Post-Traumatic Sepsis Is Associated with Increased C5a and Decreased TAFI Levels


Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Patients
2.3. Blood Processing and Analysis
2.4. Statistics
3. Results
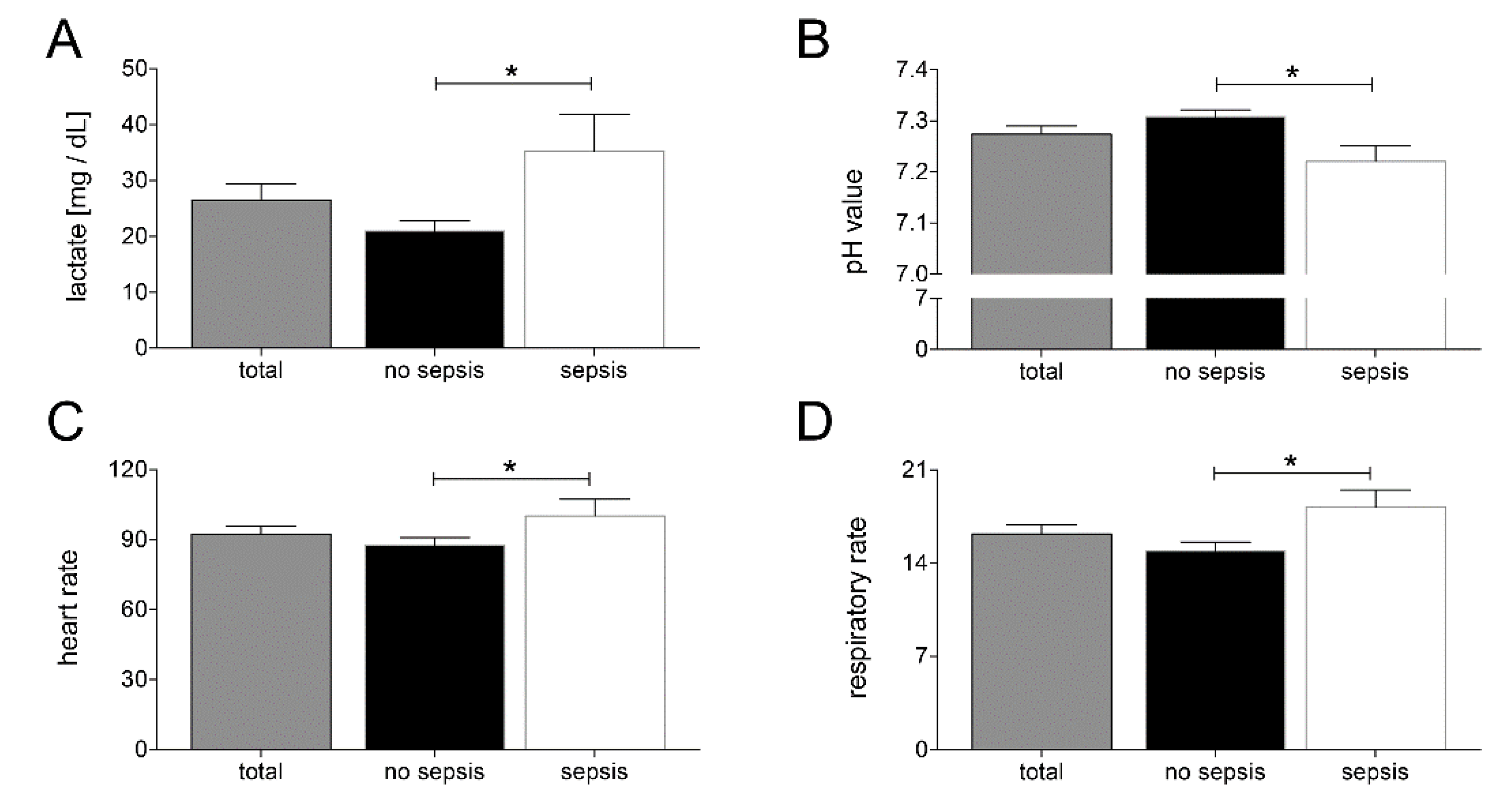
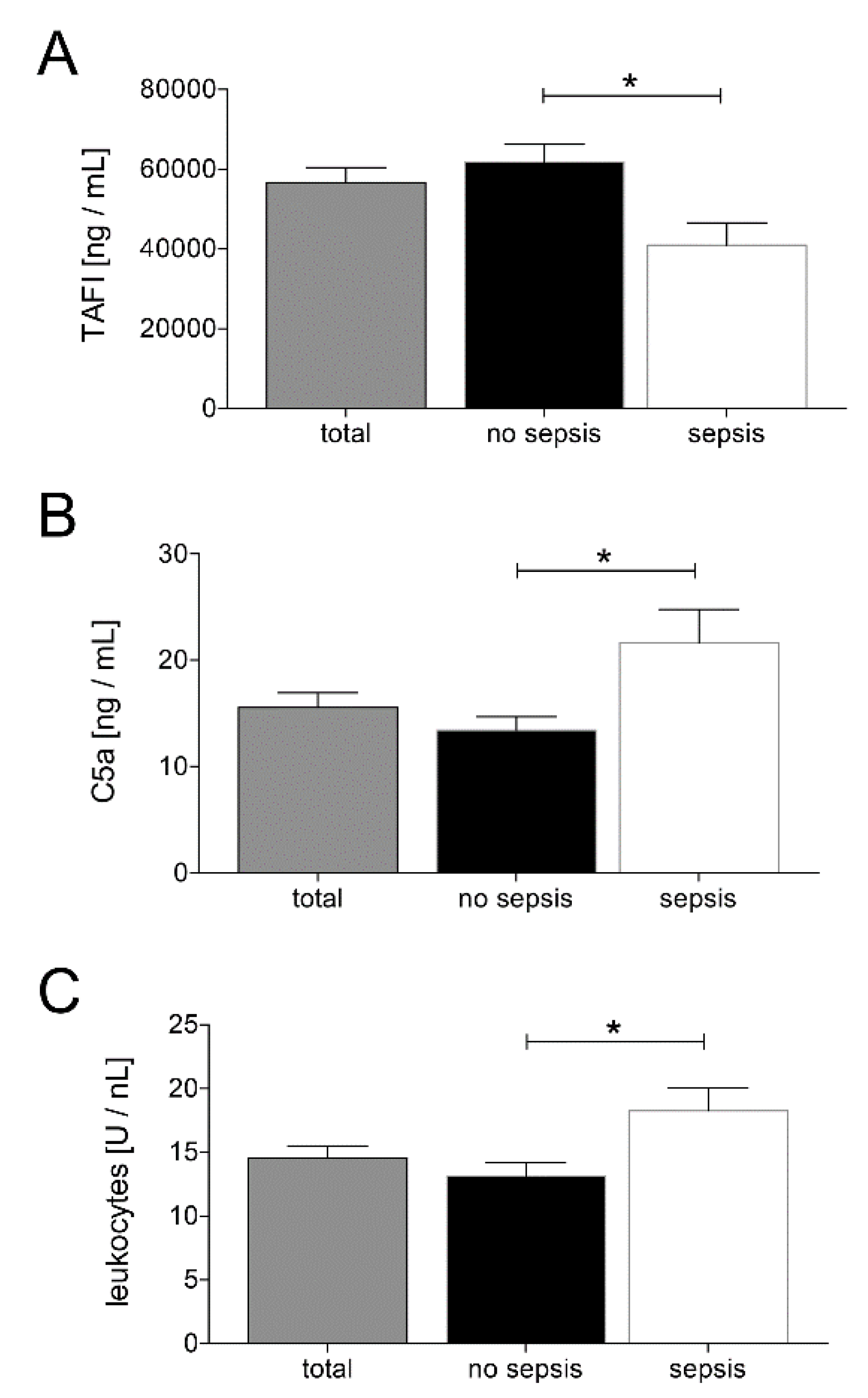
Main Findings
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Norton, R.; Kobusingye, O. Injuries. N. Engl. J. Med. 2013, 368, 1723–1730. [Google Scholar] [CrossRef]
- Osborn, T.M.; Tracy, J.K.; Dunne, J.R.; Pasquale, M.; Napolitano, L.M. Epidemiology of sepsis in patients with traumatic injury. Crit. Care Med. 2004, 32, 2234–2240. [Google Scholar] [CrossRef]
- Relja, B.; Land, W.G. Damage-associated molecular patterns in trauma. Eur. J. Trauma Emerg. Surg. 2019, 1–25. [Google Scholar] [CrossRef]
- Relja, B.; Mors, K.; Marzi, I. Danger signals in trauma. Eur. J. Trauma Emerg. Surg. 2018, 44, 301–316. [Google Scholar] [CrossRef]
- Nast-Kolb, D.; Aufmkolk, M.; Rucholtz, S.; Obertacke, U.; Waydhas, C. Multiple organ failure still a major cause of morbidity but not mortality in blunt multiple trauma. J. Trauma 2001, 51, 835–841, discussion 41-2. [Google Scholar] [CrossRef]
- Markiewski, M.M.; DeAngelis, R.A.; Lambris, J.D. Complexity of complement activation in sepsis. J. Cell Mol. Med. 2008, 12, 2245–2254. [Google Scholar] [CrossRef]
- Ward, P.A. The harmful role of c5a on innate immunity in sepsis. J. Innate Immun. 2010, 2, 439–445. [Google Scholar] [CrossRef]
- Foley, J.H.; Kim, P.Y.; Mutch, N.J.; Gils, A. Insights into thrombin activatable fibrinolysis inhibitor function and regulation. J. Thromb. Haemost. 2013, 11 (Suppl. 1), 306–315. [Google Scholar]
- Bouma, B.N.; Mosnier, L.O. Thrombin activatable fibrinolysis inhibitor (TAFI) at the interface between coagulation and fibrinolysis. Pathophysiol. Haemost. Thromb. 2003, 33, 375–381. [Google Scholar] [CrossRef]
- Muto, Y.; Suzuki, K.; Iida, H.; Sakakibara, S.; Kato, E.; Itoh, F.; Kakui, N.; Ishii, H. EF6265, a novel inhibitor of activated thrombin-activatable fibrinolysis inhibitor, protects against sepsis-induced organ dysfunction in rats. Crit. Care Med. 2009, 37, 1744–1749. [Google Scholar] [CrossRef]
