Assessment of Physical Activity Patterns in Adolescent Patients with Anorexia Nervosa and Their Effect on Weight Gain

 , ,
, ,
Abstract
1. Introduction
- Similar to adults, inpatient adolescent AN patients spend more time in light PA than age-matched healthy controls, while moderate PA and vigorous PA will be lower in AN patients.
- Within AN patients, different subgroups exist with respect to PA patterns (i.e., increased light PA or high-level PA defined as moderate PA + vigorous PA), and this PA pattern is an individual trait that remains constant over time, irrespective of therapy.
- More time spent in light PA, but not in high-level PA, on admission is a significant risk factor for lower inpatient weight gain and greater weight loss between discharge and outpatient follow-up.
2. Experimental Section
2.1. Study Populations
2.2. Anthropometry
2.3. Physical Activity Assessment
- Sedentary behavior: ≥ 1.1 to ≤ 1.8 METs
- Light-intensity PA: > 1.8 and < 3 METs
- Moderate-intensity PA: ≥ 3 to < 6 METs
- Vigorous-intensity PA: ≥ 6 METs
2.4. Statistical Analysis
3. Results
3.1. Characterization of the Study Population
3.2. General Parameters and Physical Activity of AN Patients and Healthy Controls
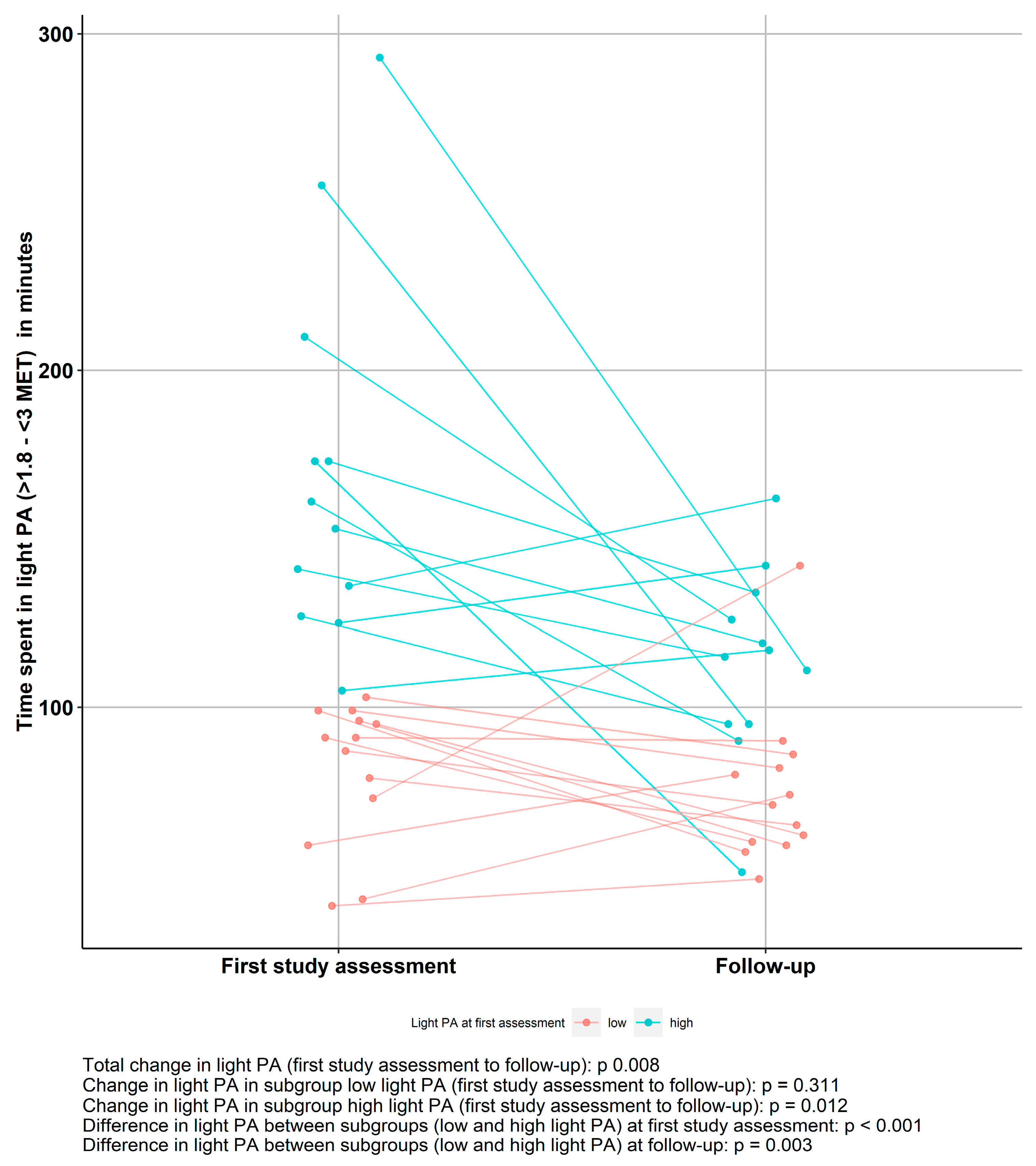
3.3. Light PA in AN Patients Over Time
3.4. Impact of light PA/ High-Level PA at Admission on Weight Trajectory
3.5. Characteristics of Patients Grouped by Low/High Levels of Light PA and Longitudinal Impact of Time Spent in Light PA
4. Discussion
4.1. Comparison of Activity Patterns Between AN Patients and Healthy Controls
4.2. Longitudinal Development of Light PA in AN Patients
4.3. Impact of PA Patterns on Weight Trajectory
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Participant Characteristics and PA | Low Light PA (n = 23) | High Light PA (n = 24) | p-value |
|---|---|---|---|
| Duration of illness, months | 12.0 (7.3/15.8) (3.0–64.0) | 9.0 (4.0/17.6) (1.0–56.0) | 0.176 |
| Admission age, y | 15.82 (14.87/16.64) (13.78–17.85) | 15.11 (13.89/16.70) (12.44–17.82) | 0.250 |
| Admission height, cm | 166.7 ± 6.4 (159.0–183.0) | 164.1 ± 4.3 (156.3–170.0) | 0.253 |
| Admission weight, kg | 43.9 ± 4.1 (39.6–53.0) | 39.8 ± 3.8 (35.3–46.5) | 0.015 |
| Admission BMI, kg/m2 | 15.84 ± 1.73 (13.90–20.40) | 14.80 ± 1.61 (12.80–19.10) | 0.135 |
| Admission BMI percentile (%) | 4.1 ± 11.7 (0.0–43.0) | 1.33 ± 4.31 (0.00–15.00) | 0.443 |
| Steps | 8586 (7136/9735) (2753–24536) | 7870 (6159/12179) (2026–26439) | 0.882 |
| Sedentary behavior (min) (≥1.1 to ≤1.8 METs) | 730 (698/789) (581–856) | 646 (497/715) (189–868) | <0.001 |
| Light PA (min) (>1.8 and <3 METs) | 73.0 (54.3/93.5) (41.0–103.0) | 192 (146/273) (105–530) | <0.001 |
| Moderate PA (min) (≥3 to <6 METs) | 73.0 (46.5/103.5) (22.0–268.0) | 89.5 (39.3/120.8) (3.0–241.0) | 0.663 |
| Vigorous PA (min) (≥6 METs) | 2.0 (1.0/10.0) (0.0–54.0) | 1.5 (0.0/8.9) (0.0–212.0) | 0.729 |
