Abstract
The objective of this study was to determine the strengths and limitations of using structured electronic health records (EHR) to identify and manage cardiometabolic (CM) health gaps. We used medication adherence measures derived from dispense data to attribute related therapeutic care gaps (i.e., no action to close health gaps) to patient- (i.e., failure to retrieve medication or low adherence) or clinician-related (i.e., failure to initiate/titrate medication) behavior. We illustrated how such data can be used to manage health and care gaps for blood pressure (BP), low-density lipoprotein cholesterol (LDL-C), and HbA1c for 240,582 Sutter Health primary care patients. Prevalence of health gaps was 44% for patients with hypertension, 33% with hyperlipidemia, and 57% with diabetes. Failure to retrieve medication was common; this patient-related care gap was highly associated with health gaps (odds ratios (OR): 1.23–1.76). Clinician-related therapeutic care gaps were common (16% for hypertension, and 40% and 27% for hyperlipidemia and diabetes, respectively), and strongly related to health gaps for hyperlipidemia (OR = 5.8; 95% CI: 5.6–6.0) and diabetes (OR = 5.7; 95% CI: 5.4–6.0). Additionally, a substantial minority of care gaps (9% to 21%) were uncertain, meaning we lacked evidence to attribute the gap to either patients or clinicians, hindering efforts to close the gaps.
1. Introduction
Cardiometabolic (CM) health is a dominant focus of secondary prevention management in primary care [1,2] The persistence of elevated CM clinical measures (e.g., elevated blood pressure, HbA1c, or low-density lipoprotein cholesterol (LDL-C)), denoted as health gaps, and related risk mediators substantially increase the risk of preventable morbidity and mortality [3,4,5,6,7]. Typically, a health gap is defined as a clinical parameter that is outside of the optimal range as defined by clinical practice guidelines (CPG). Separately, care gaps are defined as present if an action is not taken to close the health gap. Care gaps can span a range of issues. This study focused on therapeutic care gaps that are related to medication orders and adherence (referred to herein as “care gaps”). Physicians and patients can each contribute to the existence of therapeutic care gaps [8,9], e.g., when a clinician or care team member fails to prescribe CPG-recommended treatments (e.g., lab order or medication prescription) to close a health gap, or when a patient is prescribed but does not retrieve a medication intended to close a health gap. Relatively little is known about the extent to which health gaps are attributed to patient- or to provider-related care gaps.
Structured electronic health record (EHR) data are particularly well-suited to identify CM health gaps for control of blood pressure (BP), lipids, and hemoglobin A1c and can be used to facilitate individual- and population-level care. Automated algorithms can be used to extract clinical practice guideline-based outcomes, whether a patient has a health gap, and possible causes of the health gap(s) [10].
Surveillance without more specific actions to close CM health gaps does not necessarily translate to better health outcomes [11,12]. The ability to close health gaps is mediated, in part, by clinical-level (e.g., knowledge, communication, familiarity of guidelines) and patient-level factors (e.g., environment, health behaviors, genetics, etc.). However, the interactions that can occur among these factors can make it difficult to decide if an action is required for the patient, the physician, or both, which can result in delayed medication intensification or persistent clinical inertia and health gaps [13,14,15,16]. EHR structured data may often be sufficient to know if an intervention is needed but may also be lacking sufficient information to reveal what specific actions could be taken to improve patient-level outcomes. As medication dispense data are now more readily available in EHRs, it is possible to track if a patient retrieved their medication and to derive a medication adherence measure. However, little is known about the extent to which medication adherence data and use of other structured data can help to improve patient outcomes.
The objective of this study was to determine the extent to which structured EHR data can be used to readily identify health and therapeutic care gaps for CM patients. In particular, we selected medication adherence as a disease modifier to help understand if structured EHR data can provide insight into whether the underlying care gap is attributable to the physician or to the patient, as this attribution provides a basis for acting to close the gap.
2. Materials and Methods
2.1. Study Design and Population
In this retrospective analysis, a 2-year look-back period (i.e., 1 October 2013–30 September 2015) was used to define eligibility as a primary care patient. A subsequent 2-year period (1 October 2015–30 September 2017), denoted as the “Health Gap and Therapeutic Care Gap Assessment Period”, was used to identify health gaps and medication adherence status. Care gaps were assessed using structured data (e.g., diagnosis, medication order, laboratory results, etc.) in the 6-month period following identification of a health gap (Figure 1).
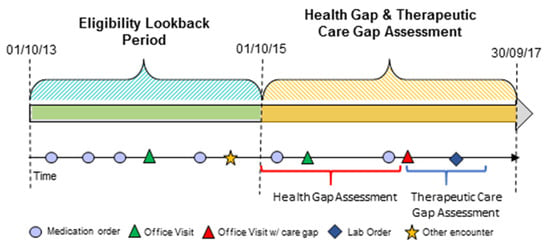
Figure 1.
Retrospective use of EHR data to identify eligible primary care patients, as well as health and care gaps.
The study was conducted at Sutter Health, a large not-for-profit health system in Northern California comprising 24 hospitals, 272 outpatient primary care practices, and approximately 1656 primary care physicians (PCPs), excluding pediatricians. We confined analyses to patients who had a Sutter primary care provider (PCP) and met the following eligibility criteria: (1) During a two-year look-back period (i.e., 1 October 2013–30 September 2015) they (i) had at least two clinical encounters with a Sutter PCP and (ii) met diagnostic criteria for hypertension, hyperlipidemia, or diabetes (details in Appendix A File 1). (2) During the health gap and care gap assessment period (i.e., 1 October 2015–30 September 2017) patients had (i) at least one CM-related clinical measure and one clinical encounter with a Sutter provider following the identification of a health gap or, for those without a health gap, following the date of the first biometric measure result in the EHR (i.e., the index date for those who had no health gap) and (ii) did not die in the 6-month post-period following the identification of a health gap. Figure 2 illustrated how the patients met eligibility criteria.
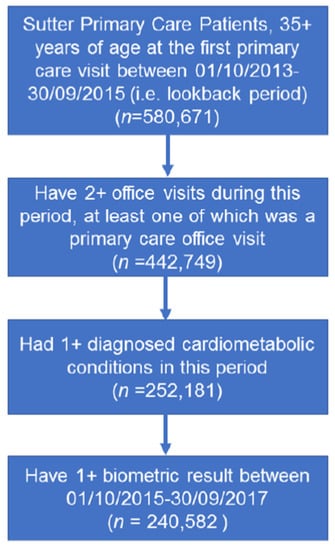
Figure 2.
Flowchart for study cohort identification. Flowchart for inclusion of Sutter primary care patients 35+ years of age to identify individuals with a cardiometabolic diagnosis and related health gap.
2.2. Data Sources
Only structured EHR data fields were used in this study and included the following: (1) encounter date and type; (2) ICD codes for encounter diagnoses, laboratory, or procedure orders; (3) clinical and laboratory measures relevant to CM disease risk factors, including body mass index (BMI), BP, lipids (i.e., low-density lipoprotein cholesterol (LDL-C), triglycerides, etc.), fasting blood glucose, HbA1c, and estimated glomerular filtration rate (eGFR) that may be modifiable or have a bearing on risk management; (4) patient sex, age, and race; and (5) medication dispense data provided by Surescripts. Dispense data were from 24,000 participating pharmacies providing coverage on more that 80% of medications dispensed for the Sutter Health primary care population. On a nightly basis, historic medication dispense data were retrieved from participating pharmacies for all patients with a scheduled encounter with a Sutter Health physician on the following day.
