
The Effect of Employee-Oriented Flexible Work on Mental Health: A Systematic Review

 ,
,  ,
,
Abstract
:1. Introduction
2. Methods
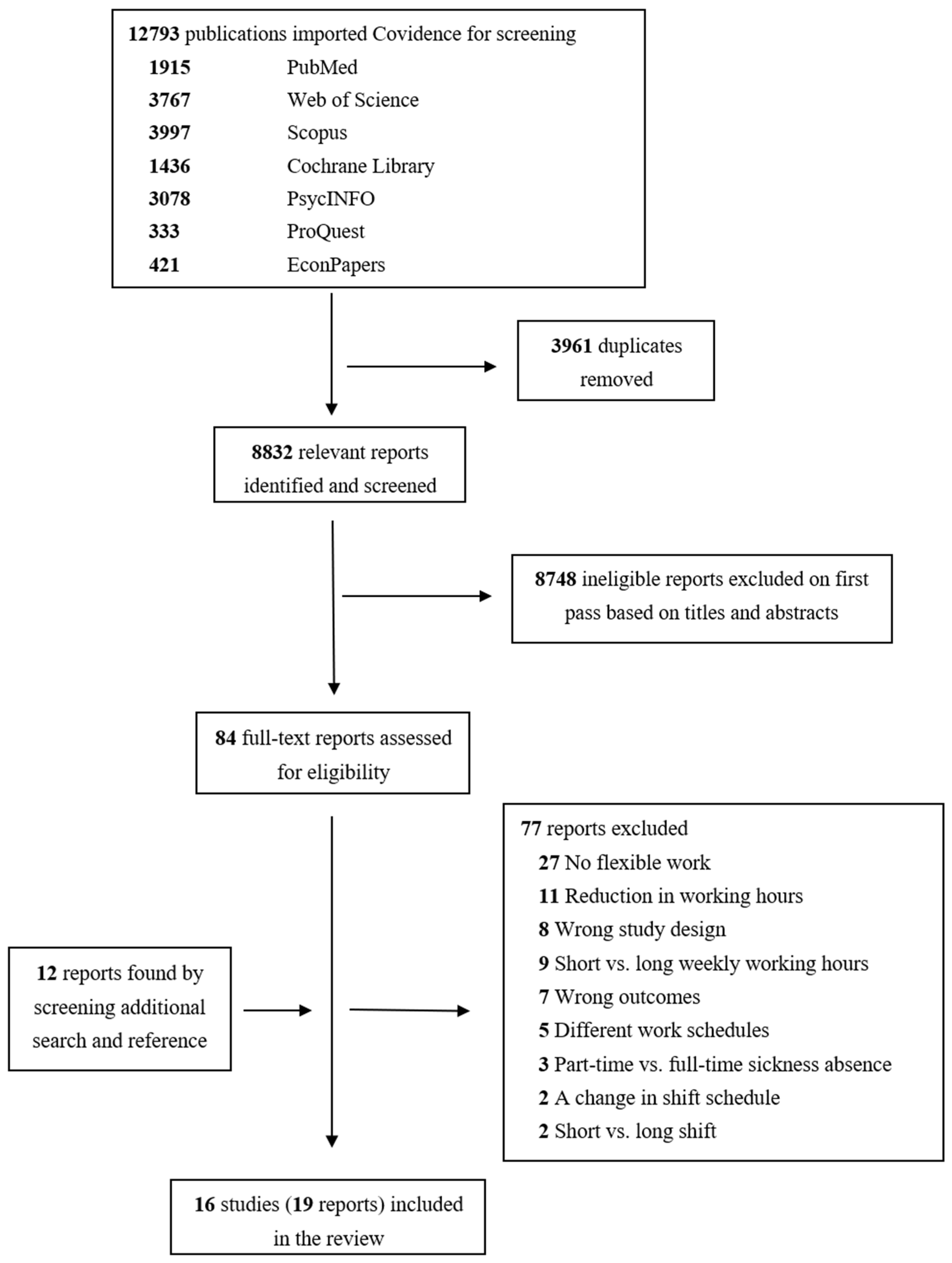
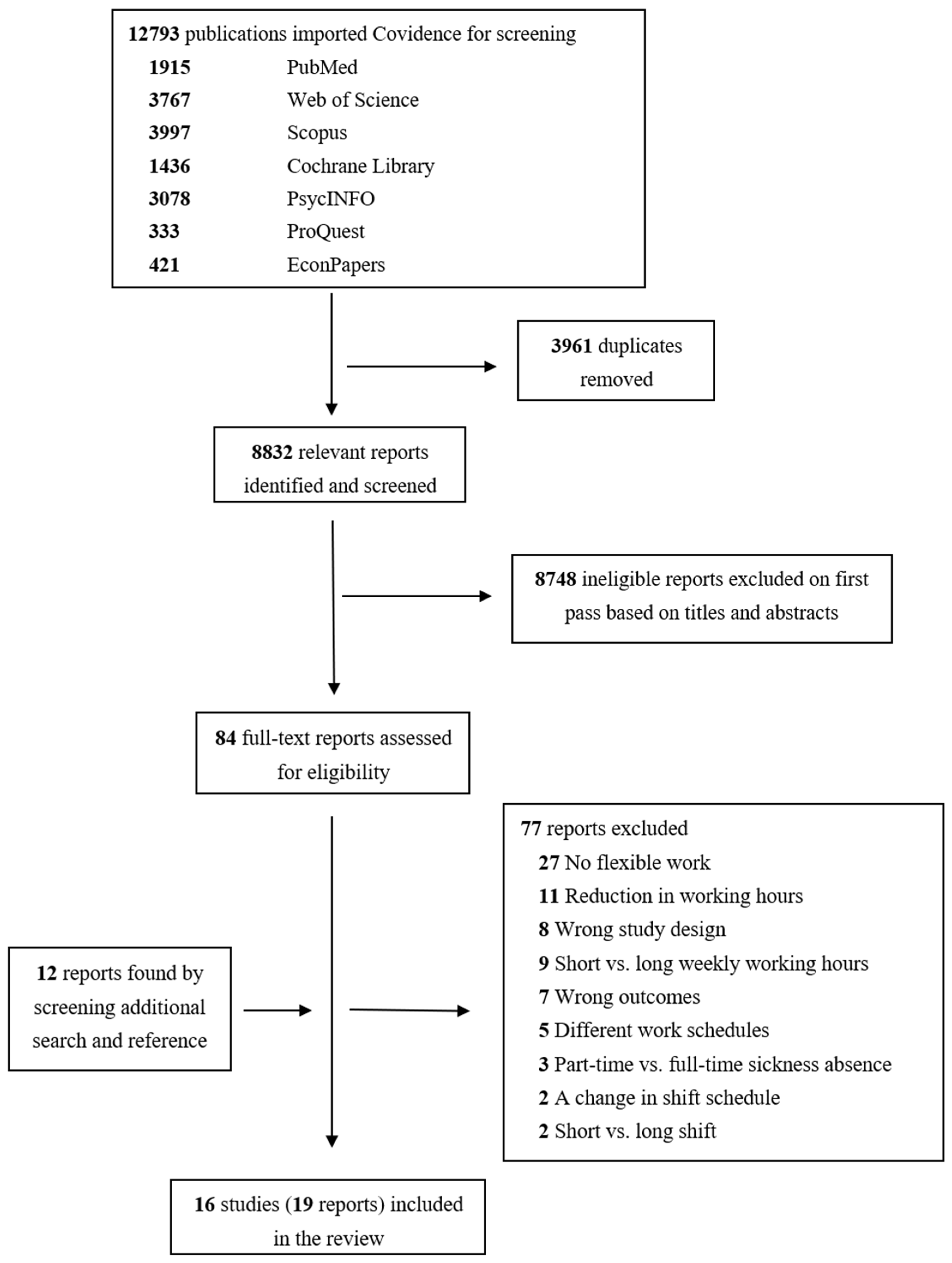
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Quality Assessment
2.4. Data Synthesis
3. Results
3.1. Worktime Control
3.2. Working from Home/Teleworking
3.3. Flexible Working Arrangements
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Ethics Approval
Conflicts of Interest
References
- Bouziri, H.; Smith, D.R.M.; Descatha, A.; Dab, W.; Jean, K. Working from home in the time of COVID-19: How to best preserve occupational health? Occup. Environ. Med. 2020, 77, 509–510. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, R.; Dellve, L.; Halleröd, B. Work despite poor health? A 14-year follow-up of how individual work accommodations are extending the time to retirement for workers with poor health conditions. SSM Popul. Health 2019, 9, 100514. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, R.; Hasselgren, C.; Dellve, L.; Seldén, D.; Larsson, D.; Stattin, M. Matching the Pieces: The Presence of Idiosyncratic Deals and Their Impact on Retirement Preferences Among Older Workers. Work Aging Retire. 2021, 7, 240–255. [Google Scholar] [CrossRef]
