Abstract
Both hyaluronic acid (HA) and calcium hydroxylapatite (CaHA) fillers have well-established indications in cosmetic medicine. Nevertheless, limited data are available on the effectiveness of combining CaHA and HA. The purpose of this report was to demonstrate the safety, tolerability, and clinical and ultrasonographic improvement of facial skin laxity using a blending technique that admixes HA and CaHA. Fifteen regular patients, including three men, between 25 and 71 years of age were reported. The participants were subjects who came regularly to the dermatologic office seeking a lifting effect without surgery. They were submitted to injection of an admixture of HA and CaHA and followed for 180 days. The clinical assessment consisted of photographic evaluation by two blind investigators, and a consensual subjective evaluation was performed by the physicians (PGAIS) using the five-point Global Aesthetic Improvement Scale. Dermal thickness was analyzed in jaw areas using high-frequency ultrasound. Subjects completed a satisfaction questionnaire with responses scored according to the five-point Global Aesthetic Improvement Scale (GAIS) to evaluate patient satisfaction. After 180 days of follow-up, clinical assessments by blinded physicians found that all patients improved. All the participants were highly satisfied with the results and reported exceptional improvement. Dermal thickness increased by 9.4% (8.2–10.8%), 14.0% (12.2–15.9%), and 18.8% (16.2–21.9%) at D90, D120, and D180, respectively, by ultrasonography. In conclusion, an injection technique using an admixture of CaHA and HA fillers was well tolerated, offering high satisfaction and long-lasting progressive benefits. The authors believe that this procedure optimizes the treatment time and results because HA promotes early volume restoration and CaHA stimulates long-term dermal remodeling through the synthesis of collagen and elastin.
1. Introduction
Minimally invasive facial procedures, rather than plastic surgery, are preferred by most patients in Latin America, of all ages, seeking natural results and less downtime [1]. Therefore, innovative office-based procedures should be developed to meet patients’ aesthetic expectations regarding facial shape, structure, and proportions, as well as the effects of aging on their faces. New indications for products and techniques evolve based on creative ideas and thorough clinical observation, leading to changes in our aesthetic practices [2].
Both calcium hydroxylapatite (CaHA) and hyaluronic acid (HA) fillers have well-established indications in cosmetic medicine. HA is a glycosaminoglycan that has become the most popular dermal filler for volume augmentation in areas of volume loss. CaHA is a biodegradable filler composed of synthetic calcium hydroxylapatite microspheres (25–45 μm in diameter) suspended in an aqueous carboxymethyl carrier gel [3,4,5,6]. Following a CaHA injection, the gel is slowly absorbed, while the microspheres are free to stimulate collagen and elastin production, angiogenesis, and dermal cell proliferation, improving the skin’s mechanical characteristics. CaHA is slowly replaced by autologous connective tissue in a process called a “regenerative pathway” [3,4].
Data regarding the clinical effectiveness of the simultaneous injection of CaHA and HA are scarce [2,7]. This study aimed to demonstrate the clinical and ultrasonographic improvement of facial appearance using an injection technique that combines HA and CaHA.
2. Materials and Methods
A retrospective report of fifteen regular patients, including three men, between 25 and 71 years of age was performed. The participants were subjects who came to the dermatologic office (Clínica Bravo—Rio de Janeiro, Brazil) seeking a lifting effect without surgery. They were submitted to the injection of an admixture of HA and CaHA and followed periodically for 180 days.
Documented data included age, health issues, the treatment indication, the CaHA-HA admixture, the injection sites, the injection technique, the injection depth, the injected volume, and adverse events. Adverse events were classified according to US FDA definitions as immediate, early, or delayed. Immediate adverse events present within minutes to hours post-procedure. Early adverse events present within days or weeks. Delayed adverse events present months to years later.
At the first visit (D0), all participants received instructions regarding the injection procedures, photography, and ultrasound evaluation. These procedures were performed in compliance with the principles of good clinical practice, all applicable laws and regulations, and the ethical principles for clinical research outlined in the Declaration of Helsinki. Written informed consent was obtained before enrollment, and all participants agreed to the publication of their pictures.
2.1. Technical Procedure
The procedure first involved an individual facial assessment and injection of an admixture of HA and CaHA.
