Abstract
The aim of this clinical case study was to observe biopsy tissues at 5 months after an autograft of a partially demineralized dentin/cementum matrix (pDDM) into a tooth-extracted socket exhibiting healing failure. A 66-year-old female presented with healing failure in the cavity for 2 months after the extraction (#36). Initial X-ray photos showed a clear remainder of lamina dura (#36), a residual root (#37), and a horizontal impaction (#38). The vital tooth (#38) was selected for pDDM. The third molar crushed by electric mill was decalcified in 1.0 L of 2.0% HNO3 for 20 min and rinsed in cold distilled water. The pDDM granules (size: 0.5–2.0 mm) were grafted immediately into the treated socket. X-ray views just after pDDM graft showed radio-opaque granules. At 5 months after pDDM graft, the surface of regenerated bone was harmonized with the mandibular line, and bone-like radio-opacity was found in the graft region. The biopsy tissue (diameter: 3.0 mm) at 5 months after pDDM graft showed that mature bone was interconnected with the remaining pDDM. The novel histological evidence highlighted that newly formed bone was connected directly with both dentin-area and cementum-area matrix of pDDM. We concluded that pDDM contributed to the regeneration of bone in the unhealed socket, and this regeneration prepared the socket for implant placement. Autogenous pDDM could be immediately recycled as an innovative biomaterial for local bone regeneration.
1. Introduction
Extracted teeth are usually discarded as potentially infectious medical waste. However, the dental community is now considering human primary and secondary teeth as a useful material resource for patients and their families [1]. The first clinical case of human dentin autograft was reported in 2003 [2], while human bone autograft dates back to 1820 in Italy. There was a very long time-lag between the autografts of dentin and bone. Demineralized dentin/cementum matrix (DDM) is a decellularized matrix prepared through demineralization (<pH 1.0), washing by saline or distilled water, and/or freeze-drying [3]. Recently, many autograft cases were reported from the world [4,5,6,7,8,9]. Additionally, familial grafts between a parent and a child were successfully achieved, and the first successful procedure occurred in South Korea [10]. In this century, the tooth-derived materials have become a realistic alternative to bone grafting [7,11].
Highly calcified tissues such as fresh cortical bone and dentin do not occur earlier in osteoinduction and bone formation than DDM and demineralized bone matrix (DBM) [12,13,14,15]. In 2016, 70% of demineralized human DDM granules (size: 1.0 mm) had a better performance in bone formation than completely DDM (cDDM) and non-demineralized dentin in rat calvarial bone defects [16]. In 2021, cortical bone plate treated supersonically with acidic electrolyzed water (pH 2.3), so-called partial DBM (pDBM), induced bone at 2 weeks, while fresh cortical bone plate did not induce bone even at 8 weeks [17]. In light of the articles [13,14,15,16,17], we believed that the apatite crystals of both calcified dentin and cortical bone should inhibit a release of bone morphogenetic proteins (BMPs) from matrices. Clinically, the immediate DDM autograft system needs speed, compared to the delayed autograft. Our team, therefore, developed the immediate autograft system of partially demineralized dentin/cementum matrix (pDDM) by using a new electric mill [3,18].
The aim of this case study was to observe the biopsy tissues obtained from the dental implant-placed region at 5 months after pDDM autograft into the socket that had exhibited healing failure (#36) for 2 months. The histological evidence highlighted that new bone was connected directly with not only dentin-area matrix, but also cementum-area matrix of pDDM.
2. Materials and Methods
2.1. Clinical Case
A 66-year-old female presented with healing failure in the extracted cavity (#36) for 2 months after the extraction in a private dental clinic. The patient was introduced to our dental clinic in 2009. Clinical diagnosis revealed healing failure in the socket. Initial X-ray photos showed a clear remaining of lamina dura (#36), a residual root (#37), and a horizontal impaction (#38) (Figure 1). Her medical history was unremarkable.
