
Disinfection Strategies for Carbapenem-Resistant Klebsiella pneumoniae in a Healthcare Facility


Abstract
1. Introduction
2. Methods
2.1. Isolation and Identification of Bacterial Strains
2.2. Disinfectants and Neutralizers
2.3. Testing the MICs and MBCs of Each Disinfectant
2.3.1. The Minimum Inhibitory Concentration Test
2.3.2. The Minimum Bactericidal Concentration Test
2.4. PCR Detection of Efflux Pump Genes
3. Results
3.1. Clinical Information of CRKP Strains
3.1.1. The Annual Detection Amount of CRKP Strains
3.1.2. Distribution of CRKP Strains in Different Specimen Types
3.1.3. Distribution of CRKP Strains in Different Departments
3.1.4. Composition of Departments That Detected CRKP Annually
3.1.5. Distribution of Specimen Types in the Top Six Departments That Detected CRKP
3.2. Antimicrobial Sensitivity Profile
3.3. MIC and MBC Results of CRKP Strains
3.3.1. Analysis of Resistance of CRKP Strains to Seven Chemical Disinfectants Commonly Used in Clinics
3.3.2. Recommended Concentration for CRKP Disinfection
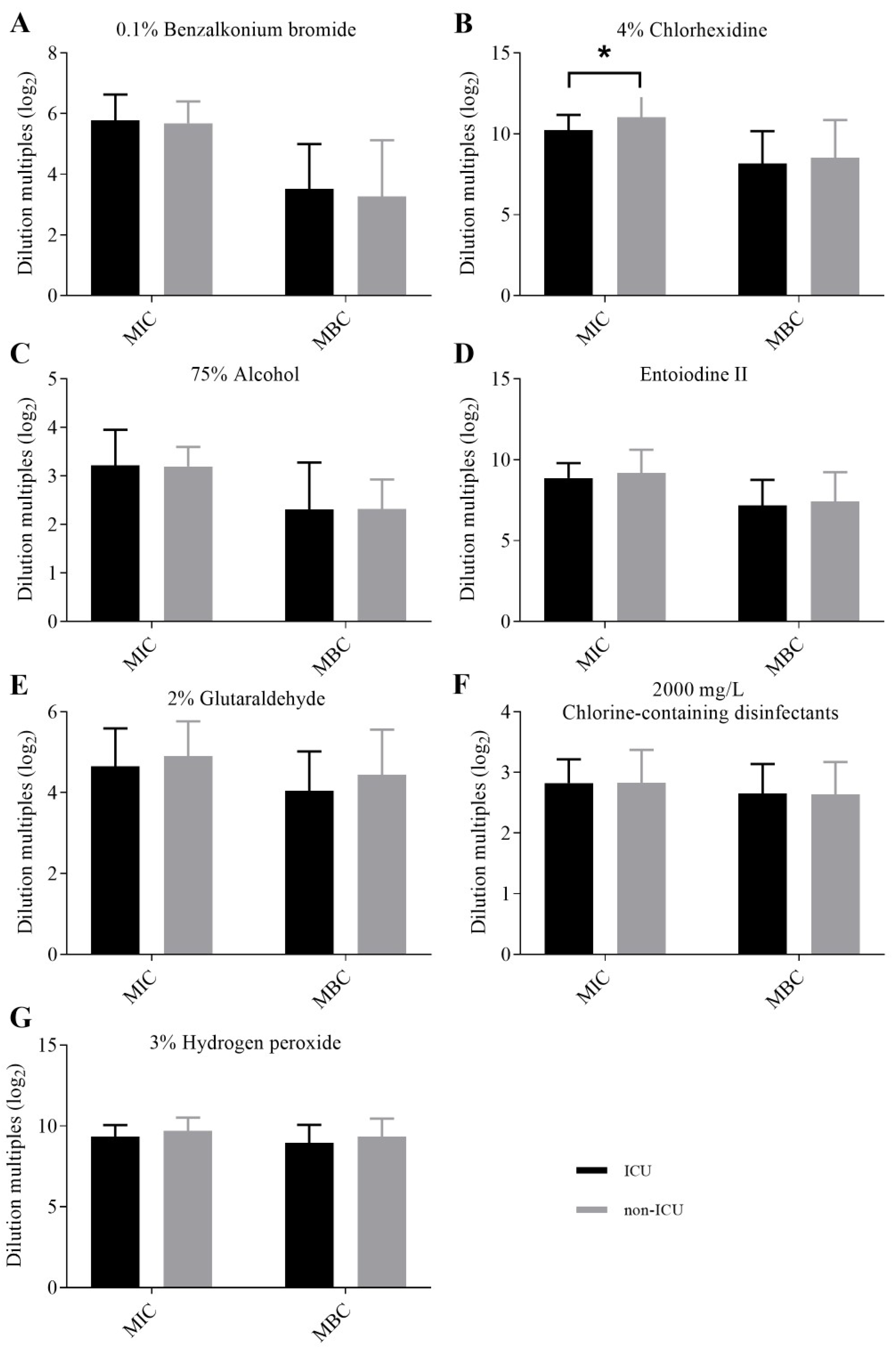
3.3.3. Comparisons of the MICs and MBCs of CRKP Strains Isolated from Different Wards and Different Specimens for Each Disinfectant
3.4. Analysis of Efflux Pump Genes
3.4.1. Detection of Efflux Pump Genes
3.4.2. Correlation between Efflux Pump Genes and Disinfectant Resistance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CRKP | carbapenem-resistant Klebsiella pneumoniae |
| MIC | minimal inhibitory concentration |
| MBC | minimum bactericidal concentration |
| ICU | intensive care unit |
| CRE | carbapenem-resistant Enterobacteriaceae |
| CDC | Centers for Disease Control and Prevention |
| RND | resistance-nodulation cell division |
| QAC | quaternary ammonium compound |
| SMR | small multidrug resistance family |
| SYS Memorial Hospital | Sun Yat-sen Memorial Hospital |
| CLSI | Clinical and Laboratory Standards Institute |
| Kpn | Klebsiella pneumoniae |
| mCIM | modified carbapenem inactivation method |
| eCIM | EDTA-modified carbapenem inactivation method |
| QC | quality control |
| ATCC | American type culture collection |
| PVP-I | povidone-iodine |
| VAP | ventilator-associated pneumonia |
References
- Lutgring, J.D. Carbapenem-resistant Enterobacteriaceae: An emerging bacterial threat. Semin. Diagn. Pathol. 2019, 36, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Nordmann, P.; Dortet, L.; Poirel, L. Carbapenem resistance in Enterobacteriaceae: Here is the storm! Trends Mol. Med. 2012, 18, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Zowawi, H.M.; Forde, B.M.; Alfaresi, M.; Alzarouni, A.; Farahat, Y.; Chong, T.M.; Yin, W.F.; Chan, K.G.; Li, J.; Schembri, M.A.; et al. Stepwise evolution of pandrug-resistance in Klebsiella pneumoniae. Sci. Rep. 2015, 5, 15082. [Google Scholar] [CrossRef] [PubMed]