To prepare the admixture of CaHA and HA, a 5.0 mL sterile polypropylene syringe was connected to a syringe with 1.5 mL of CaHA (Radiesse PlusTM; Merz, Mascot, Australia) using a female-to-female Luer lock connector. In the second step, the syringe of CaHA was removed from the Luer lock connector, and another 5.0 mL sterile polypropylene syringe filled with 2.0 mL of HA filler (Belotero IntenseTM, 25.5 mg/mL, Merz Aesthetic) was firmly connected to the first 5.0 mL sterile polypropylene syringe with CaHA via the female-to-female Luer lock connector, and these two contents were mixed until they formed a homogeneous mixture of 3.5 mL of CaHA and HA filler.
Mixing was performed with 10 strokes, and each mixing stroke consisted of one complete compression of the 5.0 mL syringe plunger followed by another complete compression of the counterpart 5.0 mL syringe (Figure 1A).
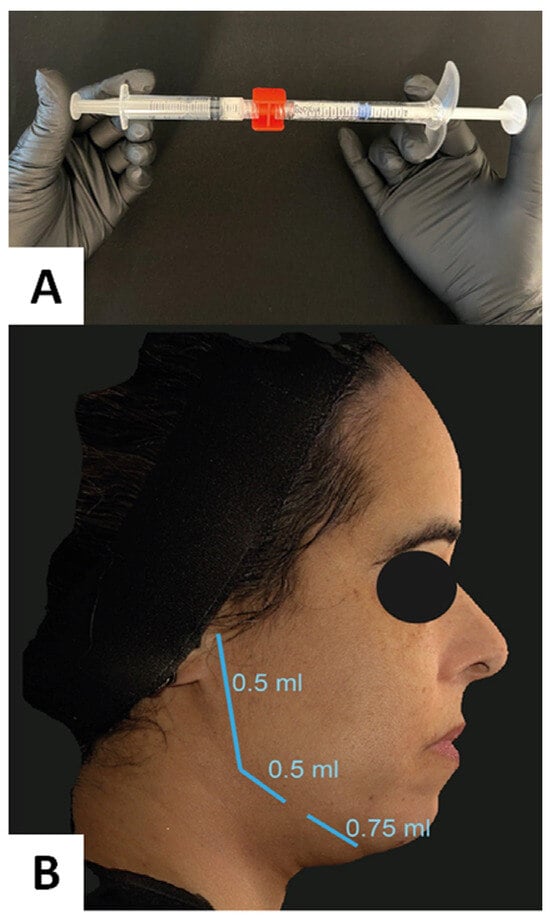
Figure 1.
(A) Demonstration of the mixing process of the two products. Ten complete strokes are necessary for a suitable admixture. (B) Schematic representation of the areas of the linear retroinjection with the cannula and the volumes of the admixed solution.
After complete mixing, a 22-gauge injection cannula was fixed to the syringe containing the admixture for the procedure.
The HA-CaHA admixture was distributed to the jaw areas, on both sides, subcutaneously, using the fan technique with a 22G cannula, after making an entry hole with a 21G needle, next to the lowest point of the post-jowl sulcus, which is usually located at the point separating the masseteric zone from the buccal zone (Figure 1B). The same physician performed all treatments.
This is an area where the facial artery usually crosses the inferior aspect of the mandible, and fibrous bands attach the periosteum to the subdermal layers. Care must be taken not to inject the filler in the apex of the jowl, as this would worsen the appearance of the jowl.
Injections were initiated in one entry point posteriorly at the inferior edge of the angle of the mandible (jowl area) in the deep subcutaneous tissue, using a 5 cm 22G cannula. Seven 0.25 mL linear back injections were performed, totaling 1.75 mL per side, to reinforce the jaw angle.
The patients were instructed that the regions that had undergone the injections should not be massaged.
The optimal candidates for the procedure are individuals exhibiting mild to moderate facial skin laxity. The procedure is contraindicated in cases of pregnancy, autoimmune diseases, individuals under the age of 18, those who are immunosuppressed, or those with permanent facial implants (e.g., silicone, PMMA). Additionally, it is contraindicated for individuals who have received temporary facial fillers in the preceding 12 months.