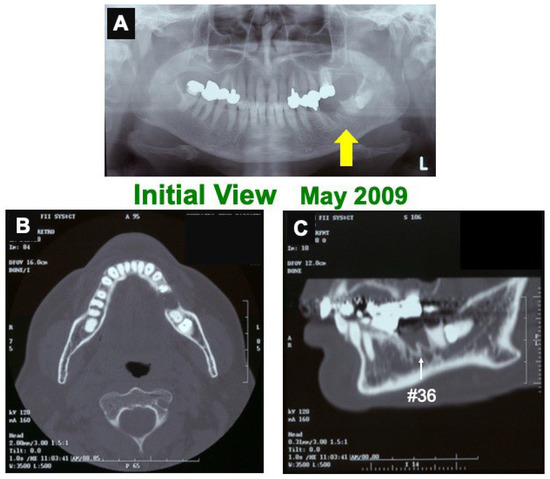
Figure 1.
Initial views of panoramic X-ray photo (A) and CT (B,C). (A) Arrow indicating clear remaining of lamina dura (#36 socket). (B) Horizontal-axis view showing frame of mandible and non-bony socket (#36). (C) Sagittal-axis view showing sclerotic line (↑) of lamina dura (#36), residual root (#37), and horizontal impaction (#38).
2.2. Surgical Procedure 1 and Preparation of pDDM
First, both #37 and #38 were extracted under local anesthesia. The impacted vital-tooth (#38) was selected for pDDM, while #37 was a non-vital. The third molar (#38) was crushed with saline ice blocks in zirconium (ZrO2) vessel at 12,000 rpm for 1 min by our newly developed electric mill (OSTEO-MILL™, WiSM Mutoh Co., Ltd., Tokyo, Japan) [15,16]. The crushed tooth granules were immediately decalcified in 1.0 L of 2.0% HNO3 solution for 20 min. The pDDM granules including cementum (size: 0.5–2.0 mm) were extensively rinsed in cold distilled water (D.W) (Figure 2).
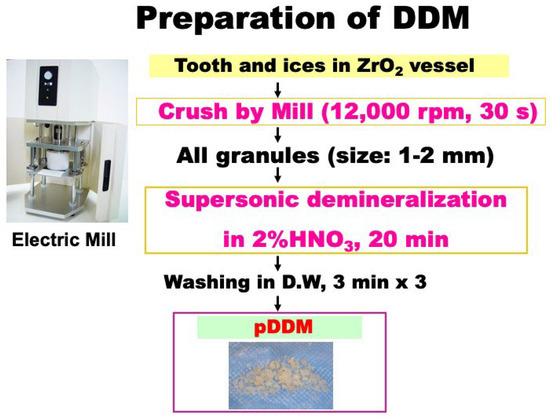
Figure 2.
Preparation of partially demineralized dentin/cementum matrix (pDDM). ZrO2: zirconium.
After the removing of epithelium and the cleaning of the socket by curettage, perforations into the dense bone in socket were performed by a curbide bur (Figure 3A), and the pDDM granules were grafted immediately into the treated socket (Figure 3B). The flap after relaxation incision was sutured with nylon threads (Figure 3C,D). The patient only took antibiotics for 2 days.
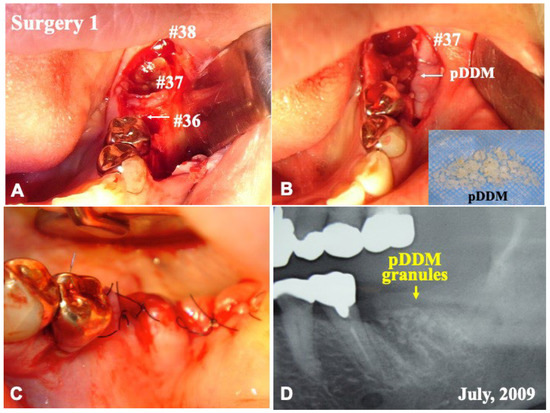
Figure 3.
Surgery 1. (A) Gross view just after elevation of flap. (B) Immediate graft of pDDM granules into treated socket (#36). (C) Closed wound by sutures. (D) X-ray showing shadow of grafted pDDM (↓) and sockets after extraction of #37 and #38.
2.3. Surgical Procedure 2 and Tissue Biopsy
At 5 months after surgery 1, tissue biopsy (hole: 3.0 mm) was carried out from the central area of a fixture placement for the tissue observation under local anesthesia (Figure 4A–C). Next, a titanium-fixture (HAp coating type: diameter, 4.2 mm; length, 10 mm; POI system, KYOCERA Co., Ltd., Kyoto, Japan) was implanted into the regenerated bone (Figure 4D), and the flap was repositioned. The patient took antibiotics for 3 days. There were no troubles until the finishing of whole treatments.
