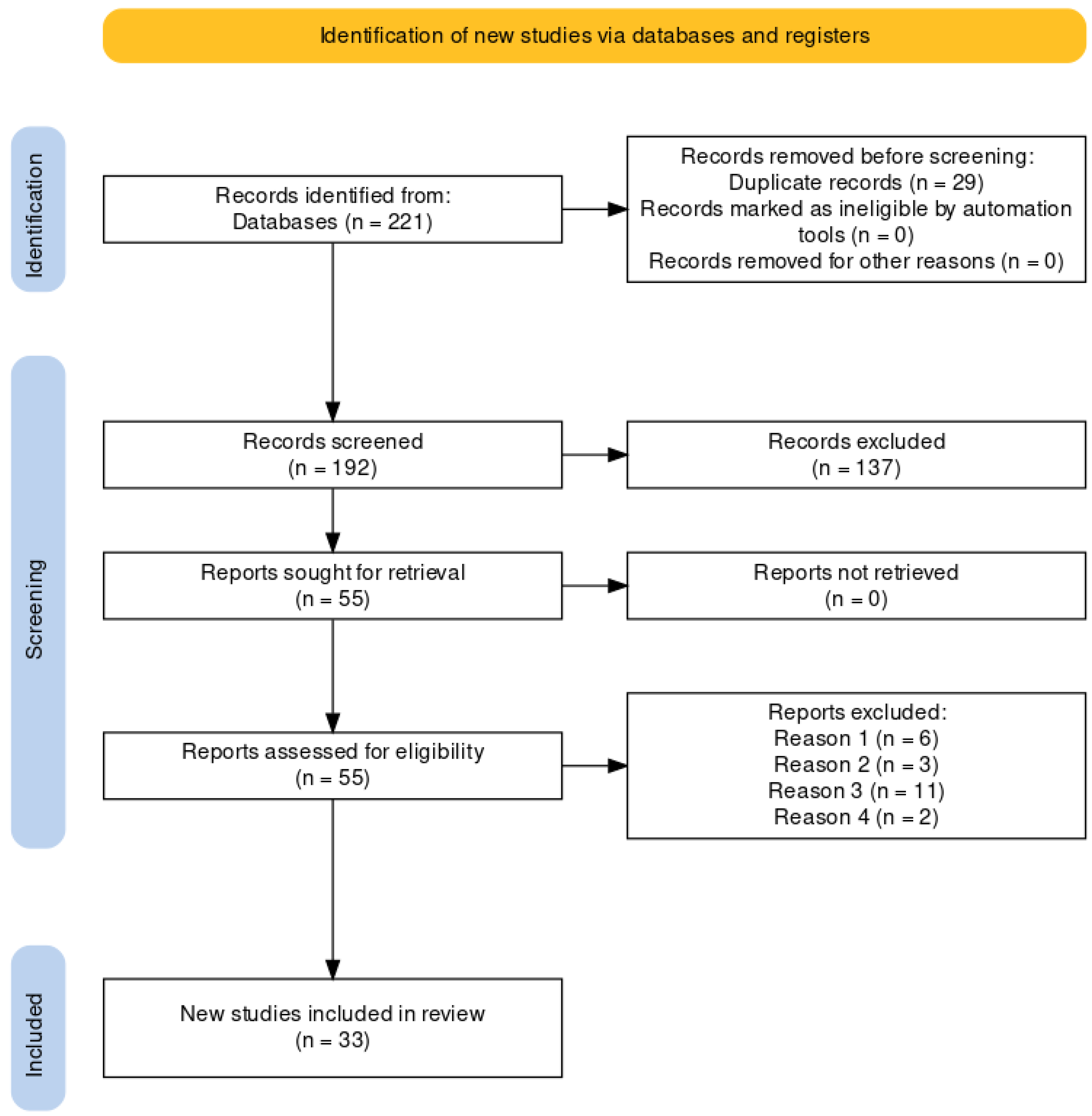
The results of the search in the different databases and the next steps applied can be seen in the flowchart represented in Figure 1. The original search yielded a total of 221 potential studies. A total of 29 duplicate publications were then eliminated. Of the remaining 192 potential articles, a first screening was done by reading the title and abstract, discarding a total of 137 publications; a total of 55 articles were proposed for full reading. Finally, 33 studies were included in the review, having met the inclusion criteria.
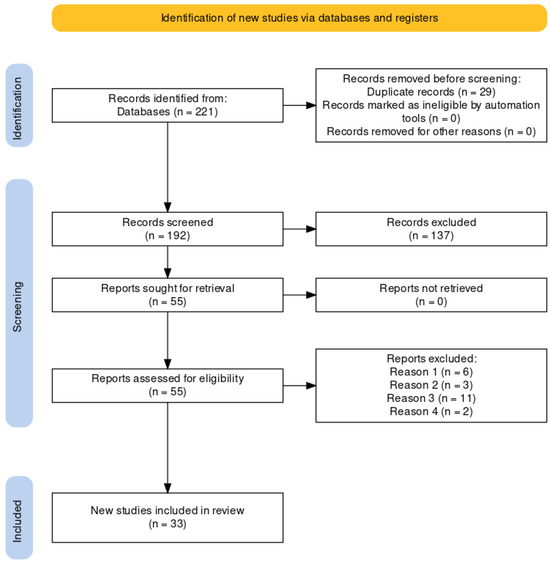
Figure 1.
Flowchart for the identification of new studies through databases and registers according to PRISMA. Reason 1: selection criterion 6; Reason 2: selection criterion 5; Reason 3: selection criterion 8; Reason 4: selection criterion 4.
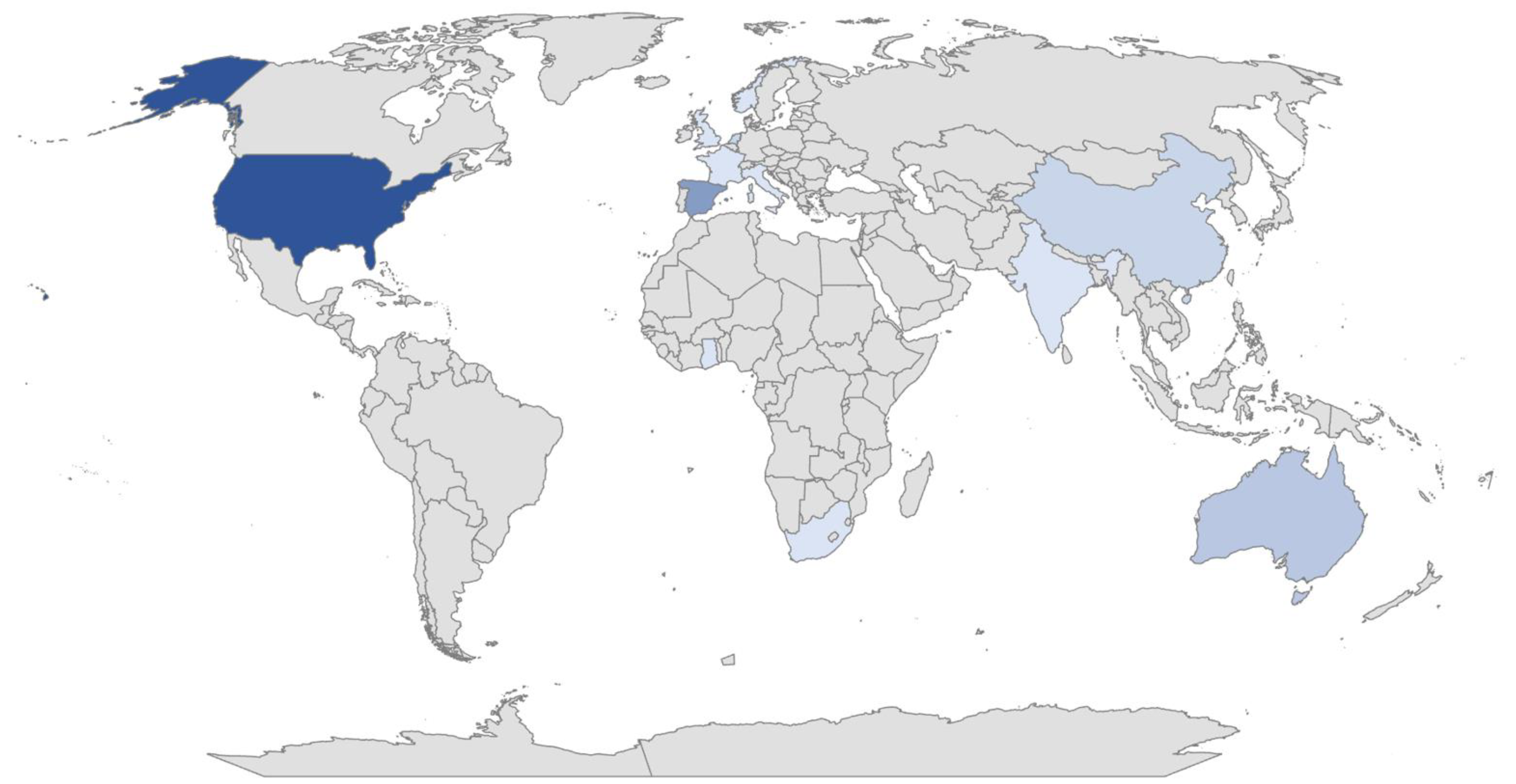
Of the publications finally selected for analysis, 15 (45.45%) dealt with the Family-Centered Care Model; 12 (36.36%) with tele-intervention and 6 (18.2%) with both. Of the total number of studies, 85% were quantitative, 6% were qualitative and 9% used a mixed methodology. These studies were conducted from different geographical locations worldwide, corresponding to the following percentages and represented in Figure 2: United States (33%), Spain (18%), Australia (9%), Netherlands (6%), China (6%), India (3%), Italy (3%), South Africa (3%), France (3%), Taiwan (3%), Republic of Korea (3%), United Kingdom (3%), Ghana (3%) and Norway (3%). Furthermore, different disciplines were involved in the research, on the one hand: physical therapy, occupational therapy, developmental therapy, speech therapy, physiotherapy, psychology, social work, pedagogy and neuropediatrics, and on the other, a variety of participants, with three main groups: family members or primary caregivers (63%), infants (24%) and clinicians (18%), with the first target group being the most predominant. Some of the studies included several of these samples simultaneously. A variety of diagnoses were also described: autism spectrum disorder (9%), visual impairment (1%), hearing impairment (18%), deafblindness (3%), motor impairment (3%), developmental delay (15%), as well as other variables or factors related to the different interactions between the practitioner, the family and/or the child.