- Ravindranath, T.M.; Goto, M.; Demir, M.; Tobu, M.; Kujawski, M.F.; Hoppensteadt, D.; Samonte, V.; Iqbal, O.; Sayeed, M.M.; Fareed, J. Tissue factor pathway inhibitor and thrombin activatable fibrinolytic inhibitor plasma levels following burn and septic injuries in rats. Clin. Appl Thromb. Hemost. 2004, 10, 379–385. [Google Scholar] [CrossRef]
- Verbon, A.; Meijers, J.C.; Spek, C.A.; Hack, C.E.; Pribble, J.P.; Turner, T.; Dekkers, P.E.; Axtelle, T.; Levi, M.; van Deventer, S.J.; et al. Effects of IC14, an anti-CD14 antibody, on coagulation and fibrinolysis during low-grade endotoxemia in humans. J. Infect. Dis. 2003, 187, 55–61. [Google Scholar] [CrossRef]
- Watanabe, R.; Wada, H.; Watanabe, Y.; Sakakura, M.; Nakasaki, T.; Mori, Y.; Nishikawa, M.; Gabazza, E.C.; Nobori, T.; Shiku, H. Activity and antigen levels of thrombin-activatable fibrinolysis inhibitor in plasma of patients with disseminated intravascular coagulation. Thromb. Res. 2001, 104, 1–6. [Google Scholar] [CrossRef]
- Relja, B.; Lustenberger, T.; Puttkammer, B.; Jakob, H.; Morser, J.; Gabazza, E.C.; Takei, Y.; Marzi, I. Thrombin-activatable fibrinolysis inhibitor (TAFI) is enhanced in major trauma patients without infectious complications. Immunobiology 2013, 218, 470–476. [Google Scholar] [CrossRef]
- Ricklin, D.; Hajishengallis, G.; Yang, K.; Lambris, J.D. Complement: A key system for immune surveillance and homeostasis. Nat. Immunol. 2010, 11, 785–797. [Google Scholar] [CrossRef]
- Ajona, D.; Ortiz-Espinosa, S.; Pio, R. Complement anaphylatoxins C3a and C5a: Emerging roles in cancer progression and treatment. Semin. Cell Dev. Biol. 2019, 85, 153–163. [Google Scholar] [CrossRef]
- Blatt, A.Z.; Saggu, G.; Kulkarni, K.V.; Cortes, C.; Thurman, J.M.; Ricklin, D.; Lambris, J.D.; Valenzuela, J.G.; Ferreira, V.P. Properdin-Mediated C5a Production Enhances Stable Binding of Platelets to Granulocytes in Human Whole Blood. J. Immunol. 2016, 196, 4671–4680. [Google Scholar] [CrossRef]
