1. Introduction
Colorectal cancer (CRC) is the third most common type of cancer worldwide, and its occurrence is responsible for nearly 10% of all deaths related to malignancies [
1]. Historically, the incidence of CRC has been low at ages younger than 50 years; however, in recent years, there has been a rising incidence of CRC at these ages [
2]. This emerging trend is prompting a rapid increase in the number of CRC cases in previously low-risk countries, a phenomenon ascribed to changes in dietary patterns and risk factors towards a more western lifestyle [
3]. The cornerstone of curative intent treatment for CRC remains surgical excision of the primary tumor [
4]. While this approach is curative for most patients, recurrence of CRC disease occurs in approximately 20% of patients [
5]. Therefore, after tumor resection, clinicians often have follow-up appointments with patients to detect any recurrence at an early and treatable stage. These follow-ups have unraveled the need for novel predictive prognosis biomarkers and well-established staging protocols to inform clinicians which patients will recur.
The American Joint Committee on Cancer first defined the Tumor Node Metastasis (TNM) staging system to inform on patients’ prognosis [
6]. Currently, TNM is the most widely used staging system for CRC, and its application in the clinic has been crucial to inform patients’ prognosis, also having a considerable and direct impact on the treatment that patients receive [
6]. However, clinical evidence suggests that the outcome of the disease varies significantly among patients within the same TNM stage [
7,
8,
9]. This is particularly noticeable at TNM stage II, wherein one-third of all patients may still die of recurrent disease [
10,
11]. Contrarily, patients at TNM stage III may be cured of the disease by surgery alone [
12]. As such, under or overtreatment may occur between stages determined by the TNM system, as previously demonstrated [
13,
14]. Additionally, the lack of consensus on the application of TNM staging and the constant update of revised versions are significant hurdles in comparing different cohorts [
9,
15,
16]. Therefore, clinical practice may benefit from the inclusion of other staging methodologies to discriminate patients who may benefit from additional therapies, such as adjuvant chemotherapies.
Over the last decade, there has been a progressive increase in our understanding of the tumor microenvironment, which prompted the identification of key players of the immune response to tumors. Particularly important and with prognostic potential in CRC are tumor-infiltrating lymphocytes (TIL), which are heterogeneous populations of T lymphocytes present in the tumor microenvironment [
17,
18,
19,
20,
21]. In this regard, the presence of CD8
+ T lymphocytes has been associated with good prognosis in different types of solid tumors [
22,
23]. This T lymphocyte population mediates anti-tumor activity through antigen-specific cytotoxicity and by producing anti-tumor cytokines, namely IFN-γ and TNF-α [
24,
25]. On the other hand, increased tumor infiltration by FoxP3-expressing T lymphocytes has been associated with reduced overall survival of patients with different types of cancer, including breast [
26], lung [
27], and cervical cancers [
28]. However, this association is not seen in all cancer types, as FoxP3
+ T lymphocyte infiltrates have been associated with good prognosis in other cancers, such as head and neck cancers [
29]. In colorectal cancer, FoxP3
+ T lymphocyte infiltrates have been associated with good and bad prognosis by different studies [
30,
31,
32,
33]. Taken together, these data warrant further investigation on the prognostic potential of FoxP3
+ T lymphocytes in colorectal cancer.
The analysis of immune infiltrates and their correlation with patients’ pathological records originated the development of staging methods based on the intratumor and invasive margin infiltration of CD3
+ and CD8
+ T lymphocytes [
34]. While the predictive capacity of TNM staging is more reliable than alternative methods, such as DNA content or genetic features, the analysis of tumor immune infiltrate has been suggested to surpass the TNM classification in multivariate analyses [
35]. Indeed, after adjusting for TNM stage, recent data suggest that the density of CD3
+ T lymphocytes remained as an independent prognostic factor [
36]. Furthermore, patients with low numbers of tumor-infiltrating CD8
+ T lymphocytes relapsed more independently of the T stage of the tumor [
19]. These data demonstrate the high prognostic utility of TILs in staging CRC patients. However, as discussed above, the interaction between different populations of TILs in the tumor or invasive margin may influence tumor progression or control. As such, it is crucial to define the prognostic utility of the different populations of T lymphocytes.