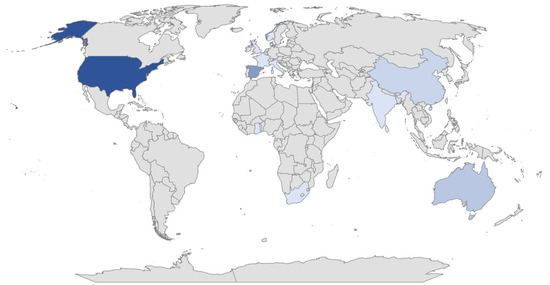
Figure 2.
Geographical territory where the research selected for this study has been carried out worldwide. Colors of higher intensity represent higher density values.
The record of the extraction of these data is summarized in Table 1. Likewise, the data concerning the degree of evidence of these studies are reflected in Table 2.

Table 1.
Extraction record and description of the studies reviewed.
Table 2.
Level of evidence and grade of recommendation according to SIGN.
3.1. Data Extraction and Synthesis
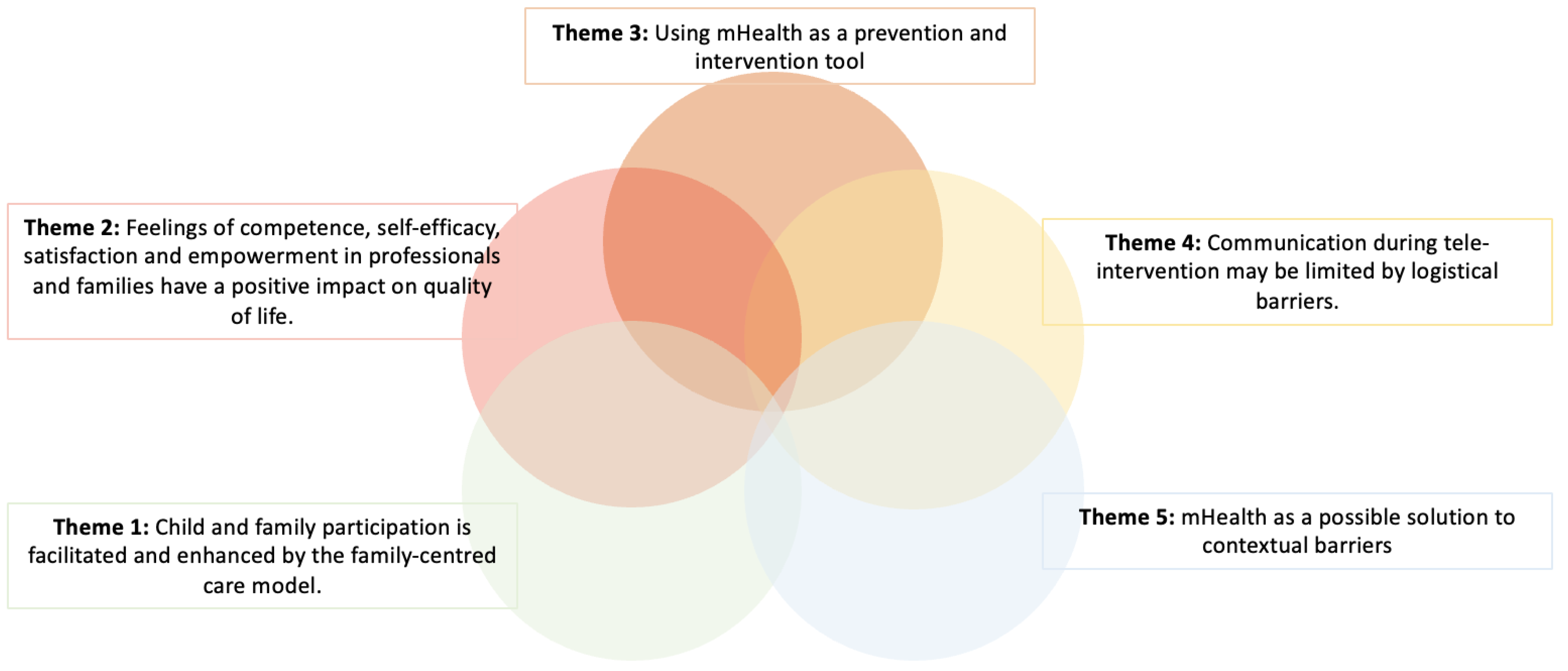
As a result of the thematic synthesis process, five main themes were identified that are in line with the objectives of the study: (1) the participation of children and family is facilitated and improved by the family-centered model of care; (2) the feeling of competence, self-efficacy, satisfaction and empowerment in professionals and families have a positive impact on quality of life; (3) the use of tele-intervention as a tool for prevention and intervention; (4) preparation for tele-intervention can improve the development of commitment; and (5) tele-intervention as a possible solution to contextual barriers (Figure 3).
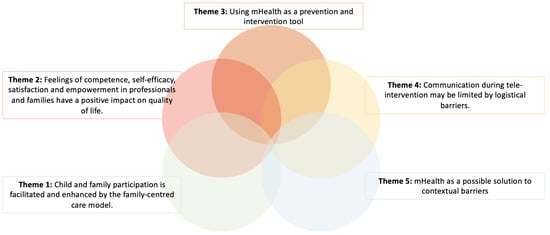
Figure 3.
Representation of the five emerging themes from the studies included in this systematic review.
This thematic synthesis has been carried out through the subtraction of the different study variables and the results provided by the authors, finally pooling the different themes mentioned above. The reason why the results are presented in this way is to illustrate the information presented in Table 1 in order to facilitate reading.
3.1.1. The Participation of Children and Family Is Facilitated and Improved by the Family-Centered Model of Care
The family-centered model of care was described as a facilitator in establishing a link with the clinical environment in the early intervention setting. This approach allowed both children and family to feel safe and motivated throughout the process [21,41,42,44,59,64,65].
Thanks to the principles that guide this model [22,25], the establishment and subsequent maintenance over time of the bonds of the therapeutic relationship is made possible. A large number of the families described the implementation of this model as positive, showing higher levels of satisfaction, confidence, competence and empowerment with the service [42,44,64].