| Time between admission and discharge, days | 95.0 (74.8/118.8) (47.0–225.0) | 121.0 (88.8/135.6) (41.0–171.0) | 0.097 |
| Discharge weight, kg | 51.4 ± 3.3 (45.3–61.1) | 45.0 ± 3.9 (36.6–52.5) | <0.001 |
| Discharge BMI, kg/m2 | 18.38 ± 0.96 (16.50–20.50) | 17.31 ± 1.15 (15.50–19.40) | <0.001 |
| Discharge BMI percentile (%) | 18.4 ± 11.1 (0.0–45.0) | 11.4 ± 8.4 (0.0–36.0) | 0.018 |
| BMI change from first study assessment to discharge kg/m² | 1.85 ± 1.41 (−0.70–4.70) | 2.60 ± 1.36 (−0.10–5.40) | 0.072 |
| BMI percentile change from first study assessment to discharge (%) | 12.0 ± 9.7 (−3.6–33.6) | 18.2 ± 10.0 (−0.5–38.6) | 0.037 |
References
- Association, American Psychiatric. Diagnostic and Statistical Manual of Mental Disorders: Dsm-5; Amer Psychiatric Pub Incorporated: Washington, DC, USA, 2013. [Google Scholar]
- Solenberger, S.E. Exercise and eating disorders: A 3-year inpatient hospital record analysis. Eat. Behav. 2001, 2, 151–168. [Google Scholar] [CrossRef]
- Achamrah, N.; Coeffier, M.; Dechelotte, P. Physical activity in patients with anorexia nervosa. Nutr. Rev. 2016, 74, 301–311. [Google Scholar] [CrossRef] [PubMed]
- Rizk, M.; Lalanne, C.; Berthoz, S.; Kern, L.; Godart, N. Problematic Exercise in Anorexia Nervosa: Testing Potential Risk Factors against Different Definitions. PLoS ONE 2015, 10, e0143352. [Google Scholar] [CrossRef] [PubMed]
- Keyes, A.; Woerwag-Mehta, S.; Bartholdy, S.; Koskina, A.; Middleton, B.; Connan, F.; Webster, P.; Schmidt, U.; Campbell, I.C. Physical activity and the drive to exercise in anorexia nervosa. Int. J. Eat. Disord. 2015, 48, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Alberti, M.; Galvani, C.; Capelli, C.; Lanza, M.; El Ghoch, M.; Calugi, S.; Dalle Grave, R. Physical fitness before and after weight restoration in anorexia nervosa. J. Sports Med. Phys. Fit. 2013, 53, 396–402. [Google Scholar]
- Bratland-Sanda, S.; Sundgot-Borgen, J.; Ro, O.; Rosenvinge, J.H.; Hoffart, A.; Martinsen, E.W. “I’m not physically active - I only go for walks”: Physical activity in patients with longstanding eating disorders. Int. J. Eat. Disord. 2010, 43, 88–92. [Google Scholar] [CrossRef]
- Gianini, L.M.; Klein, D.A.; Call, C.; Walsh, B.T.; Wang, Y.; Wu, P.; Attia, E. Physical activity and post-treatment weight trajectory in anorexia nervosa. Int. J. Eat. Disord. 2016, 49, 482–489. [Google Scholar] [CrossRef]
- Gummer, R.; Giel, K.E.; Schag, K.; Resmark, G.; Junne, F.P.; Becker, S.; Zipfel, S.; Teufel, M. High Levels of Physical Activity in Anorexia Nervosa: A Systematic Review. Eur. Eat. Disord. Rev. 2015, 23, 333–344. [Google Scholar] [CrossRef]
- Hechler, T.; Rieger, E.; Touyz, S.; Beumont, P.; Plasqui, G.; Westerterp, K. Physical activity and body composition in outpatients recovering from anorexia nervosa and healthy controls. Adapt. Phys. Act. Q. 2008, 25, 159–173. [Google Scholar] [CrossRef]