2.3. Study Outcomes: Health and Care Gaps
The primary outcomes for the study were health and care gaps. In order to identify the health gaps for hypertension, dyslipidemia, and diabetes, we began by translating corresponding clinical guidelines [17] into operational criteria that can be applied to structured EHR data.
The operational criteria were developed for health gaps as follows: a health gap exists when a clinical measure is at or above the specific threshold (e.g., systolic blood pressure [SBP] ≥ 140 mmHg) as defined by CPG criteria, which were active during the study period (see Table 1) [18]. Two sequential elevated BP measures obtained during encounters on separate days were used to define a BP health gap, consistent with American College of Cardiology (ACC)/American Heart Association (AHA) guidelines. One elevated measure was used to define an HbA1c (A1c ≥ 7) or LDL-C health gap (LDL ≥ 190, coronary heart disease (CHD) risk > 20%) [19,20]. While there may be nuances in these thresholds dependent on various personalized patient factors, for the purposes of algorithm development, the cutoffs for gap identification were simplified and standardized based on the active clinical guidelines during the study period.

Table 1.
Criteria for defining health gaps and therapeutic inertia care gaps.
The first encounter where a qualifying health gap was identified in the “Health Gap and Therapeutic Care Gap Assessment Period” was denoted as the index date (Figure 1). If there was no health gap, the index date was defined as the first encounter when the qualified clinical measure(s) was obtained, or the first PCP encounter for those who did not have a qualified measure. As two instances of elevated BP were required to define a health gap, and the index date was defined by the date of the second elevated BP measure to simulate how the gap identification would be managed in clinical practice.
Among patients who had a health gap, we created operational criteria to identify the corresponding care gaps. Medication adherence is usually not specifically articulated in the guidelines; however, it is an important factor to drive clinical actions (e.g., education, prescription, monitoring). We incorporated medication adherence into clinical treatment guidelines to create the operational criteria for identification of care gaps (Table 1) validated by Sutter Health clinicians.
Medication adherence, measured using dispense data, was extracted from the Sutter EHR for the 12-month period preceding each office encounter to calculate the proportion of days covered (PDC) for a specific medication [21]. PDC was calculated as days covered by the filled prescription period divided by 365 days (i.e., 1 year) if the medication was prescribed for more than 1 year, or divided by the number of days between first prescription and index date. If there were no medication dispense data for a given medication order, the patient was defined as not retrieving the medication. If there were medication dispense data, then the medication adherence status of a given patient was categorically defined as PDC values of ≥80% (adherent) and <80% (non-adherent) [22].
A care gap was identified within the 6-month post-period following identification of a health gap, and was assessed both with and without adherence information, because not all healthcare systems have medication adherence available in the EHR. In the absence of medication adherence data, a care gap was defined as the absence of any EHR record of a medication order or a medication adjustment (e.g., increased dose, change or add medications) for any patient with a health gap. When medication adherence data were present, a care gap was defined as follows: (i) for adherent patients with a health gap, a care gap existed if there were no record of a medication adjustment (i.e., added or intensified medication) being made to close the health gap; (ii) for non-adherent patients with a health gap, a care gap existed if there were no record that a previously prescribed medication was re-ordered or that no new medication was ordered; and (iii) for patients with a health gap who did not retrieve their medication (no dispense data present in the EHR), a care gap existed if there was no evidence of a new order to restart the medication.
2.4. Statistical Analysis
Using structured EHR data, we estimated the following: (1) the prevalence of health gaps, (2) medication adherence for patients with a health gap, and (3) the proportion of patients with care gaps.
Summary statistics were calculated for patients who met eligibility criteria for the study, and for each CM condition that included demographics, BMI, and comorbidities (measured by Charlson Comorbidity Index, or CCI) [23], as well as the prevalence of a health gap for each biometric measure (Table 2).
Table 2.
Demographic and clinical characteristics of primary care patients 35+ years old diagnosed with hypertension, hyperlipidemia, or diabetes.
Medication adherence level was categorized into three groups: (1) if medication was ordered and the patient retrieved the medication, then PDC was calculated as noted above, and we further stratified the patient into adherent (PDC ≥ 80%) or non-adherent (0 < PDC < 80%); (2) if medication was ordered and the patient did not retrieve the medication, then the patient was defined as non-adherent, but was denoted as medication not retrieved; and (3) if medication was not ordered by the clinician, the patient status was defined accordingly.
Further analyses were limited to patients with complete data (last row in Table 2, patients who had qualified lab measures and dispense data). Health gap status (yes/no) was the outcome. We assessed the extent to which health gaps are explained by a four-category adherence variable using logistic regression, reported by the odds ratio (OR) and 95% confidence interval (95% CI) (Table 3) among the population for whom dispense data were available. The regression modeling was completed, adjusting for the age at index date, sex, race (20 options categorized as African American, Asian, White, and other), ethnicity for Hispanic status yes, no, unknown), BMI (<25, 25–29.99, 30–34.99, 35+, unknown), smoking status (never, quit, smoking/passive, unknown), alcohol intake status (yes, no, unknown), CM disease severity defined by the number of CM conditions a patient had, and CCI.
Table 3.
Logistic regression model-based estimates of the odds ratio for the relationship between medication adherence, as defined by proportion of days covered (PDC) and patient health gap status with and without adjustment for other covariates a.
We further tested whether the association between medication adherence and health gaps varied among race groups by adding an interaction term between race group and medication adherence. Subgroup analyses were conducted to estimate OR and 95% CI for medication adherence and each health gap for each race group. Results are summarized in Table A1.
Care gap analysis was limited to patients who had a health gap. The criteria described in Table 1 were used to identify therapeutic care gaps for each health gap. A classification of “uncertain” was assigned to a care gap when there was a lack of evidence in the structured EHR data to document a physician’s efforts to close a health gap. Descriptive statistics were calculated to estimate the prevalence of care gaps, stratified by the medication adherence level (Table 4). Summary statistics by patient care gap status (i.e., no care gap, care gap, uncertain) on demographics, CCI, smoking status, baseline biometric value, and medication adherence are summarized in Table A2, Table A3 and Table A4.
Table 4.
Prospective therapeutic care gap (no actions taken to close health gap) status among primary care patients 35+ years old diagnosed with hypertension, hyperlipidemia, or diabetes who have a disease specific health gap by medication adherence status.
All analyses were performed using SAS Enterprise Guide 7.1 (Cary, NC, USA). The Sutter Health Institutional Review Board approved this study.
3. Results
A total of 252,181 eligible Sutter Health adult primary care patients aged 35+ years were identified (Table 2) with one or more diagnosed CM diseases (i.e., hypertension, hyperlipidemia, and diabetes).
Among the eligible primary care patients, 76% had hypertension, 75% had hyperlipidemia, and 23% had diabetes, and 17.8% had all three CM conditions. The prevalence of each CM condition varied by demographic features and health behaviors (Table 2).
Among all eligible patients, 95.4% (n = 240,582) had one or more CM clinical measure during the health gap follow-up period. Of these, 54.3% had at least one health gap. The prevalence of health gaps was 43.8% for hypertension, 57.2% for diabetes, and 33.5% for hyperlipidemia (Table 2). Among patients with qualified corresponding biometric measures, 81% had medication dispense data, varying from 75% to 85% by CM condition (Table 2).
