Abstract
Self-determination and self-advocacy are critical components of quality of life, and the instruction of these skills continues to emerge as an important outcome for Disabled people, specifically people with intellectual disability (ID). The purpose of this scoping review examined the perspectives of adults with ID and the experienced barriers when self-advocating, making choices, and goal setting. This scoping review searched multiple databases for empirical research, which collected the perspective of people with intellectual disability and what they identified as barriers to self-advocacy. Results included 30 articles with an international perspective available within the English language. The authors utilized Bronfenbrenner’s process–person–context–time (PPCT) model to identify how these barriers are experienced in various relationships and environments and throughout time. The barriers identified fell into the various aspects of the PPCT model. Understanding these barriers provides insights into ways to begin to dismantle them, and this review details recommendations for research, policy, and practices.
1. Introduction
Self-advocacy, or the ability to articulate one’s wants, needs, or goals, is essential to building confidence to speak up (Chong et al., 2024), fostering self-worth and pride (I. Smith & Mueller, 2022), increasing engagement for themselves and in the community (Chong et al., 2024; I. Smith & Mueller, 2022), and improving quality of life (Kober, 2010; Schalock et al., 2005; Wehmeyer, 2020). While self-advocacy is important for all individuals across the lifespan, it is especially important for Disabled people, as their self-advocacy efforts are often dismissed (Chong et al., 2024; I. Smith & Mueller, 2022). The authors use identity-first language, or naming the identity of the person first (i.e., Disabled), when globally referring to Disabled people, as well as person-first language, or placing a person before a disability descriptor, when referring to individuals with intellectual disability (ID), as this population advocated for this terminology to acknowledge their personhood (Grech et al., 2023). The authors used both identity-first language and person-first language to honor and acknowledge the Disability community and speak to the unique needs of people with ID.
The prevalence of eugenics ideology throughout the world in the beginning of the 20th century oppressed Disabled people, questioning their rights as humans (Rembis et al., 2018). Social institutions have long implemented policies and practices that historically marginalize the Disabled population through exclusion from education, participation in their community, access to human rights, and even criminalization of the existence of Disabled people (Heumann & Joiner 2020; Nielsen, 2012; Schweik, 2009; Rembis et al., 2018). During the disability rights movement, powerful Disabled advocates, such as Judy Heumann, Ed Roberts, and Brad Lomax called out injustices and reformed laws to create greater inclusivity and access to basic human rights (Heumann & Joiner 2020; Nielsen, 2012). The work of Disabled advocates helped to dismantle discriminatory laws and practices and implemented more inclusive policies, such as Section 504 of the Rehabilitation Act, the Individuals with Disabilities Education Act, and the Americans with Disabilities Act in the United States (Heumann & Joiner, 2020; Nielsen, 2012). The United Nations Educational, Scientific, and Cultural Organization (UNESCO), the Spanish government, and the delegates of the World Conference on Special Need Education presented the Salamanca Statement (UNESCO, 1994) urging nations across the world to provide an education to all children, youth, and adults with disabilities. Additionally, the United Nation’s Convention on the Rights of Persons with Disabilities (UNCRPD) (UNCRPD, 2016) established a set of principles as an international human rights treaty to advance the respect, dignity, and equality for Disabled people through honoring Disabled people’s many identities, their autonomy, and greater inclusion in society. Although legal advancements and more inclusive access and protections exist in nations across the world, ableist ideologies are woven into the fabric of societies, which stymies self-advocacy and socially just opportunities for Disabled people (Nario-Redmond, 2019; Nielsen, 2012; Rembis et al., 2018).
Ableism, or “ideas, practices, institutions, and social relations that presume able-bodiedness, and by doing so, construct persons with disabilities as marginalized, oppressed, and largely invisible ‘others’” (Chouinard, 1997, p. 380), negatively impacts Disabled people socially, emotionally, educationally, economically, and physically (Chouinard, 1997; Nario-Redmond, 2019). Further, ableist ideologies within education limit graduation and diploma attainment for Disabled students, thereby compromising future opportunities of seeking advanced education or employment (Nario-Redmond, 2019). Additionally, ableism fosters paternalistic behaviors, with non-disabled people making decisions for Disabled people before because they ‘know best’ (Chouinard, 1997; Nario-Redmond, 2019). Although ableism is the foundation for systemic oppression of Disabled people, people with intellectual disability (“a lifelong condition where significant limitations in both intellectual functioning and adaptive behavior emerge during the developmental period”; [The Arc, 2019, para 1]) are the among individuals who are especially impacted by ableism due to the historical marginalization resulting from institutionalization, eugenics, medical model discourses causing low expectations for people with intellectual disabilities (ID), and individualistic ideologies (Gappmayer, 2021; Kober, 2010; Schalock et al., 2005). One way to combat the pervasive negative impact of ableism, however, is by teaching and honoring self-advocacy.
1.1. Rationale
There is a growing body of research reporting the effectiveness of interventions on developing self-advocacy skills among Disabled students in US education systems (Alsaeed et al., 2023; Lee et al., 2015; Raley et al., 2018; Wehmeyer, 2020). Additionally, through the implementation of principles of UNCRPD, international education focuses on the development of self-determination skills in Disabled people (Burke et al., 2024). Despite these interventions, Disabled people—especially people with ID—are less likely to have desirable outcomes including (a) engaging in shared/support decision making (Bigby et al., 2021), (b) employment (Avellone et al., 2021), (c) independent living (Zambri et al., 2023), and overall quality of life (Kober, 2010; Schalock et al., 2005; Wehmeyer, 2020). Research documents several barriers that prevent actualization of self-advocacy leading to a high quality of life for individuals with ID, including (a) lack of knowledge and skills to self-advocate (Test et al., 2005; Shogren et al., 2017), (b) lack of opportunity for decision making or communicate their wants or needs (Shogren & Raley, 2022), (c) limited power to enact decisions due to guardianship over the person with ID (Shogren & Raley, 2022), (d) difficulty communicating (Shogren et al., 2017), and (e) low expectations (Shogren et al., 2017). Commonly cited research on barriers to self-advocacy are centered on the limitations of individuals with ID, problematizing the very nature of a Disabled individual’s existence, as opposed to ableist systems and structures that limit self-advocacy (Gappmayer, 2021). Further, commonly cited research on barriers to self-advocacy are largely from the perspectives of professionals (e.g., teachers, service providers in adult services [Shogren et al., 2017]) or parents, families, or caregivers of individuals ID (Shogren et al., 2017; Shogren & Raley, 2022), as opposed to the person most impacted by barriers to self-advocacy—individuals with ID themselves. This practice not only reinforces ableist structures and practices through epistemicide, which Patin et al. (2020) defines as, “the killing, silencing, annihilation, or devaluing of a knowledge system” (p. 2) but also compromises the social validity and effectiveness of efforts to increase self-advocacy.
1.2. Objectives
Learning about barriers to self-advocacy from the perspectives of individuals with ID can inform meaningful approaches to self-advocacy resulting in a high quality of life by addressing underlying issues that undermine self-advocacy among this population. Given that research supports self-advocacy instruction and intervention, people with ID continue to not be heard. The objective of this scoping review was to understand barriers identified by people with ID across the globe and understand how people with ID experience these barriers through the process–person–context–time model of human development to inform future research, practices, and policies that are moving in the direction of justice and inclusiveness.
