
Heat Therapy for Musculoskeletal Pain Conditions: Actionable Suggestions for Pharmacists from a Panel of Experts

Abstract
1. Introduction
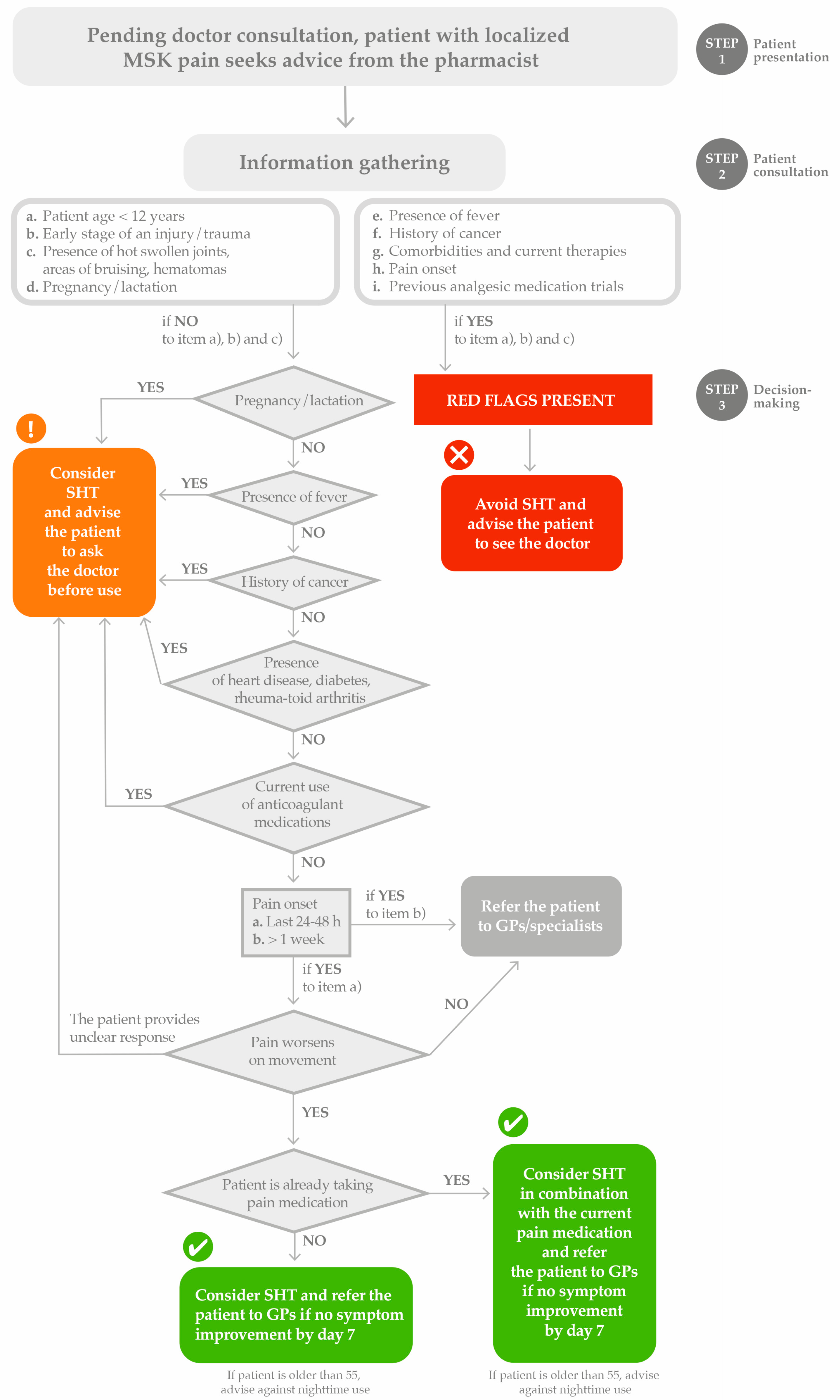
2. Pharmacy Encounters: The Patient with a Localized MSK Pain Seeking Advice
2.1. Red Flags’ Identification
2.2. HT vs. Cold Therapy in MSK Disorders
3. Guiding Pharmacists in Appropriately Selecting HT as a Single Therapeutic Option or in Combination with Over-the-Counter Analgesics
4. Conclusions and Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| DOMS | Delayed Onset Muscle Soreness |
| GP | General Practitioner |
| HT | Heat Therapy |
| LBP | Low Back Pain |
| LHA | Local Heat Application |
| MSK | Musculoskeletal |
| QoL | Quality of Life |
| ROM | Range of Motion |
| SHT | Superficial Heat Therapy |
References
- Blyth, F.M.; Briggs, A.M.; Schneider, C.H.; Hoy, D.G.; March, L.M. The global burden of musculoskeletal pain—Where to from here? Am. J. Public Health 2019, 109, 35–40. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Musculoskeletal Conditions. Available online: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions (accessed on 11 December 2024).