The study by Dick et al. [56] showed a comparison between the early intervention service and the primary care service. In the former, the context invited an understanding of the family as an active agent and, therefore, their inherent inclusion in the intervention plan from the very beginning. This generated an approach to the domains of habituation and participation which, in turn, translated into satisfaction, self-efficacy and positive perception of the service on the part of the families. The second, on the contrary, a more biomedical context, entailed placing the child as the sole focus of intervention, differing the practitioner–caregiver relationship from the previous context.
3.1.2. Feelings of Competence, Self-Efficacy, Satisfaction and Empowerment in Practitioners and Families Have a Positive Impact on Quality of Life
Practices based on the family-centered model ensure family commitment and are related to positive therapeutic outcomes [41,42,43,44,48,53,59,61,63,64,65]. As shown in the previous section, variables such as competence, self-efficacy, satisfaction, and empowerment are of great importance since, to some extent, the intervention will depend on them. Taking into account aspects such as the family’s beliefs, values and needs, as well as offering individualized support and guidance [43], are practices that favor the appearance of higher levels of the aforementioned variables, which is why their promotion is necessary and in turn generate a good therapeutic relationship [20,23].
Although there is a desire to generalize the family-centered model in current practices [22], different barriers are described that are independent of the practitioners, such as lack of time, resources, training, or aspects related to the organization and structure of the system [21,60].
On the other hand, the results obtained in the study by Cheung et al. [54] point to the need for practitioners to strengthen their knowledge and skills to provide a service based on the family-centered model. The ultimate goal is to empower caregivers by creating learning opportunities for this learning to be generalized and applied to the natural environment [72]. The findings suggest that an intervention based on these principles promotes and helps to achieve the child’s goals, as well as higher levels of caregiver satisfaction and internal motivation [63,65].
3.1.3. Use of Tele-Intervention as a Tool for Prevention and Intervention
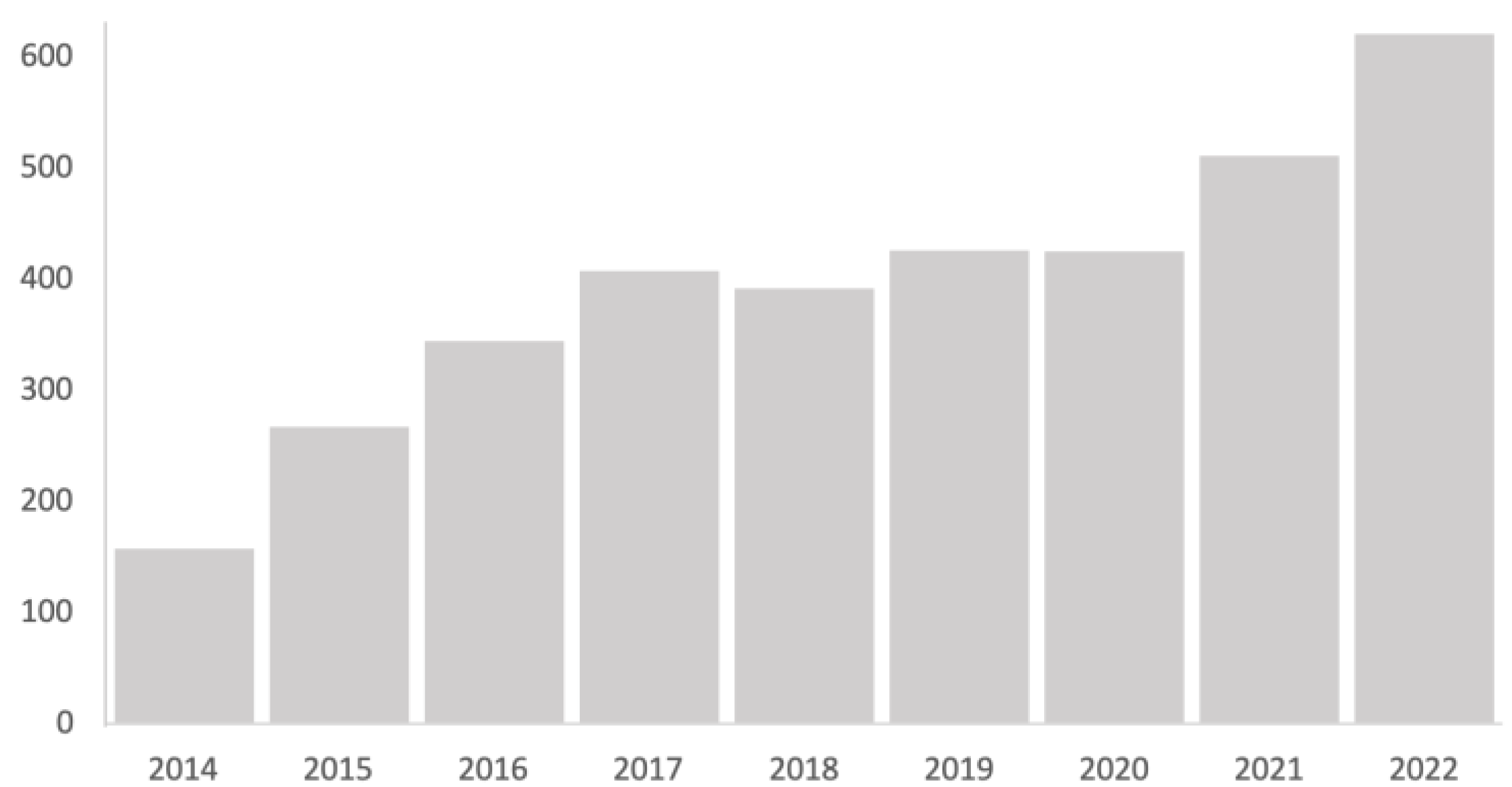
In the scientific literature, the use of tele-intervention was described in the healthcare context as an alternative tool to conventional interventions. The use of technology in this field is becoming increasingly common in assessment and intervention processes. This can be seen in the progressive increase in the number of publications that include this term in the Web of Science (Figure 4). The casuistry, the circumstances and the approach from which tele-intervention is used entails the application of techniques or forms of action that are inherent to the family-centered model: active family participation, attention to the needs and priorities demanded, joint search for solutions [42,51,63].
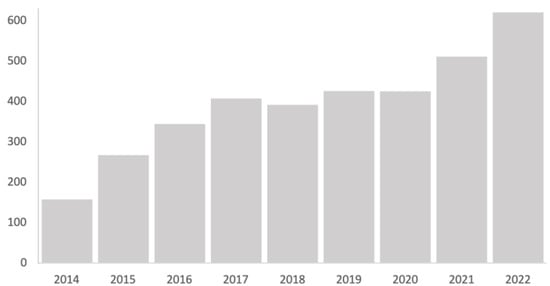
Figure 4.
Trends in the number of publications in Web of Science that include the term “mHealth” in the title in the period 2014–2022. Source: Web of Science (WOS).
The methodologies used in the community healthcare field are backed by research that ensures evidence-based clinical practice with empirical results. The implementation of new techniques or intervention models not only requires theoretical validation to justify and provide quality but also social validation.
The recent study by Martínez-Rico et al. [42] conducted in a Spanish population analyzes factors of feasibility, usefulness or possible future interventions of tele-intervention in early intervention services. It also takes into account usability, effectiveness, competence and trust, factors that are relevant to what the authors call social validity. Other studies such as those by McCarthy et al., Popova et al., García-Ventura et al., du Plessis et al., Rose et al. and Vilaseca et al. [20,21,52,58,60,66] assess factors that have to do with the technical staff who carry out the intervention, seeking their professional validation.
The global health emergency caused by COVID-19 compromised the vast majority of methodologies and techniques that were carried out in a traditional, face-to-face manner, leading to a change in their modality [73,74]. In this context, protocols and guidelines were developed to facilitate this shift towards tele-intervention. The use of tele-intervention became very important and was done with different objectives. On the one hand, a preventive vision was taken, where the objective was to provide quality information and raise awareness among the population, as well as strategies for maintaining a healthy lifestyle. On the other, from a more interventional point of view, new forms of practitioner–user communication were facilitated, and the diagnostic and treatment process was adapted without the need for travel. In other words, the aim was to act in the natural environment [75].