- Nordmann, P.; Naas, T.; Poirel, L. Global spread of Carbapenemase-producing Enterobacteriaceae. Emerg. Infect. Dis. 2011, 17, 1791–1798. [Google Scholar] [CrossRef]
- Potter, R.F.; D’Souza, A.W.; Dantas, G. The rapid spread of carbapenem-resistant Enterobacteriaceae. Drug Resist. Updates Rev. Comment. Antimicrob. Anticancer. Chemother. 2016, 29, 30–46. [Google Scholar] [CrossRef]
- Zhu, W.M.; Yuan, Z.; Zhou, H.Y. Risk factors for carbapenem-resistant Klebsiella pneumoniae infection relative to two types of control patients: A systematic review and meta-analysis. Antimicrob. Resist. Infect. Control 2020, 9, 23. [Google Scholar] [CrossRef]
- Okeah, B.O.; Morrison, V.; Huws, J.C. Antimicrobial stewardship and infection prevention interventions targeting healthcare-associated Clostridioides difficile and carbapenem-resistant Klebsiella pneumoniae infections: A scoping review. BMJ Open 2021, 11, e051983. [Google Scholar] [CrossRef]
- Xu, L.; Sun, X.; Ma, X. Systematic review and meta-analysis of mortality of patients infected with carbapenem-resistant Klebsiella pneumoniae. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 18. [Google Scholar] [CrossRef]
- Maraolo, A.E.; Corcione, S.; Grossi, A.; Signori, A.; Alicino, C.; Hussein, K.; Trecarichi, E.M.; Viale, P.; Timsit, J.F.; Veeraraghavan, B.; et al. The Impact of Carbapenem Resistance on Mortality in Patients with Klebsiella pneumoniae Bloodstream Infection: An Individual Patient Data Meta-Analysis of 1952 Patients. Infect. Dis. Ther. 2021, 10, 541–558. [Google Scholar] [CrossRef]
- Stewardson, A.J.; Marimuthu, K.; Sengupta, S.; Allignol, A.; El-Bouseary, M.; Carvalho, M.J.; Hassan, B.; Delgado-Ramirez, M.A.; Arora, A.; Bagga, R.; et al. Effect of carbapenem resistance on outcomes of bloodstream infection caused by Enterobacteriaceae in low-income and middle-income countries (PANORAMA): A multinational prospective cohort study. Lancet Infect. Dis. 2019, 19, 601–610. [Google Scholar] [CrossRef]
- Perez, F.; Bonomo, R.A. Carbapenem-resistant Enterobacteriaceae: Global action required. Lancet Infect. Dis. 2019, 19, 561–562. [Google Scholar] [CrossRef]
- Magiorakos, A.P.; Burns, K.; Rodríguez Baño, J.; Borg, M.; Daikos, G.; Dumpis, U.; Lucet, J.C.; Moro, M.L.; Tacconelli, E.; Simonsen, G.S.; et al. Infection prevention and control measures and tools for the prevention of entry of carbapenem-resistant Enterobacteriaceae into healthcare settings: Guidance from the European Centre for Disease Prevention and Control. Antimicrob. Resist. Infect. Control 2017, 6, 113. [Google Scholar] [CrossRef] [PubMed]
