
VGG-C Transform Model with Batch Normalization to Predict Alzheimer’s Disease through MRI Dataset


Abstract
:1. Introduction
- -
- Mild cognitive impairment: while generally affected by a memory deficit in many people as they age, in others it leads to problems with dementia.
- -
- Mild dementia: Cognitive impairment that sometimes affects their daily life is found in people with moderate dementia. Symptoms include memory deficits, uncertainty, personality changes, feelings of loss, and difficulty performing daily tasks.
- -
- Moderate dementia: daily life becomes much more complex, and patients require special care and support. Symptoms are comparable to mild dementia but somehow get worse. People may need more help, even combing their hair. They can also show significant personality changes; for example, they become paranoid or irritable for no reason. Sleep disturbances are also likely to occur.
- -
- Severe Dementia: At this stage, symptoms may worsen. These patients may lack communication skills and may require full-time treatment. The bladder can’t be controlled, and you can’t do small activities, such as sitting in a chair with your head raised and maintaining a normal posture. Various research paradises have been conducted to slow the abnormal degeneration of the brain, reduce medical expenses, and improve treatment. According to nih.gov’s “Alzheimer’s Disease Fact Sheet”, the failure of recent AD research studies may suggest that early intervention and diagnosis may be important for the effectiveness of treatment [5]. Various neuroimaging methods are increasingly reliant on early diagnosis of dementia, which is reflected in many new diagnostic criteria. Neuroimaging uses machine learning to increase diagnostic accuracy for various subtypes of dementia [6].
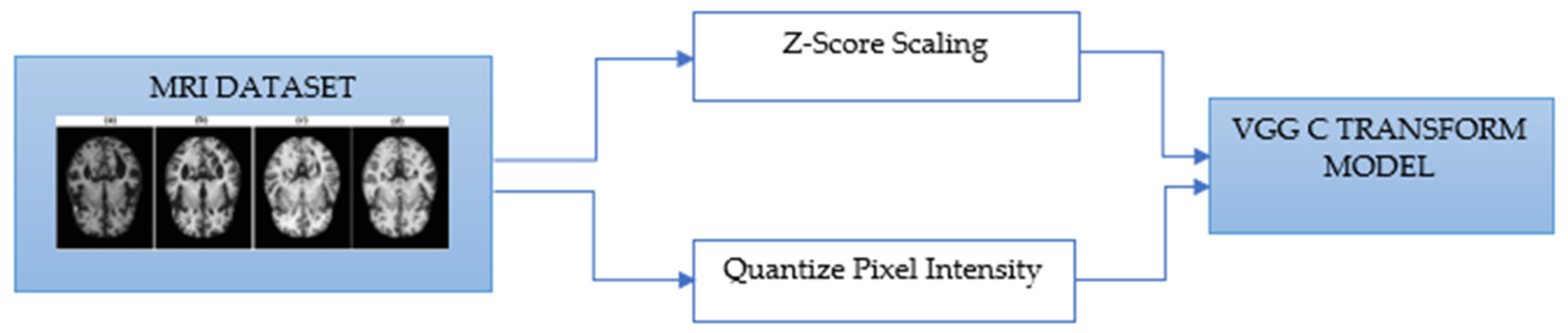
- As mentioned above, the method of diagnosing AD on MRI images compares the size of the hippocampus. However, due to the nature of the existing CNN model, it is difficult to detect because it is not sensitive to image dispersion. Therefore, additional processing of the color space of the image is required.