In this work, we analyzed the presence of lymphocyte infiltrates, specifically CD3+, CD8+, and FoxP3+ T lymphocytes, in CRC tumors including their invasive margins to evaluate their association with clinicopathological information and overall survival of patients. We did not find any associations between the presence and extent of intratumor T lymphocyte infiltrations with the clinical or pathological data of the patients. On the other hand, the infiltration of CD3+, CD8+, or FoxP3+ lymphocytes in the tumor invasive margins were associated with the pathogenesis of CRC, but only FoxP3+ T lymphocyte infiltrations were inclined to indicate favorable prognosis.
2. Materials and Methods
2.1. Patients Specimens
A total of 194 samples of colorectal cancer (CRC) at stage I to IV were used in this retrospective study. These samples were collected from patients diagnosed with CRC that underwent surgical excision of the primary tumor at the Hospital of Braga, Portugal, between January 2005 and January 2010. The CRC tissue extracted during the surgery was formalin-fixed and embedded in paraffin. Clinical and pathological data was available for 184 cases and was obtained through medical charts and pathology reports (
Table 1).
2.2. Immunohistochemistry
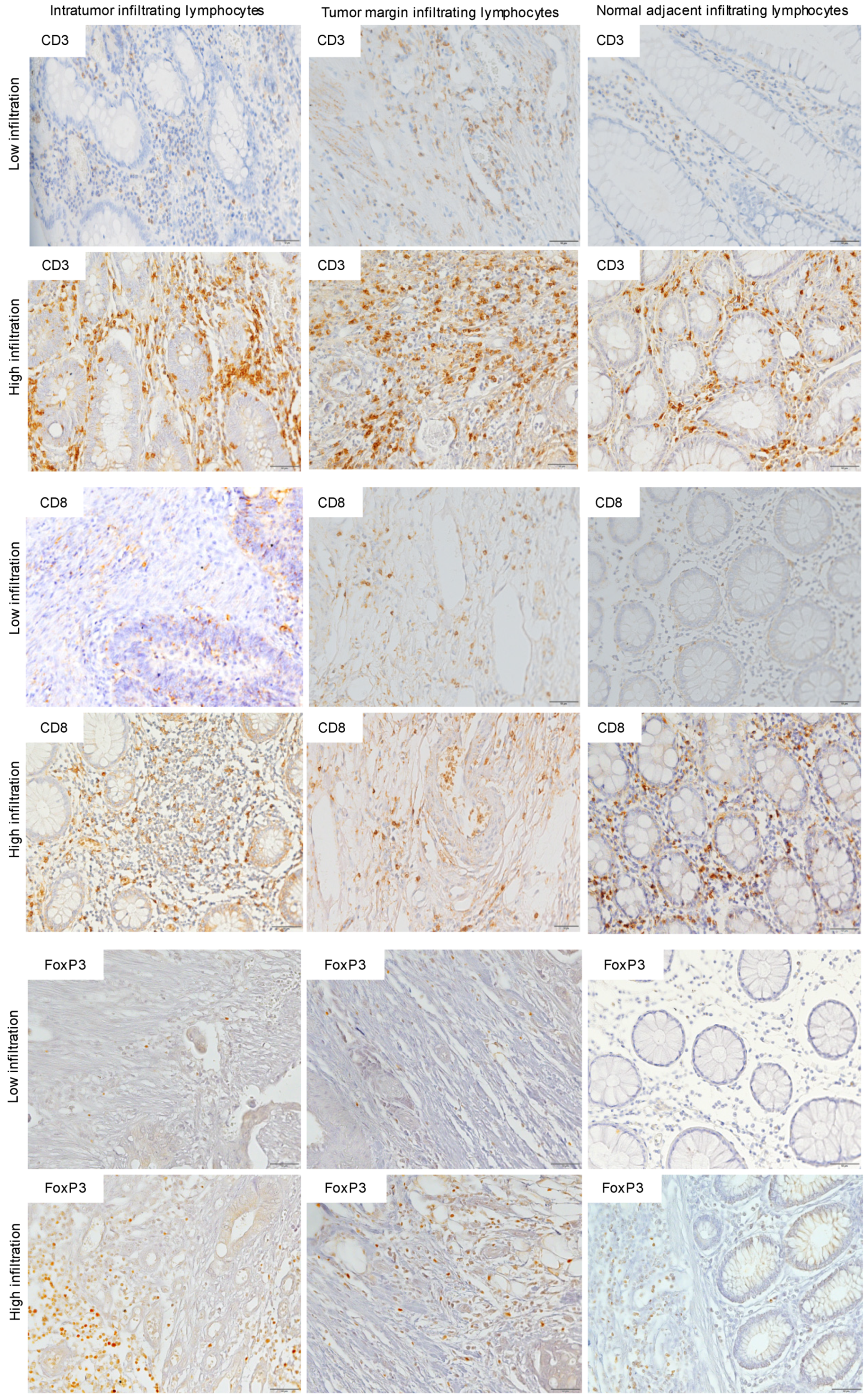
Tumor-infiltrating lymphocytes were detected by immunohistochemistry using antibodies against CD3 (MCA1477, BioRad), CD8 (ab4055, Abcam), or FoxP3 (14477782, Invitrogen). Briefly, whole-tissue sections were deparaffinized and hydrated to prepare the tissue for the staining. The slides from whole-tissue sections were incubated for 30 min in citrate buffer at 96 °C followed by incubation in hydrogen peroxide for 10 min at room temperature (RT). The slides were then incubated for 1 h with blocking solution (PBS with 5% BSA and 0.05% Tween 20) before incubation with primary antibodies at 4 °C for 16 h. After