- Satyam, A.; Graef, E.R.; Lapchak, P.H.; Tsokos, M.G.; Dalle Lucca, J.J.; Tsokos, G.C. Complement and coagulation cascades in trauma. Acute Med. Surg. 2019, 6, 329–335. [Google Scholar] [CrossRef]
- Guo, R.F.; Ward, P.A. Role of C5a in inflammatory responses. Ann. Rev. Immunol. 2005, 23, 821–852. [Google Scholar] [CrossRef]
- Clarke, A.R.; Christophe, B.R.; Khahera, A.; Sim, J.L.; Connolly, E.S., Jr. Therapeutic Modulation of the Complement Cascade in Stroke. Front. Immunol. 2019, 10, 1723. [Google Scholar] [CrossRef]
- Keshari, R.S.; Silasi, R.; Popescu, N.I.; Patel, M.M.; Chaaban, H.; Lupu, C.; Coggeshall, K.M.; Mollnes, T.E.; DeMarco, S.J.; Lupu, F. Inhibition of complement C5 protects against organ failure and reduces mortality in a baboon model of Escherichia coli sepsis. Proc. Natl. Acad. Sci. USA 2017, 114, E6390–E6399. [Google Scholar] [CrossRef]
- Declerck, P.J. Thrombin activatable fibrinolysis inhibitor. Hamostaseologie 2011, 31, 165–166;168–173. [Google Scholar] [CrossRef]
- Hugenholtz, G.C.; Meijers, J.C.; Adelmeijer, J.; Porte, R.J.; Lisman, T. TAFI deficiency promotes liver damage in murine models of liver failure through defective down-regulation of hepatic inflammation. Thromb. Haemost. 2013, 109, 948–955. [Google Scholar] [CrossRef]
- Eguchi, A.; Franz, N.; Kobayashi, Y.; Iwasa, M.; Wagner, N.; Hildebrand, F.; Takei, Y.; Marzi, I.; Relja, B. Circulating Extracellular Vesicles and Their miR “Barcode” Differentiate Alcohol Drinkers with Liver Injury and Those Without Liver Injury in Severe Trauma Patients. Front. Med. 2019, 6, 30. [Google Scholar] [CrossRef]
- Calandra, T.; Cohen, J. International Sepsis Forum Definition of Infection in the ICUCC. The international sepsis forum consensus conference on definitions of infection in the intensive care unit. Crit. Care Med. 2005, 33, 1538–1548. [Google Scholar] [CrossRef]