In the systematic review process, 2 studies were detected where the terms “COVID-19” and “Telehealth” are found in the title, and both describe the use of tele-intervention technology as an intervention tool with positive results in children [75]. Miller et al. [50] report closer follow-up of neonates after discharge from the intensive care unit, which led to increased detection of cases requiring additional referral to another service. In the paper by Kronberg et al. [63], technicians worked with a coaching-based intervention with families for 9 months. The findings suggested that the use of tele-intervention in that procedure was effective in achieving goals. A subsequent study published by Qu et al. [45] in a population with Autism Spectrum Disorder (ASD) used the same intervention method and obtained positive results in terms of family perception variables.
Subsequent research continues this line of prevention and intervention in determining aspects of the health of infants aged 0 to 6 years, showing rates of effectiveness and acceptability, in which the figure of the family and its context are highlighted in the process [42,45,51,53,54,57].
3.1.4. Communication during Tele-Intervention May Be Limited by Logistical Barriers
A previous training and interaction stage prior to the use of the tele-intervention methodology could improve the development of commitment and communication between families and practitioners. In this sense, there are two main groups to take into account: the family and the technical team.
The study by Yang et al. [62] shows reluctance about the use of telehealth in the early intervention service. Several family members reported feelings of discomfort and inability to conduct sessions remotely or skepticism that professionals could solve situations remotely. One possible explanation put forward was that the family was seeking a child-centered approach to intervention where the use of face-to-face materials with the therapist was viewed as more valuable. Other barriers to its implementation also come into play, which are consistent with the studies by Rose et al., Blaiser et al., and Li et al. [66,69,70], and are limiting for the proper functioning of the sessions. These refer to access to a line with unlimited data, broadband internet connection and electronic devices, as well as the ability to manage them.
Another barrier they highlight and which is directly related to family perceptions is adherence. Research by Li et al. [69], which made use of SMS text messages as a tool for collecting data about health programs in rural China, showed a low participation rate justified by participants as forgetfulness. In these situations, Staiano et al. [57] propose the use of automatic notifications to reinforce the sample’s use of the data collection platform or system. This method of notifications was also implemented by the team of Denis et al. [53] in order to create a more efficient case detection and referral system.
As for the professional branch, the increasingly common use of tele-intervention generates controversy on certain occasions. It is conceivable that professionals should have prior specialized training in order to be able to carry out interventions correctly. For example, McCarthy et al. [20] provided continued training in tele-intervention to professionals, adapting it to their needs and following their own protocol created years ago [76], without finding significant differences with respect to face-to-face work. In this case, it was an intervention based on the family-centered model. For their part, Popova et al. [21] advocate for future research to provide training opportunities, specifically to foster communication with families.
3.1.5. Tele-Intervention as a Possible Solution to Contextual Barriers
The use of tele-intervention has demonstrated benefits not only in purely interventional values, but there is also documentation that reflects a more logistical nature. Its application has been implemented in more remote settings or those with fewer resources as a possible solution to continuous transfers to referral health centers, usually located in urban centers. In this systematic review, 3 studies were conducted in rural or developing settings: 2 in different parts of Africa; Ghana and South Africa and 1 in China.
Both the study by du Plessis et al. and Ameyaw et al. [52,67] focused on the detection and diagnosis of deafness or hearing loss. The first study involved the establishment of an interregional network with the ultimate aim of conducting a comparative analysis between two hearing screening techniques, carrying it out remotely and face to face. The results obtained showed high rates of efficiency in terms of the time factor. Thus, families did not have to make such a long journey, which resulted in savings in time and money. The second study, focused on health professionals, discusses the use of tele-intervention as a support for the knowledge and perception of children’s hearing health, which will lead to a scalable and low-cost intervention in the prevention of childhood hearing loss or deafness. In the study by Li et al. [69], although adherence to the monitoring program was not adequate, resulting in lower response levels than the face-to-face method, the cost was lower.
4. Discussion
This systematic review aimed to describe the nature of the family-centered model and tele-intervention methodology in early childhood intervention, specifically in the 0–6 age group. At this stage, there are important developmental changes [77,78]. The maturational development of the child consists of a series of pre-established developmental patterns that are a consequence of the relationship between intrinsic factors, linked to genetics, and extrinsic factors, linked to the context and environment surrounding the child [1,3,37,79]. This process can be explained through the comprehensive model of functioning, disability and health [7,37], which is defined by three fundamental axes: bodily functions and structures, activity and participation, depending on the health condition. When there is any kind of difficulty in any of the three axes, this is known as impairment, limitation or restriction, respectively. In the event that the triad of factors is altered in its totality, this is when we will speak of disability [7,37].
If this situation occurs, the child population has care services made up of a team of experts in the pediatric area who will be in charge of providing care to those children who are at risk or who suffer from some type of affectation that restricts their capacity for participation and occupational performance, negatively affecting their quality of life [80]. The intervention of these teams can be based on different models that define the clinical practice. In the case of the family-centered model of care, its principles [22,25] facilitate the establishment and maintenance of the therapeutic bond, which enables both families and children attending the service to have positive feelings throughout the intervention process [21,41,42,44,55,59,64,65]. The inclusion of the family as an active agent in the process is the fundamental principle that relates to the intentional relationship model where the interpersonal dynamics or the interaction between the practitioner–family–child triad has the power to enable or inhibit that active participation during the process [21,55]. This is different from other models of care such as the person-centered model [81] or the system-centered model [82], where interaction with the family is merely relational [47].
The authors agree that the perception of the service is conditioned by the quality of the therapeutic relationship. When the practitioner takes into account the values, beliefs and needs of the family [43], as well as their demands and concerns [42] when agreeing on intervention goals, and provides a safe environment where support and guidance is offered [52,59,70], satisfaction, confidence, the sense of competence and empowerment increase [41,44,45,46,64]. These variables are related to the family quality of life, which is considered the ultimate goal of early intervention [59], being important predictors of service quality and social validity [42]. Likewise, the role of practitioners is of vital importance; the scientific literature points to the need for specialized training to improve skills and the development of interdisciplinary competencies for the proper functioning of early intervention services [21].
In recent years, the scientific literature has undergone a process of reorientation and paradigm shift [82], which has entailed a change in the modality of care. These changes imply a profound transformation at the organization level of professional roles and the functioning of the system [81,83,84]. A key example in 2020 was the introduction of tele-intervention on a massive scale, as a solution to the health emergency in the wake of COVID-19, which has been implemented in the field of Early Intervention using different strategies. In the study by Cason et al. [71], they highlight the incorporation of tele-intervention tools in a variety of care programs in the different states through the development of new education and research policies, and the development of secure applications, which are important for improving the quality of care services.
One of the strategic axes is related to prevention and diagnosis, where the aim is to provide quality information and raise awareness among the population to maintain a healthy lifestyle. Rose et al., Helle et al. and Pearson et al. [49,66,68] focus their research on the promotion of healthy eating habits, where they use tele-intervention methodology to transfer information of this nature. Along the same lines, studies more focused on early detection have implemented this technology to collect information based on developmental milestones or standard values of typical development. Thus, in the case of detecting any kind of deviation, this entails notifying the primary caregiver [50,53,67] and suggesting that they request an appointment with their referral center [50,53], enabling them to address it early.
Another axis is the intervention itself, where tele-intervention has been applied in different population groups and with different intervention techniques. The studies by Kronberg et al., Qu et al. and Staiano et al. [45,57,63] base their approach on the coaching technique, showing a good acceptance by families and effectiveness in terms of achieving goals and milestones. This technique is related to the facilitation of a safe environment in which support and guidance are provided [52,59,70] based on active listening and a tandem between the family and the practitioner. On the other hand, Blaiser et al. [70] and du Plessis et al. [52] focus their studies on the deaf and hard-of-hearing population, obtaining positive results in children’s language skills. Landolfi et al. [51] base their study on professional training, establishing a relationship between the level of specialization and the quality of support in interventions with hearing-impaired children. This study is related to the one by Popova et al. [21], which establishes knowing how to communicate as part of the specialization process in the family-centered model, and to that by Cheung et al. [54], which states that it is necessary for practitioners to strengthen their knowledge and skills to collaborate with families and to educate them during sessions.
Likewise, although there is a preference towards the family-centered model, in practice [60], there are barriers or impediments that make its implementation difficult [60,62,70]. In the case of rural areas or developing countries, the population faces unique challenges [85] where tele-intervention seems to promote solutions in terms of providing opportunities [52,67,69].