2. Conceptual Framework
We used Bronfenbrenner’s (2005) process–person–context–time (PPCT) model of human development, which provides a way to understand how reciprocal bioecological contexts influence human development over time (Bronfenbrenner, 2005; Bronfenbrenner & Morris, 2007; Xia et al., 2020). The PPCT model centers a person, including their personality traits, biopsychosocial characteristics such as any disabilities, genetic factors, physical appearance, or feeling emotions such as depression or happiness, within five contextual systems: the micro, meso, exo, macro, and chronosystems. The research team selected the PPCT model to analyze the barriers described because the PPCT model goes beyond locating the barriers within various contextual environments. The PPCT model considers the interaction among a person’s characteristics, relationships, and interactions within the microsystem, the context, and the impact of time (Xia et al., 2020). The microsystem involves environments and individuals in which the person interacts immediately (e.g., parents, siblings, teachers, neighborhood). Further, the PPCT model highlights the proximal processes that occur between microsystem factors and the person at the center of the model through “progressively more complex reciprocal interactions” (Bronfenbrenner & Morris, 1998, p. 996). The mesosystem involves interactions that occur among microsystem structures (e.g., home/school, work/community). The exosystem involves structures that indirectly influence the person at the center of the model (e.g., school board, work or service agency policies, state and federal laws). The macrosystem involves societal belief systems and ideologies (e.g., ableism, paternalism, racism, beauty). Finally, the chronosystem involves the impact of time and changes over time on human development (e.g., life transitions, changes in environments over time, historical events). Proximal processes, the last element of the PPCT model, involves the “progressively more complex reciprocal interaction between an active, evolving biopsychological human organism and the persons, objects, and symbols in its immediate external environment” (Bronfenbrenner & Morris, 1998, p. 996). When considering barriers to self-advocacy, understanding where barriers occur within bioecological systems can aid in developing meaningful approaches to addressing barriers across structures.
Bronfenbrenner and Morris (2007) discussed the importance of biological factors such as genetic factors, illness, brain function, and affect when considering the person engages with their environment. This scoping review also utilizes intersectionality to examine the many identities people have, including race, gender, sexual orientation, ability, sex, class, neurotype, etc., and how these identities intersect with one another causing overlapping systemic and institutional oppression (Collins, 2019; Crenshaw, 1991). Collins (2019) states that an intersectional lens examines how identities relate to power and privilege within the systems people access. Using intersectionality as an analytical tool presents critical action for a more socially just world.
3. Methods
The purpose of this scoping review was to understand what is known about the barriers to self-advocacy from the perspective of people with ID and map the existing knowledge to better understand the complexity of these barriers. The author team employed a scoping review approach to explore the breadth and depth of evidence surrounding barriers to self-advocacy (Munn et al., 2018). Using the JBI Manual for Evidence Synthesis (Peters et al., 2020), researchers engaged in the following steps: (1) identify the research questions, (2) identify relevant studies, (3) study selection, (4) assessing the data, (5) summarizing and reporting the data, and (6) presenting the results. Reporting followed the PRISMA-ScR guidelines (Tricco et al., 2018); the completed checklist is provided in Supplementary File S1.
3.1. Inclusionary and Exclusionary Criteria
3.1.1. Types of Participants
The articles reported the perspectives of people with intellectual disability, including Intellectual Disability (ID) (or ‘Learning Disability,’ the phrase used for Intellectual Disability in the UK), and common co-occurring developmental disabilities or associated syndromes such as Autism, Fragile X, Down Syndrome, and Rett Syndrome. Participants included those aged 14 years or older (the age at which high school typically starts as well as transition planning for adult life). Exclusionary criteria included participants with acquired disabilities after the age of 18 years of age, such as a traumatic brain injury, articles that did not state or disaggregate disability, and studies that included participants with disabilities other than ID.
3.1.2. Concepts
The overarching concept of this article is the barriers to self-advocacy; therefore, the articles must report barriers, challenges, obstacles, or factors to self-advocacy. The authors used Test and colleagues’ (Test et al., 2005) conceptual framework for self-advocacy to define the key constructs of self-advocacy as (a) knowledge of self (i.e., knowing strengths, goals, preferences, needs, responsibilities), (b) knowledge of rights (i.e., personal, community, legal, educational, human rights), (c) communication (i.e., body language, listening, form of communication, assertiveness), and (d) leadership (i.e., advocating for self and others, action, knowledge of resources).
3.1.3. Context
Given that the purpose of this scoping review is open to discovering the knowledge related to the barriers to self-advocacy, the articles could be from any geographic location. The articles must be written in English (the researchers were monolingual). The researchers did not apply any other limitations or boundaries on the dates of publications.
3.1.4. Types of Evidence Sources
Inclusionary criteria included peer-reviewed empirical research studies that include specific information about participant disability and age. The research team also included dissertations retrieved from ProQuest. The research team did not include inaccessible full text or policy briefs. The team also excluded literature reviews as secondary research. Further, research that utilized proxy reports was also not included.
3.2. Search Strategy
In collaboration with the social sciences research librarian from George Mason University, the team conducted searches in Proquest, EBSCO, PubMed, and Web of Science to gather research across various disciplines (e.g., education, psychology, medicine). The EBSCO database search also included other databases within its search including APA, Cinahl, ERIC, Education Complete, Medline, Psychology and Behavioral Sciences, and these databases fall under the EBSCO heading within the PRISMA chart. The following Boolean phrases, informed by Test et al.’s conceptual framework (Test et al., 2005), were used in each search: (“mental retardation” or “intellectual disabilit*” or “developmental disabilit*” or “developmental delay*” or IDD or syndrome* or autism) AND (“self advocacy” or “self advocat*” or “self determination” or “self efficacy” or “decision mak*” or autonomy) AND (barrier* or obstacle* or challenge* or factor*) AND (adult* or teen* or “high school*” or “college student*” or “postsecondary age”). The search occurred on 5 March 2025. Hand searches were not conducted as a part of the search strategy given the range of databases covering topics across disciplines to consider self-advocacy completed throughout a person’s life.
3.3. Screening, Selection, and Data Extraction
The researchers imported search findings into Covidence (2024), a web-based software program to complete a systematic review of the literature. The review protocol was developed in Covidence, and it was not registered. The first author trained all the researchers on the scoping review and inclusionary and exclusionary criteria. The research team met weekly throughout the course of the scoping review. All nine researchers screened titles and abstracts, followed by full-text review using inclusionary and exclusionary criteria for data extraction. If two members of the research team did not align at each stage of the review process, conflicts were resolved by a third member of the team. Reconciliation of these conflicts occurred at our weekly meetings. Title/abstract screening was conducted independently with consensus resolution among the team. We did not calculate inter-rater reliability. However, through a collaborative process, 100% agreement was achieved by at least two members of the team.
Through Covidence, each of the first five authors of this review utilized a review protocol and completed a data extraction of the following components: (a) method of research, (b) participant information, (c) barriers identified, and (d) bioecological factors. Data-extraction occurred individually at first, and then collectively until the team reached full consensus. We did not monitor or formally calculate the inter-rater reliability with formal statistics because we achieved 100% consensus after each data extraction among the first five authors as a research collective.
Table 1 shows the codebook definitions used by the research team for consistency during the extraction stage. After the identification of all the articles, the first author identified all the barriers from the perspective of people with ID within the article. The first and second authors reviewed the barriers identified and applied the concepts of the PPCT model to identify the bioecological factors. The authors coded each barrier with a component of the PPCT model (which often involved studies including more barriers across two more portions of the PPCT model). Through an iterative process, the authors ensured the understanding of the contextual information surrounding the barriers to best identify the PPCT component. When conflicts occurred, the first and second authors went back to the original article and consulted the primary article to best determine the PPCT component. We did not compute a formal reliability coefficient for PPCT coding; however, through this iterative process and consultation with the original article, at least two members of the research team reached a 100% agreement.

Table 1.
This table shows the codebook used by the research team during extraction.
4. Results
The database search yielded 23,379 articles after duplicates were removed. A review of titles and abstracts resulted in 195 studies to be reviewed for full text. During the full text review, 30 articles met the inclusionary criteria. Figure 1 provides a PRISMA flow diagram outlining the review process.
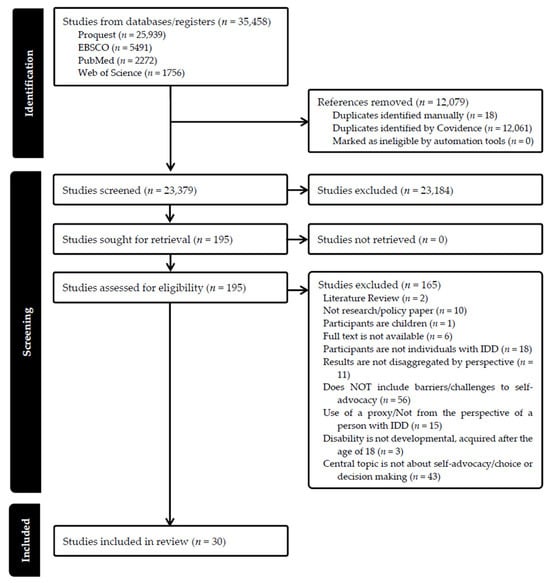
Figure 1.