- El Ghoch, M.; Calugi, S.; Pellegrini, M.; Milanese, C.; Busacchi, M.; Battistini, N.C.; Bernabe, J.; Dalle Grave, R. Measured physical activity in anorexia nervosa: Features and treatment outcome. Int. J. Eat. Disord. 2013, 46, 709–712. [Google Scholar] [CrossRef]
- Lehmann, C.S.; Hofmann, T.; Elbelt, U.; Rose, M.; Correll, C.U.; Stengel, A.; Haas, V. The Role of Objectively Measured, Altered Physical Activity Patterns for Body Mass Index Change during Inpatient Treatment in Female Patients with Anorexia Nervosa. J. Clin. Med. 2018, 7, 289. [Google Scholar] [CrossRef] [PubMed]
- Belak, L.; Gianini, L.; Klein, D.A.; Sazonov, E.; Keegan, K.; Neustadt, E.; Walsh, B.T.; Attia, E. Measurement of fidgeting in patients with anorexia nervosa using a novel shoe-based monitor. Eat. Behav. 2017, 24, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Klein, D.A.; Mayer, L.E.; Schebendach, J.E.; Walsh, B.T. Physical activity and cortisol in anorexia nervosa. Psychoneuroendocrinology 2007, 32, 539–547. [Google Scholar] [CrossRef] [PubMed]
- Bratland-Sanda, S.; Sundgot-Borgen, J.; Ro, O.; Rosenvinge, J.H.; Hoffart, A.; Martinsen, E.W. Physical activity and exercise dependence during inpatient treatment of longstanding eating disorders: An exploratory study of excessive and non-excessive exercisers. Int. J. Eat. Disord. 2010, 43, 266–273. [Google Scholar] [CrossRef]
- Kostrzewa, E.; van Elburg, A.A.; Sanders, N.; Sternheim, L.; Adan, R.A.; Kas, M.J. Longitudinal changes in the physical activity of adolescents with anorexia nervosa and their influence on body composition and leptin serum levels after recovery. PLoS ONE 2013, 8, e78251. [Google Scholar] [CrossRef]
- Dellava, J.E.; Hamer, R.M.; Kanodia, A.; Reyes-Rodriguez, M.L.; Bulik, C.M. Diet and physical activity in women recovered from anorexia nervosa: A pilot study. Int. J. Eat. Disord. 2011, 44, 376–382. [Google Scholar] [CrossRef]
- El Ghoch, M.; Calugi, S.; Pellegrini, M.; Chignola, E.; Dalle Grave, R. Physical activity, body weight, and resumption of menses in anorexia nervosa. Psychiatry Res. 2016, 246, 507–511. [Google Scholar] [CrossRef]
- Großer, J.; Hofmann, T.; Stengel, A.; Zeeck, A.; Winter, S.; Correll, C.H. Psychological and Nutritional Correlates of Objectively Assessed Physical Activity in Patients with Anorexia Nervosa, Submitted; German Association for Psychiatry, Psychotherapy and Psychosomatics Congress: Berlin, Germany, 12 January 2018. [Google Scholar]
- Bouten, C.V.; van Marken Lichtenbelt, W.D.; Westerterp, K.R. Body mass index and daily physical activity in anorexia nervosa. Med. Sci. Sports Exerc. 1996, 28, 967–973. [Google Scholar] [CrossRef][Green Version]
