Abstract
Molecular diagnostic testing is assumed to enable fast respiratory pathogen identification and contribute to improved pneumonia management. We set up a prospective clinical trial at a tertiary hospital intensive care unit including adult patients suspected of severe pneumonia from whom a lower respiratory tract sample could be obtained. During control periods (CPs), routine testing was performed, and during intervention periods (IPs), this testing was completed with the FilmArray Pneumonia Panel plus test (FA-PNEU) executed 24/7. The main objective was to measure the impact of FA-PNEU results in terms of reduced time to targeted antimicrobial treatment administration. Over a 10-month period, analysis was performed on 35 CP and 50 IP patients. The median time to targeted antimicrobial treatment administration was reduced to 4.3 h in IPs compared to 26.4 h in CPs, with 54% of IP patients having FA-PNEU results that led to a treatment modification, of which all but one were targeted. Modifications included 10 (37%) de-escalations, 7 (25.9%) escalations, 3 (11.1%) regimen switches, and 7 (25.9%) complete antimicrobial discontinuations. FA-PNEU results were available with a 42.3 h gain compared to routine identification. This prospective study confirmed retrospective data demonstrating the benefit of FA-PNEU testing in severe pneumonia management of critically ill patients through improved antimicrobial use.
1. Introduction
Critical care physicians manage patients with various types of lung infection such as community-acquired pneumonia (CAP), hospital-acquired pneumonia (HAP), and ventilator-acquired pneumonia (VAP), all of them being associated with high morbidity and mortality [1,2]. International guidelines strongly recommend the initiation of empiric therapy for patients suspected of severe pneumonia and provide an algorithm towards the orientation of narrow- or broad-spectrum antibiotics according to the risk of multidrug-resistant pathogens and mortality [3,4]. Subsequent tailoring would then be possible according to respiratory sample culture results around day 2–3. Rapid molecular testing has the ability to drastically reduce this timeslot, enabling targeted antimicrobial treatment (TAT) to be administered more rapidly and limiting the use of broad-spectrum antibiotics and its consequences of increased toxicity, high costs, and antimicrobial resistance selection [5]. For several years, multiplex PCR approaches have been made available and offer sped-up results compared to microbiological routine testing with even better microorganism recovery and co-infection detection [6,7,8]. Observational studies further suggest improved pneumonia management of intensive care unit (ICU) patients through faster implementation of the optimal treatment, yet these conclusions have to be validated by prospective interventional studies [9,10,11]. We therefore set up a clinical exploratory trial with the aim of quantifying the impact of molecular diagnostic testing results on antibiotic administration in ICU patients with suspected pneumonia.
2. Results
Over a 10-month period, 104 ICU patients with a suspicion of severe acute pneumonia were enrolled, yet a lower respiratory sample was lacking for 11 of them. Subsequently, 93 patients were endorsed during the CPs (n = 37) and IPs (n = 56 patients). Ultimately, analysis was performed on 35 patients in the CPs and 50 patients in the IPs after exclusion due to early death and erroneous allocation.
CP and IP populations were statistically comparable in terms of age, sex ratio, severity scores, comorbidities (except for cardiovascular disorders), and final diagnosis, as detailed in Table 1. CAP was the main final diagnosis, representing 51.4% and 48% of the included CP and IP patients, respectively. HAP and VAP combined concerned 28.6% of CP patients and 26% of IP patients. The main pneumonia sources were bacterial (78.6% in CPs and 62.2% in IPs) and viral (7.1% in CPs and 13.5% in IPs). Pneumonia diagnosis was reasonably excluded following negative microbiological results in 20% of CP patients and 26% of IP patients.

Table 1.
Clinical characteristics and pneumonia data of patients included in the control and intervention periods.
