
Pharmacy Students’ Perceptions of Receiving Hands-On Continuous Glucose Monitoring (CGM) Education as Part of Their Core Curriculum: A Pre-Post Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants
2.3. Study Procedures and Outcomes
2.3.1. Pre- and Post-Activity Surveys
2.3.2. Hands-On CGM Education (Table 1)

{kind=link}
{kind=link}
| Learning Type | Duration | Activities |
|---|---|---|
| Self-study (outside class time) (1.0 h) | ||
| Lecture 1 | CGM Education Part I (1.5 h) |
|
| Diabetes therapeutics (1.0 h) |
| |
| Lecture 2 | Diabetes therapeutics (2.5 h) | |
| Lecture 3 | Diabetes therapeutics (1.5 h) | |
| Lecture 4 | Diabetes therapeutics (1.5 h) | |
| Lecture 5 * | CGM education Part II (1.0 h) |
|
| Diabetes therapeutics (1.5 h) |
| |
2.3.3. Study Workflow
2.4. Statistical Analysis
3. Results
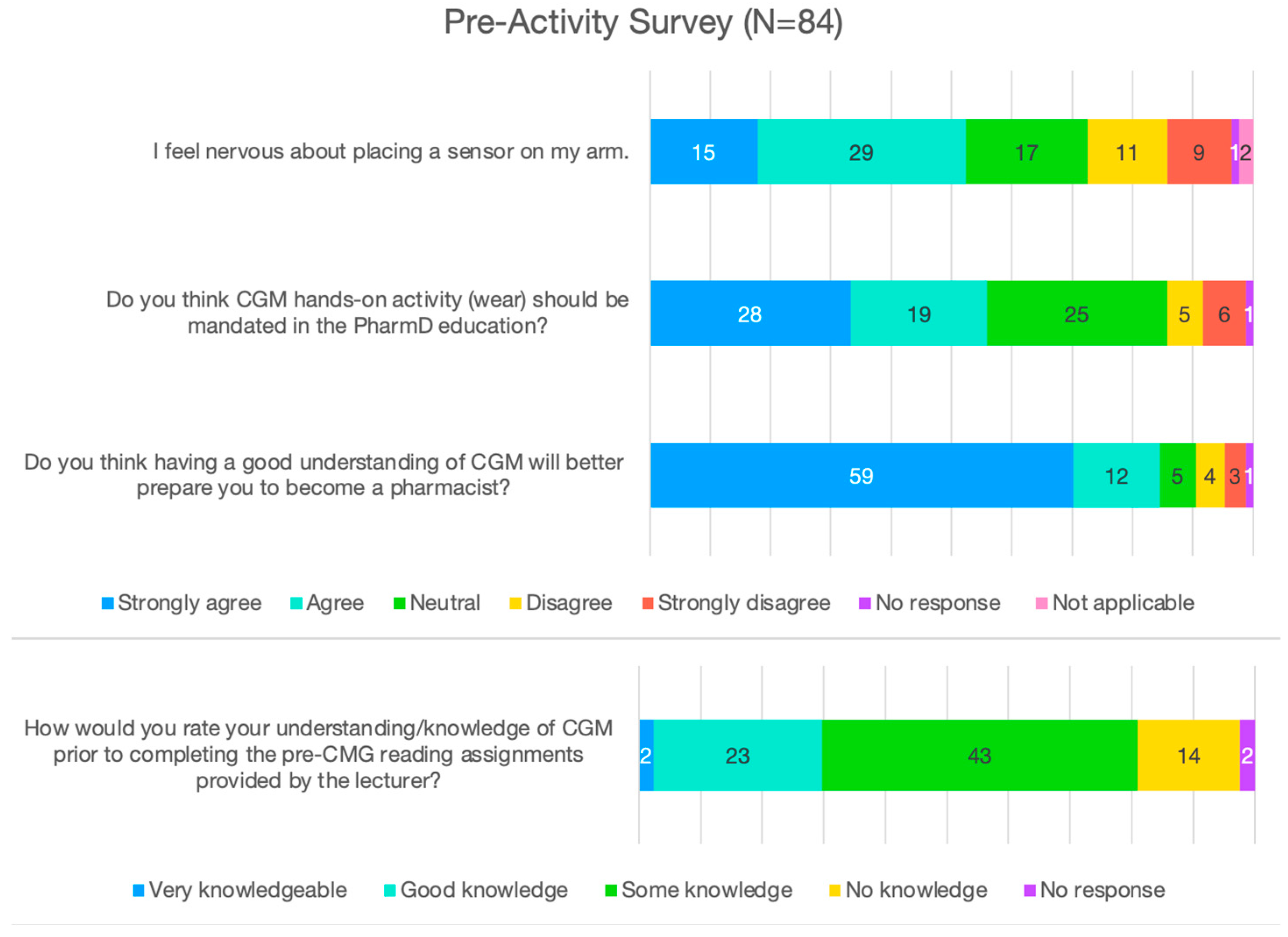
3.1. Pre-Activity Survey
3.2. Post-Activity Survey
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021. [Google Scholar]
- Sherrill, C.H.; Houpt, C.T.; Dixon, E.M.; Richter, S.J. Effect of Pharmacist-Driven Professional Continuous Glucose Monitoring in Adults with Uncontrolled Diabetes. J. Manag. Care Spec. Pharm. 2020, 26, 600–609. [Google Scholar] [CrossRef] [PubMed]
- Farmaki, P.; Damaskos, C.; Garmpis, N.; Garmpi, A.; Savvanis, S.; Diamantis, E. Complications of the Type 2 Diabetes Mellitus. Curr. Cardiol. Rev. 2020, 16, 249–251. [Google Scholar] [CrossRef]
- Isaacson, B.; Kaufusi, S.; Sorensen, J.; Joy, E.; Jones, C.; Ingram, V.; Mark, N.; Phillips, M.; Briesacher, M. Demonstrating the Clinical Impact of Continuous Glucose Monitoring Within an Integrated Healthcare Delivery System. J. Diabetes Sci. Technol. 2022, 16, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Maiorino, M.I.; Signoriello, S.; Maio, A.; Chiodini, P.; Bellastella, G.; Scappaticcio, L.; Longo, M.; Giugliano, D.; Esposito, K. Effects of Continuous Glucose Monitoring on Metrics of Glycemic Control in Diabetes: A Systematic Review With Meta-analysis of Randomized Controlled Trials. Diabetes Care 2020, 43, 1146–1156. [Google Scholar] [CrossRef]