- Margham, T. Musculoskeletal disorders: Time for joint action in primary care. Br. J. Gen. Pract. 2011, 61, 657–658. [Google Scholar] [CrossRef]
- International Pharmaceutical Federation (FIP). Managing Musculoskeletal Pain in the Community Pharmacy: Report from an International Insight Board; International Pharmaceutical Federation: The Hague, The Netherlands, 2024. [Google Scholar]
- Mujtaba, S.H.; Gazerani, P. Exploring the Role of Community Pharmacists in Pain Management: Enablers and Challenges. Pharmacy 2024, 12, 111. [Google Scholar] [CrossRef] [PubMed]
- Lubrano, E.; Mazas, P.F.; Freiwald, J.; Kruger, K.; Grattagliano, I.; Mur, E.; Silva, R.Q.; Maruri, G.R.; de Medeiros, L.S. An International Multidisciplinary Delphi-Based Consensus on Heat Therapy in Musculoskeletal Pain. Pain Ther. 2023, 12, 93–110. [Google Scholar] [CrossRef]
- Clijsen, R.; Stoop, R.; Hohenauer, E.; Aerenhouts, D.; Clarys, P.; Deflorin, C.; Taeymans, J. Local Heat Applications as a Treatment of Physical and Functional Parameters in Acute and Chronic Musculoskeletal Disorders or Pain. Arch. Phys. Med. Rehabil. 2022, 103, 505–522. [Google Scholar] [CrossRef] [PubMed]
- Rossi, R. Heat therapy for different knee diseases: Expert opinion. Front. Rehabil. Sci. 2024, 5, 1390416. [Google Scholar] [CrossRef]
- Freiwald, J.; Magni, A.; Fanlo-Mazas, P.; Paulino, E.; de Medeiros, L.S.; Moretti, B.; Schleip, R.; Solarino, G. A Role for Superficial Heat Therapy in the Management of Non-Specific, Mild-to-Moderate Low Back Pain in Current Clinical Practice: A Narrative Review. Life 2021, 11, 780. [Google Scholar] [CrossRef]
- Nadler, S.F.; Steiner, D.J.; Erasala, G.N.; Hengehold, D.A.; Hinkle, R.T.; Goodale, M.B.; Beln, S.B.; Weingand, K.W. Continuous low-level heat wrap therapy provides more efficacy than Ibuprofen and acetaminophen for acute low back pain. Spine 2022, 27, 1012–1017. [Google Scholar] [CrossRef]
- Petrofsky, J.; Laymon, M.; Alshammari, F.; Khowailed, I.A.; Lee, H. Continuous Low Level Heat Wraps; Faster Healing and Pain Relief during Rehabilitation for Back, Knee and Neck Injuries. Prev. Med. 2015, 3, 61–72. [Google Scholar]
- Petrofsky, J.; Laymon, M.S.; Alshammari, F.S.; Lee, H. Use of low level of continuous heat as an adjunct to physical therapy improves knee pain recovery and the compliance for home exercise in patients with chronic knee pain: A randomized controlled trial. J. Strength Cond. Res. 2016, 30, 3107–3115. [Google Scholar] [CrossRef]
- Petrofsky, J.; Laymon, M.; Alshammari, F.; Khowailed, I.A.; Lee, H. Use of low level of continuous heat and ibuprofen as an adjuct to physical therapy improves pain relief, range of motion and the compliance to home exercise in patients with nonspecific neck pain: A randomized controlled trial. J. Back Musculoskelet. Rehabil. 2017, 30, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Hotfiel, T.; Fanlo-Mazas, P.; Malo-Urries, M.; Paulino, E.; de Medeiros, L.S.; Blondett, M.; Vetrano, M.; Freiwald, J. Importance of heat therapy in the treatment of pain in the daily clinical practice. J. Bodyw. Mov. Ther. 2024, 38, 263–268. [Google Scholar] [CrossRef] [PubMed]