- Shankar-Hari, M.; Phillips, G.S.; Levy, M.L.; Seymour, C.W.; Liu, V.X.; Deutschman, C.S.; Angus, D.C.; Rubenfeld, G.D.; Singer, M.; Sepsis Definitions Task, F. Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 775–787. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Levi, M.; Nieuwdorp, M.; van der Poll, T.; Stroes, E. Metabolic modulation of inflammation-induced activation of coagulation. Semin. Thromb. Hemost. 2008, 34, 26–32. [Google Scholar] [CrossRef]
- Okamoto, T.; Tanigami, H.; Suzuki, K.; Shimaoka, M. Thrombomodulin: A bifunctional modulator of inflammation and coagulation in sepsis. Crit. Care Res. Pract. 2012, 2012, 614545. [Google Scholar] [CrossRef]
- Myles, T.; Nishimura, T.; Yun, T.H.; Nagashima, M.; Morser, J.; Patterson, A.J.; Pearl, R.G.; Leung, L.L. Thrombin activatable fibrinolysis inhibitor, a potential regulator of vascular inflammation. J. Biol. Chem. 2003, 278, 51059–51067. [Google Scholar] [CrossRef]
- Chakraborty, S.; Karasu, E.; Huber-Lang, M. Complement After Trauma: Suturing Innate and Adaptive Immunity. Front. Immunol. 2018, 9, 2050. [Google Scholar] [CrossRef] [PubMed]
- Burk, A.M.; Martin, M.; Flierl, M.A.; Rittirsch, D.; Helm, M.; Lampl, L.; Bruckner, U.; Stahl, G.L.; Blom, A.M.; Perl, M.; et al. Early complementopathy after multiple injuries in humans. Shock 2012, 37, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Zeerleder, S.; Schroeder, V.; Hack, C.E.; Kohler, H.P.; Wuillemin, W.A. TAFI and PAI-1 levels in human sepsis. Thromb. Res. 2006, 118, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Lustenberger, T.; Relja, B.; Puttkammer, B.; Gabazza, E.C.; Geiger, E.; Takei, Y.; Morser, J.; Marzi, I. Activated thrombin-activatable fibrinolysis inhibitor (TAFIa) levels are decreased in patients with trauma-induced coagulopathy. Thromb. Res. 2013, 131, e26–e30. [Google Scholar] [CrossRef]
- Naito, M.; Taguchi, O.; Kobayashi, T.; Takagi, T.; D’Alessandro-Gabazza, C.N.; Matsushima, Y.; Boveda-Ruiz, D.; Gil-Bernabe, P.; Matsumoto, T.; Chelakkot-Govindalayathil, A.L.; et al. Thrombin-activatable fibrinolysis inhibitor protects against acute lung injury by inhibiting the complement system. Am. J. Respir. Cell Mol. Biol. 2013, 49, 646–653. [Google Scholar] [CrossRef]