This PRISMA Flow Diagram shows the various stages of this scoping review, and the number of studies retained at each stage.
4.1. Study Samples and Methodological Approaches
Table 2 provides study locations, methodologies, and self-advocacy related topics under investigation. Studies were conducted in 13 countries (inclusive of two studies conducted in multiple countries). Of the 30 articles reviewed, the (n = 28) employed qualitative methods, and, of these 28 studies, about 28%, (n = 8) implemented participatory methods or approaches. One study utilized survey and qualitative methods, and one study employed a mixed method case study.
Table 2.
This table displays study location, methodology, and study topic for included studies.
Participant Information
Of the 30 studies, 19 studies reported participants with intellectual disability only (#1, #2, #3, #4, #7, #9, #11, #14, #15, #16, #17, #19, #20, #23, #25, #26, #27, #28, #29). Nine studies reported participants had intellectual disability and developmental disabilities or other co-cooccurring disabilities (#5, #8, #10, #12, #13, #18, #21, #24, #30). One study used the UK’s term “learning disability” for intellectual disability (#6). One study used the term “Down Syndrome” to describe participants’ disability (#22). Of the 30 studies, 19 reported dichotomous participant gender demographics (#1, #4, #6, #7, #9, #11, #14, #16, #17, #18, #19, #20, #22, #23, #24, #26, #27, #29, #30) and only three studies (10%) reported diverse gender identities (e.g., used gender-expansive terminology; #10, #13, #25). These three studies were the only ones who investigated intersections between demographics (i.e., race, gender, sexuality). Thirteen studies reported the places in which participants lived (i.e., at home with family, independent, group home, supported (#4, #6, #7, #9, #11, #15, #16, #17, #20, #21, #22, #25, #30). Only 8 studies (26.6%) reported race demographics (#6, #8, #10, #13, #21, #23, #24, #30). Ten studies reported the services participants accessed (i.e., day programs, Medicaid waiver services [#1, #5, #6, #12, #13, #14, #17, #23, #25, #27]). Two studies identified that the participants were active in a self-advocacy group (#2, #13), and one study identified if the participants were engaged in social activities (#3). Eight studies identified co-occurring neurodevelopmental disorders and/or mental health conditions (e.g., ADHD, anxiety, bipolar; [#8, #10, #12, #13, #18, #21, #24, #30]). Regarding age, five articles identified the age of the participants as 18 and older (#2, #10, #11, #17, #25). Five articles reported young adults within the range of 18–40, (#3, #14, #22, #24, #30). Ten articles considered middle age between a participant’s 20s to 50s (#1, #4, #7, #9, #12, #13, #20, #21, #28, #29). Three articles had participants with age of participants including a range of 18–70 (#6, #8, #16). Two articles had participants with an age range of 40–80 (#26, #27). Five articles had participants whose age ranged from 22 to 65 years old (#5, #15, #18, #19, #23).
4.2. Barriers Identified Within PPCT Model
4.2.1. Person
Table 3 displays the 11 articles identified barriers involving the person with ID (#7, #9, #18, #19, #20, #21, #22, #23, #24, #25, #28). Examples of barriers within this level are self-imposed limits to decision-making due to their capacity for independent decision-making (#7), a desire to be ‘normal’ (#9), communication challenges such as difficulty talking about abuse or speaking when others are upset (#9, #21), needing assistance to complete tasks (e.g., scheduling an appointment, attaining transportation, navigating complex systems such as insurance or social services [#18]), recognizing or assessing their own health concerns (#19), not feeling prepared for living or working independently (#20 #22), not having the social, emotional, or self-regulation skills to manage anxiety or fear (#25, #28), not knowing how to achieve goals/dreams (#23), sensory needs (e.g., noise aversion [#21]), hearing, speech, or physical limitations (#24), and poverty (#22).
Table 3.
This table displays PPCT Model components represented across studies.
4.2.2. Microsystem
As demonstrated in Table 3, 25 studies identified barriers within the microsystem (#1, #2, #4, #5, #6, #7, #8, #9, #10, #11, #12, #13, #14, #16, #17, #20, #21, #22, #23, #25, #26, #27, #28, #29, #30). Notably, only one study, #14, referenced teachers as part of a microsystem barrier—the rest universally referenced family members (e.g., parents, siblings) and direct support providers (e.g., residential support staff). Fifteen studies reported barriers related to the constrainment of decision-making regarding social engagement, employment, finances, living arrangements, and sexuality and relationships and assuming authority (#1, #2, #4, #5, #6, #7, #8, #10, #11, #12, #14, #16, #17, #26, #29). Similarly, three studies indicated that families or direct service providers required participants with ID to seek permission to make daily decisions or to engage in relationships (#9, #12, #29). In addition, two studies reported barriers related to a reliance on families for financial and logistical support such as transportation (#1, #21) and five studies described family and direct service provider overprotection such as unnecessary over-assistance and not allowing participants with ID or make decisions that they perceive as incorrect or risky which led to tension and dependence (#1, #8, #17, #23, #28). Four studies expanded on the ways in which conflict with family members or direct service providers (e.g., controlling siblings, disagreeing with rules) diminished opportunities for self-advocacy (#7, #11, #12, #22).
Seven studies focused on barriers in education, including families and service providers limiting education about adult concepts such as financial planning, health literacy, sexuality, transportation (#1, #9, #10, #14, #16, #17, #26). Studies also reported families or direct service providers not supporting advocacy (#13), dismissing or limiting self-advocacy efforts that they perceived disruptive to routines or expected behaviors (#2, #11, #16), and ignoring self-advocacy efforts (#2, #11, #12, #16, #21, #29, #30) or gender and sexuality identities (#10, #25). Additional barriers within the microsystem included low expectations among family and direct service providers, such as: (a) assuming there is no need to include people with ID in meetings about their future (#2, #4, #29), (b) assuming people with ID are incapable of choice-making (#2), and (c) not believing people with ID can achieve their goals and dreams (#23). In addition, misaligned desires/decisions among family members or direct service providers and the person with ID (#7, #11, #12, #22) and bullying by peers, family, or direct service providers (#5, #22, #23, #26) as barriers to self-advocacy.
These studies reflected proximal processes occurring within microsystem structures. For example, the act of family members or direct service providers preventing a person with ID to make financial decisions or health decisions disallowed them from self-advocating and completing tasks independently (#2, #4, #8, #12, #13, #14, #16, #17, #23, #29). Likewise, participants with ID indicated that family members or direct service providers ignored or silenced their advocacy efforts (#2, #11, #12, #16, #21, #29, #30) or made decisions for the person with ID (#7, #9, #14, #20, #27, #29, #30).
4.2.3. Mesosystem
The mesosystem refers to interactions between two or more microsystem structures (Bronfenbrenner, 2005; Bronfenbrenner & Morris, 2007; Tudge et al., 2022). There were two articles (n = 2) that identified barriers falling within the mesosystem (#3, #11). These studies identified barriers where the individual with ID was ignored or undervalued while the community person (i.e., doctor or news reporter) addressed the non-disabled person or caregiver accompanying the person with ID.
4.2.4. Exosystem
Twenty-nine studies identified barriers within the exosystem (#1, #2, #3, #4, #5, #6, #8, #9, #10, #11, #12, #13, #14, #15, #16, #17, #18, #19, #20, #21, #22, #23, #24, #25, #26, #27, #28, #29, #30) (See Table 3). Identified barriers focused on structural constraints such as organizational culture, hierarchies, and policies impacting people with ID including: (a) systemic issues such as staff turnover among service providers (#2, #6, #14, #16, #17, #20, #28), (b) a lack of familiarity or knowledge about the participant among staff due to ineffective policies (#5, #6), (c) inaccessible or unavailable organization staff (#15, #20, #29, #30), (d) policies that block or disregard voices of people with ID (#9, #11), and (e) a lack of resources (#15, #16, #23). Participants with ID were also limited by (a) services that were planned around the service organization, rather than being person-centered and led by individuals with ID (#2, #5, #6, #9, #12, #25) and practices and policies that infringed on personal freedoms such as making decisions about relationships, living spaces, or activities (#1, #13, #17, #21). Six studies also reported systemic financial barriers due to not being paid enough through Social Security Income (#11, #15) and limited employment opportunities (#4, #22, #24, #29). Individuals with ID also reported barriers within the healthcare system, including negative interactions with healthcare providers (#18, #19, #30), lack of approachability from providers and feeling rushed during appointments (#18, #19), lack of accommodations (#19, #30), and difficulty navigating the healthcare system (#18, #19, #30). Eleven studies reported barriers related to feeling isolated or excluded by policies, practices, or outward discrimination by structures such as community employers, group homes, and social settings such as LGBT+ affinity groups (#3, #8, #9, #10, #13, #15, #16, #21, #26, #27, #28).