- Gnanadhas, D.P.; Marathe, S.A.; Chakravortty, D. Biocides—Resistance, cross-resistance mechanisms and assessment. Expert Opin. Investig. Drugs 2013, 22, 191–206. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Weigand, M.R.; Oh, S.; Hatt, J.K.; Krishnan, R.; Tezel, U.; Pavlostathis, S.G.; Konstantinidis, K.T. Widely Used Benzalkonium Chloride Disinfectants Can Promote Antibiotic Resistance. Appl. Environ. Microbiol. 2018, 84, e01201-18. [Google Scholar] [CrossRef]
- Maillard, J.Y. Resistance of Bacteria to Biocides. Microbiol. Spectr. 2018, 6, 1–17. [Google Scholar] [CrossRef]
- Maillard, J.Y.; Bloomfield, S.; Coelho, J.R.; Collier, P.; Cookson, B.; Fanning, S.; Hill, A.; Hartemann, P.; McBain, A.J.; Oggioni, M.; et al. Does microbicide use in consumer products promote antimicrobial resistance? A critical review and recommendations for a cohesive approach to risk assessment. Microb. Drug Resist. 2013, 19, 344–354. [Google Scholar] [CrossRef]
- Grande Burgos, M.J.; Fernández Márquez, M.L.; Pérez Pulido, R.; Gálvez, A.; Lucas López, R. Virulence factors and antimicrobial resistance in Escherichia coli strains isolated from hen egg shells. Int. J. Food Microbiol. 2016, 238, 89–95. [Google Scholar] [CrossRef]
- Piddock, L.J. Clinically relevant chromosomally encoded multidrug resistance efflux pumps in bacteria. Clin. Microbiol. Rev. 2006, 19, 382–402. [Google Scholar] [CrossRef]
- Poole, K. Efflux pumps as antimicrobial resistance mechanisms. Ann. Med. 2007, 39, 162–176. [Google Scholar] [CrossRef]
- Buffet-Bataillon, S.; Tattevin, P.; Maillard, J.Y.; Bonnaure-Mallet, M.; Jolivet-Gougeon, A. Efflux pump induction by quaternary ammonium compounds and fluoroquinolone resistance in bacteria. Future Microbiol. 2016, 11, 81–92. [Google Scholar] [CrossRef]
- Nishino, K.; Yamasaki, S.; Nakashima, R.; Zwama, M.; Hayashi-Nishino, M. Function and Inhibitory Mechanisms of Multidrug Efflux Pumps. Front. Microbiol. 2021, 12, 737288. [Google Scholar] [CrossRef] [PubMed]
- Kampf, G. Biocidal Agents Used for Disinfection Can Enhance Antibiotic Resistance in Gram-Negative Species. Antibiotics 2018, 7, 110. [Google Scholar] [CrossRef] [PubMed]
- Morante, J.; Quispe, A.M. Tolerance to disinfectants (chlorhexidine and isopropanol) and its association with antibiotic resistance in clinically-related Klebsiella pneumoniae isolates. Pathog. Glob. Health 2021, 115, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Zhong, X.; Xu, H.; Chen, D.; Zhou, H.; Hu, X.; Cheng, G. First emergence of acrAB and oqxAB mediated tigecycline resistance in clinical isolates of Klebsiella pneumoniae pre-dating the use of tigecycline in a Chinese hospital. PLoS ONE 2014, 9, e115185. [Google Scholar] [CrossRef]