- Higgins, C.; Duxbury, L.; Julien, M. The relationship between work arrangements and work-family conflict. Work 2014, 48, 69–81. [Google Scholar] [CrossRef]
- Engelen, L.; Chau, J.; Young, S.; Mackey, M.; Jeyapalan, D.; Bauman, A. Is activity-based working impacting health, work performance and perceptions? A systematic review. Build. Res. Inf. 2019, 47, 468–479. [Google Scholar] [CrossRef]
- Jeffrey Hill, E.; Grzywacz, J.G.; Allen, S.; Blanchard, V.L.; Matz-Costa, C.; Shulkin, S.; Pitt-Catsouphes, M. Defining and conceptualizing workplace flexibility. Community Work Fam. 2008, 11, 149–163. [Google Scholar] [CrossRef]
- Beckers, D.G.; Kompier, M.A.; Kecklund, G.; Härmä, M. Worktime control: Theoretical conceptualization, current empirical knowledge, and research agenda. Scand. J. Work Environ. Health 2012, 291–297. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, M.; Iwasaki, K.; Sasaki, T.; Kubo, T.; Mori, I.; Otsuka, Y. Worktime control-dependent reductions in fatigue, sleep problems, and depression. Appl. Ergon. 2011, 42, 244–250. [Google Scholar] [CrossRef]