4.2.5. Macrosystem
Table 3 shows the 13 studies that included barriers within the macrosystem (#1, #2, #3, #4, #5, #9, #10 #11, #12, #13, #16, #25, #26). Thirteen studies identified ableism and discrimination (#1, #2, #3, #4, #5, #9, #10, #11, #12, #13 #16, #25, #26) as negatively impacting participants. For example, participants in study #3 described the implications of “battling disability” to advocate (p. 440), and participants in study #4 described the stigma associated with being in the community with other people with disabilities. Similarly, three studies reported additional discriminatory practices based on their race or sexuality, including being perceived as dangerous or deviant as a Black male with ID (#10, #13). Participants with ID further described how overarching ableism and stigma associated with disability and other historically marginalized identities (e.g., minoritized races, sexualities) contributed to low income and employment opportunities (#16), families and service providers maintaining low expectations and denying rights (#12, #16), and the lack of consideration of the needs and perspectives of individuals with ID within service systems (#11).
4.2.6. Chronosystem
Table 4 shows three studies that identified barriers in the chronosystem (#5, #20, #26). Barriers identified within this system included a decline of natural support as parents age (#5), as well as participants’ social networks (e.g., school, sports, leisure, employment) declining over time (#20). Additionally, #26 identified that participant aging impacted health and independence over time.
Table 4.
This table includes the different barriers identified in the studies in categories and subcategories. It also includes the number of studies referenced.
5. Discussion
The objective of this scoping review was to understand barriers identified by people with ID across the globe and understand how people with ID experience these barriers through the PPCT model of human development. The research team identified various barriers to self-advocacy from the perspective of people with ID, including challenges a person experiences (e.g., not having a specific skill), relational conflicts among family or service providers, structural barriers in how services are implemented, societal beliefs and expectations, and barriers due to aging. People with ID have the capability and power to advocate for their wants and needs, and the people (e.g., parents, families, caregivers, service providers) and the systems (e.g., education, adult service providers) that support people have a responsibility to understand the ways in which they hinder and support self-advocacy.
5.1. Notable Findings
This scoping review included articles from 13 countries providing support that barriers to self-advocacy is not a US-specific problem, but an international phenomenon. Studies most commonly occurred, however, in Europe (primarily in western Europe) North America (US and Canada), and Australia. Only one study occurred in Asia (Taiwan), and no studies occurred in South America or Africa (see Table 2). This may be, in part, because of differing cultural perceptions of disability and expectations for self-advocacy, individualistic vs. collective societies, the existence and/or nature of disability policies, as well as resources available in high vs. medium/low-income countries (Abera et al., 2025). Further, over half of the studies were published between 2019 and 2025. This further reinforces that investigating self-advocacy from the perspectives of people with ID is a relatively recent topic of investigation. Despite limited international representation in this review, the represented countries are far from a monolith, which increases the potential to advance an understanding of commonly experienced barriers across countries. In addition, Table 2 displays the wide variety of topics under investigation (e.g., sexuality, decision-making, parenting, healthcare), which further reinforces the importance of considering the barriers identified in this scoping review across compressive aspects of self-advocacy within community living and participant contexts (e.g., employment, education, relationships, living arrangements) at every level of the PPCT model of human development. On the other hand, the majority of studies included in this review utilized qualitative methods (see Table 2). Although qualitative research is not intended to be generalized (Maxwell, 2022), it is important to again consider the influence of specific cultures, communities, and policies when considering the applicability to findings. Conversely, nearly 30% of the qualitative studies incorporated participatory research methods (i.e., #1, #6, #10, #11, #13, #16, #25, #28) and the other two studies incorporated qualitative and quantitative approaches to data collection and analysis. Research in partnership with people with ID that is by, for, and with, rather than on people with ID, centers their voices and empowers people with ID (Balcazar et al., 1998; Call-Cummings et al., 2024). Additionally, partnering with people with ID through participatory approaches to share in the power of developing research questions, collecting data, and making meaning of the data can enhance participation, and also centers the research design, implementation, and meaning-making with and by people with ID (Balcazar et al.,1998; Call-Cummings et al., 2024). In short, although the studies identified in this review are not globally or methodologically representative, reciprocal learning among an international community has the potential to expedite more effective and meaningful self-advocacy research and practices.
Organizing barriers within PPCT model can inform ways in which to address the most salient issues compromising self-advocacy. Participants most frequently identified barriers within the exosystem (structures that indirectly influenced the person with ID; see Table 4) such as organizational culture, hierarchies, policies, and staff turnover (see Table 4). Exosystem barriers identified in this review reflect overwhelming evidence of disparate occurrences of community living and participation outcomes such as (a) competitive employment, (b) postsecondary education, (c) community living, and (d) relationships and community contemporaries are not comparable to other populations (ACL, n.d.; McCallion et al., 2023; Milot et al., 2021). In addition, the microsystem, including proximal processes (i.e., interactions and perceptions of family members, service providers) was the second most frequent context in which barriers occurred (see Table 4). Decades of research documents the influence of family members and direct service providers have on the outcomes of individuals with ID, as these individuals often look to families and direct service providers for guidance and support (e.g., Friedman, 2022; Luitwieler et al., 2021; McCausland et al., 2021; Milot et al., 2021; Turnbull et al., 2022). Unfortunately, barriers associated with these structures were among the most prevalent barriers reported (e.g., assuming authority, overprotection, low expectations; see Table 4). In addition, educators are also key microsystem structures found to influence self-advocacy and post-school outcomes among individuals with ID (Ferlazzo, 2022). Interestingly, apart from some minor discussion in #14, educators did not emerge as a key barrier to self-advocacy in this review, despite research indicating that school-related barriers such as low expectations among educators often forestalls self-advocacy among individuals with ID (Buchner et al., 2021; Gross et al., 2025; Francis et al., 2020). Although the absence of discussions on educators contributing to barriers to self-advocacy is encouraging, the age of participants (ranging from 18 to 80 across studies) may have curbed discussions about school. Similarly, a large body of research reports the negative impact of limited communication and collaboration among families, educators, and service providers (i.e., interactions found within the mesosystem), as well as interagency communication and collaboration on community living and participation outcomes among individuals with ID (Gross et al., 2025; McCausland et al., 2021). It is surprising that so few studies identified barriers within this system (n = 2).
Finally, intersectionality focuses on the intersection of the constructs of race, class, ability, gender, culture, and sexual orientation with power and privilege (Collins, 2019). Of the 30 articles examined, only eight reported on the race of their participants. Over 60% (n =19) of studies reported the sex of their participants in dichotomous gender, and only three articles included gender expansive terms (#10, #13, #25). Eight articles did not report on gender. The lack of robust reporting of participants’ identities, culture, race, gender, and class creates a barrier to understanding the intersectional experiences of Disabled people including people with ID. Participants in the three studies that did examine these intersections (#10, #13, #25) identified that race and/or sexual identity (e.g., gender and sexual identity being dismissed by service provider or families, self-advocacy regarding self-expression being rejected and limited, fear of discrimination), resulting in overlapping and interlocking forms of discrimination and oppression across the PPCT contexts. Identifying and naming such inequalities within society is the first step in understanding how power and social injustices exist and are reproduced.