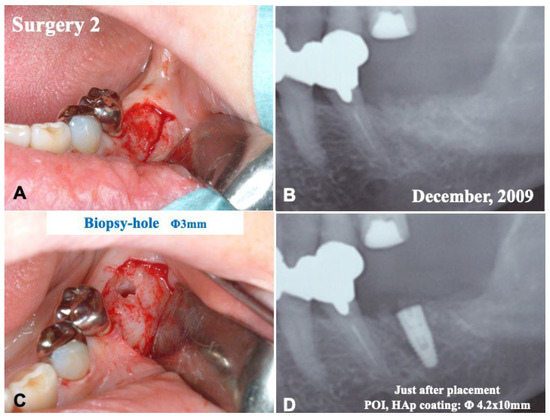
Figure 4.
Surgery 2. (A) Gross view just after elevation of flap. (B) X-ray photo showing remodeled bone-like shadow (#36). (C) Biopsy (hole: 3 mm). (D) X-ray photo showing placement of fixture.
2.4. Radiographic Evaluation
Initial X-ray photos including CT were taken in 2009 before pDDM graft. Next, X-ray photos were taken just after the pDDM graft (Figure 3D) (Surgical Procedure 1), and before and after the fixture placement (Surgical Procedure 2).
2.5. Tissue Preparation
Biopsy tissue was fixed with 10% neutral buffered formalin, decalcified for 7 days with 10% formic acid, and embedded in paraffin. Sections (with a thickness of 4 μm) were stained with hematoxylin and eosin (HE).
3. Results
3.1. Gross View and Radiographic Evaluation
Before the pDDM graft (Surgery 1), the lamina dura (#36) remained clear. (Figure 1A,C). Just after the pDDM graft, pDDM were seen like radio-opaque granules in the treated socket (Figure 3D). At 5 months (Surgery 2), a smooth surface line was seen on the graft site after the opening of mucoperiosteal flap (Figure 4A). The grafted pDDM was harmonized with the mandible, and a bone-like radio-opacity was found in the graft region (Figure 4B). A titanium-fixture was placed properly after the biopsy (Figure 4C,D). The final crown was set (Figure 5A,B) and functionality was well maintained. During the whole follow-up period, a complication, such as marginal bone loss, did not occur (Figure 5C).
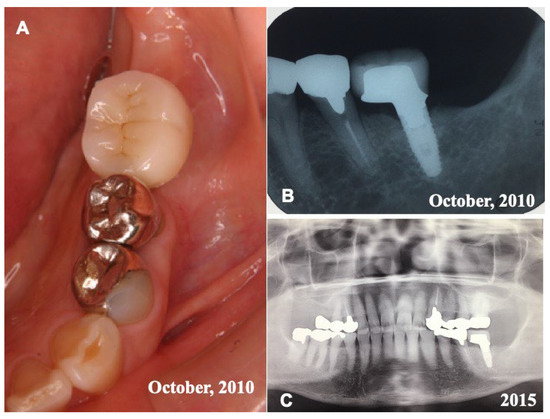
Figure 5.
Final crown and X-ray photos. (A) Set of final resin crown in 2010. (B) X-ray photo in 2010 showing fixture with crown. (C) X-ray photo in 2015 showing good appearance at 6 years after placement of fixture.
3.2. Histological Findings of Biopsy Tissue at 5 Months after pDDM Autograft
The biopsy tissue showed that mature bone was interconnected with the remained pDDM granules (Figure 6A,B). pDDM included a small patch of cementum. The regenerated bone was connected directly with dentin- and cementum-area matrix of pDDM residues (Figure 6C,D). The dentin-derived areas revealed dentinal tube spaces and acellur matrix, while the cementum-derived area showed Sharpey’s fibers structure (Figure 6D). The boundary line between the dentin- and cementum-area matrices was seen clearly (Figure 6C,D).