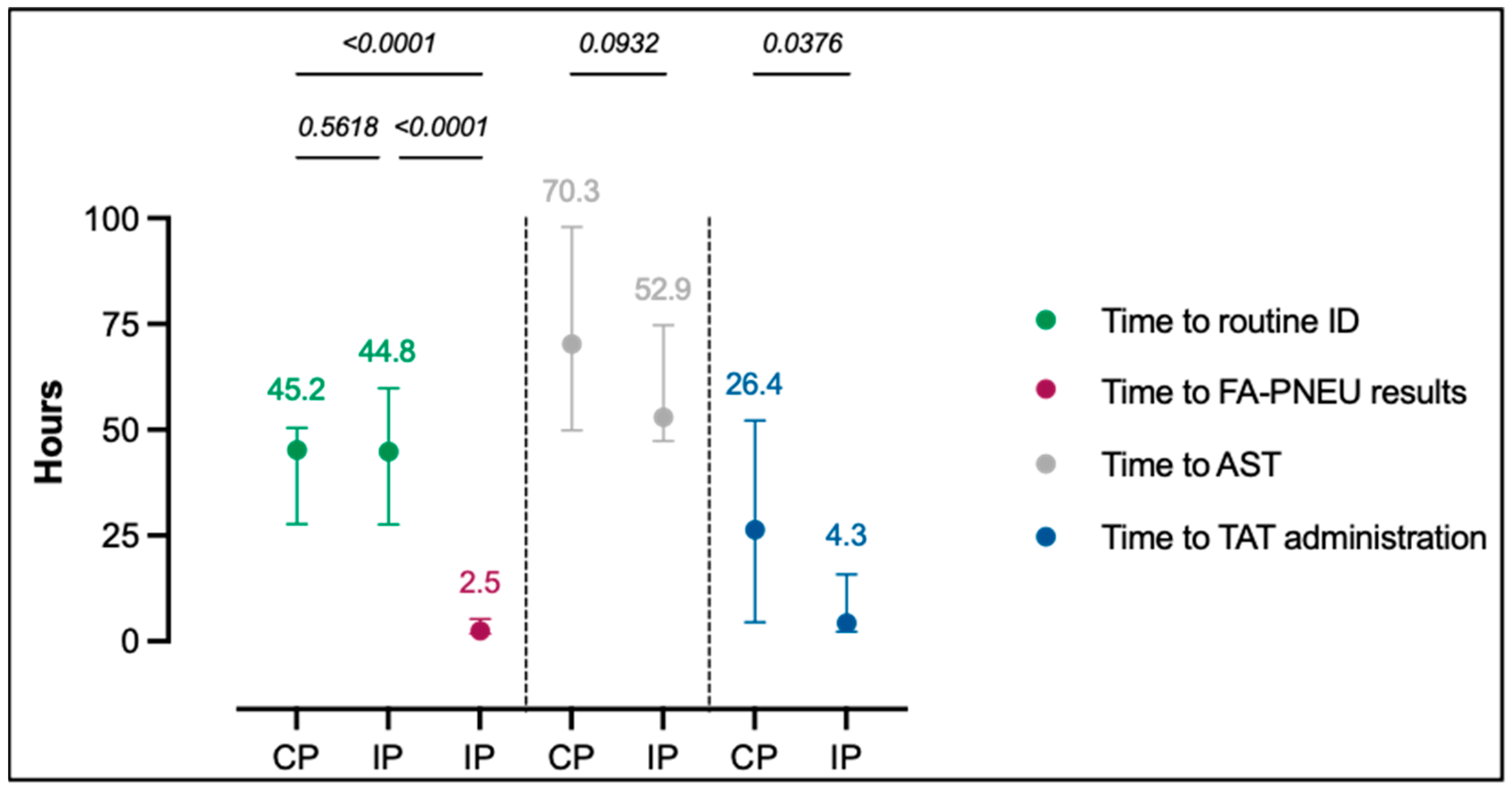
Figure 1 summarizes the median time to microbiological results and median time to the administration of TAT. FA-PNEU results were made available within a median time of 2.5 h (p < 0.001) following sample registration in the laboratory, while routine ID results required an extended median time to results of 45.2 and 44.8 h, respectively, in CPs and IPs (p = 0.5618). The median time to TAT administration was reduced to 4.3 h in IPs compared to 26.4 h in CPs (p = 0.0376).