washing with PBS, the slides were incubated with biotinylated-secondary antibodies for 1 h at RT. Slides were then incubated with streptavidin for 1 h followed by an incubation with chromogen (DAB; Dako) for 10 min, and then counterstained with hematoxylin. Amygdala sections were used as positive controls.
Immunostaining analysis was used to determine the presence of CD3, CD8, or FoxP3 infiltrates in the tumor, tumor invasive margins, and normal adjacent colon epithelium using an Olympus BX41 microscope. Immunostaining was considered positive whenever there was cytoplasmatic and membrane staining for CD3, membrane staining for CD8, and nuclei staining for FoxP3. Grading of the immunostaining was performed in a blind fashion by consensus of two experienced pathologists, without having prior knowledge of the pathological stage or any other clinical or follow-up data for each case. Briefly, all samples were first analyzed under the microscope at a magnification of 100× to determine the extent of infiltration for each marker. From this analysis, the grade of CD3 and CD8 infiltration was categorized as <10%, 10–50%, or >50%, and the grade of FoxP3 infiltration was categorized as <10%, 10–30%, or >30%, as the expression of this marker was less extensive than of CD3 or CD8. Ten high magnification fields (×400) from each region of the tumor were then semi-quantitatively analyzed to determine the number of lymphocytes that stained positive for each marker.
For statistical analysis, each section was then classified as either low (<50%) or high (>50%). Representative images (
Figure 1) were obtained under brightfield microscopy (Olympus BX61) and were recorded with a digital camera (DP70) using the Cell∧P software.
2.3. Statistical Analysis
Statistical analysis was performed using the Statistical Package for the Social program Science (SPSS), version 24.0, SPSS Inc.®, Chicago, IL, USA.