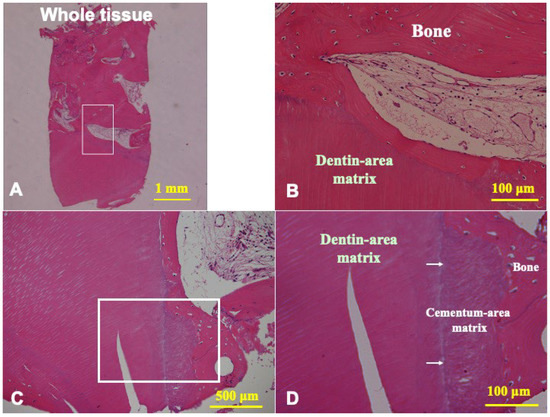
Figure 6.
Histological photographs of HE sections of biopsy tissue at 5 months after pDDM graft. (A) Whole view indicating mix of newly formed bone and residues of pDDM. (B) Higher magnification of frame in (A). New bone connected with dentin-area matrix of pDDM. (C) pDDM including small patch of cementum. Mature bone connected with cementum- and dentin-area matrix of pDDM. (D) Higher magnification of frame in (C). Cementum-area matrix directly connected with regenerated bone. Arrows indicating boundary between cementum- and dentin-area matrices.
4. Discussion
The biopsy tissue at 5 months after pDDM graft showed that the pDDM were received by the host and were harmonized with bone. Very interestingly, the histological evidence highlighted that newly formed bone was connected directly with dentin- and cementum-area matrices of the pDDM. This is novel evidence related to the direct bonding of new bone and demineralized cementum in clinical cases. We found that pDDM facilitated its adaption of the grafted site and was slowly absorbed as new bone began to form. As pDDM granules contain non-demineralized core (calcified matrix), the absorption of pDDM should take much more time than that of cDDM.
Dentin and bone are mineralized tissues and almost similar in chemical components. As bone and dentin consist of fluid (10%), collagen (20%), and apatite (70%) in weight volume [2,11], our attention for biomaterials focus on natural components such as collagen and apatite materials [19]. Both freeze-dried cDDM and cDBM are predominately composed of type I collagen (95%) and the remaining of non-collagenous proteins that contain a small amount of growth factors [20]. Both mature and immature types of bone morphogenetic protein-2 (BMP-2) were detected in human dentin and dental pulps by western-blotting [21]. Even after the demineralization of dentin and bone, active types of BMPs bind to acid-insoluble and collagen-rich matrices [11,22]. Interestingly, the strong acid treatment for bone- and dentin-derived materials increased their osteoinductivity and decreased their antigenicity [23]. Reduction and alkylation of BMP molecules resulted in the total loss of biological activity [24]. Additionally, after the processing system with 2.0% HNO3-demineralization as shown in Figure 2, bacteria free of pDDM granules were confirmed in the blood-agar medium [25]. From clinical points of view, sterilization by strong acid and safety are very important evidences for the processing procedures of hard tissue-derived graft materials [23,24,25]. After the immediate autograft of pDDM, thw patient was successfully restored to health with a dental implant. In the near future, ultrasound imaging will support histological findings and/or radiographic appearances as a non-invasive diagnostic tool [26].
5. Conclusions
The biopsy tissue at 5 months after immediate autograft of pDDM demonstrated novel histological evidences that new bone was connected directly with dentin- and cementum-area matrix of pDDM. A vital tooth-derived pDDM granules contributed to regenerate bone in an unhealed socket in a 66-year-old woman. After the pDDM autograft, the patient was successfully restored with a dental implant. Autogenous pDDM could be immediately recycled in our system as an innovative biomaterial for local bone engineering.
Author Contributions
Surgery and writing, M.M. and Y.H.; Preparation of pDDM, M.A.K.; Prosthodontics, Y.H. and M.O.; Development of DDM system, N.O., H.K. and T.A.; Graphic, M.M.; All authors have read and agreed to the published version of the manuscript.
Funding
This project was greatly supported by the grant (consortium: 2004-5) of Japan Ministry of Economy, Trade and Industry.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Health Sciences University of Hokkaido (approval code No.29) for studies involving humans.