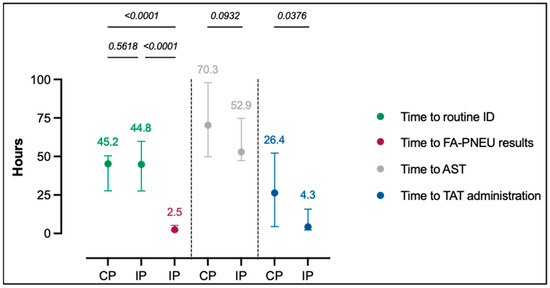
Figure 1.
Median time to microbiological results and to TAT administration in CPs and IPs. Dots represent median time and lines on each side of the dot represent interquartile ranges. Time data written above the vertical lines are expressed in hours. p-values < 0.05 were considered statistically significant. AST: antimicrobial susceptibility testing, CPs: control periods, FA-PNEU: FilmArray Pneumonia Panel plus test, ID: identification, IPs: interventional periods, TAT: targeted antimicrobial treatment.
The direct communication of FA-PNEU results in IPs led to sped-up antimicrobial modifications in 27/50 (54%) patients, as detailed in Table 2. Modifications included 10 (37%) de-escalations, 7 (25.9%) escalations, 3 (11.1%) regimen switches, and 7 (25.9%) complete antimicrobial discontinuations. All treatments initiated following FA-PNEU results were TAT, except for one patient for whom vancomycin was initiated following the FA-PNEU detection of a ≥107 copies/mL Staphylococcus aureus combined with the mecA/C and MREC resistance gene. For the latter, routine testing led to the monomicrobial growth of numerous oxacillin-susceptible S. aureus colonies. The patient was therefore ultimately treated with flucloxacillin.
Table 2.
IP ICU patients with a modified antimicrobial treatment following FA-PNEU result communication.
28-day mortality in IPs concerned 10/50 (20%) patients and 14/35 (40%) patients in CPs. The median ICU length of stay was 3 days and 21 h and 5 days and 3 h in, respectively, IPs and CPs. p-values were not statistically significant for the latter outcomes.
A comparison of FA-PNEU and IP patient routine testing results for the qualitative analysis of the 15 on-panel typical bacteria led to an overall PPA of 100% (34/34) and NPA of 97% (685/706). The main bacteria exclusively detected by FA-PNEU were H. influenzae (9), S. pneumoniae (3) and S. aureus (3). During IPs, routine analysis retrieved six respiratory viruses. FA-PNEU testing also detected the latter respiratory viruses, yet it identified four additional viruses not requested through routine testing. Four of the five resistance genes detected with FA-PNEU were in concordance with the phenotypical AST results. However, one detection of the mecA/mecC + MREJ marker was discordant with a culture-growing oxacillin-susceptible S. aureus.
3. Discussion
In this clinical exploratory trial, 52% of all IP ICU patients benefited from an accelerated TAT initiation following FA-PNEU results with a global median time reduction of 22.1 h towards TAT compared to CP patients. Similarly, in a retrospective study on adult hospitalized patients with lower respiratory tract infections, Buchan et al. measured potential for appropriate antimicrobial modifications following FA-PNEU results in 52.5% of the evaluable patients, yet they also reported inappropriate modifications in 18.2% [8]. In another retrospective multi-center study from Monard et al., early adaptation of antimicrobial therapy following FA-PNEU testing was measured at 77%, mainly consisting of de-escalation [10]. In our study, de-escalation and total treatment discontinuation accounted for 62.9% of all modifications following FA-PNEU results. The latter observations hereby strongly emphasize the usefulness of rapid molecular testing in the reduced use of broad-spectrum antibiotics. A Greek ICU team confronted on a daily basis with high rates of multidrug-resistant pathogens detected significant broad-spectrum antibiotic savings following the implementation of rapid molecular testing of severe CAP, HAP, or VAP among ICU patients [11]. Sped-up antibiotic tailoring is of major importance as it has been widely demonstrated that the use of broad-spectrum antibiotics also entails adverse effects. An impressive 20% increase in the odds of death was calculated among septic patients receiving unnecessary broad-spectrum antibiotics in an extensive cohort study including 17,430 culture-proven septic patients operated by Rhee et al. [12]. With caution for possible confounding factors, the authors partially explained this higher mortality rate by increased adverse effects, acute kidney injury, and Clostridium difficile infections. Conversely, inadequate empiric treatment was also associated with 20% higher odds of death, confirming the urgent need for rapid diagnostic tests. A Danish team performed a prospective randomized evaluation of FA-PNEU testing in guiding the treatment of patients suspected of CAP at an emergency unit [13]. Interestingly, despite an increase in more targeted antibiotic prescription, FA-PNEU testing did not impact the prescription rate of no or narrow-spectrum antibiotics 4 h after patient admission. Data analysis further failed to identify any difference in relation to ICU admissions, re-admissions within 30 days, length of stay, 30-day mortality, and in-hospital mortality. The discussed explanations were the very low national antimicrobial resistance level and the low number of events considering mortality and ICU transfer hampering the measurement of significant outcomes. Similarly, in our study, 28-day mortality and ICU length of stay were not statistically different between IPs and CPs. Yet, the latter outcomes need to be considered with caution as the sample size is limited.