- Norman, G.J.; Paudel, M.L.; Parkin, C.G.; Bancroft, T.; Lynch, P.M. Association Between Real-Time Continuous Glucose Monitor Use and Diabetes-Related Medical Costs for Patients with Type 2 Diabetes. Diabetes Technol. Ther. 2022, 24, 520–524. [Google Scholar] [CrossRef] [PubMed]
- Natale, P.; Chen, S.; Chow, C.K.; Cheung, N.W.; Martinez-Martin, D.; Caillaud, C.; Scholes-Robertson, N.; Kelly, A.; Craig, J.C.; Strippoli, G.; et al. Patient Experiences of Continuous Glucose Monitoring and Sensor-Augmented Insulin Pump Therapy for Diabetes: A Systematic Review of Qualitative Studies. J. Diabetes 2023, 15, 1048–1069. [Google Scholar] [CrossRef]
- Vascimini, A.; Saba, Y.; Baskharoun, F.; Crooks, K.; Huynh, V.; Wasson, S.; Wright, E.; Bullers, K.; Franks, R.; Carris, N.W.; et al. Pharmacist-Driven Continuous Glucose Monitoring in Community and Ambulatory Care Pharmacy Practice: A Scoping Review. J. Am. Pharm. Assoc. JAPhA 2023, 63, 1660–1668.e2. [Google Scholar] [CrossRef]
- Litten, K.; Folz, H.; Lobkovich, A.; Sherrill, C.H.; Berlie, H. Integrating Continuous Glucose Monitoring into Doctor of Pharmacy Curricula. JACCP J. Am. Coll. Clin. Pharm. 2025, 8, 129–135. [Google Scholar] [CrossRef]
- Knezevich, E.; Fuji, K.T.; Larson, K.; Muniz, G. A Cross-Sectional Survey Study Examining the Provision of Continuous Glucose Monitoring Education in U.S. Doctor of Pharmacy Programs. Pharmacy 2022, 10, 174. [Google Scholar] [CrossRef]
- Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group. Validation of Measures of Satisfaction with and Impact of Continuous and Conventional Glucose Monitoring. Diabetes Technol. Ther. 2010, 12, 679–684. [Google Scholar] [CrossRef]
- Zahid, M.; Dowlatshahi, S.; Kansara, A.H.; Sadhu, A.R. The Evolution of Diabetes Technology—Options Toward Personalized Care. Endocr. Pract. 2023, 29, 653–662. [Google Scholar] [CrossRef] [PubMed]
- Abbott. FreeStyle Libre 2 Flash Glucose Monitoring System: Useful Tips for Sensor Wear. 2021. Available online: www.freestyle.abbott (accessed on 15 January 2025).
