

Local and Systemic Antibiotics in Peri-Implantitis Management: An Umbrella Review

 ,
,  ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Protocol
- I-Intervention: locally and/or systemically administered antibiotics alone or (all);
- C-Comparison: no intervention, placebo, between different interventions (different type, routes of administration, and regimens of locally- and/or systemically-delivered antibiotics alone or in combination with other surgical or nonsurgical peri-implantitis treatments);
- O-Outcome(s): clinical and radiographic and crevicular peri-implant parameters.
2.2. Search Strategy
2.3. Study Selection and Eligibility Criteria
2.4. Data Extraction and Collection
2.5. Data Synthesis
- to characterize the type and regimen of antibiotics administered locally and/or systemically alone or in combination with other (surgical or nonsurgical) peri-implantitis treatments and comparisons;
- to assess clinical, radiographic, and crevicular peri-implant outcomes according to the type and regimen of locally- and/or systemically-delivered antibiotics administered alone or in combination with other (surgical or nonsurgical) peri-implantitis provided;
- to compare clinical, radiographic, and crevicular peri-implant outcomes after administration of locally- and/or systemically-administered antibiotics alone or in combination with other (surgical or nonsurgical) peri-implantitis vs. placebo and to each other.
2.6. Quality Assessment
3. Results
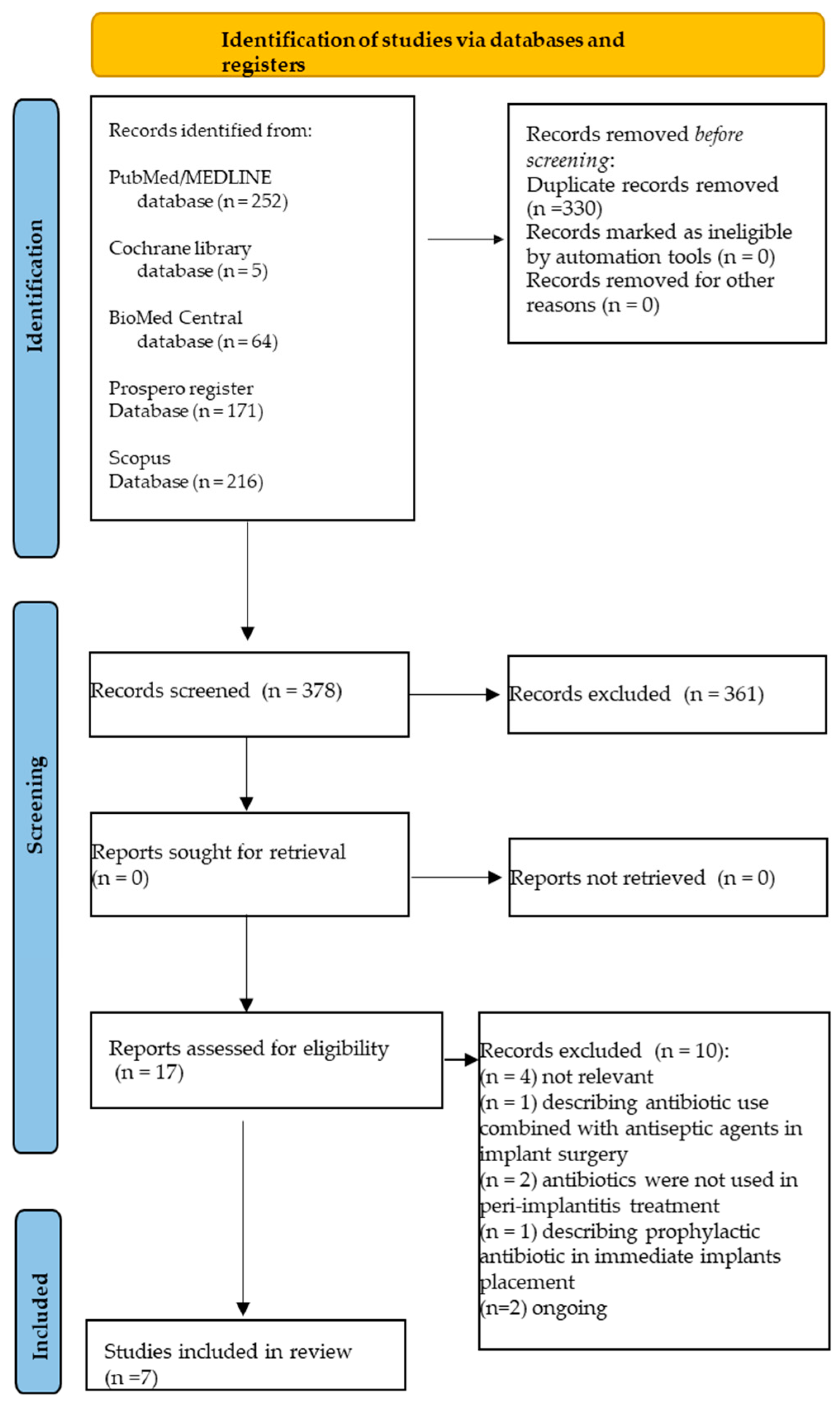
3.1. Study Selection
3.2. Study Characteristics
3.3. Local and Systemic Antibiotics in Peri-Implantitis Management
3.3.1. Locally-Delivered Antibiotics Alone and in Combination with Nonsurgical and Surgical Treatment of Peri-Implantitis
3.3.2. Systemically-Delivered Antibiotics in Combination with Nonsurgical and Surgical Treatment of Peri-Implantitis
3.3.3. Locally- Plus Systemically-Delivered Antibiotics in Combination with Nonsurgical and Surgical Treatment of Peri-Implantitis
3.4. Quality Assessment
4. Discussion
4.1. Locally-Delivered Antibiotics Alone and in Combination with Nonsurgical and Surgical Treatment of Peri-Implantitis
4.2. Systemically-Delivered Antibiotics in Combination with Nonsurgical and Surgical Treatment of Peri-Implantitis
4.3. Efficacy of Locally-Plus Systemically-Delivered Antibiotics in Combination with Nonsurgical and Surgical Treatment of Peri-Implantitis
4.4. Local and Systemic Antibiotics in Peri-Implantitis Management: Clinical Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Derks, J.; Schaller, D.; Håkansson, J.; Wennström, J.L.; Tomasi, C.; Berglundh, T. Effectiveness of implant therapy analyzed in a Swedish population: Prevalence of peri-implantitis. J. Dent. Res. 2016, 95, 43–49. [Google Scholar] [CrossRef]
- Lee, C.T.; Huang, Y.W.; Zhu, L.; Weltman, R. Prevalences of peri-implantitis and peri-implant mucositis: Systematic review and meta-analysis. J. Dent. 2017, 62, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89, 159–172. [Google Scholar] [CrossRef] [PubMed]
- Di Spirito, F.; lo Giudice, R.; Amato, M.; di Palo, M.P.; D’Ambrosio, F.; Amato, A.; Martina, S. Inflammatory, Reactive, and Hypersensitivity Lesions Potentially Due to Metal Nanoparticles from Dental Implants and Supported Restorations: An Umbrella Review. Appl. Sci. 2022, 12, 11208. [Google Scholar] [CrossRef]
- Di Spirito, F.; Schiavo, L.; Pilone, V.; Lanza, A.; Sbordone, L.; D’Ambrosio, F. Periodontal and Periimplant Diseases and Systemically Administered Statins: A Systematic Review. Dent J 2021, 9, 100. [Google Scholar] [CrossRef]