The practical set-up of rapid molecular diagnostic testing of severe pneumonia is a key component to consider during implementation. In our setting, FA-PNEU testing was performed 24/7, allowing a median time to results of 2.5 h starting from laboratory sample registration. Similarly, Crémet et al., performing FA-PNEU testing upon the sample’s laboratory arrival, reported a median turnaround time from sample collection to results of 4.3 h [6]. However, not all laboratories have the required manpower at all times nor are they necessarily in the same geographical location as the hospital. Point-of-care molecular testing has extensively proven its efficacy in emergency settings with significant reductions in antibiotic use, lengths of stay, and timely antiviral use through the rapid detection of influenza and SARS-CoV-2 [14,15]. Moreover, the latter observations could trigger a reflection on safely broadening molecular testing at the ICU patient’s bedside with severe pneumonia syndromic testing, knowing the short and straightforward sample preparation of the available commercial approaches.
FA-PNEU performances in our study were very similar to ones previously observed in various evaluation studies equally reporting >95% PPA and NPA and underlining culture-negative FA-PNEU detection of a consistent number of S. aureus and Haemophilus influenzae [8,16]. Common explanations of these discordances were low strain concentration, empirical antibiotic coverage of detected bacteria preceding sample collection, and the presence of “normal oral flora” possibly obscuring strain culture detection, hereby stressing the added value of FA-PNEU testing in the latter circumstances. Attention must be paid to the detection of the mecA/C and MREC resistance genes since false-positive detections have also been reported by other teams [6,16,17].
A regularly reported drawback of molecular testing is the qualitative detection of DNA rather than the numbering of viable microorganisms. To partially overcome this issue, FA-PNEU bacterial detection comes with semi-quantitative results, enabling the clinician to distinguish between colonizing strains and clinically relevant pathogens. Several teams suggested a positivity threshold below which the clinician was advised not to consider the identified bacteria for antimicrobial treatment [6,11]. Defining these thresholds should be part of a set of guidelines helping clinicians in the interpretation of molecular diagnostic results, knowing that antimicrobial stewardship programs are absolutely essential to reach significant clinical outcomes and cost-effectiveness for molecular tools [18,19,20].
Alongside the clear benefits of rapid molecular pneumonia diagnostic tests, consideration needs to be given to the inconveniences. First, these molecular approaches allow the detection of a large yet limited panel of respiratory pathogens. As an example, the evaluated FA-PNEU fails to detect potential nosocomial pneumonia bacterial pathogens including Citrobacter koseri, Morganella morganii, and Stenotrophomonas maltophilia. A very recent review article by Moy et al. performed a meta-analysis on the diagnostic performances of FA-PNEU for the detection of respiratory bacterial pathogens in 8968 respiratory specimens. They concluded that 9.3% of bacteria detected in a culture were not included in the panel [21]. Similarly, these tests detect broad-spectrum resistance genes that clearly do not cover all currently encountered beta-lactamases. As a result, lower respiratory tract sample cultures, the identification of significantly growing bacterial colonies, and phenotypical antimicrobial susceptibility testing remain essential. Secondly, the high cost of rapid molecular systems and their cartridges is a major barrier to their clinical routine diagnostic implementation. It is assumed that certain outcomes, such as reduced antibiotic consumption or a reduced length of stay, could compensate for the molecular testing investment; however, the valuable literature remains very limited and heterogeneous in its conclusions, hereby highlighting the urgent need for broad and well-designed randomized controlled trials [22,23].