- GBD 2021 Neck Pain Collaborators. Global, regional, and national burden of neck pain, 1990-2020, and projections to 2050: A systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2024, 6, e141–e154. [Google Scholar]
- Moretti, A.; Menna, F.; Aulicino, M.; Paoletta, M.; Liguori, S.; Iolascon, G. Characterization of Home Working Population during COVID-19 Emergency: A Cross-Sectional Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6284. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, M.W.; Brochhagen, J.; Tischer, T.; Beitzel, K.; Seil, R.; Grim, C. Risk factors and prevention strategies for shoulder injuries in overhead sports: An updated systematic review. J. Exp. Orthop. 2022, 9, 78. [Google Scholar] [CrossRef]
- Giua, C.; Minghetti, P.; Gandolini, G.; Rocco, P.; Arancio, E.; Bevacqua, T.; Floris, N.; Keber, E.; Sgcp; Musazzi, U.M. Community Pharmacist’s Role in Detecting Low Back Pain, and Patient Attitudes-A Cross-Sectional Observational Study in Italian Community Pharmacies. Int. J. Environ. Res. Public Health 2020, 17, 5965. [Google Scholar] [CrossRef]
- Ventriglia, G.; Gervasoni, F.; Franco, M.; Magni, A.; Panico, G.; Iolascon, G. Musculoskeletal Pain Management and Thermotherapy: An Exploratory Analysis of Italian Physicians’ Attitude, Beliefs, and Prescribing Habits. J. Pain Res. 2023, 16, 1547–1557. [Google Scholar] [CrossRef]
- Nadler, S.F.; Weingand, K.; Kruse, R.J. The physiologic basis and clinical applications of cryotherapy and thermotherapy for the pain practitioner. Pain Physician 2004, 7, 395–399. [Google Scholar] [CrossRef]
- Malanga, G.A.; Yan, N.; Stark, J. Mechanisms and efficacy of heat and cold therapies for musculoskeletal injury. Postgrad. Med. 2015, 127, 57–65. [Google Scholar] [CrossRef]
- Cheung, K.; Hume, P.; Maxwell, L. Delayed onset muscle soreness: Treatment strategies and performance factors. Sports Med. 2003, 33, 145–164. [Google Scholar] [CrossRef]
- Wang, Y.; Li, S.; Zhang, Y.; Chen, Y.; Yan, F.; Han, L.; Ma, Y. Heat and cold therapy reduce pain in patients with delayed onset muscle soreness: A systematic review and meta-analysis of 32 randomized controlled trials. Phys. Ther. Sport 2021, 48, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Petrofsky, J.S.; Khowailed, I.A.; Lee, H.; Berk, L.; Bains, G.S.; Akerkar, S.; Shah, J.; Al-Dabbak, F.; Laymon, M.S. Cold vs. heat after exercise-is there a clear winner for muscle soreness. J. Strength Cond. Res. 2015, 29, 3245–3252. [Google Scholar] [CrossRef] [PubMed]
- Tzortziou Brown, V.; Underwood, M.; Westwood, O.M.; Morrissey, D. Improving the management of musculoskeletal conditions: Can an alternative approach to referral management underpinned by quality improvement and behavioural change theories offer a solution and a better patient experience? A mixed-methods study. BMJ Open 2019, 9, e024710. [Google Scholar] [CrossRef] [PubMed]
- Barbee, J.; Chessher, J.; Greenlee, M. Pain Management: The Pharmacist’s evolving role. Pharm. Times 2015, 4. Available online: https://www.pharmacytimes.com/view/pain-management-the-pharmacists-evolving-role (accessed on 3 November 2024).