Simple descriptive analyses were performed, determining the total number of cases and relative frequencies for each clinical-pathological factor. To assess the existence of any association of clinical or pathological data with immunohistochemistry results, Pearson’s chi-square test and Fisher’s exact test (scattered data) were performed. Survival analysis was performed using Kaplan-Meier curves and significant differences were determined by the log-rank test. Survival was defined between the period of analysis and death from any cause. Patients who quit the study were censored on the date of the last contact. Confidence values (p) below 0.05 were considered statistically significant.
2.4. Ethics Statement
The study was approved by the Ethics Committee for Research in Life and Health Sciences at University of Minho (CEICVS 004/2020) and by the Ethics Committee of Hospital de Braga (32/2013).
4. Discussion
The interaction between tumor cells and the immune system has prompted the quantification of immune infiltrates, particularly T lymphocytes, as prognostic markers for colorectal cancer (CRC) [
35]. Herein, we analyzed the presence of lymphocyte infiltrates (CD3
+, CD8
+, or FoxP3
+ T lymphocytes) inside the tumor and the tumor invasive margins of CRC samples to evaluate their prognostic potential. We were not able to find any associations between the presence and extent of intratumor T lymphocyte infiltrates with the clinical or pathological data of the patients, indicating that, at least in our cohort, intratumor lymphocytes do not influence the pathogenesis of CRC. Crucially, when we perform the same analyses for the tumor margins, we found that the presence of high CD3
+, CD8
+, or FoxP3
+ T lymphocyte infiltrates were associated with TNM stages I-II, non-invasion of lymph nodes, and normal CEA levels. These data suggest that the presence of CD3
+, CD8
+, or FoxP3
+ T lymphocytes in the tumor invasive margins are associated with good prognostic indicators; however, we could not demonstrate any significant association between any of the T lymphocyte population analyzed and the overall survival of the patients.
In recent years, the analysis of the immune reaction inside the tumor and its invasive margins has been suggested to predict disease-free survival and overall survival of CRC patients, independently of the local extent of the tumor or the invasion of regional lymph nodes (TNM stages I, II, and III) [
36]. The prognostic potential of the tumor immune reaction prompted the development of methodologies to quantify, in situ, the extent of immune infiltrates, particularly CD3
+ and CD8
+ T lymphocytes [
35]. Several studies show that high infiltrations of CD3
+ and/or CD8
+ T lymphocytes within CRC tumors and their invasive margins were associated with early stages of the disease (TNM stages I-II) and other good prognostic indicators, including absence of lymph node metastasis and distant metastasis [
19,
38]. Our study corroborated these observations but only for CD3
+ or CD8
+ T lymphocyte infiltrates in the tumor margins. Indeed, we were unable to find any association between the presence of CD3
+ or CD8
+ T lymphocyte infiltrates inside the tumor with markers of good CRC prognosis. In this regard, previous data has shown that, while CD8
+ T lymphocytes are directly capable of killing tumor cells and positively affect prognosis in a broad range of tumors [
39,
40,
41,
42], several other studies have shown no such correlation with prognosis [
43,
44]. As such, it is possible that the tumor microenvironment could modulate the effector function of CD8
+ T lymphocytes, and that this effect may depend on environmental variables such as the microbiome [
45,
46] or the tumor inflammatory status [
47]. In this regard, alteration in the intestinal microbiota has been shown to increase intestinal tumorigenesis by enhancing inflammation and promoting T cell exhaustion [
48]. Therefore, in addition to determining the presence of CD8
+ T lymphocytes, future studies should also focus on determining their effector function.