Health gaps are highly associated with medication adherence status. Among patients who had a health gap, 26–37% were classified as adherent (i.e., ≥80% PDC) (Table 3). Compared to adherent patients, patients with a PDC < 80% (OR: 3.23, 95% CI: 2.50–4.39) were more likely to have a hyperlipidemia health gap, which was even more pronounced for those with no evidence of a medication order (OR: 5.80, 95% CI: 5.58–6.02) (Table 3). Similarly, the elevated risk of HbA1c health gap was observed for patients with PDC < 80% (OR: 1.15, 95% CI: 1.08–1.33) and more than five-fold higher risk for those with no evidence of a medication order (OR: 5.66, 95% CI: 5.35–5.99) (Table 3). The odds of having a BP health gap were slightly elevated for patients with a PDC < 80% but not statistically significant (OR: 0.97, 95% CI: 0.91–1.02). More generally, those who did not retrieve their medication and those with no medication order had elevated adjusted odds for a health gap for all three diagnosed diseases (Table 3).
The interaction term between medication adherence and race group was statistically significant for all three health gaps (p-values < 0.001). Subgroup analyses revealed that the level of the association (i.e., OR) between medication adherence and health gap varied among different race/ethnicity group, but the direction of the association (OR > 1 or OR < 1) remained the same across all racial groups (see Table A1).
Among patients with a health gap, 54.1%, 33.3%, and 64.6% also had a therapeutic care gap associated with managing BP, HbA1c, and LDL-C, respectively (Table 4). Within each medication adherence classification, the care gap status can be further grouped into yes, no, and uncertain (Table 4). For patients with a BP health gap, 31.5% patients were adherent to medication. Of those who were adherent to BP medications, therapeutic care gap status can be determined for 60% of patients (37.9% with therapeutic care gap and 22.1% without), and 40% where the care gap status was uncertain. Among patients who had an LDL health gap and were adherent to medication, 50.8% had a therapeutic care gap, 18.5% had no therapeutic care gap, and 30.8% were uncertain, which was similar for patients with an HbA1c health gap who were adherent to treatment (i.e., 47.8% with therapeutic care gap, 23.9% no therapeutic care gap, and 28.3% uncertain). However, therapeutic care gap status was uncertain for a significant portion of patients and especially among those with PDC < 80% who had hyperlipidemia (55.9%) and diabetes (70%) (Table 4). Among patients who did not retrieve a medication, 58.7%, 39.1%, and 15.6% had a therapeutic care gap identified for BP, LDL, and HbA1c management, respectively. Among patients with a health gap and no medication order, a care gap existed among 49.9% for HbA1c management and 82.1% for LDL management. Among those with no medication order, that is, no physician effort was observed to close a BP health gap, 100% of patients in this subgroup had a therapeutic care gap (Table 4) and the therapeutic care gap was attributed to a physician.
Among patients with hypertension, care gaps were more common for those with more CM conditions, those who were older (75+ years older), Black, had higher BMI, more comorbidities and did not retrieve their medications (Table A2). Among patients with dyslipidemia, care gaps were more common for those who were male, 55–64 years of age, Black, Hispanic, had a higher BMI, were smokers and had higher baseline LDL-C (Table A3). Among DM patients, care gaps were more common for males, <65 years old, and patients who did not retrieve medication (see Table A4).
4. Discussion
In this retrospective data analysis, the study team was able to identify all cardiometabolic health gaps and the majority of therapeutic care gaps using structured EHR data. Cardiometabolic therapeutic care gaps were common and varied significantly by patient medication adherence levels. The prevalence of therapeutic care gaps is distinctly different for patients who appear to not have retrieved medication versus patients who are adherent to their medication. Moreover, uncertainty in determining therapeutic care gap status varied by patient adherence level. For a significant minority of patients, the study results reveal that the use of structured EHR data alone is not sufficient to determine whether the patient, clinician, or both are responsible for a therapeutic care gap. In such instances, the reasons that a clinician did not initiate/titrate or modify medications may be documented in unstructured fields in the EHR. This suggests that progress notes and/or patient self-reported data may be useful in supporting physicians to efficiently and effectively manage care gaps, although exploring this possible solution was out-of-scope for this paper.
In the 6 months following identification of a health gap, this study found no evidence that medications were managed for more than half of patients with elevated blood pressure and LDL-C, and a third with an elevated HbA1c. This may be explained by a lack of recognition of a health gap by the physician, or by the physician’s perception of the efficacy of the medication, or by a lack of patient engagement in using the medication. The insufficient management by a physician is known as a physician care gap in this study, and the lack of patient use of the prescribed medication, known as a patient care gap, can be inferred by using EHR data to estimate patient treatment adherence. Though it is not possible to completely separate them, the actions to close a care gap are likely distinctly different when a patient appears to be non-adherent versus adherent; therefore, measuring adherence may shed light on challenges and strategies for managing therapeutic care gaps.
In the case of a medication not being ordered, the onus is most clearly on the physician and, therefore, the actions to close the care gap may be most straightforward and involve the least physician effort. For example, automated algorithms can be used to auto-pend orders for physician review when medications have not been ordered for a defined health gap. Non-adherence (i.e., medication not retrieved) can also be identified from structured EHR data and, once detected, the actions physicians can take are reordering the existing medications and/or educating patients on the importance of medications.
For patients with low adherence (PDC < 80%) the decision on appropriate actions to close a health gap is more nuanced. This study reveals that substantial uncertainty (55.9% to 70%) in care gaps status exists for low adherent patients with LDL and HbA1c health gaps. Further analysis shows that the uncertainty occurred mostly in patients with multiple therapeutic medications, where efforts to intensify medications are not straightforward to identify, in part because of definitional challenges, such as whether a care gap-closing action has been taken when at least one medication is changed to a different one but other medications remain the same. The lack of this level of detail in guidelines leads to physician’s individual judgement, which hinders standardization across different physicians and practices. Regardless of the attribution of the care gap, when low adherence is present, some automated or semi-automated actions may be possible, such as proactive outreach via tailored communications from the physician or an invitation to meet with a pharmacist, where such a resource exists.
Paradoxically, this study found that more physician work is required for adherent patients. For example, about 75% of diabetes patients with a persistent care gap were adherent to their prescribed medication, where it appears that the medication needs of the patient were not adequately managed. That is, there is no evidence in the patient’s EHR that the physician made an effort to determine if medication switching, titrating, or additions would mitigate the health gap.
In addition, we found that the prevalence of therapeutic care gaps varied by race/ethnicity groups. African American patients had a slightly higher prevalence of care gaps for hypertension and dyslipidemia, a finding consistent with prior studies on the initiation/intensification of medication [24,25,26]. Using EHR data to identify all patients with health gaps and creating targeted strategies to manage patients with different levels of medication adherence might reduce the disparity.
Physician lack of recognition, lack of follow-up, or simple time constraints [27] and administrative workload [28,29] may explain why a care gap persists. Medication management requires recognition of the health gap and then, in the moment, the need to review the patient record to understand what has been tried, a somewhat precise recall of relevant guideline knowledge, and a decision about the options that are logically worth discussing and testing. Structured and unstructured information may have to be reviewed from previous encounters. Then, the patient’s needs may have to be assessed to get to an optimal decision. The effort required to close the care gap may be more demanding than time will allow, especially if there are challenges related to patient engagement and self-management. Incomplete assessment of patient needs may simply be explained by how little time a physician has with a patient to understand needs and preferences [30,31,32,33,34,35]. As an alternative, pharmacists and other members of the care team could play a role in following up with patients to improve closure of care gaps [36,37].