Informed Consent Statement
Informed Consent was obtained from all subjects in this case.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kamiura, Y.; Kumazawa, R.; Kumazawa, T.; Murata, M.; Akazawa, T. Maxillary implant restration with autograft of decalcified dentin matrix. In Advances in Oral Tissue Engineering; Murata, M., Um, I.W., Eds.; Quintessence Publishing Co. Inc.: Chicago, IL, USA, 2014; pp. 51–53. [Google Scholar]
- Murata, M.; Akazawa, T.; Mitsugi, M.; Kabir, M.A.; Minamida, Y.; Um, I.W.; Kim, K.W.; Kim, Y.; Sun, Y.; Qin, C. Autograft of Dentin Materials for Bone Regeneration. In Advances in Biomaterials Science and Biomedical Applications; Pignatello, R., Ed.; INTECH Publisher: Rijeka, Croatia, 2013; pp. 391–403. [Google Scholar]
- Akazawa, T.; Murata, M.; Hino, J.; Nakamura, K.; Kikuchi, M.; Mitsugi, M.; Um, I.W. Surfaces design and functional control of demineralized dentin matrix granules derived from human teeth. In Advances in Oral Tissue Engineering; Murata, M., Um, I.W., Eds.; Quintessence Publishing Co, Inc.: Chicago, IL, USA, 2014; pp. 37–42. [Google Scholar]
- Kabir, M.A.; Murata, M.; Kusano, K.; Zakaria, S.M.; Noor, A.H.; Khuda, F.; Hossain, I.; Sultana, S.; Saito, T. Radiological evaluation of human dentin autografts in Bangladesh. J. Hard Tissue Biol. 2014, 23, 363–370. [Google Scholar] [CrossRef][Green Version]
- Li, P.; Zhu, H.; Huang, D. Autogenous DDM versus Bio-Oss granules in GBR for immediate implantation in periodontal postextraction sites: A prospective clinical study. Clin. Implant. Dent. Relat. Res. 2018, 20, 923–928. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Kim, Y.K.; Park, Y.H.; Park, J.C.; Ku, J.K.; Um, I.W.; Kim, J.Y. Evaluation of the healing potential of demineralized dentin matrix fixed with recombinant human bone morphogenetic protein-2 in bone grafts. Materials 2017, 10, 1049. [Google Scholar] [CrossRef] [PubMed]
- Um, I.W.; Ku, J.K.; Kim, Y.M.; Yun, P.Y.; Chang, N.H.; Kim, Y.K.; Choi, Y. Allogenic demineralized dentin matrix graft for guided bone regeneration in dental implants. Appl. Sci. 2020, 10, 4661. [Google Scholar] [CrossRef]
- Umebayashi, M.; Ohba, S.; Kurogi, T.; Noda, S.; Asahina, I. Full regeneration of maxillary alveolar bone using autogenous partially demineralized dentin matrix and particulate cancellous bone and marrow for implant-supported full arch rehabilitation. J. Oral Implantol. 2020, 1, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Okubo, N.; Ishikawa, M.; Shakya, M.; Hosono, H.; Maehara, O.; Ohkawara, T.; Ohnishi, S.; Akazawa, T.; Murata, M. Autograft of demineralized dentin matrix prepared immediately after extraction for horizontal bone augmentation of the anterior atrophic maxilla: A first case of non-vital tooth-derived dentin. J. Hard Tissue Biol. 2022, 23, 363–370. [Google Scholar] [CrossRef]
- Um, I.W.; Lee, J.K. Familial tooth bone graft. In Advances in Oral Tissue Engineering; Murata, M., Um, I.W., Eds.; Quintessence Publishing Co, Inc.: Chicago, IL, USA, 2014; pp. 67–72. [Google Scholar]
- Murata, M.; Okubo, N.; Shakya, M.; Kabir, M.A.; Yokozeki, K.; Zhu, B.W.; Ishikawa, M.; Kitamura, R.; Akazawa, T. Dentin Materials as Biological Scaffolds for Tissue Engineering. In Biomaterial-Supported Tissue Reconstruction or Regeneration; IntechOpen: London, UK, 2019; pp. 25–36. [Google Scholar]