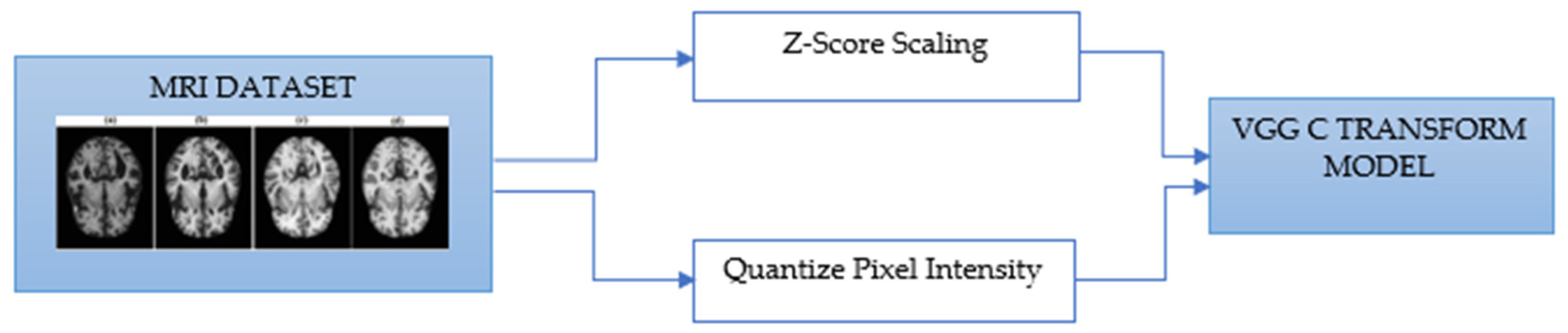
- For Z-score normalization, the interval to which each pixel belongs is converted to [−1, 1], and for min–max, it is converted to [0, 1]. During the computation of the convolutional neural network, the pixel intensity of [0, 255] is adjusted for fast convergence and accurate feature extraction.
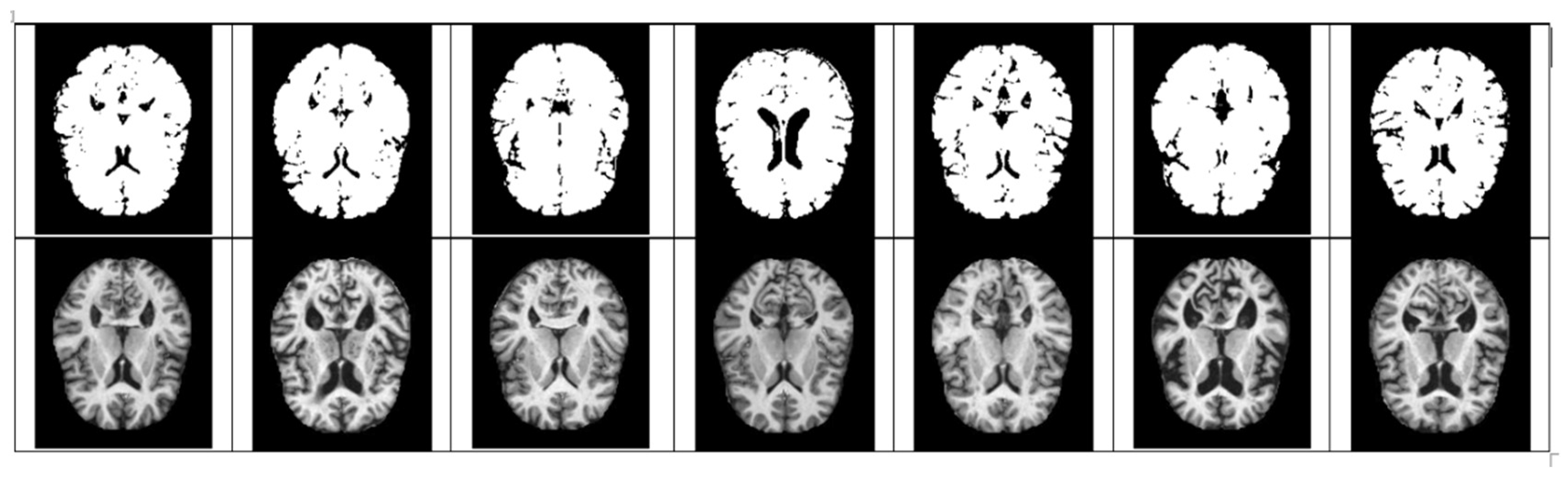