Patient care gaps may persist because of patient-level factors that are directly under the patient’s control (e.g., low treatment adherence), or completely out of the patient’s control (e.g., lack of insurance coverage) [38,39]. In reality, the lack of a structured and efficient approach to document patient’s needs and indicators of medication adherence may result in a default attribution of medication care gaps to the clinician [26,40,41]. These problems in closing care gaps are not new. The need to support physicians to make rapid and reasonable decisions on what to do next and, in particular, what to discuss with the patient, can be met by assembling and displaying relevant clinical data and patient-reported data.
In summary, to improve EHR-facilitated patient health management, three essential components of information are necessary: efficient presentation of EHR structured data (e.g., potentially through visualization), information extracted from patient-reported data (e.g., physical activity, mental fitness, self-efficacy, insurance, etc.) or progress notes (i.e., patient–clinician communication regarding the treatment plan), and translation of clinical guidelines (i.e., with relevant contextual data and risk calculators to assess guideline applicability) to inform personalized recommendations. Clinical decision support tools that contain these three components might be a solution to improve quality of care by closing both health and care gaps [42,43,44,45].
There are several limitations to this study. First, the data used for the analysis came from a single health care system with a demographically diverse population. Second, the study did not consider other care gaps (e.g., screening, referral to dietician, diabetes educator, lifestyle consultant, etc.) for which the same challenges in actionable documentation exist. However, the described approach to using EHR data can be applied to other types of care gaps. Third, EHR data may be incomplete to fully decide if health gaps were resolved or care gaps were closed as the EHR may not capture whether patients received care or medication elsewhere. The missing data problem may be addressed, in part, as Epic’s Care Everywhere and similar EHR functions increase access to patient encounter data independent of the provider group. Fourth, this study did not use free-text data (i.e., progress notes) as the team were not resourced to extract and validate treatment plans, patient behavior, and the clinician’s justification using natural language processing (NLP). Nonetheless, unstructured data hold the promise of revealing specific actionable causes of care gaps.
5. Conclusions
Structured EHR data can identify health gaps and a majority of care gaps. Actions to close health gaps vary significantly at different medication adherence levels. Using structured EHR data to identify health gaps and measure medication adherence can be a first step in identifying factors attributable to care gaps and thereby help guide the direction for clinical action. Uncertainty about the clinical actions best suited to close health gaps can be minimized by three essential components: efficient presentation of EHR structured data, integration of patient-reported data or progress notes to indicate patient preferences, and translation of clinical guidelines to inform personalized recommendations.
Author Contributions
Conceptualization, W.F.S., X.Y. and J.B.J.; methodology, X.Y. and S.M.; software, X.Y. and S.M.; validation, A.H. and K.K.; formal analysis, X.Y.; investigation, X.Y., W.F.S., H.H., J.D.-R., S.M., F.R., A.H., K.K. and J.B.J.; data curation, S.M.; writing—original draft preparation, W.F.S., X.Y. and J.B.J.; writing—review and editing, X.Y., W.F.S., H.H., J.D.-R., S.M., F.R., A.H., K.K., K.M., F.S. and J.B.J.; visualization, S.M., H.H. and F.R.; supervision, W.F.S. and J.B.J.; project administration, H.H. and K.M.; funding acquisition, W.F.S., K.M. and J.B.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by AstraZeneca.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Sutter Health (protocol code 2015.130EXP (JLib) and 1 December 2015).
Informed Consent Statement
Patient consent was waived due to the following factors: First, as an analysis of electronic health record data from more than 1 million Sutter Health patients, the study would incur extensive delays in time and increases in cost associated with identifying and contacting patients and securing authorizations. Second, authorization would likely not be obtainable from a significant number of patients as the data requested covers a 5-year period. As a result, many patients are likely no longer under the care of a Sutter Health provider.
Data Availability Statement
Data are available on request due to restrictions, e.g., privacy or ethical reasons. The data (in summary statistics, non-identifiable aggregated form) presented in this study are available on request from the corresponding author. The data are not publicly available due to patient privacy considerations that prohibit the sharing of patient-level data.
Acknowledgments
This study was initiated and led by Sutter Investigators and funded by AstraZeneca.
Conflicts of Interest
To the best of our knowledge, no conflict of interest, financial or other exists for authors with the exception of MacDonald and Sifakis. MacDonald has a potential conflict of interest as she was an employee of AstraZeneca Pharmaceuticals LP and owns AstraZeneca Pharmaceuticals LP stock. Sifakis is a former employee of AstraZeneca Pharmaceuticals LP. The funders were involved in the interpretation of data, writing of the manuscript, and decision to publish the results.
Appendix A
File 1: Operational criteria to identify patients with each cardio-metabolic condition using Electronic Health Record (EHR) data
Type II Diabetes:
Inclusion Criteria
We used the following ICD-9 diagnosis codes to identify patients with diabetes:
- 250.xx, primary diabetes (except for 250.x1 and 250.x3, which specify type I)
- 357.2, polyneuropathy in diabetes
- 362.0x, diabetic retinopathy
- 366.41, diabetic cataract
We used the following inclusion criteria to identify a patient as a diabetic.
- ≥2 diagnoses from inpatient or outpatient encounters on separate days, OR
- ≥1 diagnosis from an inpatient or outpatient encounter and ≥1 evidence of insulin, OR
- ≥1 diagnosis from an inpatient or outpatient encounter and ≥1 evidence of oral antihyperglycemic, OR
- ≥2 qualifying lab values on separate days, OR
- ≥1 qualifying lab value and ≥1 evidence of insulin, OR
- ≥1 qualifying lab value and ≥1 evidence of oral antihyperglycemic
Based on American Diabetes Association (ADA) guidelines, ref [46] qualifying lab values have been defined as:
- Hemoglobin A1c ≥ 6.5%, OR
- Oral Glucose Tolerance Test ≥ 200 mg/dL, OR
- Random/Fasting Plasma Glucose in any setting ≥ 200 mg/dL, OR
- Fasting Plasma Glucose in an inpatient ≥ 126 mg/dL
Exclusion Criteria
Patients were exluded if they had type I or gestational diabetes (below).
Type I diabetes:
- Patients whose problem list or previous encounters specify Type 1 (250.x1, 250.x3) AND contain no ICD9 codes for type II diabetes (defined above), OR
- All medication orders are for Insulin (no oral antidiabetic medication orders) AND contain no ICD9 codes for type II diabetes (defined above).
Gestational Diabetes
Patients whose problem list or previous encounters specify gestational diabetes (648.8x) AND contain no ICD9 codes for type II diabetes (defined above)
Hypertension
Inclusion Criteria:
We used the following ICD-9 diagnosis codes to identify patients with hypertension:
- 401.x
- 402.x
- 403.x
- 404.x
- 405.x
The proposed inclusion criteria for hypertensive patients do not use antihypertensive medications as a component to qualify patients because of the multiple uses of antihypertensive drugs which increases the risk of misclassifying patients as hypertensive (false positives). Thus, we have selected the following as inclusion criteria:
- ≥2 diagnoses from inpatient or outpatient encounters on separate days, OR
- ≥2 qualifying BP measurements on separate days,
The qualifying BP measurements were selected based on guideline recommendations from the Eighth Joint National Committee [47] on the management of high blood pressure in adults. The recommendation for a separate blood pressure criteria for diabetics comes from the American Diabetes Association [46].