- Costa, G.; Akerstedt, T.; Nachreiner, F.; Baltieri, F.; Carvalhais, J.; Folkard, S.; Dresen, M.F.; Gadbois, C.; Gartner, J.; Sukalo, H.G.; et al. Flexible working hours, health, and well-being in Europe: Some considerations from a SALTSA project. Chronobiol. Int. 2004, 21, 831–844. [Google Scholar] [CrossRef]
- Costa, G.; Sartori, S.; Akerstedt, T. Influence of flexibility and variability of working hours on health and well-being. Chronobiol. Int. 2006, 23, 1125–1137. [Google Scholar] [CrossRef]
- Blomgren, J.; Perhoniemi, R. Increase in sickness absence due to mental disorders in Finland: Trends by gender, age and diagnostic group in 2005–2019. Scand. J. Public Health 2021, 50, 318–322. [Google Scholar] [CrossRef] [PubMed]
- Viola, S.; Moncrieff, J. Claims for sickness and disability benefits owing to mental disorders in the UK: Trends from 1995 to 2014. BJPsych Open 2016, 2, 18–24. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Health Estimates 2014. Summary Tables: YLD by cause, age and sex, by WHO Region, 2000–2012. Available online: https://www.who.int/data/global-health-estimates (accessed on 27 August 2021).