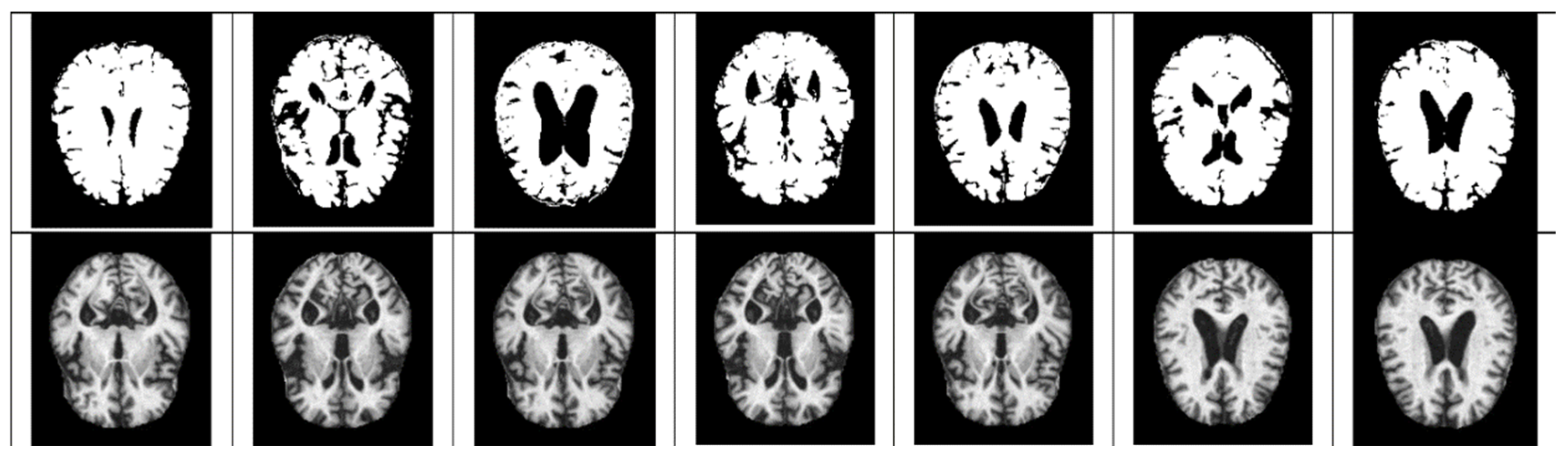
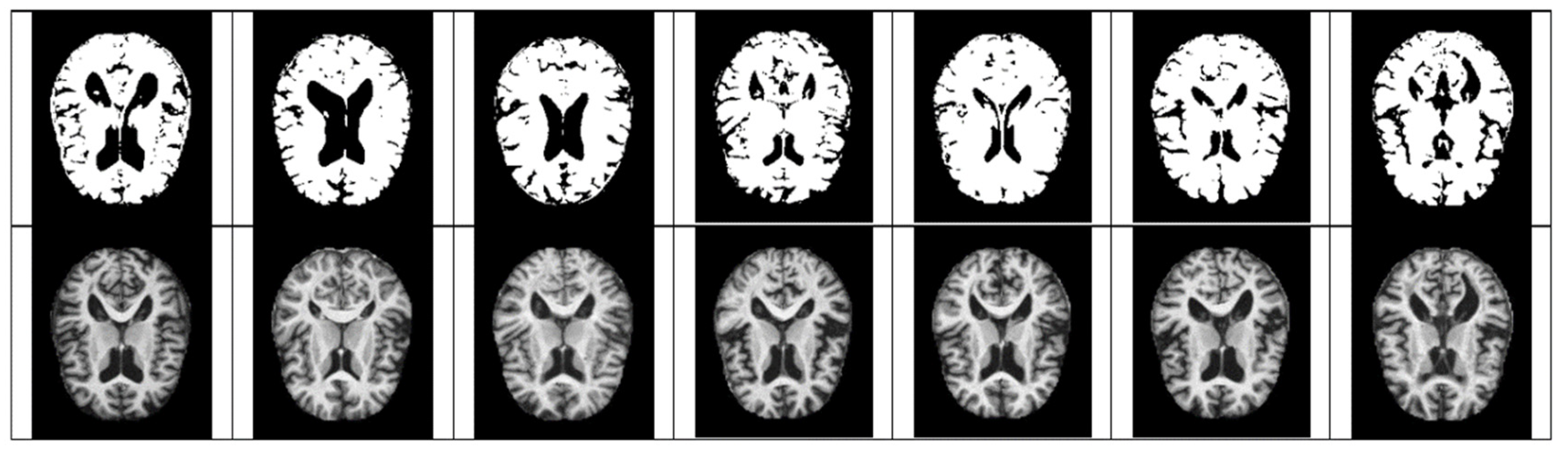
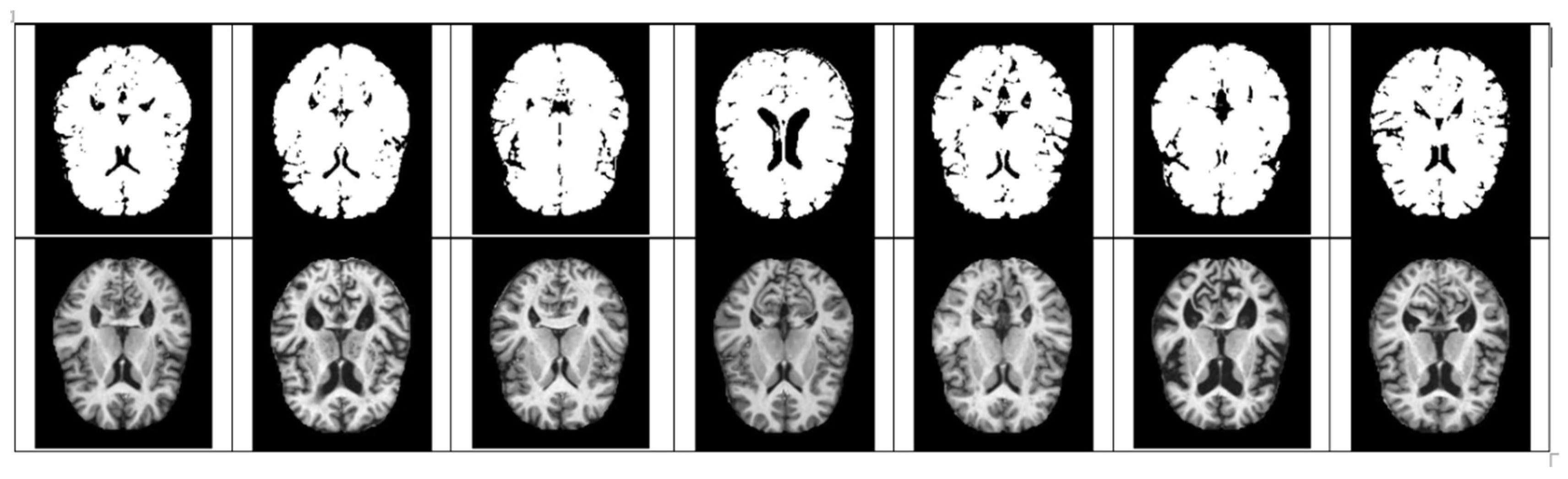
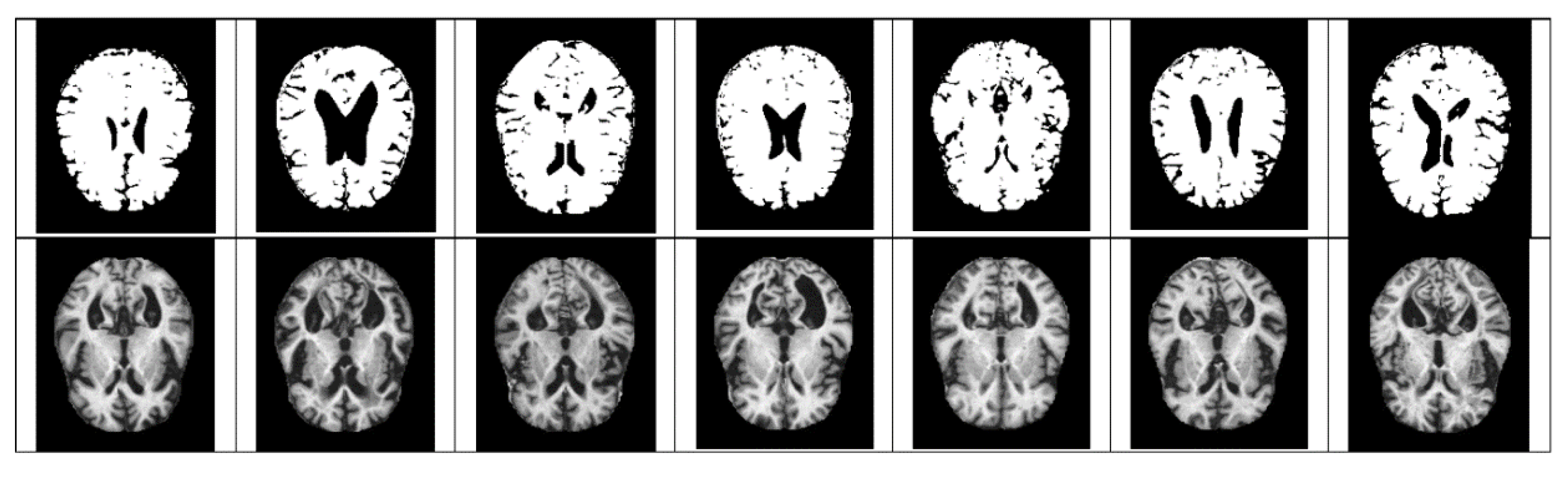
- The size space of pixels constituting the Alzheimer’s MRI data set is [0, 255]. Among them, patients with AD with reduced hippocampus will have more pixels close to zero than normal people. On the premise of this, the average value of pixel intensities in each MRI image is set as a threshold value. Alzheimer’s should recognize changes in size contraction rather than changes in brain function. Based on this information, it is necessary to set the space as an important feature for the color information of MRI rather than a feature representing the shape of the brain.