- Nishimura, T.; Myles, T.; Piliponsky, A.M.; Kao, P.N.; Berry, G.J.; Leung, L.L. Thrombin-activatable procarboxypeptidase B regulates activated complement C5a in vivo. Blood 2007, 109, 1992–1997. [Google Scholar] [CrossRef]
- Fujiwara, A.; Taguchi, O.; Takagi, T.; D’Alessandro-Gabazza, C.N.; Boveda-Ruiz, D.; Toda, M.; Yasukawa, A.; Matsushima, Y.; Miyake, Y.; Kobayashi, H.; et al. Role of thrombin-activatable fibrinolysis inhibitor in allergic bronchial asthma. Lung 2012, 190, 189–198. [Google Scholar] [CrossRef]
- Song, J.J.; Hwang, I.; Cho, K.H.; Garcia, M.A.; Kim, A.J.; Wang, T.H.; Lindstrom, T.M.; Lee, A.T.; Nishimura, T.; Zhao, L.; et al. Plasma carboxypeptidase B downregulates inflammatory responses in autoimmune arthritis. J. Clin. Investig. 2011, 121, 3517–3527. [Google Scholar] [CrossRef]
- Mook-Kanamori, B.B.; Valls Seron, M.; Geldhoff, M.; Havik, S.R.; van der Ende, A.; Baas, F.; van der Poll, T.; Meijers, J.C.; Morgan, B.P.; Brouwer, M.C.; et al. Thrombin-activatable fibrinolysis inhibitor influences disease severity in humans and mice with pneumococcal meningitis. J. Thromb. Haemost. 2015, 13, 2076–2086. [Google Scholar] [CrossRef]
- Jackson, S.P.; Darbousset, R.; Schoenwaelder, S.M. Thromboinflammation: Challenges of therapeutically targeting coagulation and other host defense mechanisms. Blood 2019, 133, 906–918. [Google Scholar] [CrossRef]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef] [PubMed]
- Bernard, G.R.; Vincent, J.L.; Laterre, P.F.; LaRosa, S.P.; Dhainaut, J.F.; Lopez-Rodriguez, A.; Steingrub, J.S.; Garber, G.E.; Helterbrand, J.D.; Ely, E.W.; et al. Efficacy and safety of recombinant human activated protein C for severe sepsis. N. Engl. J. Med. 2001, 344, 699–709. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Ramesh, M.K.; Ernest, D.; LaRosa, S.P.; Pachl, J.; Aikawa, N.; Hoste, E.; Levy, H.; Hirman, J.; Levi, M.; et al. A randomized, double-blind, placebo-controlled, Phase 2b study to evaluate the safety and efficacy of recombinant human soluble thrombomodulin, ART-123, in patients with sepsis and suspected disseminated intravascular coagulation. Crit. Care Med. 2013, 41, 2069–2079. [Google Scholar] [CrossRef] [PubMed]