5.2. Implications for Future Research
Although the pervasive existence of barriers to self-advocacy is acknowledged in the disability field (Nowakowska & Pisula, 2021; Shogren & Raley, 2022), this scoping review only yielded 30 articles that reported barriers that prevented or stymied self-advocacy from the perspective of those most impacted, people with ID. This lack of information compromises the meaningfulness and efficacy efforts to enhance self-advocacy (e.g., curriculum, interventions, policies), if they do not address underlying barriers that Disabled people identify as impacting self-advocacy. Further, Asian, Latin/South American, and African studies were not represented in this review, highlighting a need for international research. Further, most articles in this review utilized qualitative methods, which is an important way to support the voices of people with ID (Call-Cummings et al., 2024). Increased use of mixed methods (e.g., questionnaire, sorting, photovoice, adapted research methods) may enhance participation among people with ID in self-advocacy research (Glaser & Strauss, 1966). Service providers play important roles in the lives of people with ID. Despite the literature and public policies supporting and advocating for collaboration among families, educators, and professionals (Kinnunen et al., 2023; Lokman et al., 2023), this review uncovered few barriers within the mesosystem. Future research should continue to investigate the ways in which people with ID view collaboration and how collaboration grounded in encouraging and honoring self-advocacy can not only increase quality life but can also address barriers such as ableist policies and service systems. In addition, although barriers related to proximal processes were well-defined within the studies included in this scoping review, there was no discussion of the interactions within other systems or descriptions of the “trickle down” effect of ableism and discrimination on other factors such as policies within the exosystem, low expectations among microsystem structures, or internalized ableism by the person at the center of the PPCT model. More deeply understanding the relationships between and bidirectionality of barriers identified in this review can inform practices to disrupt pathways the perpetuate barriers.
Examining the nature of barriers to self-advocacy among ID demands a critical lens. Future research needs to utilize critical perspectives to understand the structural oppression, which exists for Disabled people and specifically for people with ID. The use of critical theories such as DisCrit, intersectionality, and/or critical disabilities studies can help examine barriers to self-advocacy. Because disability is a human experience (Heumann & Joiner 2020; Linton, 1998) that impacts people from all classes, genders, sexualities, and races, disability issues demand an intersectional lens (Harkins Monaco et al., 2024). Together, intersectionality and the PPCT model advance the understanding of the complexity of human development with a critical lens. Intersectionality uncovers the systems of power based on one’s intersecting identities, powers, and relational processes (Collins, 2019). DisCrit (Annamma et al., 2013) utilizes both critical race theory and intersectionality and its tenets consider the forces of racism and ableism to challenge the notions of normalcy, while privileging the multiple identities, experiences, and voices of Disabled people.
5.3. Implications for Practice and Policy
Individuals with ID often report that family members, especially parents, are key supports (e.g., advocacy; Francis et al., 2020), as well as sources of tension and conflict (as noted in this review). Given that families are the first and most consistent supporters in a person’s life, focusing on teaching families how to support self-advocacy among their children with ID from an early age has the potential to maximize the natural long-term support families provide. Person-centered planning (e.g., Making Action Plans, Circles of Support) is one culturally responsive research-based approach to creating collaborative, sustainable systems of support built around the needs, goals, preferences, and priorities of an individual with ID (Haines et al., 2017; Lockman Turner et al., 2022). This approach has the potential to mitigate many barriers to self-advocacy identified in this review (e.g., dismissal of advocacy efforts, constraint, limited opportunities for decision-making), by centering all planning decisions on the input of individuals with ID. Likewise people with ID engaging in daily supported decision-making is another approach to honor the interdependent nature of decision-making of all people by providing an intentional way Disabled people, particularly those with ID, and their allies can collaboratively discern choices (The Center for Public Representation, 2025), within and outside of meetings. In addition, dignity of risk, or a person’s right to make choices and take reasonable risks to live a self-directed life (Mental Health and Developmental Disabilities National Training Center, 2020), is an additional approach to that can prevent or counteract overprotection among families and direct service providers, a frequently cited microsystem barrier (see Table 4). In addition, professionals (e.g., educators, service providers, administrators) would benefit from professional development in ways to recognize and address ableism and other systemic forms of discrimination associated with race, heteronormativity, and other social constructs leading to systematic oppression. Such programs may include addressing implicit biases and positionality/reflexivity practices. Training for families, educators, and service programs can address how to acknowledge and value the intersectionality of people with ID through identifying their many identities of race, gender, sexual orientation, and cultural background (Harkins Monaco et al., 2024), and how people within the microsystem can reflect and build critical consciousness identifying the systemic barriers impacting these individuals and work within their own capacity to dismantle them (Collins, 2019). Barriers within this review included dismissal of gender or sexuality identity, people experiencing both racism and ableism, which indicated layered oppression (Collins, 2019).
Results from this scoping review also hold policy implications (see Table 5), including the potential for calling for person-centered planning approaches and supportive decision-making into education, service organizations, and healthcare policies and practices. In the same vein, service providers and healthcare providers require higher education preparation and/or professional development to support self-advocacy among individuals with ID.
Table 5.
This table includes implications for practitioners and policy makers within the PPCT Framework.
5.4. Limitations
First, the research team excluded the literature not written in English, subsequent studies that may have occurred since the database search in spring 2025, and other forms of publication influenced by the pool of analyzed information. Further, although the research team included “learning disability” (a phrase used for ID in the UK and Australia), they did not include this phrase as a search term. Additionally, the research team did not complete forward and backward hand searches, and this could have limited the information. Moreover, it is possible that the search and screening practices may have inadvertently excluded studies that did not include inclusionary criteria within titles and abstracts. When extracting data, the research team pulled the barriers of people with ID from the articles. Some articles utilized multiple perspectives (i.e., dyads), and the researchers only selected the barriers of people with ID mentioned within the article. Additionally, the research team utilized the information represented within the article to determine the PPCT context. Vague descriptions of barriers also may have resulted in the researchers misclassifying a barrier. For example, articles reported bullying or discrimination by “others.” In these instances, however, the researchers returned to the article for greater context to understand the barriers described.
6. Conclusions
Despite international mandates protecting self-advocacy as a fundamental human right, people with ID continue to encounter compounding layers of systemic barriers to enacting their agency. With self-advocacy serving as a critical driver to an individual’s quality of life, it is imperative to identify and redress the environmental barriers and ableist ideologies that perpetuate the exclusion and silencing of the Disability community. Therefore, the purpose of this scoping review was to center the perspectives of people with ID to identify barriers to self-advocacy, thus understanding current exclusionary approaches to self-advocacy while challenging the field’s historical reliance on proxy reports.
In analyzing the barriers identified by the Disability community through the PPCT model, this review found the majority of barriers exist predominantly in the exosystem (e.g., policies, staff turnover, etc.) and the microsystem (e.g., low expectations, overprotection, etc.). While these barriers exist in an individual’s external system, their limiting effects trickle down into the individual’s microsystem through the proximal, reciprocal processes that are influenced by ableist ideologies and other systems of oppression.
Furthermore, this scoping review highlights the current limited understanding of the barriers to self-advocacy for the Disability community due to a lack of identifying and analyzing intersectionality in research practices, as well as lack of global representation. To more comprehensively understand the lived reality of people with ID and the breadth of barriers that inhibit one to self-advocate, future research must examine how intersecting identities, especially multiply marginalized identities, compound the layers of barriers that individuals experience.
Self-advocacy cannot be actualized through interventions that solely target the individual, rather it requires a collective commitment to redesigning exclusionary practices and environments by removing barriers, prioritizing the ones identified in this review. By centering the perspectives and voices of people with ID in this process, researchers and practitioners can advance beyond the dehumanizing and ableist practices of problematizing the individuals and begin the necessary and critical work of problematizing and fixing systems.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/educsci16010097/s1, File S1: Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR).