Our study’s main drawback is the limited number of included patients. Initiated in 2019, the study was interrupted after a 10-month period following the meteoric onset of the COVID-19 pandemic. The limited number of patients in this study also resulted in its statistical weakness to significantly measure additional patient outcomes such as ICU lengths of stay and mortality rates. Similar yet broad randomized controlled trials are ongoing and intend to give a clear picture on the latter outcomes [24,25].
In summary, this preliminary prospective randomized trial confirmed retrospective data by demonstrating the benefit of FA-PNEU testing in severe pneumonia management of ICU patients and highlight the advantages and inconveniences to consider prior to implementation. Additional clinical impact and cost-effectiveness studies should enable the widespread integration of rapid molecular testing in the routine management of severe pneumonia.
4. Materials and Methods
4.1. Study Design and Setting
The prospective trial was conducted at the Cliniques universitaires Saint-Luc, a tertiary Belgian hospital, with a 22-bed medical surgery ICU. Between June 2019 and March 2020, all critically ill adult patients suspected of severe acute pneumonia were considered for enrolment, yet exclusively those from whom a lower respiratory tract sample could be obtained were ultimately included.
The control (CPs) and intervention periods (IPs) followed each other for consecutive 2-week periods. During the CPs, routine semi-quantitative bacterial cultures were performed followed by identification (ID) and antimicrobial susceptibility testing (AST) on all relevant strains.
4.2. Microbiological Testing of the Lower Respiratory Tract Samples
Routine diagnostic testing for viruses (immunofluorescence) and atypical bacteria (molecular) as well as urinary antigen testing was left to the clinician’s discretion.
During the IPs, additional molecular testing was performed 24/7, and results were immediately provided electronically and by direct phone communication to the ICU clinician pursuing antimicrobial optimization. The selected molecular test was the FilmArray Pneumonia Panel plus test (FA-PNEU, BioFire Diagnostics, Salt Lake City, UT, USA), an automated multiplex PCR test allowing the direct detection of 15 bacteria with a semi-quantitative value, 3 atypical bacteria, 9 viruses, and 7 antimicrobial resistance genes within 1 h and 15 min. Semi-quantitative measurements were reported in 104, 105, 106, or ≥107 genomic copies/mL. A threshold at ≥106 genomic copies was suggested in order to consider the detected bacteria as pathogens rather than colonizing organisms. Additionally antimicrobial stewardship guidelines were set up to guide the clinician in the selection of the most appropriate and targeted antibiotherapy following FA-PNEU results in accordance with the local resistance epidemiology. Yet, final therapeutic decisions were left to the discretion of the treating ICU clinician.
4.3. Measured Outcomes
The main outcome of the study was measurement of the impact of the FA-PNEU results in terms of reduced time to TAT administration in the IPs versus the CPs. The secondary outcomes were 28-day mortality and ICU length of stay. Additional data such as time to FA-PNEU results, time to ID, and time to AST results were compared between the CPs and IPs. Bacterial, viral, and resistance gene detection of the FA-PNEU was ultimately compared to available IP patient routine test results.
Clinical characteristics, comorbidities, and pneumonia data were compared for all patients included in the CPs versus IPs to evaluate the similarity of the 2 study populations. Among clinical characteristics, we registered patients’ age, sex, and severity scores including APACHE II (Acute Physiology and Chronic Health Evaluation II) and SOFA (Sequential Organ Failure Assessment) scores. Compared comorbidities included active malignancy, cardiovascular disorder, chronic lung disease, diabetes, neutropenia (<500 neutrophils/μL), and organ transplant. Among the pneumonia data, we analyzed the final diagnosis and the microbiological source.