- Schwarz, F.; Giannobile, W.V.; Jung, R.E. Groups of the 2nd Osteology Foundation Consensus Meeting. Evidence-based knowledge on the aesthetics and maintenance of peri-implant soft tissues: Osteology Foundation Consensus Report Part 2-Effects of hard tissue augmentation procedures on the maintenance of peri-implant tissues. Clin. Oral Implant. Res. 2018, 29, 11–13. [Google Scholar]
- Di Spirito, F.; Pelella, S.; Argentino, S.; Sisalli, L.; Sbordone, L. Oral Manifestations and the Role of the Oral Healthcare Workers in COVID-19. Oral Dis. 2022, 28, 1003–1004. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.; Di Spirito, F.; D’Ambrosio, F.; Boccia, G.; Moccia, G.; De Caro, F. Probiotics in Periodontal and Peri-Implant Health Management: Biofilm Control, Dysbiosis Reversal, and Host Modulation. Microorganisms 2022, 10, 2289. [Google Scholar] [CrossRef] [PubMed]
- Faggion, C.M., Jr.; Chambrone, L.; Listl, S.; Tu, Y.K. Network meta-analysis for evaluating interventions in implant dentistry: The case of peri-implantitis treatment. Clin. Implant. Dent. Relat. Res. 2013, 15, 576–588. [Google Scholar] [CrossRef]
- Renvert, S.; Polyzois, I.; Clafey, N. Surgical therapy for the control of peri-implantitis. Clin. Oral. Implant. Res. 2012, 23, 84–94. [Google Scholar] [CrossRef]
- Keeve, P.L.; Koo, K.T.; Ramanauskaite, A.; Romanos, G.; Schwarz, F.; Sculean, A.; Khoury, F. Surgical treatment of peri-implantitis with non-augmentative techniques. Implant. Dent. 2019, 28, 177–186. [Google Scholar] [CrossRef]
- Di Spirito, F. Oral-Systemic Health and Disorders: Latest Prospects on Oral Antisepsis. Appl. Sci. 2022, 12, 8185. [Google Scholar] [CrossRef]
- Eick, S.; Ramseier, C.A.; Rothenberger, K.; Brägger, U.; Buser, D.; Salvi, G.E. Microbiota at teeth and implants in partially edentulous patients. A 10-year retrospective study. Clin. Oral Implant. Res. 2016, 27, 218–225. [Google Scholar] [CrossRef]
- Di Spirito, F.; Toti, P.; Brevi, B.; Martuscelli, R.; Sbordone, L.; Sbordone, C. Computed Tomography Evaluation of Jaw Atrophies Before and After Surgical Bone Augmentation. Int. J. Clin. Dent. 2019, 12, 259–270. [Google Scholar]
- Valderrama, P.; Blansett, J.A.; Gonzalez, M.G.; Cantu, M.G.; Wilson, T.G. Detoxification of Implant Surfaces Affected by PeriImplant Disease: An Overview of Nonsurgical Methods. Open Dent. J. 2014, 8, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Romanos, G.; Ko, H.H.; Froum, S.; Tarnow, D. The use of CO(2) laser in the treatment of peri-implantitis. Photomed. Laser Surg. 2009, 27, 381–386. [Google Scholar] [CrossRef]
- Natto, Z.S.; Aladmawy, M.; Levi, P.A., Jr.; Wang, H.L. Comparison of the efficacy of different types of lasers for the treatment of peri-implantitis: A systematic review. Int. J. Oral Maxillofac. Implant. 2015, 30, 338–345. [Google Scholar] [CrossRef]
- Mombelli, A.; Lang, N.P. Antimicrobial treatment of peri-implant infections. Clin. Oral Implant. Res. 1992, 3, 116–162. [Google Scholar] [CrossRef]
- Van Winkelhoff, A.J. Antibiotics in the treatment of peri-implantitis. Eur. J. Oral Implant. 2012, 5, 43–50. [Google Scholar]
- D’Ambrosio, F.; Di Spirito, F.; Amato, A.; Caggiano, M.; Lo Giudice, R.; Martina, S. Attitudes towards Antibiotic Prescription and Antimicrobial Resistance Awareness among Italian Dentists: What Are the Milestones? Healthcare 2022, 10, 1585. [Google Scholar] [CrossRef]