5. Conclusions
The most current literature available alludes to the family-centered model as a purely ecological and transactional paradigm, where active work with the family core is the fundamental pillar when intervening with a child. The ultimate goal of such intervention is to enhance the quality of family life. On the other hand, tele-intervention offers the possibility of being implemented in all phases of the early childhood care process: prevention, diagnosis, and intervention, regardless of the context in which they are established. This allows for an increase in service quality, especially in rural areas that are distant from urban centers.
5.1. Limitations of the Study
It should be noted that there are some limitations within this systematic review. Firstly, the use of only three databases could have affected the findings, indirectly excluding some publications that could have been of interest. However, it was decided to select the most relevant databases in the field of study. Secondly, the scope of the review included only articles published in English and Spanish, which may have excluded studies that could have been analyzed in other languages. In addition, studies were included in a time range from 2012 to 2023 in order to show evidence from the last decade, although some studies may have been excluded if they were published previously. Finally, there is a lack of agreement in the literature for the use of terminology that was key in the search for “tele-intervention”, with a large number of expressions to refer to it, and some studies may have been excluded because they did not include the key word. In addition, a meta-analysis study would complete this research to determine with statistical tools the level of evidence of these two types of interventions. It would also allow comparison with other Early Intervention models or analyze potential moderators of the effect of the interventions.
5.2. Implications for the Practice and Future Lines of Research
The findings obtained in this systematic review could support the implementation of the family-centered model in early childhood intervention services, advocating for effective communication between the practitioner and the family, and the creation of a strong therapeutic bond that facilitates the management of the child to achieve goals in the natural environment. Along this line, further exploration of the development, maintenance and implementation of tele-intervention in different contexts and settings is needed. Also, due to the importance of the rurality factor, it would be appropriate to analyze those rural areas or developing countries where socio-economic and socio-demographic variables may have a negative impact on the implementation of certain methodologies. A comprehensive approach to Early Intervention has also been addressed, but future research could also focus on studying both types of intervention in populations with specific diagnoses. The ultimate aim is to improve services by providing the necessary training to practitioners and support to families and children, from a preventive and intervention point of view.
Finally, the development of new assessment tools validated within the context of tele-intervention could be fertile ground for the development and implementation of regulatory policies that benefit the early childhood intervention community.
Author Contributions
Conceptualization, Y.C.-S., A.F.-M., S.M.-E. and J.A.L.; methodology, Y.C.-S., S.M.-E. and J.A.L.; software, Y.C.-S.; formal analysis, E.J.-A., Y.C.-S. and J.A.L.; data curation, Y.C.-S., S.M.-E. and J.A.L.; writing—original draft preparation, Y.C.-S., A.F.-M. and J.A.L.; writing—review and editing, E.J.-A.,Y.C.-S., A.F.-M., S.M.-E., S.R.-M. and J.A.L.; supervision, E.J.-A., S.M.-E., S.R.-M., J.A.L. and J.A.P.-S.; project administration, J.A.L. and J.A.P.-S.; funding acquisition, J.A.P.-S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Government of the Principality of Asturias (Consejería de Derechos Sociales y Bienestar Principality of Asturias). Project “INYPEMA Living Lab”; Recovery, Transformation and Resilience Plan (Government of Spain); Netxt-Generation EU.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained within the article. No additional data are available.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Table A1.
First search phase: early intervention and the family-centered model.
Table A1.
First search phase: early intervention and the family-centered model.
| Web Of Science | TI = (Early Intervention OR Educational Early OR Early Intervention (Education) OR Intervention, Early (Education) OR Early Intervention, Education OR Education Early Intervention OR Intervention, Education Early OR Early Intervention Education OR Education, Early Intervention OR Intervention Education, Early OR Head Start Program* OR Program, Head Start) NOT TS = (Adult*) AND TS = (Child* OR Infant* OR Toddler* OR Preschool*) AND TI = (Family centered program* OR Family-Centered care* OR Family Centered Early Intervention*) |
| PubMed | (“Early Intervention” OR “Educational Early” OR “Early Intervention (Education)” OR “Intervention, Early (Education)” OR “Early Intervention, Education” OR “Education Early Intervention” OR “Intervention, Education Early” OR “Early Intervention Education” OR “Education, Early Intervention” OR “Intervention Education, Early” OR “Head Start Program” OR “Head Start Programs” OR “Program, Head Start” [Title]) AND (“Child*” OR “Infant*” OR “Toddler*” OR “Preschool*” [Title/Abstract]) NOT (“Adult*” [Title/Abstract]) AND (“Family centered program*” OR “Family-Centered care*” OR “Family Centered Early Intervention*” [Title]) |
| Scopus | TITLE (“Early Intervention” OR “Educational Early” OR “Early Intervention (Education)” OR “Intervention, Early (Education)” OR “Early Intervention, Education” OR “Education Early Intervention” OR “Intervention, Education Early” OR “Early Intervention Education” OR “Education, Early Intervention” OR “Intervention Education, Early” OR “Head Start Program*” OR “Program, Head Start”) not TITLE-ABS-KEY ( adult*) AND TITLE-ABS-KEY ( “Child*” OR “Infant*” OR “Toddler*” OR “Preschool*”) AND TITLE (“Family centered program*” OR “Family-Centered care*” OR “Family Centered Early Intervention*”) |
Table A2.
Second search phase: early intervention and tele-intervention.
Table A2.
Second search phase: early intervention and tele-intervention.
| Web Of Science | TI = (Telehealth OR Telemedicine OR Telerehabilitation* OR mHealth OR Tele-rehabilitation* OR Remote Rehabilitation* OR Rehabilitation*, Remote OR Virtual Rehabilitation* OR Rehabilitation*, Virtual OR Tele-Referral* OR Tele Referral* OR Virtual Medicine OR Medicine, Virtual OR Tele-Intensive Care OR Tele Intensive Care OR Tele-ICU OR Tele ICU OR Mobile Health OR Health, Mobile OR mHealth OR Telehealth OR eHealth) AND TI = (Early Intervention OR Educational Early OR Early Intervention (Education) OR Intervention, Early (Education) OR Early Intervention, Education OR Education Early Intervention OR Intervention, Education Early OR Early Intervention Education OR Education, Early Intervention OR Intervention Education, Early OR Head Start Program OR Head Start Programs OR Program, Head Start) NOT TS = (Adult*) AND TS= (Child* AND Infant*) |
| PubMed | (“Telehealth” OR “Telemedicine” OR “Telerehabilitation*” OR “mHealth” OR “Tele-rehabilitation*” OR “Remote Rehabilitation*” OR “Rehabilitation*, Remote” OR “Virtual Rehabilitation*” OR “Rehabilitation*, Virtual” OR “Tele-Referral*” OR “Tele Referral*” OR “Virtual Medicine” OR “Medicine, Virtual” OR “Tele-Intensive Care” OR “Tele Intensive Care” OR “Tele-ICU” OR “Tele ICU” OR “Mobile Health” OR “Health, Mobile” OR “mHealth” OR “Telehealth” OR “eHealth” [Title]) AND (“Early Intervention” OR “Educational Early” OR “Early Intervention (Education)” OR “Intervention, Early (Education)” OR “Early Intervention, Education” OR “Education Early Intervention” OR “Intervention, Education Early” OR “Early Intervention Education” OR “Education, Early Intervention” OR “Intervention Education, Early” OR “Head Start Program” OR “Head Start Programs” OR “Program, Head Start” [Title]) AND (“Child*” [Title/Abstract]) AND (“Infant*” [Title/Abstract]) NOT (“Adult*” [Title/Abstract]) |