- Kiger, M.E.; Varpio, L. Thematic Analysis of Qualitative Data: AMEE Guide No. 131. Med. Teach. 2020, 42, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Milovanovic, B.; Tomovic, D.L.; Jankovic, S.; Grubor, I.; Nikolic, L.V.N.M.; Nikolić, M.; Mijajlović, M.; Mrvić, S.; Divjak, A.; Milojević, A.; et al. Factors Influencing the Fear of Needles among Students of Medicine and Pharmacy. Acta Fac. Medicae Naissensis 2017, 34, 147–158. [Google Scholar] [CrossRef]
- Alrashidi, N.; Pasay an, E.; Alrashedi, M.S.; Alqarni, A.S.; Gonzales, F.; Bassuni, E.M.; Pangket, P.; Estadilla, L.; Benjamin, L.S.; Ahmed, K.E. Effects of Simulation in Improving the Self-Confidence of Student Nurses in Clinical Practice: A Systematic Review. BMC Med. Educ. 2023, 23, 815. [Google Scholar] [CrossRef]
- Sherrill, C.H.; Lee, S.; Bradley, C.L. Design and Development of a Continuous Glucose Monitoring Educational Module for Students and Practicing Pharmacists. Curr. Pharm. Teach. Learn. 2022, 14, 62–70. [Google Scholar] [CrossRef]
- Folz, H.N.; Lee, S.; Sherrill, C.H. Student Pharmacist Counseling Performance after Hands-on Continuous Glucose Monitoring Education: A Multi-Institutional Pragmatic Randomized Study. Patient Educ. Couns. 2025, 131, 108578. [Google Scholar] [CrossRef] [PubMed]
- Krouwer, J.S. Adverse Event Causes From 2022 for Four Continuous Glucose Monitors. J. Diabetes Sci. Technol. 2025, 19, 80–83. [Google Scholar] [CrossRef]
- Markov, A.M.; Krutilova, P.; Cedeno, A.E.; McGill, J.B.; McKee, A.M. Interruption of Continuous Glucose Monitoring: Frequency and Adverse Consequences. J. Diabetes Sci. Technol. 2024, 18, 1096–1101. [Google Scholar] [CrossRef]
- Sinisterra, M.; Hamburger, S.; Tully, C.; Hamburger, E.; Jaser, S.; Streisand, R. Young Children with Type 1 Diabetes: Sleep, Health-Related Quality of Life, and Continuous Glucose Monitor Use. Diabetes Technol. Ther. 2020, 22, 639–642. [Google Scholar] [CrossRef]
- Kolanczyk, D.M.; Merlo, J.R.; Bradley, B.; Flannery, A.H.; Gibson, C.M.; McBane, S.; Murphy, J.A.; Noble, J.M.; Noble, M.B.; Patton, H.M.; et al. 2023 Update to the American College of Clinical Pharmacy Pharmacotherapy Didactic Curriculum Toolkit. J. Am. Coll. Clin. Pharm. JACCP 2024, 7, 255–269. [Google Scholar] [CrossRef]
- American Diabetes Association. Standards of Medical Care in Diabetes-2022 Abridged for Primary Care Providers. Clin. Diabetes Publ. Am. Diabetes Assoc. 2022, 40, 10–38. [Google Scholar] [CrossRef]
- Lee, J.Y.; Nguyen, J.T.; Arroyo, J.; Tran, T.; Hanami, D.; Mayorga, J. Feasibility and Acceptability of Using Flash Glucose Monitoring System Sensors to Empower Lifestyle Changes in People With Prediabetes. Diabetes Care 2023, 46, e10–e11. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.Y.; Arcos, D.; Chan, D.; Karabedian, C.; Mayorga, J. Pharmacy Students’ Perceptions of Receiving Hands-On Continuous Glucose Monitoring (CGM) Education as Part of Their Core Curriculum: A Pre-Post Study. Pharmacy 2025, 13, 78. https://doi.org/10.3390/pharmacy13030078
Lee JY, Arcos D, Chan D, Karabedian C, Mayorga J. Pharmacy Students’ Perceptions of Receiving Hands-On Continuous Glucose Monitoring (CGM) Education as Part of Their Core Curriculum: A Pre-Post Study. Pharmacy. 2025; 13(3):78. https://doi.org/10.3390/pharmacy13030078
Chicago/Turabian StyleLee, Joyce Y., Daniela Arcos, Daniella Chan, Celine Karabedian, and José Mayorga. 2025. "Pharmacy Students’ Perceptions of Receiving Hands-On Continuous Glucose Monitoring (CGM) Education as Part of Their Core Curriculum: A Pre-Post Study" Pharmacy 13, no. 3: 78. https://doi.org/10.3390/pharmacy13030078
APA StyleLee, J. Y., Arcos, D., Chan, D., Karabedian, C., & Mayorga, J. (2025). Pharmacy Students’ Perceptions of Receiving Hands-On Continuous Glucose Monitoring (CGM) Education as Part of Their Core Curriculum: A Pre-Post Study. Pharmacy, 13(3), 78. https://doi.org/10.3390/pharmacy13030078