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Donaldson, S.I.; Lee, J.Y.; Donaldson, S.I. Evaluating Positive Psychology Interventions at Work: A Systematic Review and Meta-Analysis. Int. J. Appl. Posit. Psychol. 2019, 4, 113–134. [Google Scholar] [CrossRef] [Green Version]
- Mache, S.; Servaty, R.; Harth, V. Flexible work arrangements in open workspaces and relations to occupational stress, need for recovery and psychological detachment from work. J. Occup. Med. Toxicol. 2020, 15, 5. [Google Scholar] [CrossRef] [Green Version]
- Vesala, H.; Tuomivaara, S. Slowing work down by teleworking periodically in rural settings? Pers. Rev. 2015, 44, 511–528. [Google Scholar] [CrossRef]
- Moen, P.; Kelly, E.L.; Fan, W.; Lee, S.-R.; Almeida, D.; Kossek, E.E.; Buxton, O.M. Does a Flexibility/Support Organizational Initiative Improve High-Tech Employees’ Well-Being? Evidence from the Work, Family, and Health Network. Am. Sociol. Rev. 2016, 81, 134–164. [Google Scholar] [CrossRef]
- Egan, M.; Bambra, C.; Thomas, S.; Petticrew, M.; Whitehead, M.; Thomson, H. The psychosocial and health effects of workplace reorganisation. 1. A systematic review of organisational-level interventions that aim to increase employee control. J. Epidemiol. Community Health 2007, 61, 945–954. [Google Scholar] [CrossRef] [Green Version]
- Nijp, H.H.; Beckers, D.G.; Geurts, S.A.; Tucker, P.; Kompier, M.A. Systematic review on the association between employee worktime control and work–non-work balance, health and well-being, and job-related outcomes. Scand. J. Work Environ. Health 2012, 38, 299–313. [Google Scholar] [CrossRef] [Green Version]
- Joyce, K.; Pabayo, R.; Critchley, J.A.; Bambra, C. Flexible working conditions and their effects on employee health and wellbeing. Cochrane Database Syst. Rev. 2010, 2010, CD008009. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, e1003583. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.; Hernan, M.A.; Reeves, B.C.; Savovic, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Systematic reviews of etiology and risk. In Joanna Briggs Institute Reviewer’s Manual; Chapter, 7, Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2017; Available online: https://reviewersmanual.joannabriggs.org/ (accessed on 29 March 2022).
- Ding, H.; Hu, G.L.; Zheng, X.Y.; Chen, Q.; Threapleton, D.E.; Zhou, Z.H. The method quality of cross-over studies involved in Cochrane Systematic Reviews. PLoS ONE 2015, 10, e0120519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moen, P.; Kelly, E.L.; Tranby, E.; Huang, Q. Changing work, changing health: Can real work-time flexibility promote health behaviors and well-being? J. Health Soc. Behav. 2011, 52, 404–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nabe-Nielsen, K.; Garde, A.H.; Diderichsen, F. The effect of work-time influence on health and well-being: A quasi-experimental intervention study among eldercare workers. Int. Arch. Occup. Environ. Health 2011, 84, 683–695. [Google Scholar] [CrossRef]
- Albrecht, S.C.; Leineweber, C.; Ojajärvi, A.; Oksanen, T.; Kecklund, G.; Härmä, M. Association of work-time control with sickness absence due to musculoskeletal and mental disorders: An occupational cohort study. J. Occup. Health 2020, 62, e12181. [Google Scholar] [CrossRef]
- Vahtera, J.; Laine, S.; Virtanen, M.; Oksanen, T.; Koskinen, A.; Pentti, J.; Kivimaki, M. Employee control over working times and risk of cause-specific disability pension: The Finnish Public Sector Study. Occup. Environ. Med. 2010, 67, 479–485. [Google Scholar] [CrossRef]
- Ala-Mursula, L.; Vahtera, J.; Pentti, J.; Kivimaki, M. Effect of employee worktime control on health: A prospective cohort study. Occup. Environ. Med. 2004, 61, 254–261. [Google Scholar] [CrossRef] [Green Version]
- Aronsson, V.; Toivanen, S.; Leineweber, C.; Nyberg, A. Can a poor psychosocial work environment and insufficient organizational resources explain the higher risk of ill-health and sickness absence in human service occupations? Evidence from a Swedish national cohort. Scand. J. Public Health 2019, 47, 310–317. [Google Scholar] [CrossRef]