| Scopus | TITLE(“Telehealth” OR “Telemedicine” OR “Telerehabilitation*” OR “mHealth” OR “Tele-rehabilitation*” OR “Remote Rehabilitation*” OR “Rehabilitation*, Remote” OR “Virtual Rehabilitation*” OR “Rehabilitation*, Virtual” OR “Tele-Referral*” OR “Tele Referral*” OR “Virtual Medicine” OR “Medicine, Virtual” OR “Tele-Intensive Care” OR “Tele Intensive Care” OR “Tele-ICU” OR “Tele ICU” OR “Mobile Health” OR “Health, Mobile” OR “mHealth” OR “Telehealth” OR “eHealth”) AND TITLE (“Early Intervention” OR “Educational Early” OR “Early Intervention (Education)” OR “Intervention, Early (Education)” OR “Early Intervention, Education” OR “Education Early Intervention” OR “Intervention, Education Early” OR “Early Intervention Education” OR “Education, Early Intervention” OR “Intervention Education, Early” OR “Head Start Program” OR “Head Start Programs” OR “Program, Head Start”) AND TITLE (“Child*” OR “Infant*” OR “Toddler*” OR “Preschool*”) |
References
- Cruz-Hernández, J.M.; García, J.J.; Martínez, O.C.; Raso, S.M.; Villares, J.M.M. Manual de Pediatría, 4th ed.; Ergon: Madrid, Spain, 2019; ISBN 978-84-17194-65-9. [Google Scholar]
- Mulligan, S. Terapia Ocupacional en Pediatria. Proceso de Evaluación; Editorial Médica Panamericana: Madrid, Spain, 2006; ISBN 978-84-7903-981-3. [Google Scholar]
- Shonkoff, J.P.; Richter, L.; Van Der Gaag, J.; Bhutta, Z.A. An Integrated Scientific Framework for Child Survival and Early Childhood Development. Pediatrics 2012, 129, e460–e472. [Google Scholar] [CrossRef] [PubMed]
- Martínez, N.B.; Delgado-Lobete, L.; Montes-Montes, R.; Ruiz-Pérez, N.; Santos-del-Riego, S. Participation in Everyday Activities of Children with and without Neurodevelopmental Disorders: A Cross-Sectional Study in Spain. Children 2020, 7, 157. [Google Scholar] [CrossRef] [PubMed]
- Chien, C.-W.; Rodger, S.; Copley, J. Parent-Reported Participation in Children with Moderate-to-Severe Developmental Disabilities: Preliminary Analysis of Associated Factors Using the ICF Framework. Int. J. Disabil. Dev. Educ. 2017, 64, 483–496. [Google Scholar] [CrossRef]
- Günal, A.; Bumin, G.; Huri, M. The Effects of Motor and Cognitive Impairments on Daily Living Activities and Quality of Life in Children with Autism. J. Occup. Ther. Sch. Early Interv. 2019, 12, 444–454. [Google Scholar] [CrossRef]
- Fernández-López, J.A.; Fernández-Fidalgo, M.; Geoffrey, R.; Stucki, G.; Cieza, A. Funcionamiento y discapacidad: La Clasificación Internacional del Funcionamiento (CIF). Rev. Esp. Salud Publica 2009, 83, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Early Intervention Foundation What Is Early Intervention? Available online: https://www.eif.org.uk/why-it-matters/what-is-early-intervention/ (accessed on 13 December 2023).
- Fontil, L.; Sladeczek, I.E.; Gittens, J.; Kubishyn, N.; Habib, K. From Early Intervention to Elementary School: A Survey of Transition Support Practices for Children with Autism Spectrum Disorders. Res. Dev. Disabil. 2019, 88, 30–41. [Google Scholar] [CrossRef]
- Grajo, L.C.; Candler, C.; Sarafian, A. Interventions within the Scope of Occupational Therapy to Improve Children’s Academic Participation: A Systematic Review. Am. J. Occup. Ther. 2020, 74, 7402180030p1–7402180030p32. [Google Scholar] [CrossRef]
- West, G.; Lervåg, A.; Snowling, M.J.; Buchanan-Worster, E.; Duta, M.; Hulme, C. Early Language Intervention Improves Behavioral Adjustment in School: Evidence from a Cluster Randomized Trial. J. Sch. Psychol. 2022, 92, 334–345. [Google Scholar] [CrossRef]
- Novak, I.; Honan, I. Effectiveness of Paediatric Occupational Therapy for Children with Disabilities: A Systematic Review. Aust. Occup. Ther. J. 2019, 66, 258–273. [Google Scholar] [CrossRef]
- Daniolou, S.; Pandis, N.; Znoj, H. The Efficacy of Early Interventions for Children with Autism Spectrum Disorders: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 5100. [Google Scholar] [CrossRef]
- Raya, A.S.; Gual, E.M.; Elvira, J.A.M.; Salas, B.L.; Cívico, F.J.A. La atención temprana en los trastornos del espectro autista (TEA). Psicol. Educ. 2015, 21, 55–63. [Google Scholar] [CrossRef]
- Dew, A.; Bulkeley, K.; Veitch, C.; Bundy, A.; Gallego, G.; Lincoln, M.; Brentnall, J.; Griffiths, S. Addressing the Barriers to Accessing Therapy Services in Rural and Remote Areas. Disabil. Rehabil. 2013, 35, 1564–1570. [Google Scholar] [CrossRef] [PubMed]
- Dall’Alba, L.; Gray, M.; Williams, G.; Lowe, S. Early Intervention in Children (0–6 Years) with a Rare Developmental Disability: The Occupational Therapy Role. Hong Kong J. Occup. Ther. 2014, 24, 72–80. [Google Scholar] [CrossRef]
- Morgan, C.; Darrah, J.; Gordon, A.M.; Harbourne, R.; Spittle, A.; Johnson, R.; Fetters, L. Effectiveness of Motor Interventions in Infants with Cerebral Palsy: A Systematic Review. Dev. Med. Child. Neurol. 2016, 58, 900–909. [Google Scholar] [CrossRef]
- Retamal-Walter, F.; Waite, M.; Scarinci, N. Identifying Critical Behaviours for Building Engagement in Telepractice Early Intervention: An International e-Delphi Study. Int. J. Lang. Commun. Disord. 2022, 57, 645–659. [Google Scholar] [CrossRef]
- Del Toro Alonso, V.; Moreno, E.S. Introduction Family-Centered Model in Spain from a Perspective from the Life Family Quality. Rev. Educ. Inclusiva 2020, 13, 9–21. [Google Scholar]
- McCarthy, M.; Leigh, G.; Arthur-Kelly, M. Practitioners’ Self-Assessment of Family-Centered Practice in Telepractice Versus In-Person Early Intervention. J. Deaf. Stud. Deaf. Educ. 2021, 26, 46–57. [Google Scholar] [CrossRef]
- Popova, E.S.; O’Brien, J.C.; Taylor, R.R. Communicating with Intention: Therapist and Parent Perspectives on Family-Centered Care in Early Intervention. Am. J. Occup. Ther. 2022, 76, 7605205130. [Google Scholar] [CrossRef]
- Turnbull, A.P.; Summers, J.A.; Turnbull, R.; Brotherson, M.J.; Winton, P.; Roberts, R.; Snyder, P.; McWilliam, R.; Chandler, L.; Schrandt, S.; et al. Family Supports and Services in Early Intervention: A Bold Vision. J. Early Interv. 2007, 29, 187–206. [Google Scholar] [CrossRef]
- Dunst, C.J.; Espe-Sherwindt, M. Family-Centered Practices in Early Childhood Intervention. In Handbook of Early Childhood Special Education; Springer: Berlin/Heidelberg, Germany, 2016; pp. 37–55. ISBN 978-331928492-7. [Google Scholar]
- Vanderkerken, L.; Heyvaert, M.; Onghena, P.; Maes, B. Family-Centered Practices in Home-Based Support for Families with Children with an Intellectual Disability: Judgments of Parents and Professionals. J. Intellect. Disabil. 2021, 25, 331–347. [Google Scholar] [CrossRef]
- Bruder, M.B. Family-Centered Early Intervention: Clarifying Our Values for the New Millennium. Top. Early Child. Spec. Educ. 2000, 20, 105–115. [Google Scholar] [CrossRef]
- Meisels, S.J.; Atkins-Burnett, S. Assessing Intellectual and Affective Development before Age Three: A Perspective on Changing Practices. Food Nutr. Bull. 1999, 20, 23–33. [Google Scholar] [CrossRef]
- Dunst, C.; Trivette, C. Capacity-Building Family-Systems Intervention Practices. J. Fam. Soc. Work. 2009, 12, 119–143. [Google Scholar] [CrossRef]
- King, G.; Curran, C.J.; Mcpherson, A. A Four-Part Ecological Model of Community-Focused Therapeutic Recreation and Life Skills Services for Children and Youth with Disabilities. Child Care Health Dev. 2013, 39, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Melvin, K.; Meyer, C.; Scarinci, N. What Does “Engagement” Mean in Early Speech Pathology Intervention? A Qualitative Systematised Review. Disabil. Rehabil. 2020, 42, 2665–2678. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.; Plahouras, J.; Johnston, B.C.; Scaffidi, M.A.; Grover, S.C.; Walsh, C.M. Virtual Reality Simulation Training for Health Professions Trainees in Gastrointestinal Endoscopy. Cochrane Database Syst. Rev. 2018, 8, CD008237. [Google Scholar] [CrossRef]
- Tolosana, E.S.; Serrano, J.O. La Percepción Local Del Acceso a Los Servicios de Salud En Las Áreas Rurales. El Caso Del Pirineo Navarro. An. Sist. Sanit. Navar. 2021, 44, 185–194. [Google Scholar] [CrossRef]
- Rodríguez García, L.; Herrán García, I.; de La Mano Rodero, P.; Díaz Sánchez, C.; Martínez Carrillo, J. Atención temprana en tiempos de COVID-19: Investigar la/s realidad/es de la teleintervención en las prácticas centradas en la familia. Siglo Cero 2021, 1, 75–117. [Google Scholar] [CrossRef]
- Houston, K.T.; Stredler-Brown, A. A Model of Early Intervention for Children with Hearing Loss Provided through Telepractice. Volta. Rev. 2012, 112, 283–296. [Google Scholar] [CrossRef]
- Medical Subject Headings (MeSH) Telemedicine 1993. Available online: https://www.ncbi.nlm.nih.gov/mesh?Db=mesh&Cmd=DetailsSearch&Term=%22Telemedicine%22%5BMeSH+Terms%5D (accessed on 9 November 2023).