- Sukumar, S.; Martin, F.E.; Hughes, T.E.; Adler, C.J. Think before you prescribe: How dentistry contributes to antibiotic resistance. Aust. Dent. J. 2019, 65, 21–29. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; Di Spirito, F.; De Caro, F.; Lanza, A.; Passarella, D.; Sbordone, L. Adherence to Antibiotic Prescription of Dental Patients: The Other Side of the Antimicrobial Resistance. Healthcare 2022, 10, 1636. [Google Scholar] [CrossRef] [PubMed]
- Busa, A.; Parrini, S.; Chisci, G.; Pozzi, T.; Burgassi, S.; Capuano, A. Local versus systemic antibiotics effectiveness: A comparative study of postoperative oral disability in lower third molar surgery. J. Craniofacial Surg. 2014, 25, 708–709. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Booth, A.; Clarke, M.; Dooley, G.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. The nuts and bolts of PROSPERO: An international prospective register of systematic reviews. Syst. Rev. 2012, 1, 2. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocolss (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, 1000100. [Google Scholar] [CrossRef] [PubMed]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The well-built clinical question: A key to evidence-based decisions. ACPJ Club 1995, 123, 12–13. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Ltd.: Chichester, UK, 2008. [Google Scholar]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, 4008. [Google Scholar] [CrossRef]
- Alenezi, A.; Chrcanovic, B. Effects of the local administration of antibiotics on bone formation on implant surface in animal models: A systematic review and meta-analysis. Jpn. Dent. Sci. Rev. 2020, 56, 177–183. [Google Scholar] [CrossRef]
- Rodríguez Sánchez, F.; Rodríguez Andrés, C.; Arteagoitia, I. Which antibiotic regimen prevents implant failure or infection after dental implant surgery? A systematic review and meta-analysis. J. Cranio-Maxillo-Facial Surg. Off. Publ. Eur. Assoc. Cranio-Maxillo-Facial Surg. 2018, 46, 722–736. [Google Scholar] [CrossRef]
- Grusovin, M.G.; Coulthard, P.; Worthington, H.V.; Esposito, M. Maintaining and recovering soft tissue health around dental implants: A Cochrane systematic review of randomised controlled clinical trials. Eur. J. Oral Implantol. 2008, 1, 11–22. [Google Scholar]
- Caiazzo, A.; Canullo, L.; Consensus Meeting Group; Pesce, P. Consensus Report by the Italian Academy of Osseointegration on the Use of Antibiotics and Antiseptic Agents in Implant Surgery. Int. J. Oral Maxillofac. Implant. 2021, 36, 103–105. [Google Scholar] [CrossRef]
- Khan, A.; Goyal, A.; Currell, S.D.; Sharma, D. Management of Peri-Implantitis Lesions without the Use of Systemic Antibiotics: A Systematic Review. Dent. J. 2020, 8, 106. [Google Scholar] [CrossRef] [PubMed]
- Salgado-Peralvo, A.O.; Peña-Cardelles, J.F.; Kewalramani, N.; Mateos-Moreno, M.V.; Jiménez-Guerra, Á.; Velasco-Ortega, E.; Uribarri, A.; Moreno-Muñoz, J.; Ortiz-García, I.; Núñez-Márquez, E.; et al. Preventive Antibiotic Therapy in the Placement of Immediate Implants: A Systematic Review. Antibiotics 2021, 11, 5. [Google Scholar] [CrossRef] [PubMed]
- Bizelli, V.; Bassi, A.P.; Souza, E. Analysis of the Local and Systemic Adjuvant Effect of Antibiotics in the Treatment Of Peri-Implantitis Compared to Mechanical Treatment such as Monotherapy or Associated with the Adjunctive Use of Chlorhexidine: Systematic Review and Meta-Analysis. PROSPERO 2020 CRD42020209344. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020209344 (accessed on 15 November 2022).
