
The Barriers and Facilitators of Different Stakeholders When Deprescribing Benzodiazepine Receptor Agonists in Older Patients—A Systematic Review

Abstract
1. Introduction
Objective
2. Methods
3. Results
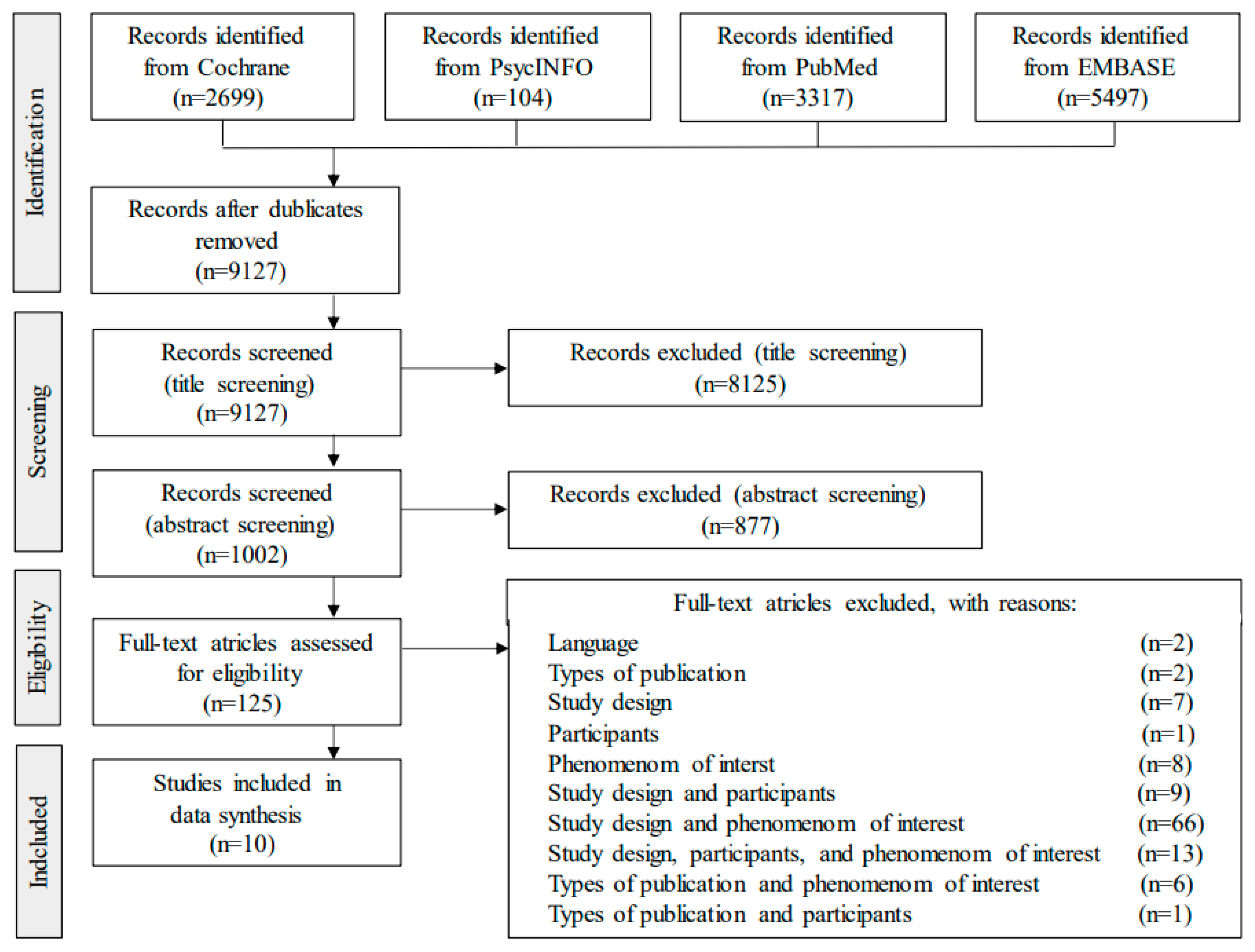
3.1. Literature Search
3.2. Description of the Articles
3.3. Quality Assessment
3.4. Barriers and Facilitators Are Shared between the Stakeholders
3.5. Shared Barriers towards Deprescribing BZRA
3.6. Shared Facilitators towards Deprescribing BZRA
3.7. Individual Barriers towards Deprescribing BZRA
3.8. Individual Facilitators towards Deprescribing BZRA
4. Discussion
4.1. Stakeholders Involved in BZRA Deprescribing: Individual and Shared Barriers and Facilitators
4.2. Stakeholder Attitudes Influence the Willingness of Patients to Deprescribe BZRA
4.3. Nurses Call for Education and Support to Facilitate BZRA Deprescribing
4.4. Caregivers Facilitate BZRA Deprescribing Due to Observed Side Effects among Patients
4.5. Future Directions for Research
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Matheson, E.; Hainer, B.L. Insomnia: Pharmacologic Therapy. Am. Fam. Physician 2017, 96, 29–35. [Google Scholar]
- Pottie, K.; Thompson, W.; Davies, S.; Grenier, J.; Sadowski, C.A.; Welch, V.; Holbrook, A.; Boyd, C.; Swenson, R.; Ma, A.; et al. Deprescribing benzodiazepine receptor agonists: Evidence-based clinical practice guideline. Can. Fam. Physician. 2018, 64, 339–351. [Google Scholar]
- Vinkers, C.H.; Olivier, B. Mechanisms Underlying Tolerance after Long-Term Benzodiazepine Use: A Future for Subtype-Selective GABA(A) Receptor Modulators? Adv. Pharmacol. Sci. 2012, 2012, 416864. [Google Scholar] [CrossRef]
- Ng, B.J.; Le Couteur, D.G.; Hilmer, S.N. Deprescribing Benzodiazepines in Older Patients: Impact of Interventions Targeting Physicians, Pharmacists, and Patients. Drugs Aging 2018, 35, 493–521. [Google Scholar] [CrossRef] [PubMed]
- Donoghue, J.; Lader, M. Usage of benzodiazepines: A review. Int. J. Psychiatry Clin. Pr. 2010, 14, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.J.; Tett, S.E. How do different age groups use benzodiazepines and antidepressants? Analysis of an Australian administrative database, 2003–2006. Drugs Aging. 2009, 26, 113–122. [Google Scholar] [CrossRef] [PubMed]
- 2019 American Geriatrics Society Beers Criteria® Update Expert Panel; Fick, D.M.; Semla, T.P.; Steinman, M.; Beizer, J.; Brandt, N.; Sandhu, S. American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar]
- Chen, L.; Farrell, B.; Ward, N.; Russell, G.; Eisener-Parsche, P.; Dore, N. Discontinuing Benzodiazepine Therapy: An Interdisciplinary Approach at a Geriatric Day Hospital. Can. Pharm. J. 2010, 143, 286–295.e3. [Google Scholar] [CrossRef]
- Stern, C.; Jordan, Z.; McArthur, A. Developing the Review Question and Inclusion Criteria. Ajn Am. J. Nurs. 2014, 114, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Det Kongelige Bibliotek. Københavns Universitetsbibliotek. Sundhedsvidenskab: Farma. 2020. Available online: https://kub.kb.dk/sund/farma (accessed on 12 May 2020).
- EndnoteTM; Version X8; Clarivate Analytics: Philadelphia, PA, USA, 2017.
- Robson, C.; McCartan, K. Real World Research; John Wiley & Sons: Chichester, UK, 2016. [Google Scholar]
- Nvivo; Version 12; QSR International: Melbourne, Australia, 2020.