- Olsen, S.; Fiechtl, B.; Rule, S. An Evaluation of Virtual Home Visits in Early Intervention: Feasibility of “Virtual Intervention”. Volta. Rev. 2012, 112, 267–281. [Google Scholar] [CrossRef]
- Page, M.; McKenzie, J.; Bossuyt, P.; Boutron, I.; Hoffmann, T.; Mulrow, C. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Organización Mundial de la Salud (OMS). Clasificación Internacional Del Funcionamiento, de la Discapacidad y de la Salud: CIF; Organización Mundial de la Salud (OMS): Geneva, Switzerland, 2001; ISBN 92-4-354542-6. [Google Scholar]
- Cohen, D.; Greenberg, J.; Stillman, D. Zotero 2006. Available online: https://www.zotero.org/download/ (accessed on 24 May 2023).
- Scottish Intercollegiate Guidelines Network. SIGN 50: A Guideline Developer’s Handbook; Scottish Intercollegiate Guidelines Network: Edinburgh, UK, 2011; ISBN 978-1-905813-25-4. [Google Scholar]
- Han, M.; Lee, E. Effectiveness of Mobile Health Application Use to Improve Health Behavior Changes: A Systematic Review of Randomized Controlled Trials. Healthc. Inform. Res. 2018, 24, 207–226. [Google Scholar] [CrossRef] [PubMed]
- Oliver, H.; Seccurro, D.; Dorich, J.; Rice, M.; Schwartz, T.; Harpster, K. “Even Though a Lot of Kids Have It, Not a Lot of People Have Knowledge of It”: A Qualitative Study Exploring the Perspectives of Parents of Children with Cerebral/Cortical Visual Impairment. Res. Dev. Disabil. 2023, 135, 104443. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Rico, G.; García-Grau, P.; Cañadas, M.; González-García, R.J. Social Validity of Telepractice in Early Intervention: Effectiveness of Family-Centered Practices. Fam. Relat. 2023, 72, 2535–2550. [Google Scholar] [CrossRef]
- van der Zee, R.B.; Dirks, E. Diversity of Child and Family Characteristics of Children with Hearing Loss in Family-Centered Early Intervention in The Netherlands. JCM 2022, 11, 2074. [Google Scholar] [CrossRef]
- Subinas-Medina, P.; Garcia-Grau, P.; Gutierrez-Ortega, M.; Leon-Estrada, I. Family-Centered Practices in Early Intervention: Family Confidence, Competence, and Quality of Life. Psychol. Soc. Educ. 2022, 14, 39–47. [Google Scholar] [CrossRef]
- Qu, L.; Chen, H.; Miller, H.; Miller, A.; Colombi, C.; Chen, W.; Ulrich, D.A. Assessing the Satisfaction and Acceptability of an Online Parent Coaching Intervention: A Mixed-Methods Approach. Front. Psychol. 2022, 13, 859145. [Google Scholar] [CrossRef]
- Muthukaruppan, S.S.; Cameron, C.; Campbell, Z.; Krishna, D.; Moineddin, R.; Bharathwaj, A.; Poomariappan, B.M.; Mariappan, S.; Boychuk, N.; Ponnusamy, R.; et al. Impact of a Family-Centred Early Intervention Programme in South India on Caregivers of Children with Developmental Delays. Disabil. Rehabil. 2022, 44, 2410–2419. [Google Scholar] [CrossRef]
- Mas, J.M.; Dunst, C.J.; Hamby, D.W.; Balcells-Balcells, A.; García-Ventura, S.; Baqués, N.; Giné, C. Relationships between Family-Centred Practices and Parent Involvement in Early Childhood Intervention. Eur. J. Spec. Needs Educ. 2022, 37, 1–13. [Google Scholar] [CrossRef]
- Dirks, E.; Szarkowski, A. Family-Centered Early Intervention (FCEI) Involving Fathers and Mothers of Children Who Are Deaf or Hard of Hearing: Parental Involvement and Self-Efficacy. J. Clin. Med. 2022, 11, 492. [Google Scholar] [CrossRef]
- Pearson, N.; Finch, M.; Sutherland, R.; Kingsland, M.; Wolfenden, L.; Wedesweiler, T.; Herrmann, V.; Yoong, S.L. An mHealth Intervention to Reduce the Packing of Discretionary Foods in Children’s Lunch Boxes in Early Childhood Education and Care Services: Cluster Randomized Controlled Trial. J. Med. Internet Res. 2022, 24, e27760. [Google Scholar] [CrossRef]
- Miller, K.; Berentson, G.; Roberts, H.; McMorris, C.; Needelman, H. Examining Early Intervention Referral Patterns in Neonatal Intensive Care Unit Follow up Clinics Using Telemedicine during COVID-19. Early Hum. Dev. 2022, 172, 105631. [Google Scholar] [CrossRef] [PubMed]
- Landolfi, E.; Continisio, G.I.; Del Vecchio, V.; Serra, N.; Burattini, E.; Conson, M.; Marciano, E.; Laria, C.; Franzè, A.; Caso, A.; et al. NeonaTal Assisted TelerehAbilitation (T.A.T.A. Web App) for Hearing-Impaired Children: A Family-Centered Care Model for Early Intervention in Congenital Hearing Loss. Audiol. Res. 2022, 12, 182–190. [Google Scholar] [CrossRef] [PubMed]
- du Plessis, D.; Mahomed-Asmail, F.; le Roux, T.; Graham, M.A.; de Kock, T.; van der Linde, J.; Swanepoel, D.W. mHealth-Supported Hearing Health Training for Early Childhood Development Practitioners: An Intervention Study. Int. J. Environ. Res. Public Health 2022, 19, 14228. [Google Scholar] [CrossRef]
- Denis, F.; Maurier, L.; Carillo, K.; Ologeanu-Taddei, R.; Septans, A.-L.; Gepner, A.; Le Goff, F.; Desbois, M.; Demurger, B.; Silber, D.; et al. Early Detection of Neurodevelopmental Disorders of Toddlers and Postnatal Depression by Mobile Health App: Observational Cross-Sectional Study. JMIR Mhealth Uhealth 2022, 10, e38181. [Google Scholar] [CrossRef]
- Cheung, W.C.; Aleman-Tovar, J.; Johnston, A.N.; Little, L.M.; Burke, M.M. A Qualitative Study Exploring Parental Perceptions of Telehealth in Early Intervention. J. Dev. Phys. Disabil. 2022, 35, 353–373. [Google Scholar] [CrossRef]
- Lee, J.; Kaat, A.J.; Roberts, M.Y. Involving Caregivers of Autistic Toddlers in Early Intervention: Common Practice or Exception to the Norm? Am. J. Speech Lang. Pathol. 2022, 31, 1755–1770. [Google Scholar] [CrossRef]
- Dick, C.C.; Ibañez, L.V.; DesChamps, T.D.; Attar, S.M.; Stone, W.L. Brief Report: Perceptions of Family-Centered Care across Service Delivery Systems and Types of Caregiver Concerns about Their Toddlers’ Development. J. Autism Dev. Disord. 2022, 52, 4181–4190. [Google Scholar] [CrossRef]
- Staiano, A.E.; Newton, R.L.; Beyl, R.A.; Kracht, C.L.; Hendrick, C.A.; Viverito, M.; Webster, E.K. mHealth Intervention for Motor Skills: A Randomized Controlled Trial. Pediatrics 2022, 149, e2021053362. [Google Scholar] [CrossRef]
- Vilaseca, R.; Ferrer, F.; Rivero, M.; Bersabé, R.M. Early Intervention Services during the COVID-19 Pandemic in Spain: Toward a Model of Family-Centered Practices. Front. Psychol. 2021, 12, 738463. [Google Scholar] [CrossRef]