- Lee, Y.; Eissenstat, S.J. A longitudinal examination of the causes and effects of burnout based on the job demands-resources model. Int. J. Educ. Vocat. Guid. 2018, 18, 337–354. [Google Scholar] [CrossRef]
- Albrecht, S.C.; Kecklund, G.; Rajaleid, K.; Leineweber, C. The longitudinal relationship between control over working hours and depressive symptoms: Results from SLOSH, a population-based cohort study. J. Affect. Disord. 2017, 215, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, S.C.; Kecklund, G.; Leineweber, C. The mediating effect of work-life interference on the relationship between work-time control and depressive and musculoskeletal symptoms. Scand. J. Work Environ. Health 2020, 46, 469–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Windeler, J.B.; Chudoba, K.M.; Sundrup, R.Z. Getting away from them all: Managing exhaustion from social interaction with telework. J. Organiz. Behav. 2017, 38, 977–995. [Google Scholar] [CrossRef]
- Henke, R.M.; Benevent, R.; Schulte, P.; Rinehart, C.; Crighton, K.A.; Corcoran, M. The Effects of Telecommuting Intensity on Employee Health. Am. J. Health Promot. 2016, 30, 604–612. [Google Scholar] [CrossRef]
- Kubo, T.; Takahashi, M.; Liu, X.; Ikeda, H.; Togo, F.; Shimazu, A.; Tanaka, K.; Kamata, N.; Kubo, Y.; Uesugi, J. Fatigue and Sleep Among Employees with Prospective Increase in Work Time Control: A 1-Year Observational Study with Objective Assessment. J. Occup. Environ. Med. 2016, 58, 1066–1072. [Google Scholar] [CrossRef]
- Shepherd-Banigan, M.; Bell, J.F.; Basu, A.; Booth-LaForce, C.; Harris, J.R. Workplace Stress and Working from Home Influence Depressive Symptoms Among Employed Women with Young Children. Int. J. Behav. Med. 2016, 23, 102–111. [Google Scholar] [CrossRef]
- Timms, C.; Brough, P.; O’Driscoll, M.; Kalliath, T.; Siu, O.L.; Sit, C.; Lo, D. Flexible work arrangements, work engagement, turnover intentions and psychological health. Asia Pac. J. Hum. Resour. 2015, 53, 83–103. [Google Scholar] [CrossRef]
- Takahashi, M.; Iwasaki, K.; Sasaki, T.; Kubo, T.; Mori, I.; Otsuka, Y. Sleep, fatigue, recovery, and depression after change in work time control: A one-year follow-up study. J. Occup. Environ. Med. 2012, 54, 1078–1085. [Google Scholar] [CrossRef]
- Hornung, S.; Glaser, J.; Rousseau, D.M.; Angerer, P.; Weigl, M. Employee-oriented leadership and quality of working life: Mediating roles of idiosyncratic deals. Psychol. Rep. 2011, 108, 59–74. [Google Scholar] [CrossRef]
- Carlson, D.S.; Grzywacz, J.G.; Kacmar, K.M. The relationship of schedule flexibility and outcomes via the work-family interface. J. Manag. Psychol. 2010, 25, 330–355. [Google Scholar] [CrossRef]
- Leineweber, C.; Falkenberg, H.; Albrecht, S.C. Parent’s Relative Perceived Work Flexibility Compared to Their Partner Is Associated with Emotional Exhaustion. Front. Psychol. 2018, 9, 640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlson, D.S.; Grzywacz, J.G.; Ferguson, M.; Hunter, E.M.; Clinch, C.R.; Arcury, T.A. Health and turnover of working mothers after childbirth via the work-family interface: An analysis across time. J. Appl. Psychol. 2011, 96, 1045–1054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucker, P.; Albrecht, S.; Kecklund, G.; Beckers, D.G.; Leineweber, C. Work time control, sleep & accident risk: A prospective cohort study. Chronobiol. Int. 2016, 33, 619–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virtanen, M.; Ferrie, J.E.; Singh-Manoux, A.; Shipley, M.J.; Stansfeld, S.A.; Marmot, M.G.; Ahola, K.; Vahtera, J.; Kivimaki, M. Long working hours and symptoms of anxiety and depression: A 5-year follow-up of the Whitehall II study. Psychol. Med. 2011, 41, 2485–2494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiller, H.; Lekander, M.; Rajaleid, K.; Hellgren, C.; Akerstedt, T.; Barck-Holst, P.; Kecklund, G. The impact of reduced worktime on sleep and perceived stress—A group randomized intervention study using diary data. Scand. J. Work Environ. Health 2017, 43, 109–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Oliveira, T.C.; Anagnostopoulos, A. The Association Between Shift Work and Affective Disorders: A Systematic Review. Chronobiol. Int. 2021, 38, 182–200. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]