- Jin Lim, S.; McGowen, K.; McGowen, T.; Vithanage, A.; Ivanovski, S. Is There a Benefit to Adjunctive Antibiotics in Nonsurgical Therapy for Peri-Implantitis? A Systematic Review and Meta-Analysis of Randomised-Controlled Trials. PROSPERO 2018 CRD42018102067. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42018102067 (accessed on 15 November 2022).
- Esposito, M.; Coulthard, P.; Oliver, R.; Thomsen, P.; Worthington, H.V. Antibiotics to prevent complications following dental implant treatment. Cochrane Database Syst. Rev. 2003, CD004152. [Google Scholar] [CrossRef]
- Ata-Ali, J.; Ata-Ali, F.; Ata-Ali, F. Do antibiotics decrease implant failure and postoperative infections? A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2014, 43, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Toledano, M.; Osorio, M.T.; Vallecillo-Rivas, M.; Toledano-Osorio, M.; Rodríguez-Archilla, A.; Toledano, R.; Osorio, R. Efficacy of local antibiotic therapy in the treatment of peri-implantitis: A systematic review and meta-analysis. J. Dent. 2021, 113, 103790. [Google Scholar] [CrossRef] [PubMed]
- Passarelli, P.C.; Netti, A.; Lopez, M.A.; Giaquinto, E.F.; De Rosa, G.; Aureli, G.; Bodnarenko, A.; Papi, P.; Starzy ’nska, A.; Pompa, G.; et al. Local/Topical Antibiotics for Peri-Implantitis Treatment: A Systematic Review. Antibiotics 2021, 10, 1298. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, C.Y.; Stathopoulou, P.G.; Graham, L.K.; Korostoff, J.; Chen, Y.W. Efficacy of Antibiotics Used as an Adjunct in the Treatment of Peri-implant Mucositis and Peri-implantitis: A Systematic Review and Meta-analysis. Int. J. Oral Maxillofac. Implant. 2022, 37, 235–249. [Google Scholar] [CrossRef]
- Øen, M.; Leknes, K.N.; Lund, B.; Bunæs, D.F. The efficacy of systemic antibiotics as an adjunct to surgical treatment of peri-implantitis: A systematic review. BMC Oral Health 2021, 21, 666. [Google Scholar] [CrossRef] [PubMed]
- Toledano-Osorio, M.; Vallecillo, C.; Toledano, R.; Aguilera, F.S.; Osorio, M.T.; Muñoz-Soto, E.; García-Godoy, F.; Vallecillo-Rivas, M. A Systematic Review and Meta-Analysis of Systemic Antibiotic Therapy in the Treatment of Peri-Implantitis. Int. J. Environ. Res. Public Health 2022, 19, 6502. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Grusovin, M.G.; Tzanetea, E.; Piattelli, A.; Worthington, H.V. Interventions for replacing missing teeth: Treatment of perimplantitis. Cochrane Database Syst. Rev. 2010, CD004970. [Google Scholar] [CrossRef]
- Zhao, Y.; Pu, R.; Qian, Y.; Shi, J.; Si, M. Antimicrobial photodynamic therapy versus antibiotics as an adjunct in the treatment of periodontitis and peri-implantitis: A systematic review and meta-analysis. Photodiagnosis Photodyn. Ther. 2021, 34, 102231. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, J.; Oh, J.; Inglehart, M.; Aronovich, S. Etiology, Diagnosis and Treatment of Peri-Implantitis—A National Survey of AAOMS Members. J. Oral Maxillofac. Surg. 2017, 75, 355–356. [Google Scholar] [CrossRef]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-Implant Diseases and Conditions: Consensus Report of Workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, 286–291. [Google Scholar] [CrossRef]
- Mishler, O.P.; Shiau, H.J. Management of peri-implant disease: A current appraisal. J. Evid. Based Dent. Pract. 2014, 14, 53–59. [Google Scholar] [CrossRef]
- Mombelli, A.; Müller, N.; Cionca, N. The epidemiology of peri-implantitis. Clin. Oral Implants Res. 2012, 23 (Suppl. 6), 67–76. [Google Scholar] [CrossRef]
- Rokaya, D.; Srimaneepong, V.; Wisitrasameewon, W.; Humagain, M.; Thunyakitpisal, P. Peri-implantitis Update: Risk Indicators, Diagnosis, and Treatment. Eur. J. Dent. 2020, 14, 672–682. [Google Scholar] [CrossRef]
- Chala, M.; Anagnostaki, E.; Mylona, V.; Chalas, A.; Parker, S.; Lynch, E. Adjunctive Use of Lasers in Peri-Implant Mucositis and Peri-Implantitis Treatment: A Systematic Review. Dent. J. 2020, 8, 68. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; Caggiano, M.; Schiavo, L.; Savarese, G.; Carpinelli, L.; Amato, A.; Iandolo, A. Chronic Stress and Depression in Periodontitis and Peri-Implantitis: A Narrative Review on Neurobiological, Neurobehavioral and Immune–Microbiome Interplays and Clinical Management Implications. Dent. J. 2022, 10, 49. [Google Scholar] [CrossRef]
- Figuero, E.; Graziani, F.; Sanz, I.; Herrera, D.; Sanz, M. Management of peri-implant mucositis and peri-implantitis. Periodontol. 2000 2014, 66, 255–273. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.; Mombelli, A. The therapy of peri-implantitis: A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 325–345. [Google Scholar] [CrossRef]
- Rodrigues, R.M.; Gonçalves, C.; Souto, R.; Feres-Filho, E.J.; Uzeda, M.; Colombo, A.P. Antibiotic resistance profile of the subgingival microbiota following systemic or local tetracycline therapy. J. Clin. Periodontol. 2004, 31, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Thompson, W.; Williams, D.; Pulcini, C.; Sanderson, S.; Calfon, P.; Verma, M. Tackling Antibiotic Resistance: Why Dentistry Matters. Int. Dent. J. 2021, 71, 450–453. [Google Scholar] [CrossRef]
- Landecker, H. Antibiotic resistance and the biology of history. Body Soc. 2016, 22, 19–52. [Google Scholar] [CrossRef]
- World Health Organization. Antimicrobial Resistance (who.int). Available online: https://www.who.int/health-topics/antimicrobial-resistance (accessed on 31 July 2022).