- Li, J.; Zhang, H.; Ning, J.; Sajid, A.; Cheng, G.; Yuan, Z.; Hao, H. The nature and epidemiology of OqxAB, a multidrug efflux pump. Antimicrob. Resist. Infect. Control 2019, 8, 44. [Google Scholar] [CrossRef]
- Fan, Y.F.; Cui, S.Y.; Zhang, C.; Xu, X.M. Investigation of acquired drug-resistant genes and strains relationship in Pseudomonas aeruginosa isolated from burn patients. Zhonghua shao shang za zhi = Zhonghua shaoshang zazhi = Chin. J. Burn. 2018, 34, 83–87. [Google Scholar] [CrossRef]
- Shafaati, M.; Boroumand, M.; Nowroozi, J.; Amiri, P.; Kazemian, H. Correlation Between qacE and qacE∆1 Efflux Pump Genes, Antibiotic and Disinfectant Resistant Among Clinical Isolates of E.coli. Recent Pat. Anti-Infect. Drug Discov. 2016, 11, 189–195. [Google Scholar] [CrossRef]
- Guo, J.; Li, C. Molecular epidemiology and decreased susceptibility to disinfectants in carbapenem-resistant Acinetobacter baumannii isolated from intensive care unit patients in central China. J. Infect. Public Health 2019, 12, 890–896. [Google Scholar] [CrossRef]
- Carvalho, I.; Chenouf, N.S.; Carvalho, J.A.; Castro, A.P.; Silva, V.; Capita, R.; Alonso-Calleja, C.; Enes Dapkevicius, M.L.N. Multidrug-resistant Klebsiella pneumoniae harboring extended spectrum β-lactamase encoding genes isolated from human septicemias. PLoS ONE 2021, 16, e0250525. [Google Scholar] [CrossRef]
- Miller, S.; Humphries, R.M. Clinical laboratory detection of carbapenem-resistant and carbapenemase-producing Enterobacteriaceae. Expert Rev. Anti-Infect. Ther. 2016, 14, 705–717. [Google Scholar] [CrossRef]
- Tsai, Y.M.; Wang, S.; Chiu, H.C.; Kao, C.Y. Combination of modified carbapenem inactivation method (mCIM) and EDTA-CIM (eCIM) for phenotypic detection of carbapenemase-producing Enterobacteriaceae. BMC Microbiol. 2020, 20, 315. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Shan, K.; Xu, B.; Li, J. Determining the resistance of carbapenem-resistant Klebsiella pneumoniae to common disinfectants and elucidating the underlying resistance mechanisms. Pathog. Glob. Health 2015, 109, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Feßler, A.T.; Schug, A.R.; Geber, F.; Scholtzek, A.D.; Merle, R.; Brombach, J.; Hensel, V.; Meurer, M.; Michael, G.B.; Reinhardt, M.; et al. Development and evaluation of a broth macrodilution method to determine the biocide susceptibility of bacteria. Vet. Microbiol. 2018, 223, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Uzer Celik, E.; Tunac, A.T.; Ates, M.; Sen, B.H. Antimicrobial activity of different disinfectants against cariogenic microorganisms. Braz. Oral Res. 2016, 30, e125. [Google Scholar] [CrossRef][Green Version]