4.4. Data Handling and Statistical Analysis
Statistical analyses were performed using GraphPad Prism 10.0.0 (San Diego, CA, USA). Normality of distribution was assessed using a D’Agostino–Pearson test with a log-transformation. An unpaired t-test and chi-squared test were used for data comparison between CPs and IPs. p-values < 0.05 were considered statistically significant. Concordance between FA-PNEU and routine results was evaluated through a calculation of positive and negative percentage agreement (PPA/NPA).
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Hospital-Faculty Ethics Committee Saint-Luc—UCL (National number: B403).
Author Contributions
Design, A.V. and P.-F.L.; patient inclusion, X.W. and P.-F.L.; data collection and analysis, A.V., J.F. and A.A.; writing—original draft preparation, A.V.; writing—review and editing, J.F., A.A, H.R.-V., X.W. and P.-F.L.; visualization, A.V.; supervision, X.W. and P.-F.L.; project administration, A.V.; funding acquisition, A.V. and P.-F.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by BioFire Diagnostics (Salt Lake City, UT, USA) as they supplied two FilmArray systems and the tests. Biofire Diagnostics did not have any role in the design of the study nor in the collection, analysis, or interpretation of data.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Hospital-Faculty Ethics Committee Saint-Luc—UCL (national number: B403).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data generated and analyzed during this study are available upon reasonable request from the corresponding author.
Acknowledgments
We thank all interns from the intensive care units for their collaboration in the inclusion of the critically ill patients. We also thank all laboratory technicians and interns from the clinical laboratory who performed the testing.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- Papazian, L.; Klompas, M.; Luyt, C.E. Ventilator-associated pneumonia in adults: A narrative review. Int. Care Med. 2020, 46, 888–906. [Google Scholar] [CrossRef] [PubMed]
- Martin-Loeches, I.; Torres, A.; Nagavci, B.; Aliberti, S.; Antonelli, M.; Bassetti, M.; Bos, L.D.; Chalmers, J.D.; Derde, L.; de Waele, J.; et al. ERS/ESICM/ESCMID/ALAT guidelines for the management of severe community-acquired pneumonia. Intensive Care Med. 2023, 49, 615–632. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Niederman, M.S.; Chastre, J.; Ewig, S.; Fernandez-Vandellos, P.; Hanberger, H.; Kollef, M.; Li Bassi, G.; Luna, C.M.; Martin-Loeches, I.; et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: Guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur. Respir. J. 2017, 50, 1700582. [Google Scholar] [CrossRef] [PubMed]
- Teshome, B.F.; Vouri, S.M.; Hampton, N.; Kollef, M.H.; Micek, S.T. Duration of Exposure to Antipseudomonal β-Lactam Antibiotics in the Critically Ill and Development of New Resistance. Pharmacotherapy 2019, 39, 261–270. [Google Scholar] [CrossRef]
- Crémet, L.; Gaborit, B.; Bouras, M.; Drumel, T.; Guillotin, F.; Poulain, C.; Persyn, E.; Lakhal, K.; Rozec, B.; Vibet, M.A.; et al. Evaluation of the FilmArray® Pneumonia Plus Panel for Rapid Diagnosis of Hospital-Acquired Pneumonia in Intensive Care Unit Patients. Front. Microbiol. 2020, 11, 2080. [Google Scholar] [CrossRef]