- Among the VGG family, the VGG-C Transform model with batch normalization added to the VGG-C model showed the highest performance with a test accuracy of about 0.9999. However, since the size of the MRI image is 208 × 176, distortion and loss of pixel information occur in the process of resizing to 224 × 224. Therefore, we propose a VGG model-based architecture that can learn while maintaining the original MRI size. Existing CNNs report high performance for images with the same aspect ratio. This is because images in the real world vary in size and need to be transformed into fixed-size metrics to learn through CNN. However, since all images in a given data set have the same aspect ratio, it is important to find input values of appropriate size. Moreover, due to the data imbalance problem, the AUC score is used as an evaluation indicator. The rest of the paper is arranged as follows: Section 2 describes the related studies. The proposed method is explained in Section 3. Section 4 summarizes the results. The discussion is presented in Section 5, and the conclusion is given in Section 6.
2. Related Work
3. Materials and Method
3.1. Data Preprocess
3.1.1. Scaling
3.1.2. Quantize Pixel Intensity
3.1.3. ConvNet Configuration
4. Experiment and Results
4.1. Software Tools for Experimental
4.2. Quantize Pixel Intensity
4.3. Design Experiments
4.4. Experimental Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AD | Alzheimer’s Disease |
| CNN | Convolutional Neural Network |
| PET | Positron Emission Tomography |
| HC | Healthy Control |
| SVN | Support Vector Machine |
| KNN | K-nearest Neighbor |
| MCI | Mild Cognitive Impairment |
| EMCI | Early MCI |
| LMCI | Late MCI |
| NRCD | National Center for Dementia Research |
| PET | Positron Emission Tomography |
| RF | Random Forest |
| NC | Normal Control |
| GM | Gray Matter |
Appendix A

References
- Liu, S.; Liu, S.; Cai, W.; Che, H.; Pujol, S.; Kikinis, R.; Feng, D.; Fulham, M.J. Multimodal neuroimaging feature learning for multiclass diagnosis of Alzheimer’s disease. IEEE Trans. Biomed. Eng. 2015, 62, 1132–1140. [Google Scholar] [CrossRef] [PubMed]
- Przedborski, S.; Vila, M.; Jackson-Lewis, V. Series introduction: Neurodegeneration: What is it and where are we? J. Clin. Investig. 2003, 111, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Giorgio, J.; Landau, S.M.; Jagust, W.J.; Tino, P.; Kourtzi, Z. Modelling prognostic trajectories of cognitive decline due to Alzheimer’s disease. NeuroImage Clin. 2020, 26, 102199. [Google Scholar] [CrossRef] [PubMed]
- Patterson, C. World Alzheimer Report 2018 the State of the Art of Dementia Research: New Frontiers; Alzheimer’s Disease International: London, UK, 2018. [Google Scholar]
- Alzheimer’s Disease Fact Sheet. 2019. Available online: https://www.nia.nih.gov/health/alzheimers-disease-fact-sheet (accessed on 11 May 2022).
- Stamate, D.; Smith, R.; Tsygancov, R.; Vorobev, R.; Langham, J.; Stahl, D.; Reeves, D. Applying deep learning to predicting dementia and mild cognitive impairment. In Artificial Intelligence Applications and Innovations (IFIP Advances in Information and Communication Technology); Springer: Cham, Switzerland, 2020; Volume 584, pp. 308–319. [Google Scholar] [CrossRef]
- De, A.; Chowdhury, A.S. DTI based Alzheimer’s disease classification with rank modulated fusion of CNNs and random forest. Expert Syst. Appl. 2021, 169, 114338. [Google Scholar] [CrossRef]
- Ieracitano, C.; Mammone, N.; Hussain, A.; Morabito, F.C. novel multi-modal machine learning based approach for automatic classification of EEG recordings in dementia. Neural Netw. 2020, 123, 176–190. [Google Scholar] [CrossRef]
- Kim, Y. Are we being exposed to radiation in the hospital? Environ. Health Toxicol. 2016, 31, e2016005. [Google Scholar] [CrossRef]
- KaggleDataset. Available online: https://www.kaggle.com/datasets/jboysen/mri-and-alzheimers (accessed on 19 May 2022).