- Baseri, N.; Najar-Peerayeh, S.; Bakhshi, B.; Campanile, F. Phenotypic and genotypic changes of Staphylococcus aureus in the presence of the inappropriate concentration of chlorhexidine gluconate. BMC Microbiol. 2022, 22, 100. [Google Scholar] [CrossRef]
- Amini Tapouk, F.; Nabizadeh, R.; Mirzaei, N.; Hosseini Jazani, N.; Yousefi, M.; Valizade Hasanloei, M.A. Comparative efficacy of hospital disinfectants against nosocomial infection pathogens. Antimicrob. Resist. Infect. Control 2020, 9, 115. [Google Scholar] [CrossRef]
- Kim, H.B.; Wang, M.; Park, C.H.; Kim, E.C.; Jacoby, G.A.; Hooper, D.C. oqxAB encoding a multidrug efflux pump in human clinical isolates of Enterobacteriaceae. Antimicrob. Agents Chemother. 2009, 53, 3582–3584. [Google Scholar] [CrossRef]
- Hennequin, C.; Robin, F. Correlation between antimicrobial resistance and virulence in Klebsiella pneumoniae. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2016, 35, 333–341. [Google Scholar] [CrossRef]
- Hu, Y.; Anes, J.; Devineau, S.; Fanning, S. Klebsiella pneumoniae: Prevalence, Reservoirs, Antimicrobial Resistance, Pathogenicity, and Infection: A Hitherto Unrecognized Zoonotic Bacterium. Foodborne Pathog. Dis. 2021, 18, 63–84. [Google Scholar] [CrossRef]
- Pitout, J.D.; Nordmann, P.; Poirel, L. Carbapenemase-Producing Klebsiella pneumoniae, a Key Pathogen Set for Global Nosocomial Dominance. Antimicrob. Agents Chemother. 2015, 59, 5873–5884. [Google Scholar] [CrossRef]
- Sękowska, A.; Gospodarek, E.; Kusza, K. The prevalence of infections and colonisation with Klebsiella pneumoniae strains isolated in ICU patients. Anaesthesiol. Intensive Ther. 2014, 46, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Liu, C.; Shen, Z.; Zhou, H.; Cao, J.; Chen, S.; Lv, H.; Zhou, M.; Wang, Q.; Sun, L.; et al. Prevalence, risk factors and molecular epidemiology of carbapenem-resistant Klebsiella pneumoniae in patients from Zhejiang, China, 2008–2018. Emerg. Microbes Infect. 2020, 9, 1771–1779. [Google Scholar] [CrossRef] [PubMed]
- Muntean, D.; Horhat, F.G. Multidrug-Resistant Gram-Negative Bacilli: A Retrospective Study of Trends in a Tertiary Healthcare Unit. Medicina 2018, 54, 92. [Google Scholar] [CrossRef] [PubMed]
- Cristina, M.L.; Sartini, M.; Ottria, G.; Schinca, E.; Cenderello, N.; Crisalli, M.P.; Fabbri, P.; Lo Pinto, G.; Usiglio, D.; Spagnolo, A.M. Epidemiology and biomolecular characterization of carbapenem-resistant Klebsiella pneumoniae in an Italian hospital. J. Prev. Med. Hyg. 2016, 57, E149–E156. [Google Scholar] [PubMed]
- CHINET. Available online: http://www.chinets.com/ (accessed on 5 February 2020).