- Enne, V.I.; Aydin, A.; Baldan, R.; Owen, D.R.; Richardson, H.; Ricciardi, F.; Russell, C.; Nomamiukor-Ikeji, B.O.; Swart, A.M.; High, J.; et al. Multicentre evaluation of two multiplex PCR platforms for the rapid microbiological investigation of nosocomial pneumonia in UK ICUs: The INHALE WP1 study. Thorax 2022, 77, 1220–1228. [Google Scholar] [CrossRef]
- Buchan, B.W.; Windham, S.; Balada-Llasat, J.M.; Leber, A.; Harrington, A.; Relich, R.; Murphy, C.; Dien Bard, J.; Naccache, S.; Ronen, S.; et al. Practical Comparison of the BioFire FilmArray Pneumonia Panel to Routine Diagnostic Methods and Potential Impact on Antimicrobial Stewardship in Adult Hospitalized Patients with Lower Respiratory Tract Infections. J. Clin. Microbiol. 2020, 58, e00135-20. [Google Scholar] [CrossRef]
- Guillotin, F.; Poulain, C.; Gaborit, B.; Bouras, M.; Cinotti, R.; Lakhal, K.; Vourc’h, M.; Rozec, B.; Asehnoune, K.; Vibet, M.A.; et al. Potential Impact of Rapid Multiplex PCR on Antimicrobial Therapy Guidance for Ventilated Hospital-Acquired Pneumonia in Critically Ill Patients, A Prospective Observational Clinical and Economic Study. Front. Cell Infect. Microbiol. 2022, 12, 804611. [Google Scholar] [CrossRef]
- Monard, C.; Pehlivan, J.; Auger, G.; Alviset, S.; Tran Dinh, A.; Duquaire, P.; Gastli, N.; d’Humières, C.; Maamar, A.; Boibieux, A.; et al. Multicenter evaluation of a syndromic rapid multiplex PCR test for early adaptation of antimicrobial therapy in adult patients with pneumonia. Crit. Care 2020, 24, 434. [Google Scholar] [CrossRef]
- Stafylaki, D.; Maraki, S.; Vaporidi, K.; Georgopoulos, D.; Kontoyiannis, D.P.; Kofteridis, D.P.; Chamilos, G. Impact of Molecular Syndromic Diagnosis of Severe Pneumonia in the Management of Critically Ill Patients. Microbiol. Spectr. 2022, 10, e0161622. [Google Scholar] [CrossRef] [PubMed]
- Rhee, C.; Kadri, S.S.; Dekker, J.P.; Danner, R.L.; Chen, H.C.; Fram, D.; Zhang, F.; Wang, R.; Klompas, M.; CDC Prevention Epicenters Program. Prevalence of Antibiotic-Resistant Pathogens in Culture-Proven Sepsis and Outcomes Associated With Inadequate and Broad-Spectrum Empiric Antibiotic Use. JAMA Netw. Open 2020, 3, e202899. [Google Scholar] [CrossRef] [PubMed]
- Cartuliares, M.B.; Rosenvinge, F.S.; Mogensen, C.B.; Skovsted, T.A.; Andersen, S.L.; Østergaard, C.; Pedersen, A.K.; Skjøt-Arkil, H. Evaluation of point-of-care multiplex polymerase chain reaction in guiding antibiotic treatment of patients acutely admitted with suspected community-acquired pneumonia in Denmark: A multicentre randomised controlled trial. PLoS Med. 2023, 20, e1004314. [Google Scholar] [CrossRef] [PubMed]
- Martinot, M.; Greigert, V.; Gravier, S.; Klein, S.; Eyriey, M.; Pachart, A.; Kaiser, J.D.; Zadeh, M.M.; De Briel, D.; Gottwalles, Y.; et al. Positive Impact of a Point-of-Care Molecular Influenza Test in the Emergency Department During the 2017-2018 Seasonal Influenza Epidemic. Open Forum. Infect. Dis. 2019, 6, ofz312. [Google Scholar] [CrossRef] [PubMed]
- Clark, T.W.; Beard, K.R.; Brendish, N.J.; Malachira, A.K.; Mills, S.; Chan, C.; Poole, S.; Ewings, S.; Cortes, N.; Nyimbili, E.; et al. Clinical impact of a routine, molecular, point-of-care, test-and-treat strategy for influenza in adults admitted to hospital (FluPOC): A multicentre, open-label, randomised controlled trial. Lancet Respir. Med. 2021, 9, 419–429. [Google Scholar] [CrossRef]
- Webber, D.M.; Wallace, M.A.; Burnham, C.A.; Anderson, N.W. Evaluation of the BioFire FilmArray Pneumonia Panel for Detection of Viral and Bacterial Pathogens in Lower Respiratory Tract Specimens in the Setting of a Tertiary Care Academic Medical Center. J. Clin. Microbiol. 2020, 58, e00343-20. [Google Scholar] [CrossRef]