Author Contributions
Conceptualization, C.D.E., G.L.F.; methodology, C.D.E., G.L.F., K.C.-R.; validation, C.D.E., G.L.F., K.C.-R.; formal analysis, C.D.E., G.L.F., K.C.-R., K.H., S.H.E.; investigation, C.D.E., G.L.F., K.C.-R., K.H., S.H.E., J.D., J.A.H., E.M., T.J.E.; data curation, C.D.E., G.L.F., K.C.-R.; writing—original draft preparation, C.D.E., G.L.F., K.C.-R., K.H., writing—review and editing, C.D.E., G.L.F., K.C.-R., K.H., E.M., S.H.E., J.D., J.A.H.; visualization, C.D.E., G.L.F., K.C.-R.; supervision, C.D.E., G.L.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
We thank our research librarian, Christopher Lowder, for his assistance, feedback, and support. We thank the research investigative team for their support and dedication to article screening.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ID | Intellectual Disability |
| PPCT | Process-person-context-time |
| US | United States |
References
- Abera, M., Francis, G. L., Nega, A., Dawud, S., Ali, M., Shibabaw, G., Araya, B., Haines, S., & Aldersey, H. M. (2025). Collaboration for the inclusion of students with disabilities in K-12 education in Gondar, Ethiopia. African Journal of Disability, 14, 1–11. [Google Scholar] [CrossRef]
- ACL. (n.d.). Improving the lives of older adults and people with disabilities through services, research, and education. Administration of Community Living. Available online: https://acl.gov/sites/default/files/news%202019-01/FinalCityACLIGPrint.pdf (accessed on 28 September 2025).
- Alsaeed, A., Mansouri, M. C., Shogren, K. A., Raley, S. K., Kurth, J. A., Leatherman, E. M., & Lockman Turner, E. (2023). A systematic review of interventions to promote self-determination for students with extensive support needs. Research and Practice for Persons with Severe Disabilities, 48(1), 3–24. [Google Scholar] [CrossRef]
- Annamma, S. A., Connor, D., & Ferri, B. (2013). Dis/ability critical race studies (DisCrit): Theorizing at the intersections of race and dis/ability. Race Ethnicity and Education, 16(1), 1–31. [Google Scholar] [CrossRef]
- Avellone, L., Camden, J., Taylor, J., & Wehman, P. (2021). Employment outcomes for students with intellectual disabilities in postsecondary education programs: A scoping review. Journal of Postsecondary Education and Disability, 34(3), 223–238. Available online: https://files.eric.ed.gov/fulltext/EJ1325428.pdf (accessed on 28 September 2025).
- Azzopardi-Lane, C., & Callus, A. M. (2014). Constructing sexual identities: People with intellectual disability talking about sexuality. British Journal of Learning Disabilities, 43(1), 32–37. [Google Scholar] [CrossRef]
- Balcazar, F. E., Keys, C. B., Kaplan, D. L., & Suarez-Balcazar, Y. (1998). Participatory action research and people with disabilities: Principles and challenges. Canadian Journal of Rehabilitation, 12(3), 105–112. [Google Scholar] [CrossRef]
- Bellon, M., Gendera, S., Robinson, S., Cahalan, T., & Fisher, K. R. (2025). Peer-led self-advocacy for people with intellectual disability through the lens of “freedom through encounter”. Journal of Intellectual & Developmental Disability, 50(1), 1–9. [Google Scholar] [CrossRef]
- Bigby, C., Douglas, J., Smith, E., Carney, T., Then, S. N., & Wiesel, I. (2021). “I used to call him a non-decision-maker-I never do that anymore”: Parental reflections about training to support decision-making of their adult offspring with intellectual disabilities. Disability and Rehabilitation, 44(21), 6356–6364. [Google Scholar] [CrossRef]
- Björnsdóttir, K., & Johannesson, I. A. (2009). People with intellectual disabilities in Iceland: A bourdieuean interpretation of self-advocacy. Intellectual and Developmental Disabilities, 47(6), 436–446. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. (2005). Making human beings human: Bioecological perspectives on human development. Sage. [Google Scholar]
- Bronfenbrenner, U., & Morris, P. A. (1998). The bioecological model of human development. In R. M. Lerner (Ed.), Handbook of child psychology (pp. 993–1027). Wiley and Sons. [Google Scholar]
- Bronfenbrenner, U., & Morris, P. A. (2007). The bioecological model of human development. In W. Damon, & R. M. Lerner (Eds.), Handbook of child psychology (6th ed., Vol. 1, pp. 793–828). John Wiley & Sons, Inc. [Google Scholar] [CrossRef]
- Buchner, T., Shelvin, M., Donovan, M. A., Gercke, M., Goll, H., Šiška, J., Janyšková, K., Smogorzewska, J., Szumski, G., Vlachou, A., Demo, H., Feyerer, E., & Corby, D. (2021). Same progress for all? Inclusive education, the United Nations Convention on the Rights of Person with Disabilities and Students with Intellectual Disability in European Countries. Journal of Policy and Practice in Intellectual Disabilities, 18(1), 7–22. [Google Scholar] [CrossRef]
- Burke, K. M., Shogren, K. A., Parente, A., Alsaeed, A., Myers, A. M., & Aleong, S. (2024). Self-determination research: Current and future directions. Behavioral Sciences, 14(7), 613. [Google Scholar] [CrossRef]
- Call-Cummings, M., Dazzo, G., & Hauber-Özer, M. (2024). Critical participatory inquiry: An interdisciplinary guide. Sage. [Google Scholar]
- Callus, A. M., Bonello, I., Mifusd, C., & Fenech, R. (2019). Overprotection in the lives of people with intellectual disability in Malta: Knowing what is control and what is enabling support. Disability & Society, 34(3), 345–367. [Google Scholar] [CrossRef]
- Carbone, L. A. S. (2016). Autonomy in the California disability services system [Doctoral dissertation, Walden University]. ProQuest Dissertations and Theses Global. [Google Scholar]
- Chapman, M., Bannister, S., Davies, J., Fleming, S., Graham, C., McCaster, A., Seddon, A., Weldon, A., The Better Together Stronger Together Research Team & Whittell, B. (2011). Speaking up about advocacy: Findings from a partnership research project. British Journal of Learning Disabilities, 40, 71–80. [Google Scholar] [CrossRef]
- Chong, K., Cheah, K. J., & Manokara, V. (2024). Our lives, our voices: Impact of self-advocacy program on persons with intellectual developmental disability. Advances in Neurodevelopmental Disorder, 8(1), 42–63. [Google Scholar] [CrossRef]
- Chouinard, V. (1997). Making space for disabling differences: Challenging ableist geographies. Environment & Planning D: Society & Space, 15(4), 379. [Google Scholar] [CrossRef]
- Collins, P. H. (2019). Intersectionality as critical social theory. Duke Press. [Google Scholar]
- Covidence. (2024). [Web-based software]. Available online: https://www.covidence.org/ (accessed on 5 March 2025).
- Crenshaw, K. (1991). Mapping the margins: Intersectionality, identity, politics, and violence against women of color. Stanford Law Review, 43(6), 1241–1299. [Google Scholar] [CrossRef]
- Curryer, B., Stancliffe, R. J., Dew, A., & Wiese, M. Y. (2018). Choice and control within family relationships: The lived experience of adults with intellectual disability. Intellectual and Developmental Disabilities, 56(3), 188–201. [Google Scholar] [CrossRef]
- Dew, A., Collings, S., Dillon Savage, I., Gentle, E., & Dowse, L. (2019). “Living the life I want”: A framework for planning engagement with people with intellectual disability and complex support needs. Journal of Applied Research in Intellectual Disabilities, 32(2), 401–412. [Google Scholar] [CrossRef]
- Ferlazzo, L. (2022, February 27). What teachers have learned since the pandemic closed schools (Opinion). Education Week. Available online: https://www.edweek.org/leadership/opinion-2-years-on-what-have-we-learned-about-teaching-in-a-pandemic/2022/02 (accessed on 11 December 2025).