- Chen, I.L.; Lee, C.H.; Su, L.H.; Tang, Y.F.; Chang, S.J.; Liu, J.W. Antibiotic consumption and healthcare-associated infections caused by multidrug-resistant gram-negative bacilli at a large medical center in Taiwan from 2002 to 2009: Implicating the importance of antibiotic stewardship. PLoS ONE 2013, 8, e65621. [Google Scholar] [CrossRef] [PubMed]
- Assadian, O.; Harbarth, S.; Vos, M.; Knobloch, J.K.; Asensio, A.; Widmer, A.F. Practical recommendations for routine cleaning and disinfection procedures in healthcare institutions: A narrative review. J. Hosp. Infect. 2021, 113, 104–114. [Google Scholar] [CrossRef]
- Chen, Y.; Liao, K.; Huang, Y.; Guo, P.; Huang, H.; Wu, Z.; Liu, M. Determining the susceptibility of carbapenem resistant Klebsiella pneumoniae and Escherichia coli strains against common disinfectants at a tertiary hospital in China. BMC Infect. Dis. 2020, 20, 88. [Google Scholar] [CrossRef]
- Bhatia, M.; Loomba, P.S.; Mishra, B.; Dogra, V.; Thakur, A. Reduced susceptibility of carbapenem-resistant Klebsiella pneumoniae to biocides: An emerging threat. Indian J. Med. Microbiol. 2016, 34, 355–358. [Google Scholar] [CrossRef]
- Williamson, D.A.; Carter, G.P.; Howden, B.P. Current and Emerging Topical Antibacterials and Antiseptics: Agents, Action, and Resistance Patterns. Clin. Microbiol. Rev. 2017, 30, 827–860. [Google Scholar] [CrossRef]
- Jackson, L.; Owens, M. Does oral care with chlorhexidine reduce ventilator-associated pneumonia in mechanically ventilated adults? Br. J. Nurs. 2019, 28, 682–689. [Google Scholar] [CrossRef]
- James, P.; Worthington, H.V.; Parnell, C.; Harding, M.; Lamont, T.; Cheung, A.; Whelton, H.; Riley, P. Chlorhexidine mouthrinse as an adjunctive treatment for gingival health. Cochrane Database Syst. Rev. 2017, 3, Cd008676. [Google Scholar] [CrossRef] [PubMed]
- Scallan, R.M.; Gerathy, S.; Price, J.; Lazarus, A.M.; Metter, E.J.; Talbot, L.A. Preoperative Chlorhexidine Gluconate Bathing on a Military Medical-Surgical Unit. Mil. Med. 2020, 185 (Suppl. S2), 15–20. [Google Scholar] [CrossRef] [PubMed]
- Strich, J.R.; Palmore, T.N. Preventing Transmission of Multidrug-Resistant Pathogens in the Intensive Care Unit. Infect. Dis. Clin. N. Am. 2017, 31, 535–550. [Google Scholar] [CrossRef] [PubMed]
- Edmiston, C.E., Jr.; Bruden, B.; Rucinski, M.C.; Henen, C.; Graham, M.B.; Lewis, B.L. Reducing the risk of surgical site infections: Does chlorhexidine gluconate provide a risk reduction benefit? Am. J. Infect. Control 2013, 41 (Suppl. S5), S49–S55. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Disinfectants | MICs | MIC50 | MIC90 | QC Strains | MBCs | MBC50 | MBC90 | QC Strains | ||
|---|---|---|---|---|---|---|---|---|---|---|
| ATCC 700603 MIC | ATCC 25922 MIC | ATCC 700603 MBC | ATCC 25922 MBC | |||||||
| 0.1% Benzalkonium bromide | 16–256 | 64 | 32 | 32 | 128 | 1–128 | 16 | 2 | 4 | 32 |
| 4% Aqueous chlorhexidine | 256–32768 | 2048 | 512 | 1024 | 16384 | 16–32768 | 512 | 32 | 256 | 512 |
| 75% Alcohol | 4–64 | 8 | 8 | 8 | 8 | 2–64 | 4 | 4 | 4 | 4 |
| Entoiodine II | 64–8192 | 512 | 256 | 256 | 16384 | 16–4096 | 128 | 32 | 128 | 8192 |
| 2% Glutaraldehyde | 8–128 | 32 | 16 | 64 | 64 | 4–64 | 16 | 8 | 32 | 64 |
| 2000 mg/L Chlorine-containing disinfectants | 2–16 | 8 | 4 | 8 | 8 | 2–8 | 8 | 4 | 8 | 8 |
| 3% Hydrogen peroxide | 256–2048 | 1024 | 512 | 1024 | 2048 | 64–2048 | 512 | 256 | 512 | 1024 |
| Iodine | Chlorhexidine | 75% Alcohol |