- Di Spirito, F.; Argentino, S.; Martuscelli, R.; Sbordone, L. Mronj Incidence After Multiple Teeth Extractions in Patients Taking Oral Bis-Phosphonates Without “Drug Holiday”: A Retrospective Chart Review. Oral Implantol. 2019, 12, 105–110. [Google Scholar]
- Di Spirito, F.; Scelza, G.; Fornara, R.; Giordano, F.; Rosa, D.; Amato, A. Post-operative endodontic pain management: An overview of systematic reviews on post-operatively administered oral medications and integrated evidence-based clinical recommendations. Healthcare 2022, 10, 760. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Polyzois, I. Treatment of pathologic peri-implant pockets. Periodontol. 2000 2018, 76, 18. [Google Scholar] [CrossRef]
- Cha, J.K.; Lee, J.S.; Kim, C.S. Surgical therapy of peri-implantitis with local minocycline: A 6-month randomized controlled clinical trial. J. Dent. Res. 2019, 98, 288–295. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Data Extracted and Collected from the Systematic Reviews Included in the Present Umbrella Review | |
|---|---|
| Systematic reviews | Authors, Year |
| Journal | |
| Meta-analysis | |
| Funding | |
| Quality | |
| Conclusions | |
| Studies included in the systematic reviews | Characteristics |
| (number and design) | |
| Population | |
| (sample size, mean age, gender ratio) | |
| Peri-implantitis sites | |
| (dental implants’ number, position, and survival) | |
| Administered antibiotics | Local or systemic antibiotics |
| (type, delivery vehicle, regimen, duration) | |
| Combined peri-implant treatment (if any) | |
| (type, sessions, follow-up) | |
| Peri-implant outcomes (statistically significant) | Clinical parameters |
| Radiographic parameters | |
| Crevicular parameters | |
| Authors, Year | Reason for Exclusion |
|---|---|
| Alenzi, A., 2020 [31] | Not pertinent |
| Rodríguez Sánchez, 2018 [32] | Not pertinent |
| Grusovin, M. G., 2010 [33] | Not pertinent |
| Caiazzo, 2021 [34] | Antibiotics used in combination with antiseptics in implant surgery |
| Khan, 2020 [35] | Antibiotics were not used in peri-implantitis treatment |
| Salgado-Peralvo, 2021 [36] | Antibiotics used as prophylaxis in immediate implants placement |
| Bizelli, 2020 [37] | Review ongoing |
| Soo Jim Lin, 2018 [38] | Review ongoing |
| Esposito, M., 2003 [39] | Not pertinent |
| Ata-Ali, 2013 [40] | Antibiotics were used in postoperative infections and implant failure |
| Authors, Year Reference Journal Meta-Analysis Funding Quality | Studies (Number and Design) Population Sample Size Mean Age Gender Ratio Peri-Implantitis Sites (Dental Implants’ Number, Position, and Survival) | Administered Antibiotics Local or Systemic (Type, Delivery Vehicle, Regimen, Duration) Combined Peri-Implant Treatment (Type, Sessions, Follow-Up) | Peri-Implant Outcomes (Statistically Significant) Clinical Parameters Radiographic Parameters Crevicular Parameters | Conclusions |
|---|---|---|---|---|
| Toledano, 2021 [41] Journal of Dent Systematic review and Meta-analysis Low quality | Studies: n.12 RCT (n.7) CS (n.1) CCS (n.3) PS (n.1) Population sample size n.365 Implants n.463 Mean age: MD Gender ratio: MD Dental implants affected Number: MD Position: MD Characteristics: MD Survival: MD | Local antibiotics: yes Type: minocycline, doxycycline, lincomycin, erythromycin, tetracycline Delivery vehicle: gel, microspheres, fibers, powdered, bone graft, ointment Duration: 4, 6, and 12 months Systemic antibiotics: no Combined peri-implant treatment: no | PPD BoP | The local antibiotic administration reduces peri-implant probing depths and bleeding on probing in patients affected by peri-implantitis, compared to control groups without local antibiotic application |