{kind=link}
| N of Studies | Study | Country | Follow-Up Time (Years) | Population | Sample | Age (Mean, Range, or %) | % of Female Sex | Exposure or Intervention | Outcome | Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Cluster randomized controlled trials | ||||||||||
| 1 | Moen 2016 [18] | USA | 1 | Employees and managers of a large firm’s IT division | 865 (436 intervention group, 429 control group) | Birth year: 1946–1980 | 37.9 | The intervention to facilitate working at home and to improve employees’ control over working time, shift scheduling, and when, where, and how to do their work. | Burnout, perceived stress, psychological distress | Among total sample, the intervention significantly decreased burnout. |
| Non-randomized controlled trials | ||||||||||
| 2 | Moen 2011 [27] | USA | 0.5 | White-collar workers of corporate headquarters of Best Buy Co., Inc. | 659 (325 intervention, 334 control) | 32 | 48.4 | The natural experiment moved employees from conventional practices to environments wherein they did not need permission to modify their work location or schedules. | Emotional exhaustion, psychological distress | Intervention did not directly change emotional exhaustion or psychological distress, but indirectly affected these outcomes by increasing schedule control and decreasing negative work-home spillover, which both improved well-being outcomes. |
| 3 | Nabe-Nielsen 2011 [28] | Denmark | 1 | Eldercare workers | 35 intervention subgroup A, 187 controls | 44 to 45 | 100 | Worktime self-scheduling via a computer program (subgroup A) | Self-reported stress | The intervention increased employee involvement in planning of their working hours but did not decrease stress. |
| Cross-over studies | ||||||||||
| 4 | Mache 2020 [16] | Germany | 1 | Full-time employees of a large technology company | 71 | 39 | 53.5 | Transition into open workspaces including flexible working arrangements | Occupational stress | Occupational stress decreased one year after flexible working arrangements. |
| 5 | Vesala 2015 [17] | Finland | 0.1 to 0.25 | A sample of knowledge workers | 39 | 44 | 50 | One week telework in the rural archipelago environment | Stress, emotional exhaustion, and work engagement | Stress reduced during the telework period and did not reach the original level after experiment. Emotional exhaustion reduced during telework but returned to the original level after experiment. Telework had no effect on work engagement. |
| Prospective cohort studies | ||||||||||
| 6 | Albrecht 2020a [29] | Finland | 7 | Full-time employees of public sector | 22599 | 39% were ≥50 years | 75 | Worktime control | Sickness absence due to depression or anxiety | Control over daily hours and control over time off were not associated with sickness absence due to depression or anxiety. |
| 6 | Vahtera 2010 [30] | Finland | 4.4 | Employees of public sector | 30700 | 44.8 | 77.5 | Worktime control | Disability pension due to mental disorders | Self-assessed, but not co-worker assessed worktime control was associated with lower risk of disability pension among women. |
| 6 | Ala-Mursula 2004 [31] | Finland | 3 | Permanent full-time employees of public sector | 4218 | Men 46, women 45 | 78.6 | Worktime control | Psychological distress | Low worktime control was related to high psychological distress in women. |
| 7 | Aronsson 2019 [32] | Sweden | 2 | General working population who worked at least 30% full-time | 4408 | 51 | 58 | Worktime control | Burnout | Population attributable fraction of burnout for low worktime control was 5% for human service occupations and 7% for other occupations. |
| 8 | Lee 2018 [33] | USA | 1.5 | Employees from 26 different technology offices | 507 | Not reported | 45 | Control over working hours/schedule | Burnout | A positive correlation between low control over working hours and burnout. |