- Moser, E.; Stadlbauer, A.; Windischberger, C.; Quick, H.H.; Ladd, M.E. Magnetic resonance imaging methodology. Eur. J. Nucl. Med. Mol. Imag. 2009, 36, 30–41. [Google Scholar] [CrossRef]
- Mansourifar, H.; Shi, W. Deep Synthetic Minority Oversampling Technique. arXiv 2020, arXiv:2003.09788. [Google Scholar]
- Dubey, S. Alzheimer’s Dataset. 2019. Available online: https://www.kaggle.com/tourist55/alzheimers-dataset-4-class-of-images (accessed on 19 May 2022).
- Rieke, J.; Eitel, F.; Weygandt, M.; Haynes, J.D.; Ritter, K. Visualizing convolutional networks for MRI-based diagnosis of Alzheimer’s disease. In Understanding and Interpreting Machine Learning in Medical Image Computing Applications (Lecture Notes in Computer Science); Springer: Cham, Switzerland, 2018; Volume 11038, pp. 24–31. [Google Scholar] [CrossRef]
- Lu, D.; Initiative, A.D.N.; Popuri, K.; Ding, G.W.; Balachandar, R.; Beg, M.F. Multimodal and multiscale deep neural networks for the early diagnosis of Alzheimer’s disease using structural MR and FDG-PET images. Sci. Rep. 2018, 8, 5697. [Google Scholar] [CrossRef]
- Gupta, Y.; Lee, K.H.; Choi, K.Y.; Lee, J.J.; Kim, B.C.; Kwon, G.R. Early diagnosis of Alzheimer’s disease using combined features from voxel-based morphometry and cortical, subcortical, and hippocampus regions of MRI T1 brain images. PLoS ONE 2019, 14, e0222446. [Google Scholar] [CrossRef]
- Ahmed, S.; Choi, K.Y.; Lee, J.J.; Kim, B.C.; Kwon, G.-R.; Lee, K.H.; Jung, H.Y. Ensembles of patch-based classifiers for diagnosis of alzheimer diseases. IEEE Access 2019, 7, 73373–73383. [Google Scholar] [CrossRef]
- Basher, A.; Kim, B.C.; Lee, K.H.; Jung, H.Y. Volumetric featurebased Alzheimer’s disease diagnosis from sMRI data using a convolutional neural network and a deep neural network. IEEE Access 2021, 9, 29870–29882. [Google Scholar] [CrossRef]
- Nawaz, H.; Maqsood, M.; Afzal, S.; Aadil, F.; Mehmood, I.; Rho, S. A deep feature-based real-time system for alzheimer disease stage detection. Multimed. Tools Appl. 2020, 80, 1–19. [Google Scholar] [CrossRef]
- Ieracitano, C.; Mammone, N.; Bramanti, A.; Hussain, A.; Morabito, F.C. A convolutional neural network approach for classification of dementia stages based on 2D-spectral representation of EEG recordings. Neurocomputing 2019, 323, 96–107. [Google Scholar] [CrossRef]
- Jain, R.; Jain, N.; Aggarwal, A.; Hemanth, D.J. Convolutional neural network based Alzheimer’s disease classification from magnetic resonance brain images. Cognit. Syst. Res. 2019, 57, 147–159. [Google Scholar] [CrossRef]
- Mehmood, A.; Yang, S.; Feng, Z.; Wang, M.; Ahmad, A.S.; Khan, R.; Maqsood, M.; Yaqub, M. A transfer learning approach for early diagnosis of Alzheimer’s disease on MRI images. Neuroscience 2021, 460, 43–52. [Google Scholar] [CrossRef]
- Shi, J.; Zheng, X.; Li, Y.; Zhang, Q.; Ying, S. Multimodal neuroimaging feature learning with multimodal stacked deep polynomial networks for diagnosis of Alzheimer’s disease. IEEE J. Biomed. Health Informat. 2018, 22, 173–183. [Google Scholar] [CrossRef]