| Passarelli, 2021 [42] Antibiotics Systematic review Critically low quality | Studies: n.5 RCT (n.5) Population sample size n.250 Implants n.333 Mean age: MD Gender ratio: MD Dental implants affected Number: MD Position: MD Characteristics: MD Survival: MD | Local antibiotics: yes Type: minocycline, doxycycline Delivery vehicle: microspheres, ointment Systemic antibiotics: yes Type: MTZ Combined peri-implant treatment: no Type: nonsurgical (SRP) and surgical treatment | PPD BoP GI | After 6 months, GI showed a statistically significant improvement in a group treated with local minocycline, compared with the placebo control. After 4 months, PPD and BoP were improved in SRP +minocycline-MTZ group than in SRP alone group. Local antibiotic use can be considered a valid approach to treating peri-implantitis |
| Wang, 2022 [43] Int J Oral Maxillofac Implants Systematic review and Meta-analysis Low quality | Studies: n.10 RCT (n.7) CS (n.3) Population sample size n.355 Implants n.596 Mean age: 51.5–69.9 y.o. Gender ratio: MD Dental implants affected: MD Position: MD Characteristics: MD Survival: MD | Local antibiotics: yes (3 studies) Type: tetracycline, doxycycline, doxycycline hyclate, minocycline, periocline Regimen: application of local antibiotics subgingivally Systemic antibiotics: yes (7 studies) Type: AZM, AMX, MTZ Regimens: AZM (500 mg/24 h on 1st d and 250 mg/24 h on d 2 to 4) Duration: 4 d; AZM (500 mg/24 h for 3 d before scaling and root planing) Duration: 3 d; AMX (1.5 mg/24 h 3 d preoperatively and 7 d postoperatively) Duration: 10 d; AZM (500 mg/24 h on the d of surgery, and 250 mg/24 h postoperatively for 4 d) Duration: 5 d; MTZ (400 mg/24 h) + AMX (500 mg/8 h) Duration: 14 d Combined peri-implant treatment: yes Type: nonsurgical (SRP) +/− surgical treatment (OFD) Follow-up: 36 months | BoP PPD RBL | The use of adjunctive antibiotics to treat peri-implantitis provided potential benefits in BoP for up to 12 months post-therapy |
| Oen, M., 2021 [44] BMC Oral Health Systematic review Low quality | Studies: n.9 RCT (n = 2) SR (n = 7) Population sample size MD Implants MD Mean age: MD Gender ratio: MD Dental implants affected Number: MD Position: MD Characteristics: MD Survival: MD | Local antibiotics: no Systemic antibiotics: yes Type: AMX, AZM Combined peri-implant treatment: yes Type: nonsurgical and surgical treatment | BoP PPD PIBL RBL | No strong evidence exists for the use of systemic antibiotics to improve the clinical outcomes in the surgical treatment of peri-implantitis |
| Toledano-Osorio, 2022 [45] Int. J. Environ. Res. Public Health Systematic review and Meta-analysis Low quality | Studies: n.18 RCT (n.9) PS (n.9) Population sample size n.605 Implants n.870 Mean age: MD Gender ratio: MD Dental implants affected Number: MD Position: MD Characteristics: MD Survival: MD | Local antibiotics: no Systemic antibiotics: yes Type: AZM, AMX, AMX plus MTZ Duration: variable Combined peri-implant treatment: yes Type: nonsurgical (SRP) and surgical treatment Follow-up: 10 d, 1, 6 weeks, 1–3–6–12–36–54 months | PPD BoP PI RBL CAL GI | In the treatment of peri-implantitis, systemic antibiotic somministration did not reduce either PPD nor BoP. A reduction of the clinical attachment level, a lower suppuration and recession, less bone loss, and a reduction in total bacterial counts |
| Esposito, M., 2004 [46] The Cochrane Database of Systematic Reviews Review Critically low quality | Studies: n.1 RCTs (n.1) Population sample size MD Implants MD Mean age: MD Gender ratio: MD Dental implants affected Number: MD Position: MD Characteristics: MD Survival: MD | Local antibiotics: yes Type: MTZ gel 25% Duration: 12 weeks Systemic antibiotics: yes/no Combined peri-implant treatment: no MTZ vs. nonsurgical (SRP) treatment | PI BoP PPD | No differences were found between the case and the control |
| Zhao, 2021 [47] Photodiagnosis and Photodynamic therapy Systematic review and Meta-analysis Critically low quality | Studies: n.13 RCT (n.11) N/D (n = 2) Population sample size MD Implants MD Mean age: MD Gender ratio: MD Dental implants affected Number: MD Position: MD Characteristics: MD Survival: MD | Local antibiotics: yes (1/2 local applications) Systemic antibiotics: yes Combined peri-implant treatment: yes Type: nonsurgical (SRP) and surgical treatment | PPD BoP CAL | Meta-analysis outcomes revealed equal clinical evidence for aPDT and antibiotics in periodontitis and peri-implantitis. In addition, aPDT significantly reduced the red complex in both diseases. |