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Canham, S.L.; Gallo, J.; Simoni-Wastila, L. Perceptions of Benzodiazepine Dependence Among Women Age 65 and Older. J. Gerontol. Soc. Work. 2014, 57, 872–888. [Google Scholar] [CrossRef] [PubMed]
- Heser, K.; Pohontsch, N.J.; Scherer, M.; Löffler, A.; Luck, T.; Riedel-Heller, S.G.; Maier, W.; Parker, D.; Haenisch, B.; Jessen, F. Perspective of elderly patients on chronic use of potentially inappropriate medication–Results of the qualitative CIM-TRIAD study. PLoS ONE 2018, 13, e0202068. [Google Scholar] [CrossRef]
- Martin, P.; Tannenbaum, C. A realist evaluation of patients’ decisions to deprescribe in the EMPOWER trial. Bmj Open 2017, 7, e015959. [Google Scholar] [CrossRef] [PubMed]
- Tannenbaum, C.; Martin, P.; Tamblyn, R.; Benedetti, A.; Ahmed, S. Reduction of inappropriate benzodiazepine prescriptions among older adults through direct patient education: The EMPOWER cluster randomized trial. JAMA Intern. Med. 2014, 174, 890–898. [Google Scholar] [CrossRef] [PubMed]
- Williams, F.; Mahfouz, C.; Bonney, A.; Pearson, R.; Seidel, B.; Dijkmans-Hadley, B.; Ivers, R. A circle of silence: The attitudes of patients older than 65 years of age to ceasing long-term sleeping tablets. Aust. Fam. Physician 2016, 45, 506–511. [Google Scholar] [PubMed]
- Cook, J.M.; Marshall, R.; Masci, C.; Coyne, J.C. Physicians’ Perspectives on Prescribing Benzodiazepines for Older Adults: A Qualitative Study. J. Gen. Intern. Med. 2007, 22, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Šubelj, M.; Vidmar, G.; Švab, V. Prescription of benzodiazepines in Slovenian family medicine: A qualitative study. Wien. Klin. Wochenschr. 2010, 122, 474–478. [Google Scholar] [CrossRef]
- Anthierens, S.; Grypdonck, M.; De Pauw, L.; Christiaens, T. Perceptions of nurses in nursing homes on the usage of benzodiazepines. J. Clin. Nurs. 2009, 18, 3098–3106. [Google Scholar] [CrossRef] [PubMed]
- Pickering, A.N.; Hamm, M.E.; Bs, A.D.; Hanlon, J.T.; Thorpe, C.T.; Gellad, W.F.; Radomski, T.R. Older Patient and Caregiver Perspectives on Medication Value and Deprescribing: A Qualitative Study. J. Am. Geriatr. Soc. 2020, 68, 746–753. [Google Scholar] [CrossRef] [PubMed]
- Reeve, E.; Shakib, S.; Hendrix, I.; Roberts, M.S.; Wiese, M.D. Review of deprescribing processes and development of an evidence-based, patient-centred deprescribing process. Br. J. Clin. Pharm. 2014, 78, 738–747. [Google Scholar] [CrossRef]
- Scott, I.A.; Hilmer, S.N.; Reeve, E.; Potter, K.; Le Couteur, D.; Rigby, D.; Martin, J.H. Reducing inappropriate polypharmacy: The process of deprescribing. JAMA Intern. Med. 2015, 175, 827–834. [Google Scholar] [CrossRef] [PubMed]
- Kua, C.-H.; Mak, V.S.; Lee, S.W.H. Perspectives of health professionals towards deprescribing practice in Asian nursing homes: A qualitative interview study. BMJ Open 2019, 9, e030106. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, F. Perceptions of German GPs on benefits and risks of benzodiazepines and Z-drugs. Swiss Med. Wkly. 2013, 143, 13745. [Google Scholar] [CrossRef]
- Heinemann, S.; Brockmöller, J.; Hagmayer, Y.; Himmel, W. Why Z-drugs are used even if doctors and nurses feel unable to judge their benefits and risks—A hospital survey. Eur. J. Clin. Pharm. 2019, 76, 285–290. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Stakeholder | No. of Participants | Setting (Country) | Gender %F | Age | BZRA Consumption and Prescribing | Data Collection Method (Analytical Method) | First Author (Year) [Ref. No.] |