- Liu, C.-F.; Padhy, S.; Ramachandran, S.; Wang, V.X.; Efimov, A.; Bernal, A.; Shi, L.; Vaillant, M.; Ratnanather, J.T.; Faria, A.V.; et al. Using deep siamese neural networks for detection of brain asymmetries associated with Alzheimer’s disease and mild cognitive impairment. Magn. Reson. Imag. 2019, 64, 190–199. [Google Scholar] [CrossRef]
- Wang, H.; Shen, Y.; Wang, S.; Xiao, T.; Deng, L.; Wang, X.; Zhao, X. Ensemble of 3D densely connected convolutional network for diagnosis of mild cognitive impairment and Alzheimer’s disease. Neurocomputing 2019, 333, 145–156. [Google Scholar] [CrossRef]
- Shankar, K.; Lakshmanaprabu, S.K.; Khanna, A.; Tanwar, S.; Rodrigues, J.J.; Roy, N.R. Alzheimer detection using group grey wolf optimization based features with convolutional classifier. Comput. Electr. Eng. 2019, 77, 230–243. [Google Scholar] [CrossRef]
- Janghel, R.; Rathore, Y. Deep convolution neural network based system for early diagnosis of Alzheimer’s disease. IRBM 2020, 1, 1–10. [Google Scholar] [CrossRef]
- Ge, C.; Qu, Q.; Gu, I.Y.-H.; Jakola, A.S. Multiscale deep convolutional networks for characterization and detection of Alzheimer’s disease using MR images. In Proceedings of the 2019 IEEE International Conference on Image Processing (ICIP), Taipei, Taiwan, 22–25 September 2019; Volume 12, pp. 789–793. [Google Scholar] [CrossRef]
- Pan, T.; Zhao, J.; Wu, W.; Yang, J. Learning imbalanced datasets based on SMOTE and Gaussian distribution. Inf. Sci. 2020, 512, 1214–1233. [Google Scholar] [CrossRef]
- Bi, X.; Wang, H. Early Alzheimer’s disease diagnosis based on EEG spectral images using deep learning. Neural Netw. 2019, 114, 119–135. [Google Scholar] [CrossRef] [PubMed]
- Brownlee, J. A Gentle Introduction to the Rectified Linear Unit (ReLU). 2020. Available online: https://machinelearningmastery.com/rectified-linear-activation-function-for-deep-learning-neural-networks/ (accessed on 21 May 2022).
- Sarraf, S.; DeSouza, D.D.; Anderson, J.; Tofighi, G. DeepAD: Alzheimer’s disease classification via deep convolutional neural networks using MRI and fMRI. bioRxiv 2016. [Google Scholar] [CrossRef]
- Afzal, S.; Maqsood, M.; Nazir, F.; Khan, U.; Aadil, F.; Awan, K.M.; Mehmood, I.; Song, O.-Y. A data augmentationbased framework to handle class imbalance problem for Alzheimer’s stage detection. IEEE Access 2019, 7, 115528–115539. [Google Scholar] [CrossRef]
- Jordan, J. Normalizing Your Data. 2018. Available online: https://www.jeremyjordan.me/batch-normalization/ (accessed on 21 May 2022).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref. | Method | Author’s Name | No. of. Classes | Accuracy (%) |
|---|---|---|---|---|
| [12] | Multiscale deep learning | Lu nar | Binary Class (AD vs. HC) | 82.4 |
| [13] | Combined feature technique | Gupta nar | Binary Class (AD vs. HC) | 96.42 |
| [14] | Ensemble model | Ahmed et al. | Binary Class (AD vs. HC) | 94.03 |
| [17] | 2D CNN | Ieracitano et al. | Binary Class (AD, MCI) | 89.8 |
| [18] | CNN | Jain sun | Three class (NC, EMCI, LMCI) | 95.73 |
| [19] | Transfer Learning | Mehmood sun | Binary class (AD vs. NC) | 98.73 |
| [20] | Deep polynomial network | Shi et al. | Multiclass (AD vs. NC) | 55.34 |