- Bang, G.; Urist, M.R. Bone induction in excavation chambers in matrix of decalcified dentin. Arch. Surg. 1964, 94, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Yeomans, J.D.; Urist, M.R. Bone induction by decalcified dentine implanted into oral, osseous and muscle tissues. Arch. Oral Biol. 1964, 12, 999–1008. [Google Scholar] [CrossRef]
- Huggins, C.; Wiseman, S.; Reddi, A.H. Transformation of fibroblasts by allogeneic and xenogeneic transplants of demineralized tooth and bone. J. Exp. Med. 1970, 132, 1250–1258. [Google Scholar] [CrossRef] [PubMed]
- Shakya, M.; Yokozeki, K.; Akazawa, T.; Murata, M. Rapid bone induction of cortical bone treated with ultrasonic demineralization in acidic electrolyzed water. J. Hard Tissue Biol. 2018, 27, 269–271. [Google Scholar] [CrossRef]
- Koga, T.; Minamizato, T.; Kawai, Y.; Miura, K.; Nakatani, Y.; Sumita, Y.; Asahina, I. Bone regeneration using dentin matrix depends on the degree of demineralization and particle size. PLoS ONE 2016, 11, e0147235. [Google Scholar] [CrossRef] [PubMed]
- Shakya, M.; Murata, M.; Yokozeki, K.; Akazawa, T.; Nagayasu, H.; Adhikari, B.R.; Upadhyaya, C. Accelerated bone induction of adult rat compact bone plate scratched by ultrasonic scaler using acidic electrolyzed water. Materials 2021, 17, 3347. [Google Scholar] [CrossRef] [PubMed]
- Murata, M.; Akazawa, T.; Takahata, M.; Ito, M.; Tazaki, J.; Hino, J.; Nakamura, K.; Iwasaki, N.; Shibata, T.; Arisue, M. Bone induction of human tooth and bone crushed by newly developed automatic mill. J. Ceram. Soc. Jpn. 2010, 118, 434–437. [Google Scholar] [CrossRef][Green Version]
- Murata, M.; Maki, F.; Sato, D.; Shibata, T.; Arisue, M. Bone augmentation by onlay implant using recombinant human BMP-2 and collagen on adult rat skull without periosteum. Clin. Oral Implant. Res. 2000, 11, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Finkelman, R.D.; Mohan, S.; Jennings, J.C.; Taylor, A.K.; Jepsen, S.; Baylink, D.J. Quantitation of growth factors IGF-I, SGF/IGF-II, and TGF-beta in human dentin. J. Bone Min. Res. 1990, 5, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Arakawa, T.; Murata, M.; Takuma, T.; Arisue, M. Expression of bone morphogenetic proteins (BMPs) in human dental pulp tissues. J. Hard Tissue Biol. 2007, 16, 199–204. [Google Scholar] [CrossRef][Green Version]
- Urist, M.R.; Iwata, H.; Ceccotti, P.L.; Dorfman, R.L.; Boyd, S.D.; McDowell, R.M.; Chien, C. Bone morphogenesis in implants of insoluble bone gelatin. Proc. Nat. Acad. Sci. USA 1973, 70, 3511–3515. [Google Scholar] [CrossRef] [PubMed]
- Reddi, A.H. Bone matrix in the solid state: Geometric influence on differentiation of fibroblasts. Adv. Biol. Med. Phys. 1974, 15, 1–18. [Google Scholar] [PubMed]
- Luyten, F.P.; Cunningham, N.S.; Ma, S.; Muthukumaran, N.; Hammonds, R.G.; Nevins, W.B.; Woods, W.I.; Reddi, A.H. Purification and partial amino acid sequence of osteogenin, a protein initiating bone differentiation. J. Biol. Chem. 1989, 264, 13377–13380. [Google Scholar] [CrossRef]
- Fujita, M.; Uehara, O.; Miyakawa, H.; Naito, S.; Kabir, M.A.; Murata, M.; Nakazawa, F. Detection of bacteria in human tooth-derived biomaterials. In Advances in Oral Tissue Engineering; Murata, M., Um, I.W., Eds.; Quintessence Publishing Co, Inc.: Chicago, IL, USA, 2014; pp. 31–32. [Google Scholar]
- Patil, S.; Alkahtani, A.; Bhandi, S.; Mashyakhy, M.; Alvarez, M.; Alroomy, R.; Hendi, A.; Varadarajan, S.; Reda, R.; Raj, A.T.; et al. Ultrasound imaging versus radiographs in differentiating periapical lesions: A systematic review. Diagnostics 2021, 3, 1208. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).