2.2. Data Analysis
The primary outcomes of the study were clinical evaluation, dermal thickness, and patient satisfaction. Standardized images were obtained using Vectra 3D imaging systemTM (Canfield, NJ, USA) at D0, D30, D60, D90, D120, and D180 and its vector analysis program (markerless tracking). It provides a dynamic assessment of skin surface changes. Skin surfaces are automatically aligned, tracked, and mapped.
Two board-certified dermatologists were engaged in this study as blind investigators to evaluate changes in the sagging skin of the jawline using the Physician Global Aesthetic Improvement Scale (PGAIS), an independently rated overall cosmetic improvement scale, 120 days after the procedure. PGAIS is an ordinal subjective scale that rates the change in global appearance as worse, no change, improved, much improved, or very much improved.
Dermal thickness was analyzed at jaw areas using a linear 18 MHz transducer, a high-frequency ultrasound Logic E device (GE Healthcare) with a high-frequency linear probe (L18i-RS), at D0, D90, D120, and D180 by the same experienced radiologist. This assessment was made in the jaw regions. The right side was treated with HA-CaHA, and a small region on the left preauricular region (1 cm2) received no treatment, serving as a control.
Patient satisfaction was evaluated by subjects using a satisfaction questionnaire, the five-point Subject Global Aesthetic Improvement Scale (SGAIS). Subjects were asked about possible adverse events using the standardized questionnaire, and an expert dermatologist visually examined the treatment area at each follow-up visit.
Categorical and ordinal data are represented by percentiles [8]. Quantitative data are represented by the mean and standard deviation (SD) if normality was evidenced by the Shapiro–Wilk test [9]. Longitudinal data were evaluated using a generalized linear mixed model, and post hoc analysis was performed using a sequential Šidák procedure. Significance was established as p < 0.05 [10].
3. Results
All 15 participants underwent the combined procedure and completed the 180-day follow-up. The mean (SD) age was 47.0 (14.2) years, and the Fitzpatrick phototypes were: type II, two participants; type III, six participants; and type IV, seven participants.
No additional applications or protocol deviances regarding volume or dilution were required. No infections, nodules, ischemia, or other relevant adverse events were noted, but mild pain (in four patients), ecchymosis (in two patients), and local edema (in five patients) occurred after the injections, but they resolved spontaneously.
All the participants evidenced improvement in facial laxity based on a combination of volume replacement in the jaw area, increased dermal thickness, improved definition of the mandibular angle, and a sharper contour (Figure 2).

Figure 2.
Combined technique for facial filling with the blending of hyaluronic acid (Belotero IntenseTM) and calcium hydroxylapatite (RadiesseTM). Clinical pictures at D0 (left) and D180 (right).
The evaluation of the facial volume changes and the vectors evidenced by the comparison of D0 and D180 3D images are presented in Figure 3. The gain in volume is more prominent at the jaw angle. The arrows (vectors of the direction of the movement) in red show greater lifting toward the jaw angle. In the case of the patients evaluated in this study, this technology can confirm the patients’ improvements with detailed evidence through the review of the results and refinement of the technique.
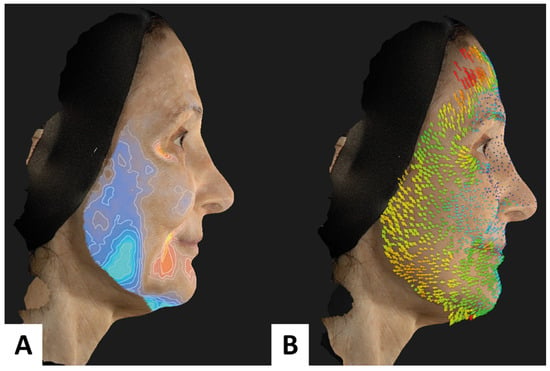
Figure 3.
Combined technique for facial filling with hyaluronic acid (Belotero IntenseTM) and calcium hydroxylapatite (RadiesseTM). Volume (A) and vector (B) evaluation.
There were no major adverse events related to the procedure. All the participants reported being highly satisfied at D120, and all their GAIS scores resulted in 1 (exceptional improvement). Among the physicians, the rates for PGAIS scores were: PGAIS 1 (very much improved), two cases (13%); PGAIS 2 (very improved), eleven cases (73%); and PGAIS 3 (improved), three cases (13%).