- Calabro, M.A.; Lee, J.M.; Saint-Maurice, P.F.; Yoo, H.; Welk, G.J. Validity of physical activity monitors for assessing lower intensity activity in adults. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 119. [Google Scholar] [CrossRef]
- van Hoye, K.; Mortelmans, P.; Lefevre, J. Validation of the SenseWear Pro3 Armband using an incremental exercise test. J Strength Cond. Res. 2014, 28, 2806–2814. [Google Scholar] [CrossRef]
- Johannsen, D.L.; Calabro, M.A.; Stewart, J.; Franke, W.; Rood, J.C.; Welk, G.J. Accuracy of armband monitors for measuring daily energy expenditure in healthy adults. Med. Sci. Sports Exerc. 2010, 42, 2134–2140. [Google Scholar] [CrossRef] [PubMed]
- Stengel, A.; Haas, V.; Elbelt, U.; Correll, C.U.; Rose, M.; Hofmann, T. Leptin and Physical Activity in Adult Patients with Anorexia Nervosa: Failure to Demonstrate a Simple Linear Association. Nutrients 2017, 9, 1210. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R.J.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef]
- Sauchelli, S.; Arcelus, J.; Sanchez, I.; Riesco, N.; Jimenez-Murcia, S.; Granero, R.; Gunnard, K.; Banos, R.; Botella, C.; de la Torre, R.; et al. Physical activity in anorexia nervosa: How relevant is it to therapy response? Eur. Psychiatry J. Assoc. Eur. Psychiatr. 2015, 30, 924–931. [Google Scholar] [CrossRef]
- Casper, R.C. Not the Function of Eating, but Spontaneous Activity and Energy Expenditure, Reflected in “Restlessness” and a “Drive for Activity” Appear to Be Dysregulated in Anorexia Nervosa: Treatment Implications. Front. Psychol. 2018, 9, 2303. [Google Scholar] [CrossRef]
- Garland, T.J.; Schutz, H.; Chappell, M.A.; Keeney, B.K.; Meek, T.H.; Copes, L.E.; Acosta, W.; Drenowatz, C.; Maciel, R.C.; van Dijk, G.; et al. The biological control of voluntary exercise, spontaneous physical activity and daily energy expenditure in relation to obesity: Human and rodent perspectives. J. Exp. Biol. 2011, 214, 206–229. [Google Scholar] [CrossRef]
- Kullmann, S.; Giel, K.E.; Hu, X.; Bischoff, S.C.; Teufel, M.; Thiel, A.; Zipfel, S.; Preissl, H. Impaired inhibitory control in anorexia nervosa elicited by physical activity stimuli. Soc. Cogn. Affect Neurosci. 2014, 9, 917–923. [Google Scholar] [CrossRef]
- Gordon-Larsen, P.; Nelson, M.C.; Popkin, B.M. Longitudinal physical activity and sedentary behavior trends: Adolescence to adulthood. Am. J. Prev. Med. 2004, 27, 277–283. [Google Scholar] [CrossRef]
- Nelson, M.C.; Gordon-Larsen, P.; Adair, L.S.; Popkin, B.M. Adolescent physical activity and sedentary behavior: Patterning and long-term maintenance. Am. J. Prev. Med. 2005, 28, 259–266. [Google Scholar] [CrossRef]