- Gastli, N.; Loubinoux, J.; Daragon, M.; Lavigne, J.P.; Saint-Sardos, P.; Pailhoriès, H.; Lemarié, C.; Benmansour, H.; d’Humières, C.; Broutin, L.; et al. Multicentric evaluation of BioFire FilmArray Pneumonia Panel for rapid bacteriological documentation of pneumonia. Clin. Microbiol. Infect. 2021, 27, 1308–1314. [Google Scholar] [CrossRef]
- Timbrook, T.T.; Morton, J.B.; McConeghy, K.W.; Caffrey, A.R.; Mylonakis, E.; LaPlante, K.L. The Effect of Molecular Rapid Diagnostic Testing on Clinical Outcomes in Bloodstream Infections: A Systematic Review and Meta-analysis. Clin. Infect. Dis. 2017, 64, 15–23. [Google Scholar] [CrossRef]
- Pliakos, E.E.; Andreatos, N.; Shehadeh, F.; Ziakas, P.D.; Mylonakis, E. The Cost-Effectiveness of Rapid Diagnostic Testing for the Diagnosis of Bloodstream Infections with or without Antimicrobial Stewardship. Clin. Microbiol. Rev. 2018, 31, e00095-17. [Google Scholar] [CrossRef]
- Banerjee, R.; Teng, C.B.; Cunningham, S.A.; Ihde, S.M.; Steckelberg, J.M.; Moriarty, J.P.; Shah, N.D.; Mandrekar, J.N.; Patel, R. Randomized Trial of Rapid Multiplex Polymerase Chain Reaction-Based Blood Culture Identification and Susceptibility Testing. Clin. Infect. Dis. 2015, 61, 1071–1080. [Google Scholar] [CrossRef]
- Moy, A.C.; Kimmoun, A.; Merkling, T.; Berçot, B.; Caméléna, F.; Poncin, T.; Deniau, B.; Mebazaa, A.; Dudoignon, E.; Dépret, F.; et al. Performance evaluation of a PCR panel (FilmArray® Pneumonia Plus) for detection of respiratory bacterial pathogens in respiratory specimens: A systematic review and meta-analysis. Anaesth. Crit. Care Pain. Med. 2023, 42, 101300. [Google Scholar] [CrossRef] [PubMed]
- Andrews, D.; Chetty, Y.; Cooper, B.S.; Virk, M.; Glass, S.K.; Letters, A.; Kelly, P.A.; Sudhanva, M.; Jeyaratnam, D. Multiplex PCR point of care testing versus routine, laboratory-based testing in the treatment of adults with respiratory tract infections: A quasi-randomised study assessing impact on length of stay and antimicrobial use. BMC Infect. Dis. 2017, 17, 671. [Google Scholar] [CrossRef] [PubMed]
- Timbrook, T.T.; Wigmosta, T.B.; Hemmert, R.B.; Dimas, J.B.; Krause, A.; Spinali, S.; Thelen, M.; Tongio, I.; Tissier, J.L. Measuring clinical outcomes of highly multiplex molecular diagnostics for respiratory infections: A systematic review and conceptual framework. Antimicrob. Steward. Healthc. Epidemiol. 2023, 3, e9. [Google Scholar] [CrossRef] [PubMed]
- High, J.; Enne, V.I.; Barber, J.A.; Brealey, D.; Turner, D.A.; Horne, R.; Peters, M.; Dhesi, Z.; Wagner, A.P.; Pandolfo, A.M.; et al. INHALE: The impact of using FilmArray Pneumonia Panel molecular diagnostics for hospital-acquired and ventilator-associated pneumonia on antimicrobial stewardship and patient outcomes in UK Critical Care-study protocol for a multicentre randomised controlled trial. Trials 2021, 22, 680. [Google Scholar] [CrossRef]
- Serigstad, S.; Ritz, C.; Faurholt-Jepsen, D.; Markussen, D.; Ebbesen, M.H.; Kommedal, Ø.; Bjørneklett, R.O.; Heggelund, L.; Clark, T.W.; van Werkhoven, C.H.; et al. Impact of rapid molecular testing on diagnosis, treatment and management of community-acquired pneumonia in Norway: A pragmatic randomised controlled trial (CAPNOR). Trials 2022, 23, 622. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).