- Sadjadi, J.; Cureton, E.L.; Twomey, P.; Victorino, G.P. Transfusion, not just injury severity, leads to posttrauma infection: A matched cohort study. Am. Surg. 2009, 75, 307–312. [Google Scholar] [PubMed]
- Claridge, J.A.; Sawyer, R.G.; Schulman, A.M.; McLemore, E.C.; Young, J.S. Blood transfusions correlate with infections in trauma patients in a dose-dependent manner. Am. Surg. 2002, 68, 566–572. [Google Scholar] [PubMed]
- Taylor, R.W.; O’Brien, J.; Trottier, S.J.; Manganaro, L.; Cytron, M.; Lesko, M.F.; Arnzen, K.; Cappadoro, C.; Fu, M.; Plisco, M.S.; et al. Red blood cell transfusions and nosocomial infections in critically ill patients. Crit. Care Med. 2006, 34, 2302–2308, quiz 9. [Google Scholar] [CrossRef]
- Patel, S.V.; Kidane, B.; Klingel, M.; Parry, N. Risks associated with red blood cell transfusion in the trauma population, a meta-analysis. Injury 2014, 45, 1522–1533. [Google Scholar] [CrossRef]
- Jongerius, I.; Porcelijn, L.; van Beek, A.E.; Semple, J.W.; van der Schoot, C.E.; Vlaar, A.P.J.; Kapur, R. The Role of Complement in Transfusion-Related Acute Lung Injury. Trans. Med. Rev. 2019, 33, 236–242. [Google Scholar] [CrossRef]
- Semple, J.W.; Rebetz, J.; Kapur, R. Transfusion-associated circulatory overload and transfusion-related acute lung injury. Blood 2019, 133, 1840–1853. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subjects and Trauma Characteristics | Total (n = 48) | No Sepsis a (n = 34) | Sepsis b (n = 14) | p < 0.05 a vs. b |
|---|---|---|---|---|
| age (years), mean ± sem | 52.23 ± 2.74 | 48.45 ± 3.74 | 56,54 ± 3.68 | ns |
| gender (male, %) | 33 (68.75%) | 22 (64.71%) | 11 (78.57%) | ns |
| trauma mechanism (falls) | 23 (47.92%) | 16 (47.06%) | 7 (50.00%) | ns |
| ISS | 24.95 ± 1.75 | 25.78 ± 2.36 | 23.46 ± 2.79 | ns |
| AIS ≥ 3 (n, %) | ||||
| Head | 22 (45.83%) | 16 (47.06%) | 6 (42.86%) | ns |
| Chest | 16 (33.33%) | 11 (32.35%) | 5 (35.71%) | ns |