Qualifying BP measurements:
- BP ≥ 140/90 for any patient
- BP ≥ 130/80 for diabetics
Although guidelines recommend a slightly higher threshold (150 systolic, 90 diastolic) for patients 60 years or older, our clinicians elected to keep the definition at 140/90 for all patients 18 years or older. Patients qualify as hypertensive if either their systolic OR diastolic blood pressure is above the indicated threshold.
Exclusion Criteria
We used the following as rules for excluding patients with white coat hypertension, prehypertension, elevated blood pressure, and transiently elevated blood pressure from acute medical condition [48].
- Problem list specifies “white coat hypertension,” “prehypertension,” or “elevated blood pressure”
- All ICD9s explicitly reference 796.2 (elevated BP reading without a diagnosis of hypertension)
- Exclude BP measurements made in inpatient, emergency department, or ambulatory surgery center settings from contributing to a diagnosis.
Dyslipidemia
We used the following diagnosis codes to identify patients with dyslipidemia:
- 272.x
We used the following inclusion criteria to identify a patient as a dyslipidemic.
- ≥2 diagnoses from inpatient or outpatient encounters on separate days, OR
- ≥1 diagnosis from inpatient or outpatient encounters on separate days AND ≥ 1 qualifying lab value or ≥ 1 medication order, OR
- ≥2 qualifying lab values on separate days
Qualifying lab values are defined based on the ATP III guidelines [49]. More recent guidelines from the American College of Cardiology and American Heart Association in 2013 [20]. do not contain specific, numeric lipid goals; however, due to the likely absence of dyslipidemia diagnoses in the EHR, we recommend using a baseline lab value for the identification of dyslipidemic patients.
- LDL ≥ 160 mg/dL (4.14 mmol/L)
Table A1.
Logistic Regression model-based estimates of the odds ratio for the relationship between medication adherence, as defined by proportion of days covered (PDC) and patient health gap status with and without adjustment for other covariates, stratified by race group.
Table A1.
Logistic Regression model-based estimates of the odds ratio for the relationship between medication adherence, as defined by proportion of days covered (PDC) and patient health gap status with and without adjustment for other covariates, stratified by race group.
| Patient Medication Adherence | Hypertension Health Gap (n =83,033) | Hyperlipidemia Health Gap (n = 54,647) | Diabetes Health Gap (n = 31,297) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| PCT | Unadjusted | Adjusted a | PCT | Unadjusted | Adjusted a | PCT | Unadjusted | Adjusted a | |
| White | |||||||||
| 80%+ PDC | 7.7% | Ref | Ref | 27.1% | Ref | Ref | 33.7% | Ref | Ref |
| 0–79% PDC | 36.6% | 1.10 (1.05–1.15) | 1.01 (0.96–1.05) | 6.8% | 2.89 (2.70–3.09) | 2.94 (2.74–3.15) | 10.9% | 1.10 (0.99–1.21) | 1.14 (1.03–1.26) |
| Patient did not retrieve medication | 39.4% | 1.39 (1.36–1.43) | 1.20 (1.16–1.23) | 27.3% | 1.61 (1.53–1.69) | 1.68 (1.61–1.77) | 25.3% | 1.24 (1.16–1.33) | 1.26 (1.17–1.36) |
| No medication order | 16.3% | 1.43 (1.39–1.48) | 1.21 (1.17–1.25) | 38.9% | 4.64 (4.44–4.84) | 6.11 (5.83–6.4) | 30.2% | 5.67 (5.26–6.11) | 5.52 (5.11–5.96) |
| African American | |||||||||
| 80%+ PDC | 12.3% | Ref | Ref | 25.5% | Ref | Ref | 31.2% | Ref | Ref |
| 0–79% PDC | 40.6% | 0.96 (0.83–1.11) | 0.87 (0.75–1.01) | 10.2% | 2.67 (2.09–3.42) | 2.70 (2.09–3.48) | 15.8% | 1.22 (0.92–1.61) | 1.27 (0.95–1.69) |
| Patient did not retrieve medication | 33.5% | 1.53 (1.37–1.70) | 1.30 (1.16–1.45) | 23.5% | 2.06 (1.69–2.51) | 2.07 (1.68–2.53) | 23.1% | 1.41 (1.11–1.78) | 1.49 (1.17–1.91) |
| No medication order | 13.6% | 1.54 (1.33–1.77) | 1.30 (1.12–1.51) | 40.9% | 3.64 (3.05–4.34) | 4.71 (3.88–5.73) | 30.0% | 6.92 (5.38–8.90) | 7.31 (5.63–9.49) |
| Asian | |||||||||
| 80%+ PDC | 8.5% | Ref | Ref | 22.2% | Ref | Ref | 32.4% | Ref | Ref |
| 0–79% PDC | 38.8% | 1.16 (1.05–1.28) | 1.05 (0.95–1.17) | 7.2% | 2.87 (2.51–3.29) | 3.25 (2.81–3.75) | 10.6% | 1.22 (1.02–1.46) | 1.28 (1.06–1.53) |
| Patient did not retrieve medication | 38.0% | 1.50 (1.41–1.59) | 1.28 (1.19–1.36) | 25.9% | 1.64 (1.48–1.81) | 1.75 (1.58–1.95) | 27.7% | 1.34 (1.18–1.53) | 1.42 (1.24–1.62) |
| No medication order | 14.6% | 1.59 (1.46–1.73) | 1.31 (1.20–1.43) | 44.7% | 3.30 (3.01–3.60) | 5.43 (4.90–6.02) | 29.3% | 5.21 (4.57–5.93) | 5.37 (4.69–6.14) |
| Other | |||||||||
| 80%+ PDC | 9.1% | Ref | Ref | 23.9% | Ref | Ref | 34.2% | Ref | Ref |
| 0–79% PDC | 35.1% | 0.98 (0.91–1.07) | 0.89 (0.82–0.97) | 8.2% | 2.76 (2.45–3.09) | 2.92 (2.58–3.29) | 13.7% | 1.12 (0.96–1.30) | 1.19 (1.02–1.38) |
| Patient did not retrieve medication | 39.1% | 1.57 (1.50–1.66) | 1.33 (1.27–1.41) | 25.4% | 1.84 (1.68–2.01) | 1.93 (1.76–2.12) | 25.6% | 1.22 (1.08–1.37) | 1.26 (1.12–1.42) |
| No medication order | 16.8% | 1.64 (1.54–1.75) | 1.37 (1.29–1.47) | 42.5% | 3.57 (3.30–3.86) | 5.13 (4.70–5.60) | 26.5% | 5.89 (5.22–6.65) | 6.14 (5.42–6.95) |
a—adjusted for age, sex, BMI, number of CM conditions, ethnicity, smoking status, alcohol status and corresponding baseline biometric value.
Table A2.
Demographic and clinical characteristics of primary care patients 35+ years old who are included in care gap analysis for hypertension in Table 4.
Table A2.