- International Pharmaceutical Federation (FIP). Using Heat Therapy for the Management of Musculoskeletal Pain: Guidance for Pharmacists; International Pharmaceutical Federation: The Hague, The Netherlands, 2024. [Google Scholar]
- Ventriglia, G.; Franco, M.; Magni, A.; Gervasoni, F. Treatment Algorithms for Continuous Low-Level Heat Wrap Therapy for the Management of Musculoskeletal Pain: An Italian Position Paper. J. Pain Res. 2024, 17, 4075–4084. [Google Scholar] [CrossRef]
- Piquer-Martinez, C.; Urionagüena, A.; Benrimoj, S.I.; Calvo, B.; Martinez-Martinez, F.; Fernandez-llimos, F.; Garcia-Cardenas, V.; Gastelurrutia, M.A. Integration of community pharmacy in primary health care: The challenge. Res. Soc. Adm. Pharm. 2022, 18, 3444–3447. [Google Scholar] [CrossRef]
- Shrestha, S.; Iqbal, A.; Teoh, S.L.; Khanal, S.; Gan, S.H.; Lee, S.W.H.; Paudyal, V. Impact of pharmacist-delivered interventions on pain-related outcomes: An umbrella review of systematic reviews and meta-analyses. Res. Soc. Adm. Pharm. 2024, 20, 34–51. [Google Scholar] [CrossRef]

{kind=link}
| Pharmacist-Led Patient Pain Assessment | Questions |
|---|---|
| Duration of the pain | When it started and how long it has lasted? Have you been suffering for more than a week? |
| How the pain started | What were you doing when the pain started? |
| Characteristics of the pain | What does your pain feel like? Point to where it hurts the most. Where does your pain go from there? What makes your pain better or worse? Does the pain get worse during night-time? |
| Pain course | Would you consider yourself constantly in pain? |
| Pain severity | Please rate your pain by selecting a number between 0 and 10 that best describes your pain at its worst in the last 24 h |
| Current pain management | What treatments or medications, if any, are you receiving for your pain? |
| Given the increasing burden of MSK disorders among the general population, pharmacists’ proximity to the community should be better exploited to optimize MSK care provision. |
| Adequate training and education on MSK pain management, including the use of non-pharmacological approaches, including SHT, would empower pharmacists to provide the patients with well-informed advice and appropriate interventions. |
| A hands-on approach to the management of MSK pain is desirable to build and maintain pharmacists’ competency in counselling patients on using SHT as a valuable non-pharmacological option either alone or in combination with over-the-counter pain medications. |
| Establishing collaborative relationships with other healthcare professionals, such as GPs, physiatrists, orthopedics, and physiotherapists may facilitate a multidisciplinary approach to patient care and promote a full integration of the pharmacists into MSK pain care pathways. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nossa, F.; Franco, M.; Magni, A.; Raimondo, E.; Ventriglia, G.; Gervasoni, F. Heat Therapy for Musculoskeletal Pain Conditions: Actionable Suggestions for Pharmacists from a Panel of Experts. Pharmacy 2025, 13, 63. https://doi.org/10.3390/pharmacy13030063
Nossa F, Franco M, Magni A, Raimondo E, Ventriglia G, Gervasoni F. Heat Therapy for Musculoskeletal Pain Conditions: Actionable Suggestions for Pharmacists from a Panel of Experts. Pharmacy. 2025; 13(3):63. https://doi.org/10.3390/pharmacy13030063
Chicago/Turabian StyleNossa, Flavia, Massimiliano Franco, Alberto Magni, Emanuela Raimondo, Giuseppe Ventriglia, and Fabrizio Gervasoni. 2025. "Heat Therapy for Musculoskeletal Pain Conditions: Actionable Suggestions for Pharmacists from a Panel of Experts" Pharmacy 13, no. 3: 63. https://doi.org/10.3390/pharmacy13030063
APA StyleNossa, F., Franco, M., Magni, A., Raimondo, E., Ventriglia, G., & Gervasoni, F. (2025). Heat Therapy for Musculoskeletal Pain Conditions: Actionable Suggestions for Pharmacists from a Panel of Experts. Pharmacy, 13(3), 63. https://doi.org/10.3390/pharmacy13030063