| [21] | Siamese network | Liu et al. | Binary class (MCI vs. AD) | 92.72 |
| [22] | 3D CNN | Van et al. | Binary class (AD vs. MCI) | 97.52 |
| [24] | VGG16 | Jangel and Rator | Binary class (AD vs. NC) | 73.46 |
| [25] | 3D CNN | Ge et al. | Binary class (AD vs. NC) | 93.53 |
| [28] | 3D View model | Preferred sun | Binary class (AD vs. NC) | 95.11 |
| ConvNet Configuration | |||||
|---|---|---|---|---|---|
| A | A-LRN | B | C | D | E |
| 11 weight layers | 11 weight layers | 13 weight layers | 16 weight layers | 16 weight layers | 19 weight layers |
| Input (224 × 224 RGB image) | |||||
| Conv3-64 | Conv3-64 LRN | Conv3-64 Conv3-64 | Conv3-64 Conv3-64 | Conv3-64 Conv3-64 | Conv3-64 Conv3-64 |
| Maxpool | |||||
| Conv3-128 | Conv3-128 | Conv3-128 Conv3-128 | Conv3-128 Conv3-128 | Conv3-128 Conv3-128 | Conv3-128 Conv3-128 |
| Maxpool | |||||
| Conv3-256 Conv3-256 | Conv3-256 Conv3-256 | Conv3-256 Conv3-256 | Conv3-256 Conv3-256 Conv1-256 | Conv3-256 Conv3-256 Conv3-256 | Conv3-256 Conv3-256 Conv3-256 Conv3-256 |
| Maxpool | |||||
| Conv3-512 Conv3-512 | Conv3-512 Conv3-512 | Conv3-512 Conv3-512 | Conv3-512 Conv3-512 Conv1-512 | Conv3-512 Conv3-512 Conv3-512 | Conv3-512 Conv3-512 Conv3-512 Conv3-512 |
| Maxpool | |||||
| Conv3-512 Conv3-512 | Conv3-512 Conv3-512 | Conv3-512 Conv3-512 | Conv3-512 Conv3-512 Conv1-512 | Conv3-512 Conv3-512 Conv3-512 | Conv3-512 Conv3-512 Conv3-512 Conv3-512 |
| Maxpool | |||||
| FC-4096 | |||||
| FC-4096 | |||||
| FC-1000 | |||||
| Soft-max | |||||
| Model | VGG A | VGG B | VGG-C T | VGG D | VGG E | Our Work | |
|---|---|---|---|---|---|---|---|
| Train | Accuracy | 0.9876 | 0.8990 | 0.9800 | 0.9663 | 0.9143 | 0.9999 |
| F1-score | 0.9945 | 0.9185 | 0.9927 | 0.9837 | 0.9284 | 0.9998 | |
| Precision | 0.9945 | 0.9173 | 0.9906 | 0.9941 | 0.9706 | 0.9997 | |
| Recall | 0.9945 | 0.9197 | 0.9947 | 0.9735 | 0.8897 | 1.0000 | |
| Test | Accuracy | 0.7550 | 0.7480 | 0.8013 | 0.7415 | 0.7245 | 0.7746 |
| F1-score | 0.7696 | 0.7513 | 0.8040 | 0.7380 | 0.7097 | 0.7799 | |
| Precision | 0.7702 | 0.7372 | 0.7895 | 0.7761 | 0.7553 | 0.7744 | |
| Recall | 0.7697 | 0.7659 | 0.8191 | 0.7035 | 0.6693 | 0.7855 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tuvshinjargal, B.; Hwang, H. VGG-C Transform Model with Batch Normalization to Predict Alzheimer’s Disease through MRI Dataset. Electronics 2022, 11, 2601. https://doi.org/10.3390/electronics11162601
Tuvshinjargal B, Hwang H. VGG-C Transform Model with Batch Normalization to Predict Alzheimer’s Disease through MRI Dataset. Electronics. 2022; 11(16):2601. https://doi.org/10.3390/electronics11162601
Chicago/Turabian StyleTuvshinjargal, Batzaya, and Heejoung Hwang. 2022. "VGG-C Transform Model with Batch Normalization to Predict Alzheimer’s Disease through MRI Dataset" Electronics 11, no. 16: 2601. https://doi.org/10.3390/electronics11162601
APA StyleTuvshinjargal, B., & Hwang, H. (2022). VGG-C Transform Model with Batch Normalization to Predict Alzheimer’s Disease through MRI Dataset. Electronics, 11(16), 2601. https://doi.org/10.3390/electronics11162601