The dermal thickness, assessed by high-frequency ultrasonography on the jaw throughout the follow-up, is presented in Figure 4 and Figure 5, evidencing an increase in the dermal thickness only on the side treated with the HA-CaHA admixture. A progressive mean (CI 95%) increase in dermal thickness was noted: 0.5% (0.1–0.9%), 5.2% (4.1–6.2%), 9.4% (8.2–10.8%), 14.0% (12.2–15.9%), and 18.8% (16.2–21.9%) at D30, D60, D90, D120, and D180, respectively. The superior performance of CaHA compared with the control side was detected from D90 (p < 0.01).
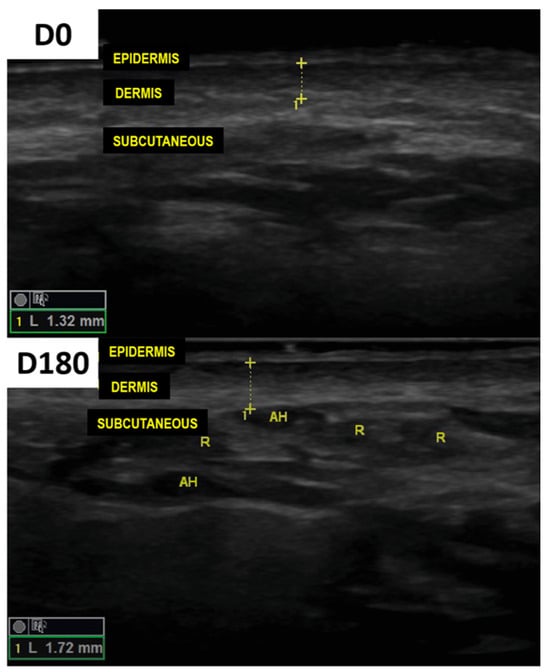
Figure 4.
High-frequency ultrasound from the preauricular area revealed a substantial increase in the thickness of the dermis from D0 to D180.
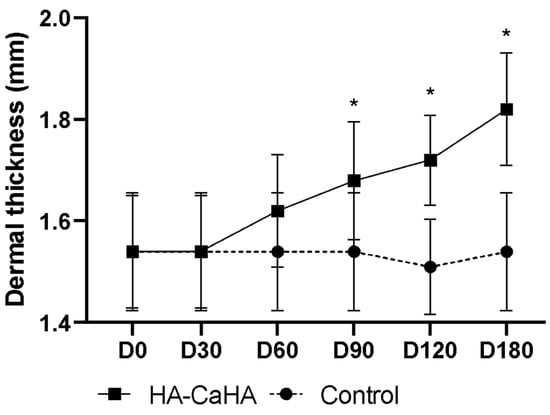
Figure 5.
Dermal thickness (preauricular area) as assessed by high-frequency ultrasonography throughout the follow-up (* p < 0.01 between treatments).
4. Discussion
Minimally invasive (nonsurgical) facial cosmetic procedures (e.g., neurotoxin, fillers, and biostimulators) have a low rate of adverse effects and a brief downtime, resulting in a natural appearance for facial beautification [11]. Furthermore, these procedures can be repeated periodically according to individual cosmetic demands [12].
Dermal fillers give the face a youthful appearance by augmenting areas of volume loss, contour defects, and wrinkles resulting from facial aging [4,6]. A sagging jawline is a key indicator of facial aging and can significantly affect a subject’s appearance. A well-defined jawline signifies youth and increases the attractiveness of the lower face. For women, the most aesthetically desired angle is between 120 and 130 degrees. In men, the optimal angle is 130 degrees; less than 120 creates a squarer jawline, and greater than 130 creates a more oval jawline [13,14,15].
HA-based injectable fillers are currently the gold standard for volumization procedures in facial rejuvenation. The gel from the CaHA injection dissolves within the first three months, while the biostimulation of collagen lasts for months. However, CaHA sometimes undergoes unexpected early volume loss due to rapid gel absorption before neocollagenesis [16]. The authors hypothesize that the HA filler compensates for the volume loss that occurs when the gel dissipates from the microspheres in the CaHA filler before biostimulation is established.