| Abdomen | 7 (14.58%) | 4 (11.76%) | 3 (21.43%) | ns |
| Extremity | 10 (20.83%) | 7 (20.59%) | 3 (21.43%) | ns |
| Physiologic Characteristics | Total (n = 48) | No Sepsis a (n = 34) | Sepsis b (n = 14) | p < 0.05 a vs. b |
|---|---|---|---|---|
| SBP < 90 mm Hg (ED, n, %) | 5 (10.42%) | 2 (5.71%) | 3 (21.43%) | ns |
| PRBC transfusion within 24 h (Units) | 4.84 ± 1.18 | 3.81 ± 1.53 | 7.14 ± 2.01 | ns |
| PRBC transfusion total (Units) | 6.98 ± 1.41 | 5.46 ± 21.74 | 10.50 ± 2.50 | <0.05 |
| FFP transfusion within 24 h (Units) | 2.54 ± 0.69 | 1.65 ± 0.71 | 4.31 ± 1.45 | ns |
| FFP transfusion total (Units) | 2.68 ± 0.75 | 1.73 ± 0.75 | 4.43 ± 1.56 | ns |
| INR (ED) | 1.34 ± 0.08 | 1.36 ± 0.11 | 1.31 ± 0.06 | ns |
| PTT (ED, s) | 36.13 ± 2.79 | 37.12 ± 3.88 | 33.72 ± 1.62 | ns |
| PLT count (ED, × 103/μL) | 201.40 ± 10.34 | 198.00 ± 12.44 | 210.30 ± 18.97 | ns |
| Outcome | Total (n = 48) | No Sepsis a (n = 34) | Sepsis b (n = 14) | p < 0.05 a vs. b |
|---|---|---|---|---|
| ICU stay (days) | 11.71 ± 1.82 | 7.00 ± 1.16 | 22.14 ± 4.12 | <0.0001 |
| in-hospital stay (days) | 25.67 ± 3.13 | 19.00 ± 2.90 | 41.07 ± 6.43 | <0.001 |
| in-hospital mortality (n, %) | 6 (12.5%) | 2 (5.88%) | 4 (28.57%) | <0.05 |
| Correlation Analysis | Pearson r | p-Value | Number of Pairs |
|---|---|---|---|
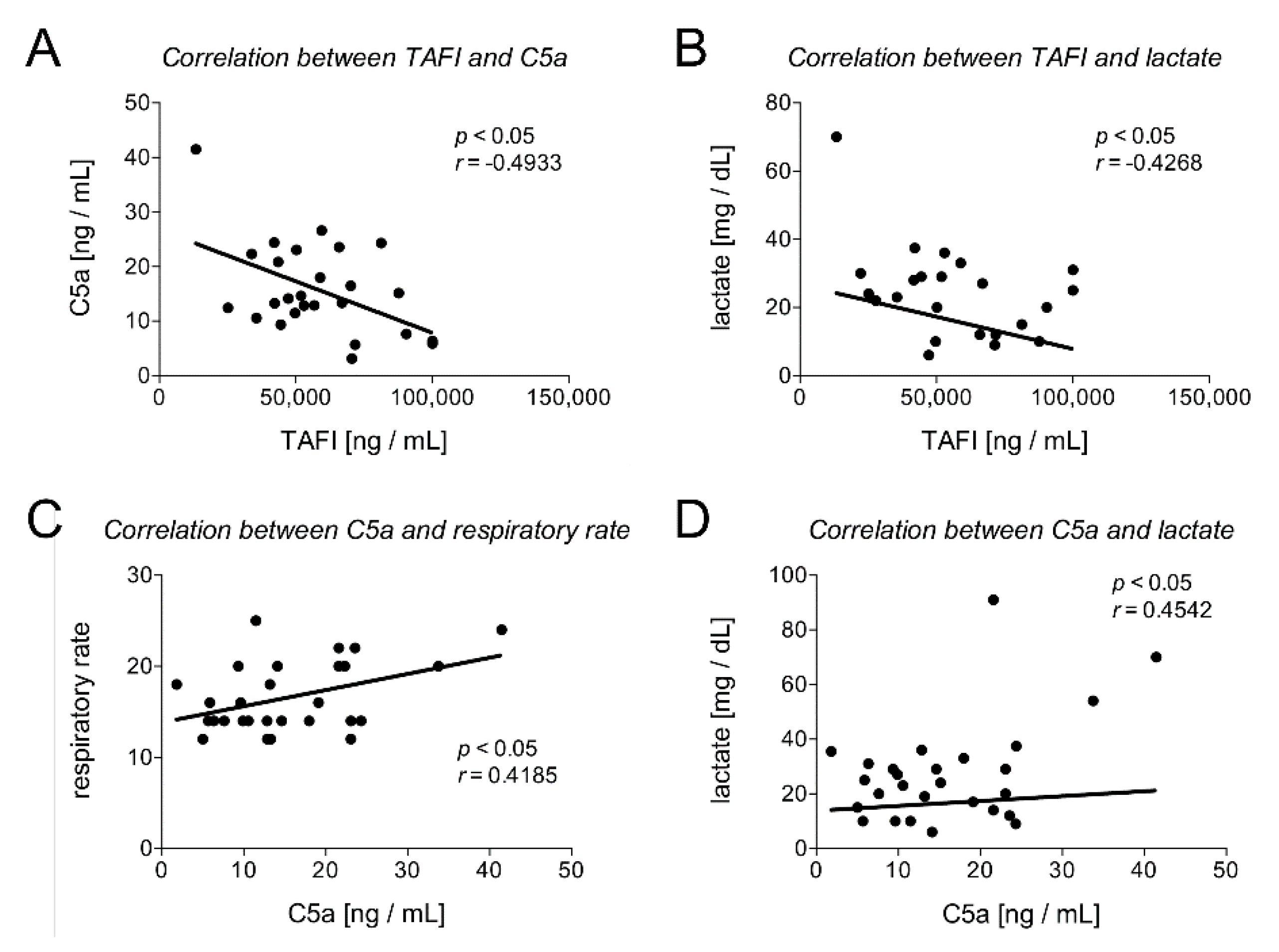
| TAFI and C5a | −0.4933 | 0.0104 | 26 |
| TAFI and leukocytes | −0.2442 | 0.1855 | 31 |
| TAFI and lactate | −0.4268 | 0.0423 | 23 |
| TAFI and pH | 0.2079 | 0.3532 | 22 |
| TAFI and heart rate | −0.2603 | 0.2304 | 23 |
| TAFI and respiratory rate | −0.3685 | 0.0915 | 22 |
| TAFI and SOFA score | −0.3865 | 0.0422 | 28 |
| TAFI and INR | −0.0499 | 0.7860 | 32 |
| TAFI and TPT | 0.0299 | 0.8750 | 30 |
| TAFI and PTT | 0.0369 | 0.8409 | 32 |
| TAFI and PLT | −0.3048 | 0.0085 | 33 |
| C5a and leukocytes | −0.2260 | 0.1918 | 35 |
| C5a and lactate | 0.4542 | 0.0173 | 27 |
| C5a and pH | −0.0805 | 0.6839 | 28 |
| C5a and heart rate | 0.2416 | 0.2068 | 29 |
| C5a and respiratory rate | 0.4185 | 0.0266 | 28 |