|---|---|---|---|---|---|---|---|
| Patients | 12 | Other (USA) | 100% | 65–89 | Near daily or daily BZRA use ≥3 months | Semi structured interview (Thematic analysis) | Canham (2014) [15] |
| Patients | 5 | Hospital (Canada) | - | 79–91 | Daily BZRA use ranging from recent initiation to 30 years | Semi structured interview (Constant comparative analysis) | Chen (2010) [8] |
| Patients | 10 * | GP (Germany) | 80% | 86–96 | Nine participants had a chronic BZRA use. One participant non-chronic BZRA use. | Semi structured interview (Content analysis) | Heser (2018) [16] |
| Patients | 21 ** | Pharmacy (Canada) | 72% | 74.6 ± 6.3 | Chronic users of BZRA | Semi structured interview (Thematic content analysis) | Martin (2017) [17] |
| Patients | 123 *** | Pharmacy (Canada) | 69% | 74 ± 6.3 | The mean duration of BZRA use was 10 years | Semi structured interview (Content analysis) | Tannenbaum (2014) [18] |
| Patients | 17 | GP (Australia) | 76% | 77 (F), 73 (M) (mean) | Nocturnal BZRA use ranging from 1 year to more than 20 years | Semi structured interview (Constant comparative analysis) | Williams (2016) [19] |
| Physicians | 33 | Other (USA) | 33% | 47 (mean) | Practice characteristics include family medicine, geriatrics, and general internists | Semi structured interview (Narrative analysis) | Cook (2007) [20] |
| Physicians | 10 | GP (Slovenia) | 20% | **** | Five low- and high-prescribing family physicians, respectively. The high prescribers had practiced 18 years on average, which is six years more than of the low prescribers | Semi structured interview (Thematic analysis) | Subelj (2010) [21] |
| Nurses | 33 | Nursing home (Belgium) | 76% | 37 (mean) | All nurses had a bachelor’s degree Mean years of experience was 14 | Focus group and semi-structured interview (Thematic analysis) | Anthierens (2009) [22] |
| Caregivers | 17 | Other (USA) | 82% | 22–69 | 10 caregivers cared for family members, 7 were employed via home care agencies, nursing homes, group homes ***** | Focus group (Thematic analysis) | Pickering (2020) [23] |
| Shared Barriers | |||
|---|---|---|---|
| Patients | Physicians | Nurses | |
| Themes | Frequency [Ref. No.] | Frequency [Ref. No.] | Frequency [Ref. No.] |
| Finding BZRA to be an effective treatment | 4 [16,17,19] | 2 [20] | 2 [22] |
| Finding BZRA provide comfort for the patient | 5 [8,15,16] | No data | 1 [22] |
| Conceive that BZRA does not harm the patient | 3 [17,18,19] | 2 [20] | No data |
| Concern about withdrawal symptoms | 4 [8,17,19] | 2 [20] | No data |
| Ageism: Finding deprescribing BZRA as unnecessary due the age of the patient | 3 * [8,16,17] | 2 [20] | No data |
| Lack of knowledge | 6 [8,16,19] Including side effects, alternative treatments, dependence | No data | 9 [22] Including side effects, effects, sleep in general |
| Working environment and procedures | No data | 10 [20,21] Incl. lack of time, deprescribing not being prioritized, concern about losing patients, lacking strategies to taper, and cooperation with specialists/psychiatrists | 14 [22] Incl. lack of time, lacking assessment and observations of the need for continued BZRA treatment, staff shortage, high work pressure, task-oriented work, lack of involvement in medicine |
| Shared Facilitators | |||
| Patients | Physicians | Nurses and Caregivers | |