High-frequency ultrasound is a reliable method for assessing dermal thickness; moreover, the dermal homogeneity of the pixels can represent the density of parallel fibers of dermal collagen [17].
The results suggest that dermatologists mix fillers to improve short- and long-term treatment outcomes, and increase volume. Additionally, some products with the combination of HA and CaHA for prompt injection have recently been introduced. A comparison of the efficacy and cost-effectiveness of admixing these substances or using pre-mixed commercial products is warranted.
By adding volume to support the soft tissues, biocompatible soft tissue fillers, such as CaHA and HA fillers with high elasticity (G prime), improve the definition of the jawline and create a rejuvenated and more youthful appearance [13].
Mixing HA to obtain volume restoration with CaHA to enhance collagen stimulation is an intriguing idea with promise [18,19]. This study has potential limitations due to the lack of a control group. However, facial aging is not thought to improve without intervention. Further studies are warranted to explore the injection technique and HA-CaHA proportion that yields the best results. The authors are following these patients for up to one year.
5. Conclusions
An injection technique that uses an admixture of CaHA and HA fillers was well tolerated, offering high satisfaction and long-lasting progressive benefits. The authors believe that this procedure optimizes the treatment time and results because HA promotes early volume restoration, and CaHA stimulates long-term dermal regenerative pathways, i.e., through the synthesis of collagen and elastin.
Author Contributions
Conceptualization, B.B., R.C., L.P. and L.B.; formal analysis, B.B. and M.E.; resources, M.E.; data curation, B.B. and M.E.; writing—original draft preparation, B.B., R.C., L.P. and L.B. All authors have read and agreed to the published version of the manuscript.
Funding
Merz has provided the hyaluronic acid and the calcium hydroxyapatite that were applied in the patients. Medical writing support was provided by Merz Brazil, following Good Publication Practice guidelines. APC was funded by Merz Brazil.
Institutional Review Board Statement
All procedures in studies involving human participants were performed in accordance with the Declaration of Helsinki (as revised in 2013). All patients provided informed consent for the case details and images to be published in this report. Institutional Review Board appraisal was not required or sought as this report was not part of a prospective or systematic investigation of filler treatments. Moreover, it followed general principles for routine CaHA, HA, and injection. Institutional approval was not required to publish these unidentified cases.
Informed Consent Statement
Written informed consent was obtained from all patients to publish their anonymized data in this paper.
Data Availability Statement
Data are available under contact with the corresponding author.
Acknowledgments
We would like to thank the patients who allowed us to publish their anonymized photos.
Conflicts of Interest
Bruna S. F. Bravo is a medical consultant of Merz, Allergan and L’Oréal; Laís Bezerra de Menezes Penedo declares no conflict of interest; Raquel de Melo Carvalho declares no conflict of interest; Mariana Calomeni Elias was hired for the ultrasonography exams of this study.
References
- Devgan, L.; Singh, P.; Durairaj, K. Minimally Invasive Facial Cosmetic Procedures. Otolaryngol. Clin. N. Am. 2019, 52, 443–459. [Google Scholar] [CrossRef] [PubMed]
- Felix Bravo, B.; Bezerra de Menezes Penedo, L.; de Melo Carvalho, R.; Amante Miot, H.; Calomeni Elias, M. Improvement of Facial Skin Laxity by a Combined Technique With Hyaluronic Acid and Calcium Hydroxylapatite Fillers: A Clinical and Ultrasonography Analysis. J. Drugs Dermatol. 2022, 21, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Lizzul, P.F.; Narurkar, V.A. The role of calcium hydroxylapatite (Radiesse) in nonsurgical aesthetic rejuvenation. J. Drugs Dermatol. 2010, 9, 446–450. [Google Scholar] [PubMed]