| 9 | Albrecht 2017 [34] | Sweden | 6 | General working population | 2722 | 47 | 58.6 | Worktime control | Depressive symptoms | Low control over daily hours and low control over time off were associated with higher subsequent depressive symptoms. |
| 9 | Albrecht 2020b [35] | Sweden | 6 | General working population | 26804 | 49 | 55.4 | Worktime control | Depressive symptoms | Work-life imbalance partially mediated the relationship between worktime control and depressive symptoms. |
| 10 | Windeler 2017 [36] | USA | 0.3 | Employees of the IT business unit of a financial services firm | 51 | 43 | 39 | Teleworking for 1–2 days per week | Work exhaustion | Work exhaustion increased as interpersonal interaction increased. Part-time telework reduced the effect of interpersonal interaction on work exhaustion. |
| 11 | Henke 2016 [37] | USA | 2 | Active prudential financial employees | 3703 | 88% were <55 years | 62 | Prime time telecommuters, off-hour telecommuters | Depression, stress | A U-shaped or J-shaped association between the number of hours worked from home per month and depression. No association with stress. |
| 12 | Kubo 2016 [38] | Japan | 1 | Employees of a manufacturing industry and a research institute | 37 | 41.9 | 23 | Worktime control | Subjectively assessed accumulated fatigue and objectively measured fatigue | Increase in worktime control during one-year follow-up was not associated with accumulated fatigue but had positive effect on objectively measured fatigue. |
| 13 | Shepherd-Banigan 2016 [39] | USA | 2 | Working women who returned to work within six months after childbirth | 570 | 29.6 | 100 | Schedule flexibility, working from home | Depressive symptoms | Working from home reduced depressive symptoms, but schedule flexibility and number of hours worked from home were not associated with changes in depressive symptoms. |
| 14 | Timms 2015 [40] | Australia | 1 | Employees representing education, banking, and public/community services | 823 | 43 | 72 | Flexible working arrangements | Psychological strain work engagement | Use of flexible work arrangement was associated with lower work engagement and higher psychological strain. |
| 15 | Takahashi 2012 [41] | Japan | 1.3 | Daytime managers, professionals, and clerical, sales or transportation workers | 2382 | 40.6 | 34.8 | Worktime control | Fatigue, depressive symptoms | High worktime control was related to lower levels of fatigue and depressive symptoms. |
| 16 | Hornung 2011 [42] | Germany | 1 | Medical doctors | 91 | 39.4 | 47 | Flexibility idiosyncratic deals: (1) working time flexibility, (2) work schedule flexibility, and (3) influence over working hours. | Work-family conflict, work-related well-being (work engagement). | Idiosyncratic deals related were not associated with work-family conflict or with work engagement. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shiri, R.; Turunen, J.; Kausto, J.; Leino-Arjas, P.; Varje, P.; Väänänen, A.; Ervasti, J. The Effect of Employee-Oriented Flexible Work on Mental Health: A Systematic Review. Healthcare 2022, 10, 883. https://doi.org/10.3390/healthcare10050883
Shiri R, Turunen J, Kausto J, Leino-Arjas P, Varje P, Väänänen A, Ervasti J. The Effect of Employee-Oriented Flexible Work on Mental Health: A Systematic Review. Healthcare. 2022; 10(5):883. https://doi.org/10.3390/healthcare10050883
Chicago/Turabian StyleShiri, Rahman, Jarno Turunen, Johanna Kausto, Päivi Leino-Arjas, Pekka Varje, Ari Väänänen, and Jenni Ervasti. 2022. "The Effect of Employee-Oriented Flexible Work on Mental Health: A Systematic Review" Healthcare 10, no. 5: 883. https://doi.org/10.3390/healthcare10050883
APA StyleShiri, R., Turunen, J., Kausto, J., Leino-Arjas, P., Varje, P., Väänänen, A., & Ervasti, J. (2022). The Effect of Employee-Oriented Flexible Work on Mental Health: A Systematic Review. Healthcare, 10(5), 883. https://doi.org/10.3390/healthcare10050883