| Authors, Year | Local Antibiotics Regimen | Controls | Outcomes | Conclusion |
|---|---|---|---|---|
| Toledano, 2021 [41] | Minocycline (“Arestin” in microspheres, “Periocycline” in ointment) | aPDT or Placebo | PPD BoP RBL | PPD and BoP have become reduced after local administration of antibiotics in many cases |
| Doxycycline gel (“Atridox”, “Ligosan”) and bone graft “D-Plex 500“ | SRP alone (two studies) or No treatment (one study) | |||
| Lincomycin gel | No treatment | |||
| Erythromycin gel | No treatment | |||
| Tetracycline fibers “Actisite” | No treatment | |||
| MTZ gel “Elyzol” | PCT | |||
| Passarelli, 2021 [42] | Minocycline microspheres | Chlorhexidine 0.1 mL gel 1% | BoP PPD PI | No differences between the groups |
| Esposito, 2019 [46] | MTZ gel 25% (3 mm subgingivally) | UPD with carbon fiber tip inserted 1–2 mm subgingivally at the lowest power for 15 s | Implant failure | No differences between the two groups |
| Author(s), Year | Local Antibiotics (Regimen) + Combined Intervention | Controls | Outcomes | Conclusion |
|---|---|---|---|---|
| Passarelli, 2021 [42] | Doxycycline hyclate 8.5% + SRP | SRP | BoP PPD PI CAL GI | After 4 months, statistically significant differences between groups emerged for the CAL, BoP, and PPD |
| Minocycline 10 mg in 0.5 g of ointment + surgical treatment | Placebo + SRP | After 6 months, a statistically significant improvement emerged for GI and PPD | ||
| Minocycline ointment ( +/−metronidazole) + nonsurgical treatment | SRP | After 4 months, a statistically significant improvement emerged for BoP and PPD | ||
| Wang, 2021 [43] | Tetracycline hydrochloride delivery by monolithic ethylene vinyl acetate fiber (for one time of antibiotic with a duration of 10 days) + rubber cup polishing + SRP | PPD BoP | Local antibiotics in peri-implantitis should provide potential benefits in clinical outcomes for up to 12 months after therapy | |
| Doxycycline “Atridox” subgingivally for one time + SRP and irrigation with 0.2% CHX | ||||
| Minocycline “Periocline” applied subgingivally + OFD at 1, 3, and 6 months | ||||
| Esposito, 2019 [46] | Doxycycline hyclate 8.5% “Atridox” applied through a syringe with a blunt cannula in the peri-implant sulcus + SRP | SRP + subgingival irrigation with 0.2% CHX | Implant failure | After 4 months, doxycycline improved CAL and PPD of about 0.6 mm compared to mechanical debridement |
| Zhao, 2021 [47] | Minocycline gel + UPD | SRP/UDP + aPDT | BoP CAL PPD | PPD, BoP, and CAL significantly decreased in the two groups as compared to the baseline but not between the groups |
| Minocycline hydrochloride microspheres + SRP | SRP + aPDT | |||
| MTZ 400 mg + AMX 500 mg + SRP | SRP + aPDT |
| Author(s), Year | Systemically-delivered Antibiotics (Regimen) + Combined Intervention | Controls | Outcomes | Conclusion |
|---|---|---|---|---|
| Toledano-Osorio, 2022 [45] | AZM (500 mg/24 h at 1st d and 250 mg/24 h for 2–4 d) + MISD | MISD + aPDT | BoP PPD | Systemically-delivered antibiotics should be carefully evaluated in peri-implantitis management considering the risk of antibiotic resistance |
| AMX (500 mg/8 h) + MTZ (400 mg/24 h for 14 d) + NSD | NSD + Placebo | |||
| AMX (500 mg/8 h for 8 d) + MTZ (400 mg/12 h for 8 d) + porous titanium granule + OFD | OFD + antibiotics | |||
| AMX (500 mg/24 h for 7 d) + MTZ (400 mg/8 h for 7 d) + OFD | N/D | |||
| MTZ (250 mg/8 h for 7 d) + NSD | N/D | |||
| MTZ (500 mg/8 h for 7 d) + MISD | N/D | |||
| AMX (750 mg/12 h) + MISD | MISD | |||
| AZM (250 mg/12 h on the d of surgery + 250 mg/24 h for 4 d) + OFD | OFD | |||
| AMX (500 mg/8 h for 7 d) + MTZ (500 mg/24 h for 7 d) + MISD | MISD | |||
| Clindamycin + MTZ + AZM + tetracicline (for 4 w) + MTZ + AMX + ciprofloxacin + sulfonamide + trimethroprim + MTZ (for 2 w) | N/D | |||
| AMX 750 mg/12 h for 10 d (3 d prior to surgery) + OFD + resective techniques | Resective techniques + antiseptic + OFD | |||