- de Almeida, A.T.; Figueredo, V.; da Cunha, A.L.G.; Casabona, G.; de Faria, J.R.C.; Alves, E.V.; Sato, M.; Branco, A.; Guarnieri, C.; Palermo, E. Consensus Recommendations for the Use of Hyperdiluted Calcium Hydroxyapatite (Radiesse) as a Face and Body Biostimulatory Agent. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2160. [Google Scholar] [CrossRef] [PubMed]
- van Loghem, J.; Sattler, S.; Casabona, G.; Cotofana, S.; Fabi, S.G.; Goldie, K.; Gout, U.; Kerscher, M.; Lim, T.S.; de Sanctis Pecora, C.; et al. Consensus on the Use of Hyaluronic Acid Fillers from the Cohesive Polydensified Matrix Range: Best Practice in Specific Facial Indications. Clin. Cosmet. Investig. Dermatol. 2021, 14, 1175–1199. [Google Scholar] [CrossRef] [PubMed]
- Keen, M.A. Hyaluronic Acid in Dermatology. Skinmed 2017, 15, 441–448. [Google Scholar] [PubMed]
- Lorenc, Z.P.; Bass, L.M.; Fitzgerald, R.; Goldberg, D.J.; Graivier, M.H. Composite Facial Volumization with Calcium Hydroxylapatite (CaHA) for the Treatment of Aging. Aesthet. Surg. J. 2018, 38, S18–S23. [Google Scholar] [CrossRef] [PubMed]
- Miola, A.C.; Miot, H.A. Comparing categorical variables in clinical and experimental studies. J. Vasc. Bras. 2022, 21, e20210225. [Google Scholar] [CrossRef] [PubMed]
- Miot, H.A. Assessing normality of data in clinical and experimental trials. J. Vasc. Bras. 2017, 16, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Miola, A.C.; Miot, H.A. P-value and effect-size in clinical and experimental studies. J. Vasc. Bras. 2021, 20, e20210038. [Google Scholar] [CrossRef] [PubMed]
- Akinbiyi, T.; Othman, S.; Familusi, O.; Calvert, C.; Card, E.B.; Percec, I. Better Results in Facial Rejuvenation with Fillers. Plast. Reconstr. Surg. Glob. Open 2020, 8, e2763. [Google Scholar] [CrossRef] [PubMed]
- Wollina, U.; Goldman, A. Long lasting facial rejuvenation by repeated placement of calcium hydroxylapatite in elderly women. Dermatol. Ther. 2020, 33, e14183. [Google Scholar] [CrossRef] [PubMed]
- Dallara, J.M.; Baspeyras, M.; Bui, P.; Cartier, H.; Charavel, M.H.; Dumas, L. Calcium hydroxylapatite for jawline rejuvenation: Consensus recommendations. J. Cosmet. Dermatol. 2014, 13, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Vazirnia, A.; Braz, A.; Fabi, S.G. Nonsurgical jawline rejuvenation using injectable fillers. J. Cosmet. Dermatol. 2020, 19, 1940–1947. [Google Scholar] [CrossRef] [PubMed]
- Waldman, S.R. Aesthetic Treatment of the Jawline and Perioral Area. Facial Plast. Surg. 2019, 35, 119–120. [Google Scholar] [CrossRef] [PubMed]
- Fakih-Gomez, N.; Kadouch, J. Combining Calcium Hydroxylapatite and Hyaluronic Acid Fillers for Aesthetic Indications: Efficacy of an Innovative Hybrid Filler. Aesthetic Plast. Surg. 2022, 46, 373–381. [Google Scholar] [CrossRef] [PubMed]
- de Caetano, V.N.L.; Soares, J.L.; Bagatin, E.; Miot, H.A. Reliable assessment of forearm photoageing by high-frequency ultrasound: A cross-sectional study. Int. J. Cosmet. Sci. 2016, 38, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Pavicic, T.; Few, J.W.; Huber-Vorländer, J. A novel, multistep, combination facial rejuvenation procedure for treatment of the whole face with incobotulinumtoxinA, and two dermal fillers-calcium hydroxylapatite and a monophasic, polydensified hyaluronic acid filler. J. Drugs Dermatol. 2013, 12, 978–984. [Google Scholar] [PubMed]
- Viscomi, B.; Faria, G.; Hernandez, C.A.; Perez, L.; Spada, J.; De la Fuente, V.; Muniz, M. Contouring Plus: A Comprehensive Approach of the Lower Third of the Face with Calcium Hydroxylapatite and Hyaluronic Acid. Clin. Cosmet. Investig. Dermatol. 2023, 16, 911–924. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).