- Francis, G. L., Reed, A. S., & Howard, M. E. (2020). Interactions with and between families and professionals in college: Perspectives of young adults with intellectual and developmental disabilities. Inclusion, 8(2), 163–179. [Google Scholar] [CrossRef]
- Friedman, C. (2022). The impact of human service provider quality on the personal outcomes of people with intellectual and developmental disabilities. Frontiers in Rehabilitation Sciences, 17(2), 780168. [Google Scholar] [CrossRef]
- Gappmayer, G. (2021). Disentangling disablism and ableism: The social norm of being able and its influence on social interactions with people with intellectual disabilities. Journal of Occupational Science, 28(1), 102–113. [Google Scholar] [CrossRef]
- Glaser, B. G., & Strauss, A. L. (1966). The purpose and credibility of qualitative research. Nursing Research, 15(1), 56–61. [Google Scholar] [CrossRef] [PubMed]
- Grech, L. B., Koller, D., & Olley, A. (2023). Furthering the person-first versus identity-first language debate. Australian Psychologist, 58(4), 223–232. [Google Scholar] [CrossRef]
- Gross, J. M. S., Francis, G. L., Choi, H. J., Stanley, J. L., & Bowen, E. (2025). Professionals need information too: Exploratory data from the Family Employment Awareness Training (FEAT) in Kansas. Inclusion, 13(2), 87–101. [Google Scholar] [CrossRef]
- Groves, E., Rayner, K., & Muncer, S. (2017). “It’s good, they’re like me; the same but different.” An interpretative phenomenological analysis of the identities of women with down’s syndrome. Journal of Applied Research in Intellectual Disabilities, 31(3), 445–453. [Google Scholar] [CrossRef]
- Haines, S. J., Francis, G. L., Shepherd, K., Ziegler, M., & Mabika, G. (2017). Partnership bound: Using MAPS with transitioning students and families from all backgrounds. Career Development and Transition for Exceptional Individuals, 41(2), 122–126. [Google Scholar] [CrossRef]
- Harkins Monaco, E. A., Stansberry Brusnahan, L. L., Fuller, M. C., & Odima, M. (Eds.). (2024). Disability, intersectionality, and belonging in special education: Socioculturally sustaining practices. Rowman & Littlefield. [Google Scholar]
- Heumann, J. E., & Joiner, K. (2020). Being Heumann: An unrepentant memoir of a disability rights activist. Beacon Press. [Google Scholar]
- Hughes, O. E. (2024). Inclusive research to promote gender and sexual self-determination for LGBTQ+ adults with intellectual and developmental disabilities [Doctoral dissertation, Boston University]. ProQuest Dissertations and Theses Global. [Google Scholar]
- Iriarte, E. G., O’Brien, P., McConkey, R., Wolfe, M., & O’Doherty, S. (2014). Identifying the key concerns of Irish persons with intellectual disability. Journal of Applied Research in Intellectual Disabilities, 27(6), 564–575. [Google Scholar] [CrossRef]
- Kinnunen, A., Vesterinen, A., Kippola-Pääkkönen, A., & Karhula, M. (2023). Partnership working among families, therapists and educationalists to enhance collaboration enabling participation of children with intellectual disabilities. Disabilities, 3(3), 396–409. [Google Scholar] [CrossRef]
- Kober, R. (Ed.). (2010). Enhancing the quality of life of people with intellectual disabilities: From theory to practice (Vol. 41). Springer Science & Business Media. [Google Scholar]
- Lee, S. H., Wehmeyer, M. L., & Shogren, K. A. (2015). Effect of instruction with the self-determined learning model of instruction on students with disabilities: A meta-analysis. Education and Training in Autism and Developmental Disabilities, 50(2), 237–247. [Google Scholar] [CrossRef]
- Li, Y. F., Liu, C. T., & Zhao, Y. (2024). Understanding self-determination learning experiences among Taiwanese adults with severe disabilities. Journal of Developmental and Physical Disabilities, 36(6), 1121–1145. [Google Scholar] [CrossRef]
- Linton, S. (1998). Claiming disability: Knowledge and identity. New York University Press. [Google Scholar]
- Lockman Turner, E., Bubash, S., Fialka-Feldman, M., & Hayes, A. (2022). Circles of support and self-direction: An interview highlighting a journey of friendship and managing services. Inclusive Practices, 1(2), 75–78. [Google Scholar] [CrossRef]
- Lokman, S., Frielink, N., Didden, R., & Embregts, P. J. C. M. (2023). Experienced support at work, team climate and collaboration in teams working with people with mild intellectual disabilities and severe challenging behaviour in residential care: A cross-sectional study. Journal of Intellectual Disability Research, 67(8), 782–795. [Google Scholar] [CrossRef]
- Luitwieler, N., Luijkx, J., Salavati, M., Van der Schans, C. P., Van der Putten, A. J., & Waninge, A. (2021). Variables related to the quality of life of families that have a child with severe to profound intellectual disabilities: A systematic review. Heliyon, 7(7), e07372. [Google Scholar] [CrossRef]
- Maxwell, J. A. (2022). Generalization as an issue for qualitative research design. In The SAGE handbook of qualitative research design (Vol. 2, pp. 327–338). SAGE Publications Ltd. [Google Scholar] [CrossRef]
- McCallion, P., Carroll, R., & McCarron, M. (2023). Barriers to community participation for adults aging with an intellectual disability in Ireland: A longitudinal study. Inclusion, 11(3), 204–217. [Google Scholar] [CrossRef]
- McCausland, D., Murphy, E., McCarron, M., & McCallion, P. (2021). The potential for person-centred planning to support the community participation of adults with an intellectual disability. Journal of Intellectual Disabilities, 26(3), 603–623. [Google Scholar] [CrossRef] [PubMed]
- Mental Health and Developmental Disabilities National Training Center. (2020). Self-determination & dignity of risk. Available online: https://www.mhddcenter.org/wp-content/uploads/2020/07/Self-Determination-Dignity-of-Risk-Fact-Sheet.pdf (accessed on 11 November 2025).
- Miller, A. L., Frye, D., Green, T., Mitchell, C., Garcia, G., Huereña, J., Moore, T., & Turnage, V. (2022). (Re) defining their place at the table: Frank discussions by adults with disabilities on contemporary self-advocacy. Journal of Applied Research in Intellectual Disabilities, 35(3), 777–788. [Google Scholar] [CrossRef]
- Milot, E., Couvrette, R., & Grandisson, M. (2021). Perspectives of adults with intellectual disabilities and key individuals on community participation in inclusive settings: A Canadian exploratory study. Journal of Intellectual & Developmental Disability, 46(1), 58–66. [Google Scholar] [CrossRef]
- Mogensen, L. L., Drake, G., McDonald, J., & Sharp, N. (2024). Young people with intellectual disability speak out about life after school: “I want to do more in life than just… be a disability person”. Journal of Intellectual & Developmental Disability, 49(2), 121–133. [Google Scholar] [CrossRef]
- Munn, Z., Peters, M. D., Stern, C., Tufanaru, C., McArthur, A., & Aromataris, E. (2018). Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Medical Research Methodology, 18(1), 143. [Google Scholar] [CrossRef] [PubMed]
- Nario-Redmond, M. R. (2019). Ableism: The causes and consequences of disability prejudice. John Wiley & Sons, Incorporated. [Google Scholar] [CrossRef]
- Nielsen, K. E. (2012). A disability history of the United States (Vol. 2). Beacon Press. [Google Scholar]
- Nonnemacher, S. L., & Bambara, L. M. (2011). “I’m supposed to be in charge”: Self-advocates’ perspectives on their self-determination support needs. Intellectual and Developmental Disabilities, 49(5), 327–340. [Google Scholar] [CrossRef]
- Nowakowska, I., & Pisula, E. (2021). Self-advocates with intellectual disability about their work as social educators—A qualitative polish study. Qualitative Research in Education, 10(1), 1–30. [Google Scholar] [CrossRef]
- Parchomiuk, M., Żyta, A., & Ćwirynkało, K. (2025). Challenges ahead: Exploring external barriers to self-determination in individuals with intellectual disabilities. Research in Developmental Disabilities, 156, 104895. [Google Scholar] [CrossRef] [PubMed]
- Patin, B., Sebastian, M., Yeon, J., & Bertolini, D. (2020). Toward epistemic justice: An approach for conceptualizing epistemicide in the information professions. Proceedings of the Association for Information Science and Technology, 57(1), e242. [Google Scholar] [CrossRef]
- Peters, M. D. J., Marnie, C., Tricco, A. C., Pollock, D., Munn, Z., Alexander, L., McInerney, P., Godfrey, C. M., & Khalil, H. (2020). Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Synthesis, 18(10), 2119–2126. [Google Scholar] [CrossRef]
- Petner-Arrey, J., & Copeland, S. R. (2015). ‘You have to care.’ Perceptions of promoting autonomy in support settings for adults with intellectual disability. British Journal of Learning Disabilities, 43(1), 38–48. [Google Scholar] [CrossRef]
- Potvin, L. A., Fulford, C., Ouellette-Kuntz, H., & Cobigo, V. (2019). What adults with intellectual and developmental disabilities say they need to access annual health examinations: System navigation support and person-centered care. Canadian Family Physician, 65(Suppl. S1), S47–S52. [Google Scholar]
- Pouls, K. P., Mastebroek, M., Ligthart, S. J., Assendelft, W. J., Leusink, G. L., & Koks-Leensen, M. C. (2024). Primary mental healthcare for adults with mild intellectual disabilities: Patients’ perspectives. European Journal of General Practice, 30(1), 2354414. [Google Scholar] [CrossRef]
- Puyaltó, C., & Pallisera, M. (2020). Living independently in Spain: Barriers and supports from the views of people with intellectual disabilities. International Journal of Disability, Development and Education, 67(3), 306–319. [Google Scholar] [CrossRef]
- Raley, S. K., Mumbardó-Adam, C., Shogren, K. A., Simó-Pinatella, D., & Giné, C. (2018). Curricula to teach skills associated with self-determination: A review of existing research. Education and Training in Autism and Developmental Disabilities, 53(4), 353–362. [Google Scholar] [CrossRef]
- Rembis, M., Kudlick, C., & Nielsen, K. E. (Eds.). (2018). The Oxford handbook of disability history. Oxford University Press. [Google Scholar] [CrossRef]
- Ruef, M. B., & Turnbull, A. P. (2002). The perspectives of individuals with cognitive disabilities and/or autism on their lives and their problem behavior. Research and Practice for Persons with Severe Disabilities, 27(2), 125–140. [Google Scholar] [CrossRef]
- Schalock, R. L., Verdugo, M. A., Jenaro, C., Wang, M., Wehmeyer, M., Jiancheng, X., & Lachapelle, Y. (2005). Cross-cultural study of quality of life indicators. American Journal on Mental Retardation, 110(4), 298–311. [Google Scholar] [CrossRef]
- Schweik, S. M. (2009). The ugly laws: Disability in public (Vol. 3). NYU Press. Available online: http://www.jstor.org/stable/j.ctt9qgf13 (accessed on 17 August 2025).