| Themes | Frequency [Ref. No.] | Frequency [Ref. No.] | Frequency [Ref. No.] |
| Education | 1 [17] Education tool: deprescribing brochure on benzodiazepines | 1 [21] Education about psychiatric disorder from psychiatrists | 1 [22] Nurses Education about sleep hygiene |
| Improving cooperation between healthcare personnel | No data | 2 [21] Cooperation and clear instructions from psychiatrists | 2 [22] Nurses Address sleep problems by interdisciplinary team |
| Patient-motivation | 3 [8,17] Motivation from the physician/pharmacist | 1 [21] Physicians providing motivation to the patients | No data |
| Awareness of side effects | 1 [8] Describe BZRA side effects relevant to the patient’ complaints | No data | 1 [23] Caregivers Benzodiazepines are of low value due to of their side effects |
| Individual Barriers | |||
|---|---|---|---|
| Patients | Physicians | Nurses | |
| Theme Frequency [ref.no.] | Dependence and feeling unable to reduce or cessation, relying on BZRA for comfort and feeling unable to sleep without it 17 [15,16,17,19] | Expected patient resistance towards deprescribing of BZRA 7 [20] | Unequal balance of power between nurses and physicians, including nurses feeling their options are not considered or valued 8 [22] |
| Theme Frequency [ref.no.] | Discouragement or lack of support from physician 4 [17,18] | Reluctance to deprescribe treatment from functioning patients 2 [20,21] | General attitude that BZRA should not be avoided and continued use is necessary 1 [22] |
| Individual Facilitators | |||
| Patients | Physicians | Nurses | |
| Theme Frequency [ref.no.] | The patients are willing to stop BZRA treatment 2 [8,19] | The physicians know and agree with guidelines instructing that BZRA is only for short-term use 1 [20] | Involving the nurses in the patient´ medications and evaluation of medications can encourage the nurses to facilitate deprescribing 2 [22] |
| Theme Frequency [ref.no.] | Mentioning deprescribing to patients and giving the patient time to consider the benefits 2 [8,17] | No data | Systematic work procedures to record their observations on patients’ sleep 2 [22] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rasmussen, A.F.; Poulsen, S.S.; Oldenburg, L.I.K.; Vermehren, C. The Barriers and Facilitators of Different Stakeholders When Deprescribing Benzodiazepine Receptor Agonists in Older Patients—A Systematic Review. Metabolites 2021, 11, 254. https://doi.org/10.3390/metabo11040254
Rasmussen AF, Poulsen SS, Oldenburg LIK, Vermehren C. The Barriers and Facilitators of Different Stakeholders When Deprescribing Benzodiazepine Receptor Agonists in Older Patients—A Systematic Review. Metabolites. 2021; 11(4):254. https://doi.org/10.3390/metabo11040254
Chicago/Turabian StyleRasmussen, Anja Fog, Sarah Sonne Poulsen, Lykke Ida Kaas Oldenburg, and Charlotte Vermehren. 2021. "The Barriers and Facilitators of Different Stakeholders When Deprescribing Benzodiazepine Receptor Agonists in Older Patients—A Systematic Review" Metabolites 11, no. 4: 254. https://doi.org/10.3390/metabo11040254
APA StyleRasmussen, A. F., Poulsen, S. S., Oldenburg, L. I. K., & Vermehren, C. (2021). The Barriers and Facilitators of Different Stakeholders When Deprescribing Benzodiazepine Receptor Agonists in Older Patients—A Systematic Review. Metabolites, 11(4), 254. https://doi.org/10.3390/metabo11040254