| AMX (500 mg/8 h for 7 d) + MISD | MISD + probiotic | |||
| AZM (500 mg/24 h for 3 d) + full mouth SRP | Full mouth SRP | |||
| Ornidazole (1.000 mg for 10 d) + MISD | N/D | |||
| AMX (500 mg/8 h for 7 d) + MTZ (400 mg/8 h for 7 d) + +NSD | MISD + aPDT | |||
| Antibiotics N/D (prior to surgery for 1 w, the d of surgery, and 7 d after) + OFD + bone graft + resorbable membrane | OFD + bone graft + antibiotic | |||
| AMX (500 mg/8 h for 7 d) + MTZ (400 mg/8 h for 7 d) + OFD | N/D | |||
| AMX (500 mg/8 h for 5 d) + MTZ (400 mg/8 h for 5 d) + MISD | MISD alone | |||
| Wang, 2021 [43] | AZM (500 mg on 1 d and 250 mg on 2 and 4 d) + SRP + rubber cup polishing | BoP PPD | Systemic antibiotics, in peri-implantitis, should provide potential benefits in clinical outcomes for up 12 mo. post-therapy | |
| AZM (500 mg/d for 3 d preoperatively) + SRP | ||||
| AMX (1.5 g for 3 d preoperatively and 7 d postoperatively) + OFD + bone recontouring + rubber cup polishing + CHX 0.2% | ||||
| MTZ (400 mg/24 h for 14 d) + AMX (500 mg/8 h for 14 d) + SRP | ||||
| AZM (500 mg/24 h on the d of surgery + 250 mg/24 h postoperatively for 4 d + OFD | ||||
| Oen, 2021 [44] | AMX 750 mg/12 h + CHX 0.2%+ MISD | No treatment | PPD PIBL | The use of systemic antibiotics as an adjunct to surgical treatment of peri-implantitis did not show beneficial effects |
| AZM (250 mg/12 h for 2 d and 250/24 h for 4 d) | ||||
| Zhao, 2021 [47] | MTZ (500 mg/24 h) + AMX (500 mg/8 h for 7 d) + UDP | UPD + aPDT | BoP CAL PPD | The two groups had a significant decrease in PPD, BoP, and CAL compared to the baseline. Antibiotics reduced PPD, CAL, and BoP after 3 mo. for intergroup comparison |
| AMX (375 mg/8 h for 7 d) + MTZ (250 mg/8 h for 7 d) + SRP | SRP + aPDT | Antibiotics significantly reduced PPD and CAL for intergroup comparison | ||
| Clarithromycin (500 mg/24 h for 3 d) + aPDT | aPDT or aPDT + SRP | Antibiotics significantly reduced PPD for intergroup comparison | ||
| MTZ (400 mg/24 h) + AMX (500 mg/8 h for 7 d) + SRP | N/D | A significant decrease in PPD, BoP, and CAL in the two groups was recorded compared to the baseline. aPDT significantly reduced CAL in moderate peri-implant defects in intergroup comparison |
| Author(s), Year | Local Antibiotics +/− Combined Intervention | Systemic Antibiotics +/− Combined Intervention | Outcomes | Conclusion |
|---|---|---|---|---|
| Wang, 2021 [43] | Minocycline “Periocline” + OFD + SRP at 1, 3, 6 months | AMX (500 mg/8 h for 3 d) | BoP PPD | Systemic antibiotics in peri-implantitis management should provide benefits in clinical outcomes for up 12 mo. post-therapy |
| Esposito, 2019 [39] | MTZ 25% gel “Elyzol” + tetracycline hydrochloride “Ambramicine” + apically repositioned flap | AMX (50 mg/kg/d for 8 d) + SRP before surgery | PPD CAL REC | There were no baseline imbalances for plaque, marginal bleeding, PPD, CAL, and REC, and no differences after 2 years |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boccia, G.; Di Spirito, F.; D’Ambrosio, F.; Di Palo, M.P.; Giordano, F.; Amato, M. Local and Systemic Antibiotics in Peri-Implantitis Management: An Umbrella Review. Antibiotics 2023, 12, 114. https://doi.org/10.3390/antibiotics12010114
Boccia G, Di Spirito F, D’Ambrosio F, Di Palo MP, Giordano F, Amato M. Local and Systemic Antibiotics in Peri-Implantitis Management: An Umbrella Review. Antibiotics. 2023; 12(1):114. https://doi.org/10.3390/antibiotics12010114
Chicago/Turabian StyleBoccia, Giovanni, Federica Di Spirito, Francesco D’Ambrosio, Maria Pia Di Palo, Francesco Giordano, and Massimo Amato. 2023. "Local and Systemic Antibiotics in Peri-Implantitis Management: An Umbrella Review" Antibiotics 12, no. 1: 114. https://doi.org/10.3390/antibiotics12010114
APA StyleBoccia, G., Di Spirito, F., D’Ambrosio, F., Di Palo, M. P., Giordano, F., & Amato, M. (2023). Local and Systemic Antibiotics in Peri-Implantitis Management: An Umbrella Review. Antibiotics, 12(1), 114. https://doi.org/10.3390/antibiotics12010114