Demographic and clinical characteristics of primary care patients 35+ years old who are included in care gap analysis for hypertension in Table 4.
| Patients with or without Therapeutic Care Gap for Hypertension | |||||
|---|---|---|---|---|---|
| Baseline Status | Category | With Care Gap (n = 25,060) | No Care Gap (n = 44,892) | Uncertain (n = 13,028) | p-Value |
| Diagnosed CM Diseases | 1 | 19.5% | 21.8% | 31.3% | <0.001 |
| 2 | 49.0% | 49.5% | 48.4% | ||
| 3 | 31.5% | 27.7% | 20.3% | ||
| Gender | Female | 56.4% | 55.8% | 56.0% | 0.44 |
| Male | 43.6% | 44.2% | 44.0% | ||
| Age | 35–44 | 3.2% | 3.2% | 5.7% | <0.001 |
| 45–54 | 11.5% | 13.1% | 17.0% | ||
| 55–64 | 21.0% | 22.6% | 24.2% | ||
| 65–74 | 29.8% | 29.0% | 26.9% | ||
| 75+ | 34.6% | 32.1% | 26.2% | ||
| Race | White | 67.6% | 66.7% | 68.8% | <0.001 |
| Black | 5.4% | 4.8% | 4.1% | ||
| Asian | 9.9% | 11.2% | 9.4% | ||
| Other | 17.1% | 18.3% | 17.7% | ||
| Hispanic | Yes | 10.0% | 10.0% | 9.9% | 0.95 |
| No | 90.0% | 90.0% | 90.1% | ||
| BMI | <25 | 22.4% | 21.9% | 24.3% | <0.001 |
| 25–29 | 34.0% | 35.3% | 35.6% | ||
| 30–34 | 24.3% | 22.6% | 22.8% | ||
| 35+ | 19.0% | 18.6% | 16.8% | ||
| Missing | 0.3% | 0.6% | 0.5% | ||
| Smoking Status | Yes | 5.9% | 6.3% | 6.7% | <0.001 |
| Passive or quit | 40.9% | 38.0% | 35.9% | ||
| No | 53.2% | 55.7% | 57.4% | ||
| Charlson Score | 0 | 51.6% | 59.9% | 63.2% | <0.001 |
| 1–2 | 39.1% | 33.7% | 30.8% | ||
| 3+ | 9.3% | 6.4% | 5.9% | ||
| Baseline SBP | Mean(std) | 153.4 (13.4) | 151.9 (12.6) | 150.4 (11.9) | 0.34 |
| Baseline DBP | Mean(std) | 81.7 (11.3) | 81.9 (10.9) | 82.7 (10.3) | 0.31 |
| Baseline Adherence | ≥80% | 10.2% | 15.4% | 5.7% | <0.001 |
| 0–79% | 41.3% | 84.6% | 24.8% | ||
| Not retrieved | 48.5% | 0% | 41.1% | ||
| No medication order | 0% | 0% | 28.4% | ||
Table A3.
Demographic and clinical characteristics of primary care patients 35+ years old who are included in care gap analysis for dyslipidemia in Table 4.
Table A3.
Demographic and clinical characteristics of primary care patients 35+ years old who are included in care gap analysis for dyslipidemia in Table 4.
| Patients with or without Therapeutic Care Gap for Dyslipidemia | |||||
|---|---|---|---|---|---|
| Baseline Status | Category | With Care Gap (n = 10,972) | No Care Gap (n = 26,748) | Uncertain (n = 3644) | p-Value |
| Diagnosed CM Diseases | 1 | 20.3% | 22.3% | 10.6% | <0.001 |
| 2 | 46.1% | 50.2% | 43.2% | ||
| 3 | 33.6% | 27.5% | 46.2% | ||
| Gender | Female | 56.7% | 60.8% | 60.4% | <0.001 |
| Male | 43.3% | 39.2% | 39.6% | ||
| Age | 35–44 | 5.8% | 6.1% | 3.8% | <0.001 |
| 45–54 | 21.4% | 21.8% | 16.4% | ||
| 55–64 | 32.8% | 30.7% | 27.0% | ||
| 65–74 | 26.0% | 24.5% | 27.9% | ||
| 75+ | 14.0% | 17.0% | 24.9% | ||
| Race | White | 60.7% | 61.8% | 61.8% | <0.001 |
| Black | 4.7% | 3.7% | 4.1% | ||
| Asian | 14.0% | 15.6% | 14.4% | ||
| Other | 20.6% | 19.0% | 19.7% | ||
| Hispanic | Yes | 12.5% | 9.9% | 11.3% | <0.001 |
| No | 87.5% | 90.1% | 88.8% | ||
| BMI | <25 | 19.6% | 24.4% | 20.9% | <0.001 |
| 25–29 | 37.9% | 37.7% | 37.3% | ||
| 30–34 | 24.8% | 22.7% | 24.4% | ||
| 35+ | 17.4% | 14.9% | 17.0% | ||
| Missing | 0.3% | 0.4% | 0.4% | ||
| Smoking Status | Yes | 8.0% | 5.9% | 6.6% | <0.001 |
| Passive or quit | 33.9% | 31.8% | 36.5% | ||
| No | 58.1% | 62.3% | 57.0% | ||
| Charlson Score | 0 | 65.6% | 68.6% | 57.3% | <0.001 |
| 1–2 | 29.1% | 27.1% | 35.4% | ||
| 3+ | 5.3% | 4.3% | 7.3% | ||
| Baseline LDL-C | Mean(std) | 155.2 (33.7) | 148.0 (29.2) | 138.1 (29.3) | 0.02 |
| Baseline Adherence | ≥80% | 15.6% | 10.2% | 25.6% | <0.001 |
| 0–79% | 7.3% | 6.0% | 18.5% | ||
| Not retrieved | 13.7% | 14.3% | 55.9% | ||
| No medication order | 63.5% | 69.5% | 0% | ||
Table A4.
Demographic and clinical characteristics of primary care patients 35+ years old who are included in care gap analysis for diabetes in Table 4.
Table A4.
Demographic and clinical characteristics of primary care patients 35+ years old who are included in care gap analysis for diabetes in Table 4.