As discussed above, we also found that the high accumulation of FoxP3
+ T lymphocytes in the tumor margins was associated with TNM stages I-II, normal CEA levels, and, more importantly, with the non-invasion of lymph nodes. While FoxP3 can be transiently expressed by recently activated T cells in humans, the expression of this transcription factor also marks a population of regulatory T lymphocytes that can downregulate immune responses and, consequently, dampen anti-tumor immune mechanisms [
49,
50,
51]. Since we did not evaluate the function of FoxP3
+ lymphocytes, we were not able to discriminate between the regulatory and non-regulatory populations of FoxP3
+ lymphocytes. This is an important limitation of our study, as it prevented us from drawing any conclusion on the prognostic potential of the regulatory population of FoxP3-expressing lymphocytes. However, we suggest that the immunosuppressive capacity of the regulatory population of FoxP3-expressing lymphocytes may be important in CRC to control continuous and aggressive inflammatory responses that may favor tumor proliferation [
52,
53]. Our data are in accordance with previous data showing that high frequencies of FoxP3
+ T lymphocytes are associated with early T stages and absence of lymph node involvement [
31]. However, other studies also found associations between high FoxP3
+ T lymphocyte infiltrations and increased survival of CRC patients [
32,
54], which we did not find. Despite this, the high accumulation of these cells in the tumor margins resulted in an average gain of 14 months of the patients’ life expectancy (
p = 0.092). It is important to note that previous studies have also reported an association between high FoxP3
+ lymphocyte infiltrations and advanced CRC [
33,
55]. Additionally, the presence of FoxP3
+ T lymphocyte infiltrates were associated with poor prognosis in different types of cancers, including breast [
26], lung [
27], pancreatic [
56], ovarian [
57], and cervical [
28] cancers. These data show that the presence of FoxP3
+ T lymphocytes is not always associated with a good prognosis. As this population may downregulate immune responses, we suggest that their protective effect and their prognostic potential may depend on the inflammatory status of the tumor. As such, future research is required to consolidate the prognostic significance and the context wherein FoxP3
+ T lymphocytes have prognostic significance.
Our data point to the location of immune cells in relation to the tumor as an important factor for prognosis. Indeed, while we did not find any association between intratumor T lymphocytes with clinical or pathological data in the tumor margins, the extent of CD3
+, CD8
+, and FoxP3
+ lymphocyte infiltrations were all associated with good prognostic indicators. It is tempting to speculate that the intratumor-infiltrating T lymphocytes may be modulated by the tumor microenvironment, while in the tumor margins, these populations are able to maintain their functions for longer periods. As discussed above, this may explain the lack of association between the high intratumor infiltration of CD8
+ T lymphocytes and markers of good prognostic or even overall survival seen in other studies [
32,
35,
38]. Taken together, the distribution of immune cells, as well as their functional capability, may be important in predicting patients’ prognosis.
The potential limitations in analyzing tumor-infiltrating lymphocytes and perform direct comparisons with other studies include the various criteria used in different studies and the heterogeneity in the patterns of tumor-infiltrating lymphocytes [
58]. In our study, we accounted for this heterogeneity by staining large samples of tumor tissue with the different lymphocyte markers, including samples with normal adjacent tissue. The assessment of the immunostainings and analysis of the extent of lymphocyte infiltration in the different areas of the tumor by an experienced pathologist ensured that the heterogeneous expression patterns of the different markers used were seen in the context of the entire tumor section. Moreover, automated counting methods, which are not available in all laboratories and have been used in multiple studies, may not yield results comparable to the usual method. In all, further studies need to take into account the heterogeneity of lymphocyte infiltrates and evaluating methods.
In conclusion, our results indicate that only the presence of high infiltrates of CD3
+, CD8
+, and FoxP3
+ T lymphocytes in the tumor invasive margins are associated with good prognostic indicators and potentially limit the aggressiveness and spread of CRC. The presence of lymphocyte infiltrates inside the tumor was not associated with any clinical or pathological parameter. However, while previous studies showed an association between high lymphocytic infiltrations, particularly CD8
+, and survival of CRC patients [
35,
38,
59], we were unable to find any association between intratumor or tumor invasive margin lymphocyte infiltrations and overall survival. As such, while the consensus is that the tumor immune reaction may be a good prognostic indicator for CRC, and, in some cases, may even surpass the TNM staging system, our study suggests that this may not be the case for all populations.



 ,
, 


{kind=link}
{kind=link}