Quaternary Ammonium Compounds | 3% Hydrogen Peroxide | Chlorine-Containing Disinfectants | 2% Glutaraldehyde | ||
|---|---|---|---|---|---|---|---|---|
| MBCMAX a | A quarter of stock solution | 2.5 g/L Aqueous chlorhexidine | Half of stock solution | Stock solution (1000 mg/L) | 468.75 mg/L | 1000 mg/L | 0.50% | |
| Skin and mucous membrane b | Skin | Stock solution | ≥2 g/L Alcoholic chlorhexidine | Stock solution | Stock solution | |||
| Mucous membrane, wound | ≥2 g/L Alcoholic chlorhexidine (wipe), ≥2 g/L Aqueous chlorhexidine (rinse, gargle) | 1000–2000 mg/L (wipe) | 3% (flush, gargle) | |||||
| Environmental surface c | Bacterial propagator, mycobacterium tuberculosis, fungus, lipophilic virus | Stock solution | 400–700 mg/L | |||||
| Bacterial propagator, fungus, lipophilic virus | 1000–2000 mg/L | |||||||
| All bacteria (including spores), fungus, virus | 1000–2000 mg/L | 2000–5000 mg/L | ||||||
| Cleaning supplies b | Wash towel | 250 mg/L | ||||||
| Floor towel | 500 mg/L | |||||||
| Flexible endoscope d | ≥2% Alkaline solution | |||||||
| Recommended concentration e | ≥2.5 g/L Aqueous chlorhexidine (rinse, gargle) | 1000 mg/L |
| Positive Detection Patterns | Positive Numbers (n) | Percentage (%) |
|---|---|---|
| qacE∆1-sul1 + oqxA | 25 | 39.1 |
| qacE∆1-sul1 | 14 | 21.9 |
| qacE∆1-sul1 + oqxA + oqxB | 6 | 9.4 |
| oqxA | 5 | 7.8 |
| oqxA + oqxB | 3 | 4.7 |
| qacE∆1-sul1 + oqxB | 1 | 1.6 |
| oqxB | 1 | 1.6 |
| Genes | Numbers | 0.1% Benzalkonium Bromide | 4% Aqueous Chlorhexidine | 75% Alcohol | Entoiodine II | 2% Glutaraldehyde | 2000 mg/L Chlorine-Containing Disinfectants | 3% Hydrogen Peroxide | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MIC | MBC | MIC | MBC | MIC | MBC | MIC | MBC | MIC | MBC | MIC | MBC | MIC | MBC | ||
| oqxA | +: 39 | 0.733 | 0.052 | 0.946 | 0.744 | 0.366 | 0.690 | 0.993 | 0.194 | 0.630 | 0.119 | 0.417 | 0.994 | 0.033 * | 0.001 * |
| −: 25 | |||||||||||||||
| oqxB | +: 11 | 0.375 | 0.993 | 0.454 | 0.820 | 0.453 | 0.532 | 0.315 | 0.146 | 0.767 | 0.701 | 0.942 | 0.505 | 0.882 | 0.341 |
| −: 53 | |||||||||||||||
| qacE∆1-sul1 | +: 46 | 0.039 * | 0.807 | 0.285 | 0.679 | 0.861 | 0.820 | 0.160 | 0.885 | 0.093 | 0.498 | 0.968 | 0.413 | 0.367 | 0.563 |
| −: 18 | |||||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ni, L.; Zhang, Z.; Shen, R.; Liu, X.; Li, X.; Chen, B.; Wu, X.; Li, H.; Xie, X.; Huang, S. Disinfection Strategies for Carbapenem-Resistant Klebsiella pneumoniae in a Healthcare Facility. Antibiotics 2022, 11, 736. https://doi.org/10.3390/antibiotics11060736
Ni L, Zhang Z, Shen R, Liu X, Li X, Chen B, Wu X, Li H, Xie X, Huang S. Disinfection Strategies for Carbapenem-Resistant Klebsiella pneumoniae in a Healthcare Facility. Antibiotics. 2022; 11(6):736. https://doi.org/10.3390/antibiotics11060736
Chicago/Turabian StyleNi, Lijia, Zhixian Zhang, Rui Shen, Xiaoqiang Liu, Xuexue Li, Baiji Chen, Xiquan Wu, Hongyu Li, Xiaoying Xie, and Songyin Huang. 2022. "Disinfection Strategies for Carbapenem-Resistant Klebsiella pneumoniae in a Healthcare Facility" Antibiotics 11, no. 6: 736. https://doi.org/10.3390/antibiotics11060736
APA StyleNi, L., Zhang, Z., Shen, R., Liu, X., Li, X., Chen, B., Wu, X., Li, H., Xie, X., & Huang, S. (2022). Disinfection Strategies for Carbapenem-Resistant Klebsiella pneumoniae in a Healthcare Facility. Antibiotics, 11(6), 736. https://doi.org/10.3390/antibiotics11060736