| Patients with or without Therapeutic Care Gap for Diabetes | |||||
|---|---|---|---|---|---|
| Baseline Status | Category | With Care Gap (n = 10,051) | No Care Gap (n = 7703) | Uncertain (n = 4927) | p-Value |
| Diagnosed CM Diseases | 1 | 1.8% | 1.2% | 2.0% | <0.001 |
| 2 | 19.0% | 16.5% | 18.5% | ||
| 3 | 79.2% | 82.8% | 79.5% | ||
| Gender | Female | 45.6% | 48.2% | 48.3% | <0.001 |
| Male | 54.4% | 51.8% | 51.7% | ||
| Age | 35–44 | 6.6% | 5.0% | 5.7% | |
| 45–54 | 21.9% | 17.5% | 17.9% | <0.001 | |
| 55–64 | 28.6% | 28.0% | 25.8% | ||
| 65–74 | 26.5% | 28.3% | 27.0% | ||
| 75+ | 16.5% | 21.3% | 23.5% | ||
| Race | White | 52.8% | 52.6% | 51.4% | 0.13 |
| Black | 4.5% | 5.4% | 5.2% | ||
| Asian | 18.5% | 18.2% | 19.0% | ||
| Other | 24.0% | 23.9% | 24.4% | ||
| Hispanic | Yes | 15.2% | 16.2% | 15.7% | 0.31 |
| No | 84.8% | 83.8% | 84.3% | ||
| BMI | <25 | 13.0% | 13.4% | 15.1% | <0.001 |
| 25–29 | 29.6% | 29.2% | 31.5% | ||
| 30–34 | 28.2% | 27.6% | 27.4% | ||
| 35+ | 28.8% | 29.5% | 25.5% | ||
| Missing | 0.4% | 0.3% | 0.5% | ||
| Smoking Status | Yes | 6.0% | 6.2% | 6.3% | 0.31 |
| Passive or quit | 35.4% | 36.9% | 35.7% | ||
| No | 58.6% | 56.8% | 58.6% | ||
| Charlson Score | 0 | 42.9% | 42.6% | 45.6% | 0.001 |
| 1–2 | 46.2% | 46.5% | 44.5% | ||
| 3+ | 10.9% | 10.9% | 9.9% | ||
| Baseline HbA1c | Mean(std) | 8.3 (1.5) | 8.2 (1.4) | 8.0 (1.3) | 0.20 |
| Baseline Adherence | ≥80% | 21.8% | 91.7% | 35.5% | <0.001 |
| 0–79% | 5.1% | 8.3% | 29.1% | ||
| Not retrieved | 57.9% | 0% | 14.8% | ||
| No medication order | 15.1% | 0% | 20.7% | ||
References
- Sperling, L.S.; Mechanic, J.I.; Neeland, I.J.; Herrick, C.J.; Després, J.-P.; Ndumele, C.E.; Vijayaraghavan, K.; Handelsman, Y.; Puckrein, G.A.; Araneta, M.R.G.; et al. The CardioMetabolic Health Alliance: Working Toward a New Care Model for the Metabolic Syndrome. J. Am. Coll. Cardiol. 2015, 66, 1050–1067. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Committee on Quality of Health Care in America; Kohn, L.T.; Corrigan, J.M.; Donaldson, M.S. To Err is Human: Building a Safer Health System; Kohn, L.T., Corrigan, J.M., Donaldson, M.S., Eds.; National Academies Press: Washington, DC, USA, 2000. Available online: http://www.ncbi.nlm.nih.gov/books/NBK225182/ (accessed on 19 June 2018).
- Glynn, L.G. Multimorbidity: Another key issue for cardiovascular medicine. Lancet 2009, 374, 1421–1422. [Google Scholar] [CrossRef]
- Nichols, G.A.; Joshua-Gotlib, S.; Parasuraman, S. Independent Contribution of A1C, Systolic Blood Pressure, and LDL Cholesterol Control to Risk of Cardiovascular Disease Hospitalizations in Type 2 Diabetes: An Observational Cohort Study. J. Gen. Intern. Med. 2013, 28, 691–697. [Google Scholar] [CrossRef]
- Emerging Risk Factors Collaboration. Association of Cardiometabolic Multimorbidity With Mortality. JAMA 2015, 314, 52–60. [Google Scholar] [CrossRef]
- Colayco, D.C.; Niu, F.; McCombs, J.S.; Cheetham, T.C. A1C and Cardiovascular Outcomes in Type 2 Diabetes: A nested case-control study. Diabetes Care 2010, 34, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Stratton, I.; Cull, C.A.; Adler, A.I.; Matthews, D.R.; Neil, H.A.W.; Holman, R.R. Additive effects of glycaemia and blood pressure exposure on risk of complications in type 2 diabetes: A prospective observational study (UKPDS 75). Diabetologia 2006, 49, 1761–1769. [Google Scholar] [CrossRef] [PubMed]
- Okemah, J.; Peng, J.; Quiñones, M. Addressing Clinical Inertia in Type 2 Diabetes Mellitus: A Review. Adv. Ther. 2018, 35, 1735–1745. [Google Scholar] [CrossRef] [PubMed]
- Haghighatpanah, M.; Nejad, A.S.M.; Haghighatpanah, M.; Thunga, G.; Mallayasamy, S. Factors that Correlate with Poor Glycemic Control in Type 2 Diabetes Mellitus Patients with Complications. Osong Public Health Res. Perspect. 2018, 9, 167–174. [Google Scholar] [CrossRef]
- Kruse, C.S.; Stein, A.; Thomas, H.; Kaur, H. The use of Electronic Health Records to Support Population Health: A Systematic Review of the Literature. J. Med. Syst. 2018, 42, 214. [Google Scholar] [CrossRef]
- Kawamoto, K.; Anstrom, K.J.; Anderson, J.B.; Bosworth, H.B.; Lobach, D.F.; McAdam-Marx, C.; Ferranti, J.M.; Shang, H.; Yarnall, K.S.H. Long-Term Impact of an Electronic Health Record-Enabled, Team-Based, and Scalable Population Health Strategy Based on the Chronic Care Model. AMIA Annu. Symp. Proc. 2017, 2016, 686–695. [Google Scholar]
- Coleman, K.; Austin, B.T.; Brach, C.; Wagner, E.H. Evidence on the Chronic Care Model in the new millennium. Health Aff. 2009, 28, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Paul, S.K.; Klein, K.; Thorsted, B.L.; Wolden, M.L.; Khunti, K. Delay in treatment intensification increases the risks of cardiovascular events in patients with type 2 diabetes. Cardiovasc. Diabetol. 2015, 14, 100. [Google Scholar] [CrossRef]
- Riddle, M.C.; Karl, D.M. Individualizing targets and tactics for high-risk patients with type 2 diabetes: Practical lessons from ACCORD and other cardiovascular trials. Diabetes Care 2012, 35, 2100–2107. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nichols, G.A.; Koo, Y.H.; Shah, S.N. Delay of insulin addition to oral combination therapy despite inadequate glycemic control: Delay of insulin therapy. J. Gen. Intern. Med. 2007, 22, 453–458. [Google Scholar] [CrossRef]
- Crowley, M.J.; Holleman, R.; Klamerus, M.L.; Bosworth, H.B.; Edelman, D.; Heisler, M. Factors associated with persistent poorly controlled diabetes mellitus: Clues to improving management in patients with resistant poor control. Chronic Illn. 2014, 10, 291–302. [Google Scholar] [CrossRef]
- Rao, T.S.; Tandon, A. Clinical Practice Guidelines: Principles for Clinical Practice. Indian J. Psychiatry 2017, 59 (Suppl. S1), S5–S6. [Google Scholar] [CrossRef] [PubMed]
- U.S. Preventive Services Task Force. Screening for High Blood Pressure: U.S. Preventive Services Task Force Reaffirmation Recommendation Statement. Ann. Intern. Med. 2007, 147, 783–786. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Standards of Medical Care in Diabetes—2013. Diabetes Care 2013, 36 (Suppl. S1), S11–S66. [Google Scholar] [CrossRef]
- Stone, N.; Robinson, J.G.; Lichtenstein, A.H.; Merz, C.N.B.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.; et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129 (Suppl. S2), S46–S48. [Google Scholar] [CrossRef]