| C5a and SOFA score | 0.3795 | 0.0386 | 30 |
| C5a and INR | −0.0199 | 0.9055 | 38 |
| C5a and TPT | −0.2056 | 0.2291 | 36 |
| C5a and PTT | 0.0731 | 0.6629 | 38 |
| C5a and PLT | 0.0138 | 0.9353 | 37 |
| Parameter | Cut-Off Value | Sensitivity % (95% CI) | Specificity % (95% CI) | AUC (95% CI) | p-Value |
|---|---|---|---|---|---|
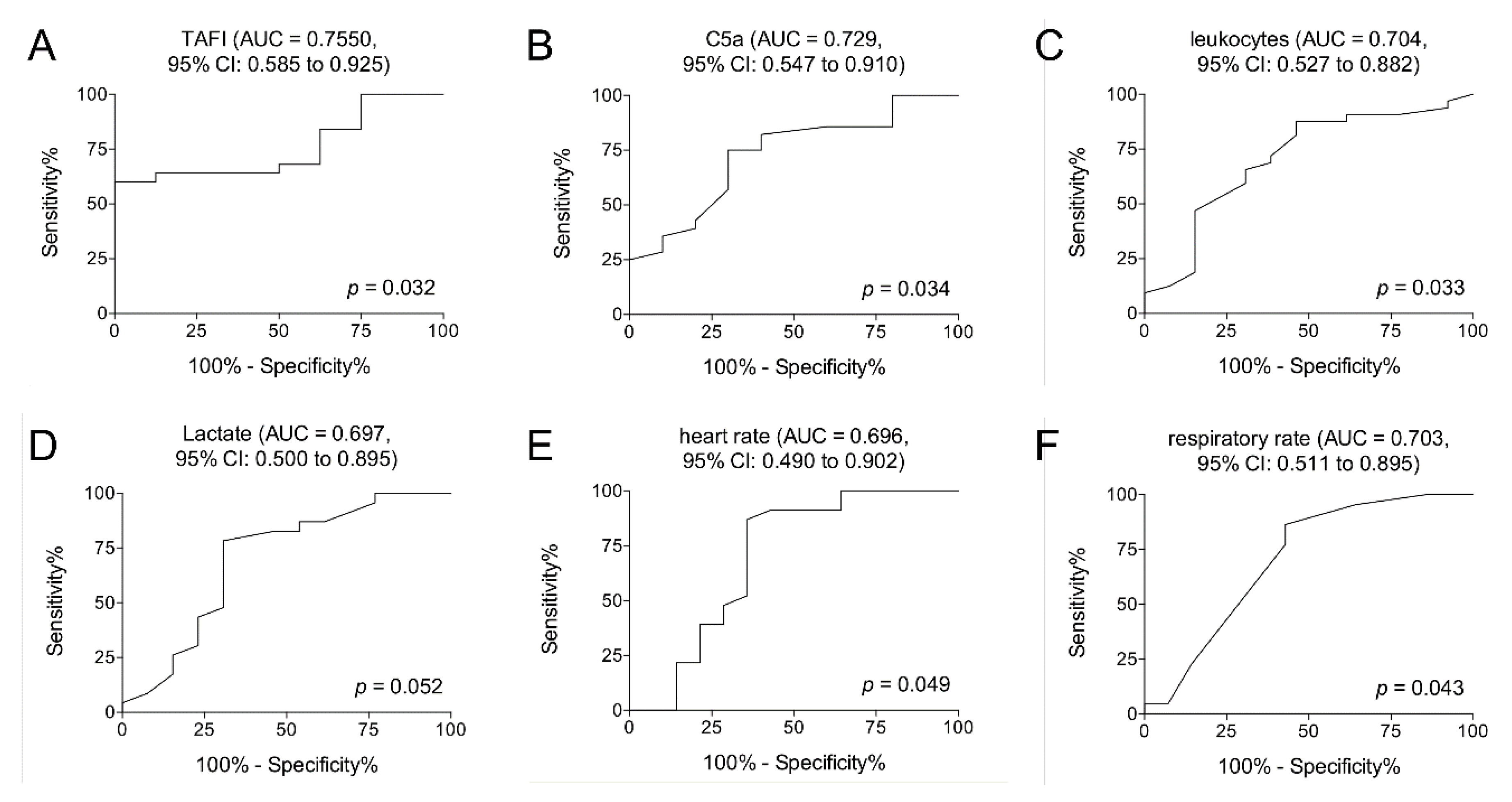
| TAFI [ng/mL] | >54857 | 64.00 (42.52 to 82.03) | 87.50 (47.35 to 99.68) | 0.7550 (0.585 to 0.925) | 0.032 |
| C5a [ng/mL] | <17.00 | 75.00 (55.13 to 89.31) | 70.00 (34.75 to 93.33) | 0.7286 (0.547 to 0.910) | 0.034 |
| leukocytes [U/nL] | <14.50 | 65.63 (46.81 to 81.43) | 69.23 (38.57 to 90.91) | 0.7043 (0.527 to 0.882) | 0.033 |
| lactate [mg/dL] | <28.50 | 78.26 (56.30 to 92.54) | 69.23 (38.57 to 90.91) | 0.6973 (0.500 to 0.895) | 0.052 |
| heart rate | <102.5 | 86.96 (66.41 to 97.22) | 64.29 (35.14 to 87.24) | 0.6957 (0.490 to 0.902) | 0.049 |
| respiratory rate | <15.00 | 63.64 (40.66 to 82.80) | 64.29 (35.14 to 87.24) | 0.7029 (0.511 to 0.895) | 0.043 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vollrath, J.T.; Marzi, I.; Herminghaus, A.; Lustenberger, T.; Relja, B. Post-Traumatic Sepsis Is Associated with Increased C5a and Decreased TAFI Levels. J. Clin. Med. 2020, 9, 1230. https://doi.org/10.3390/jcm9041230
Vollrath JT, Marzi I, Herminghaus A, Lustenberger T, Relja B. Post-Traumatic Sepsis Is Associated with Increased C5a and Decreased TAFI Levels. Journal of Clinical Medicine. 2020; 9(4):1230. https://doi.org/10.3390/jcm9041230
Chicago/Turabian StyleVollrath, Jan Tilmann, Ingo Marzi, Anna Herminghaus, Thomas Lustenberger, and Borna Relja. 2020. "Post-Traumatic Sepsis Is Associated with Increased C5a and Decreased TAFI Levels" Journal of Clinical Medicine 9, no. 4: 1230. https://doi.org/10.3390/jcm9041230
APA StyleVollrath, J. T., Marzi, I., Herminghaus, A., Lustenberger, T., & Relja, B. (2020). Post-Traumatic Sepsis Is Associated with Increased C5a and Decreased TAFI Levels. Journal of Clinical Medicine, 9(4), 1230. https://doi.org/10.3390/jcm9041230