- Jemes-Campana, I.-C.; Romero-Galisteo, R.-P.; Galvez-Ruiz, P.; Labajos-Manzanares, M.-T.; Moreno-Morales, N. Service Quality in Early Intervention Centres: An Analysis of Its Influence on Satisfaction and Family Quality of Life. Children 2021, 8, 716. [Google Scholar] [CrossRef]
- García-Ventura, S.; Mas, J.M.; Balcells-Balcells, A.; Giné, C. Family-Centred Early Intervention: Comparing Practitioners’ Actual and Desired Practices. Child. Care Health Dev. 2021, 47, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.-H.; Liu, T.-W. Does Parental Education Level Matter? Dynamic Effect of Parents on Family-Centred Early Intervention for Children with Hearing Loss. Int. J. Disabil. Dev. Educ. 2021, 68, 457–478. [Google Scholar] [CrossRef]
- Yang, H.W.; Burke, M.; Isaacs, S.; Rios, K.; Schraml-Block, K.; Aleman-Tovar, J.; Tompkins, J.; Swartz, R. Family Perspectives toward Using Telehealth in Early Intervention. J. Dev. Phys. Disabil. 2021, 33, 197–216. [Google Scholar] [CrossRef]
- Kronberg, J.; Tierney, E.; Wallisch, A.; Little, L.M. Early Intervention Service Delivery via Telehealth During COVID-19: A Research-Practice Partnership. Int. J. Telerehabil 2021, 13, e6363. [Google Scholar] [CrossRef] [PubMed]
- Park, H.I.; Park, H.Y.; Yoo, E.; Han, A. Impact of Family-Centered Early Intervention in Infants with Autism Spectrum Disorder: A Single-Subject Design. Occup. Ther. Int. 2020, 2020, 1427169. [Google Scholar] [CrossRef]
- Hughes-Scholes, C.H.; Gavidia-Payne, S. Early Childhood Intervention Program Quality: Examining Family-Centered Practice, Parental Self-Efficacy and Child and Family Outcomes. Early Child. Educ. J. 2019, 47, 719–729. [Google Scholar] [CrossRef]
- Rose, J.; Glazebrook, C.; Wharrad, H.; Siriwardena, A.N.; Swift, J.A.; Nathan, D.; Weng, S.F.; Atkinson, P.; Ablewhite, J.; McMaster, F.; et al. Proactive Assessment of Obesity Risk during Infancy (ProAsk): A Qualitative Study of Parents’ and Professionals’ Perspectives on an mHealth Intervention. BMC Public Health 2019, 19, 294. [Google Scholar] [CrossRef]
- Ameyaw, G.A.; Ribera, J.; Anim-Sampong, S. Interregional Newborn Hearing Screening via Telehealth in Ghana. J. Am. Acad. Audiol. 2019, 30, 178–186. [Google Scholar] [CrossRef]
- Helle, C.; Hillesund, E.R.; Omholt, M.L.; Øverby, N.C. Early Food for Future Health: A Randomized Controlled Trial Evaluating the Effect of an eHealth Intervention Aiming to Promote Healthy Food Habits from Early Childhood. BMC Public Health 2017, 17, 729. [Google Scholar] [CrossRef]
- Li, Y.; Wang, W.; van Velthoven, M.H.; Chen, L.; Car, J.; Rudan, I.; Zhang, Y.; Wu, Q.; Du, X.; Scherpbier, R.W. Text Messaging Data Collection for Monitoring an Infant Feeding Intervention Program in Rural China: Feasibility Study. J. Med. Internet Res. 2013, 15, e269. [Google Scholar] [CrossRef] [PubMed]
- Blaiser, K.M.; Behl, D.; Callow-Heusser, C.; White, K.R. Measuring Costs and Outcomes of Tele-Intervention When Serving Families of Children Who Are Deaf/Hard-of-Hearing. Int. J. Telerehabil 2013, 5, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Cason, J.; Behl, D.; Ringwalt, S. Overview of States’ Use of Telehealth for the Delivery of Early Intervention (IDEA Part C) Services. Int. J. Telerehabil 2012, 4, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Schertz, H.H.; Horn, K. Facilitating Toddlers’ Social Communication from within the Parent-Child Relationship: Application of Family-Centered Early Intervention and Mediated Learning Principles. In Handbook of Parent-Implemented Interventions for Very Young Children with Autism; Siller, M., Morgan, L., Eds.; Springer: Berlin/Heidelberg, Germany, 2018; pp. 141–154. ISBN 978-3-319-90994-3. [Google Scholar]
- Badawy, S.M.; Radovic, A. Digital Approaches to Remote Pediatric Health Care Delivery during the COVID-19 Pandemic: Existing Evidence and a Call for Further Research. JMIR Pediatr. Parent. 2020, 3, e20049. [Google Scholar] [CrossRef] [PubMed]
- To, W.-M.; Lee, P.K.C. mHealth and COVID-19: A Bibliometric Study. Healthcare 2023, 11, 1163. [Google Scholar] [CrossRef] [PubMed]
- Giansanti, D. The Role of the mHealth in the Fight against the COVID-19: Successes and Failures. Healthcare 2021, 9, 58. [Google Scholar] [CrossRef]
- McCarthy, M. The RIDBC Telepractice Training Protocol: A Model for Meeting ASHA Roles and Responsibilities. Perspect. Telepractice 2013, 3, 49–60. [Google Scholar] [CrossRef]
- Majnemer, A. Benefits of Early Intervention for Children with Developmental Disabilities. Semin. Pediatr. Neurol. 1998, 5, 62–69. [Google Scholar] [CrossRef]
- Papalia, D.; Feldman, R.; Martorell, G. Desarrollo Humano; McGraw-Hill: New York, NY, USA, 2013; ISBN 978-607-15-0933-8. [Google Scholar]
- Shonkoff, J.P. Building a New Biodevelopmental Framework to Guide the Future of Early Childhood Policy. Child. Dev. 2010, 81, 357–367. [Google Scholar] [CrossRef]
- Federación Estatal de Asociaciones de Profesionales de Atención Temprana. Libro Blanco de La Atención Temprana; Real Patronato de Discapacidad: Madrid, Spain, 2003. [Google Scholar]
- Collins, J. The Person-Centered Way: Revolutionizing Quality of Life in Long-Term Care; BookSurge Publishing: South Carolina, SC, USA, 2010; ISBN 978-1-4392-4614-6. [Google Scholar]
- Martínez, T. La Atención Centrada en la Persona en Los Servicios Gerontológicos: Modelos de Atención e Instrumentos de Evaluación; Universidad de Oviedo: Oviedo, Spain, 2015. [Google Scholar]
- García-Sánchez, F.A.; Escorcia, C.T.; Sánchez-López, M.C.; Orcajada, N.; Hernández-Pérez, E. Atención Temprana Centrada En La Familia. Siglo Cero 2014, 45, 6–27. [Google Scholar]
- Gine, C.; Gracia, M.; Velaseca, R.; Garcia-Die, M.T. Rethinking Early Childhood Intervention: Proposals for Future Development. Infanc. Y Aprendiz. 2006, 29, 297–313. [Google Scholar] [CrossRef]
- European Commision. The Impact of Demographic Change in a Changing Environment; European Commission: Brussels, Belgium, 2023. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).