- Vink, N.M.; Klungel, O.H.; Stolk, R.P.; Denig, P. Comparison of various measures for assessing medication refill adherence using prescription data. Pharmacoepidemiol. Drug Saf. 2009, 18, 159–165. [Google Scholar] [CrossRef]
- Haynes, R.B.; Taylor, D.W.; Sackett, D.L.; Gibson, E.S.; Bernholz, C.D.; Mukherjee, J. Can simple clinical measurements detect patient noncompliance? Hypertension 1980, 2, 757–764. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Mathur, R.; Farmer, R.E.; Eastwood, S.V.; Chaturvedi, N.; Douglas, I.; Smeeth, L. Ethnic disparities in initiation and intensification of diabetes treatment in adults with type 2 diabetes in the UK, 1990–2017: A cohort study. PLoS Med. 2020, 17, e1003106. [Google Scholar] [CrossRef] [PubMed]
- Khunti, K.; Gomes, M.; Pocock, S.; Shestakova, M.V.; Pintat, S.; Fenici, P.; Hammar, N.; Medina, J. Therapeutic inertia in the treatment of hyperglycaemia in patients with type 2 diabetes: A systematic review. Diabetes Obes. Metab. 2018, 20, 427–437. [Google Scholar] [CrossRef]
- Milman, T.; Joundi, R.A.; Alotaibi, N.M.; Saposnik, G. Clinical inertia in the pharmacological management of hypertension: A systematic review and meta-analysis. Medicine 2018, 97, e11121. [Google Scholar] [CrossRef]
- Gundersen, L. Physician Burnout. Ann. Intern. Med. 2001, 135, 145. [Google Scholar] [CrossRef]
- Bodenheimer, T.; Sinsky, C. From triple to quadruple aim: Care of the patient requires care of the provider. Ann. Fam. Med. 2014, 12, 573–576. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Dyrbye, L.N.; West, C.P. Addressing Physician Burnout: The Way Forward. JAMA 2017, 317, 901–902. [Google Scholar] [CrossRef]
- Saposnik, G.; Sempere, A.P.; Raptis, R.; Prefasi, D.; Selchen, D.; Maurino, J. Decision making under uncertainty, therapeutic inertia, and physicians’ risk preferences in the management of multiple sclerosis (DIScUTIR MS). BMC Neurol. 2016, 16, 58. [Google Scholar] [CrossRef]
- Zafar, A.; Stone, M.A.; Davies, M.J.; Khunti, K. Acknowledging and allocating responsibility for clinical inertia in the management of Type 2 diabetes in primary care: A qualitative study. Diabet. Med. 2015, 32, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Basile, J. Clinical inertia and blood pressure goal attainment. J. Clin. Hypertens. 2009, 11 (Suppl. S1), S5–S12. [Google Scholar] [CrossRef]
- Phillips, L.S.; Branch, W.T.; Cook, C.B.; Doyle, J.P.; El-Kebbi, I.M.; Gallina, D.L.; Miller, C.D.; Ziemer, D.C.; Barnes, C.S. Clinical inertia. Ann. Intern. Med. 2001, 135, 825–834. [Google Scholar] [CrossRef]
- Gil-Guillén, V.F.; Orozco-Beltrán, D.; Márquez-Contreras, E.; Durazo-Arvizu, R.; Cooper, R.; Pita-Fernández, S.; González-Segura, D.; Carratala-Munuera, C.; De Pablo, J.L.M.; Pallares, V.; et al. Is there a predictive profile for clinical inertia in hypertensive patients? An observational, cross-sectional, multicentre study. Drugs Aging 2011, 28, 981–992. [Google Scholar] [CrossRef]
- Balkau, B.; Halimi, S.; Blickle, J.; Attali, C.; Avignon, A.; Amelineau, E.; Chartier, I.; Geoffroy, M.-A.; Verges, B.l. Reasons for non-intensification of therapy in type 2 diabetes patients uncontrolled by oral monotherapy in general practice in France: The DIAttitude study. Diabetologia 2013, 56, S117. [Google Scholar] [CrossRef]
- Cowart, K.; Sando, K. Pharmacist Impact on Treatment Intensification and Hemoglobin A1C in Patients With Type 2 Diabetes Mellitus at an Academic Health Center. J. Pharm. Pract. 2019, 32, 648–654. [Google Scholar] [CrossRef]
- Cowart, K. Overcoming Clinical Inertia in Diabetes Management: Pharmacist Opportunities. US Pharm. 2018, 43, 25–34. Available online: https://www.uspharmacist.com/article/overcoming-clinical-inertia-in-diabetes-management-pharmacist-opportunities (accessed on 10 June 2021).
- Jin, J.; Sklar, G.E.; Min Sen Oh, V.; Chuen Li, S. Factors affecting therapeutic compliance: A review from the patient’s perspective. Ther. Clin. Risk Manag. 2008, 4, 269–286. [Google Scholar] [CrossRef] [PubMed]
- Alexandre, K.; Desrichard, O.; Burnand, B.; Peytremann-Bridevaux, I. Factors influencing self-management in adults with diabetes: An umbrella review protocol. JBI Database Syst. Rev. Implement. Rep. 2017, 15, 2630–2637. [Google Scholar] [CrossRef] [PubMed]
- Ziemer, D.C.; Miller, C.D.; Rhee, M.K.; Doyle, J.P.; Watkins, C.; Cook, C.B.; Gallina, D.L.; El-Kebbi, I.M.; Barnes, C.S.; Dunbar, V.G.; et al. Clinical inertia contributes to poor diabetes control in a primary care setting. Diabetes Educ. 2005, 31, 564–571. [Google Scholar] [CrossRef]
- Salanitro, A.; Agee, B.; Burczyk-Brown, J.; Funkhouser, E.M.; Muntner, P.; Crenshaw, K.; Horton, T.; Halanych, J.; Richman, J.; Kaffka, J.; et al. Appropriate inaction and clinical inertia. J. Gen. Intern. Med. 2010, 25, S223–S224. [Google Scholar]
- O’Connor, P.J.; Sperl-Hillen, J.M.; Rush, W.A.; Johnson, P.E.; Amundson, G.H.; Asche, S.E.; Ekstrom, H.L.; Gilmer, T.P. Impact of Electronic Health Record Clinical Decision Support on Diabetes Care: A Randomized Trial. Ann. Fam. Med. 2011, 9, 12–21. [Google Scholar] [CrossRef]
- Dubey, V.; Glazier, R. Preventive care checklist form. Evidence-based tool to improve preventive health care during complete health assessment of adults. Can. Fam. Phys. 2006, 52, 48–55. [Google Scholar]
- Taylor, E.F.; Machta, R.M.; Meyers, D.S.; Genevro, J.; Peikes, D.N. Enhancing the primary care team to provide redesigned care: The roles of practice facilitators and care managers. Ann. Fam. Med. 2013, 11, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Misra-Hebert, A.D.; Rabovsky, A.; Yan, C.; Hu, B.; Rothberg, M.B. A Team-based Model of Primary Care Delivery and Physician-patient Interaction. Am. J. Med. 2015, 128, 1025–1028. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 2. Classification and diagnosis of diabetes. Diabetes Care 2015, 38 (Suppl. S1), S8–S16. [Google Scholar] [CrossRef] [PubMed]
- James, P.A.; Oparil, S.; Carter, B.L.; Cushman, W.C.; Himmelfarb, C.D.; Handler, J.; Lackland, D.T.; Lefevre, M.L.; MacKenzie, T.D.; Ogedegbe, O.; et al. 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014, 311, 507–520. [Google Scholar] [CrossRef]
- Rakotz, M.K.; Ewigman, B.G.; Sarav, M.; Ross, R.E.; Robicsek, A.; Konchak, C.W.; Gavagan, T.F.; Baker, D.W.; Hyman, D.J.; Anderson, K.P.; et al. A technology-based quality innovation to identify undiagnosed hypertension among active primary care patients. Ann. Fam. Med. 2014, 12, 352–358. [Google Scholar] [CrossRef]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).