- Scott, M., Foley, K. R., Bourke, J., Leonard, H., & Girdler, S. (2014). “I have a good life”: The meaning of well-being from the perspective of young adults with Down Syndrome. Disability and Rehabilitation, 36(15), 1290–1298. [Google Scholar] [CrossRef]
- Shogren, K. A., & Broussard, R. (2011). Exploring the perceptions of self-determination of individuals with intellectual disability. Intellectual and Developmental Disabilities, 49(2), 86–102. [Google Scholar] [CrossRef]
- Shogren, K. A., & Raley, S. K. (Eds.). (2022). Self-determination and causal agency theory: Integrating research into practice. Springer. [Google Scholar] [CrossRef]
- Shogren, K. A., Wehmeyer, M. L., & Singh, N. N. (Eds.). (2017). Handbook of positive psychology in intellectual and developmental disabilities: Translating research into practice. Springer. [Google Scholar] [CrossRef]
- Sinclair, J., Gilson, C. B., & Dulas, H. (2024). “I’m going to be a working person”: Self-determination in employment settings for adults with intellectual and developmental disabilities. Career Development and Transition for Exceptional Individuals, 47(3), 159–171. [Google Scholar] [CrossRef]
- Smith, E. M., Zirnsak, T. M., Bartlett, K., Power, J., & Bigby, C. (2024). ‘Because it’s who I am’: Self-determination of LGBTQ adults with intellectual disability. Disability & Society, 40(7), 1990–2010. [Google Scholar] [CrossRef]
- Smith, I., & Mueller, C. O. (2022). The importance of disability identity, self-advocacy, and disability activism. Inclusive Practices, 1(2), 47–54. [Google Scholar] [CrossRef]
- Strnadová, I. (2019). Transitions in the lives of older adults with intellectual disabilities: “Having a sense of dignity and independence”. Journal of Policy and Practice in Intellectual Disabilities, 16(1), 58–66. [Google Scholar] [CrossRef]
- Strnadová, I., & Evans, D. (2015). Older women with intellectual disabilities: Overcoming barriers to autonomy. Journal of Policy and Practice in Intellectual Disabilities, 12(1), 12–19. [Google Scholar] [CrossRef]
- Test, D. W., Fowler, C. H., Wood, W. M., Brewer, D. M., & Eddy, S. (2005). A conceptual framework of self-advocacy for students with disabilities. Remedial and Special Education, 26(1), 43–54. [Google Scholar] [CrossRef]
- The Arc of the United States. (2019). Quality of life. Available online: https://thearc.org/position-statements/quality-of-life-summary/ (accessed on 20 August 2025).
- The Center for Public Representation. (2025). About supported decision–making. Available online: https://supporteddecisions.org/about-supported-decision-making/ (accessed on 17 November 2025).
- Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., & Levac, D. (2018). PRISMA extension for scoping reviews (PRISMAScR): Checklist and explanation. Annals of Internal Medicine, 169(7), 467–473. [Google Scholar] [CrossRef] [PubMed]
- Tudge, J. R. H., Merçon-Vargas, E. A., & Payir, A. (2022). Urie Bronfenbrenner’s bioecological theory: Its development, core concepts, and critical issues. In K. Adamsons, A. L. Few-Demo, C. Proulx, & K. Roy (Eds.), Sourcebook of family theories and methodologies. Springer. [Google Scholar] [CrossRef]
- Turnbull, A., Turnbull, R., Francis, G. L., Burke, M., Kyzar, K., Haines, S. J., Gershwin, T., Shepherd, K. G., Holdren, N., & Singer, G. (2022). Families and professionals: Trusting partnerships in general and special education (8th ed.). Pearson. [Google Scholar] [CrossRef]
- United Nations Convention on the Rights of Person with Disabilities. (2016, December 13). Available online: https://social.desa.un.org/issues/disability/crpd/convention-on-the-rights-of-persons-with-disabilities-crpd (accessed on 1 January 2026).
- United Nations Educational, Scientific and Cultural Organization (UNESCO) & España. Ministerio de Educación y Ciencia. (1994). The salamanca statement and framework for action on special needs education. Available online: https://unesdoc.unesco.org/ark:/48223/pf0000098427 (accessed on 11 November 2025).
- Vaucher, C., Cudré-Mauroux, A., & Piérart, G. (2020). Environmental, personal, and relational barriers and facilitators to self-determination among adults with intellectual disabilities. Scandinavian Journal of Disability Research, 22(1), 97–107. [Google Scholar] [CrossRef]
- Wass, S., Safari, M. C., Haugland, S., & Omland, H. O. (2021). Transitions from school to sheltered employment in Norway–Experiences of people with intellectual disabilities. British Journal of Learning Disabilities, 49(3), 373–382. [Google Scholar] [CrossRef]
- Wehmeyer, M. L. (2020). The importance of self-determination to the quality of life of people with intellectual disability: A perspective. International Journal of Environmental Research and Public Health, 17(19), 7121. [Google Scholar] [CrossRef]
- Witwer, A. N., Rosencrans, M. E., Taylor, C. A., Cobranchi, C., Krahn, G. L., Havercamp, S. M., & Ohio State University Nisonger RRTC on Health and Function. (2025). Working with adults with intellectual disability and clinicians to advance mental health treatment: Informing practice guidelines and research. Journal of Mental Health Research in Intellectual Disabilities, 18(1), 1–29. [Google Scholar] [CrossRef]
- Xia, M., Li, X., & Tudge, J. R. (2020). Operationalizing Urie Bronfenbrenner’s process-person-context-time model. Human Development, 64(1), 10–20. [Google Scholar] [CrossRef]
- Zambri, I. M., Amin, A. S., Kamil, N. K. M., Akhir, N. M., Sutan, R., Khairuddin, K. F., & Abdullah, W. A. W. (2023). Factor affecting independent living of persons with intellectual disabilities: A systematic review. International Journal of Academic Research in Progressive Education and Development, 12(1), 623–644. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.