- Chantler, I.; Szabo, C.P.; Green, K. Muscular strength changes in hospitalized anorexic patients after an eight week resistance training program. Int. J. Sports Med. 2006, 27, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Werneck, A.O.; Silva, E.C.A.; Bueno, M.R.O.; Vignadelli, L.Z.; Oyeyemi, A.L.; Romanzini, C.L.P.; Ronque, E.R.V.; Romanzini, M. Association(s) Between Objectively Measured Sedentary Behavior Patterns and Obesity Among Brazilian Adolescents. Pediatric Exerc. Sci. 2019, 31, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Augustin, N.H.; Mattocks, C.; Cooper, A.R.; Ness, A.R.; Faraway, J.J. Modelling fat mass as a function of weekly physical activity profiles measured by actigraph accelerometers. Physiol. Meas. 2012, 33, 1831–1839. [Google Scholar] [CrossRef] [PubMed]
- Machado-Rodrigues, A.M.; Coelho-e-Silva, M.J.; Mota, J.; Padez, C.; Ronque, E.; Cumming, S.P.; Malina, R.M. Cardiorespiratory fitness, weight status and objectively measured sedentary behaviour and physical activity in rural and urban Portuguese adolescents. J. Child Health Care Prof. Work. Child. Hosp. Community 2012, 16, 166–177. [Google Scholar] [CrossRef] [PubMed]
- Allender, S.; Kremer, P.; de Silva-Sanigorski, A.; Lacy, K.; Millar, L.; Mathews, L.; Malakellis, M.; Swinburn, B. Associations between activity-related behaviours and standardized BMI among Australian adolescents. J. Sci. Med. Sport 2011, 14, 512–521. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.A.; Skidmore, P.M.; Stoner, L.; Harrex, H.; Saeedi, P.; Black, K.; Barone Gibbs, B. Associations of accelerometer-measured sedentary time, sedentary bouts, and physical activity with adiposity and fitness in children. J. Sports Sci. 2020, 38, 114–120. [Google Scholar] [CrossRef]
- Altenburg, T.M.; Singh, A.S.; van Mechelen, W.; Brug, J.; Chinapaw, M.J. Direction of the association between body fatness and self-reported screen time in Dutch adolescents. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 4. [Google Scholar] [CrossRef]
- Hands, B.P.; Chivers, P.T.; Parker, H.E.; Beilin, L.; Kendall, G.; Larkin, D. The associations between physical activity, screen time and weight from 6 to 14 yrs: The Raine Study. J. Sci. Med. Sport 2011, 14, 397–403. [Google Scholar] [CrossRef]
- Kantanista, A.; Osinski, W. Underweight in 14 to 16 year-old girls and boys: Prevalence and associations with physical activity and sedentary activities. Ann. Agric. Environ. Med. Aaem 2014, 21, 114–119. [Google Scholar]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R.J.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S504. [Google Scholar] [CrossRef]


| Participant Characteristics and PA | AN Total (n = 47) | Healthy Controls (n = 20) | p-Value |
|---|---|---|---|
| Age, years | 15.70 (14.68/16.64) (12.44–17.85) | 15.02 (13.59/15.84) (12.07–17.86) | 0.139 |
| Height, centimeters | 164.3 ± 6.4 (150.2–183.0) | 165.1 ± 7.1 (153.0–178.0) | 0.672 |
| Weight, kilograms | 42.2 ± 6.0 (31.3–58.2) | 57.3 ± 9.4 (38.8–70.8) | <0.001 |
| BMI, kilogram/meter2 | 15.60 ± 1.78 (12.80–20.40) | 20.96 ± 2.88 (16.00–27.60) | <0.001 |
| BMI, percentile | 4.6 ± 9.9 (0.0–43.0) | 51.8 ± 25.5 (7.0–93.0) | <0.001 |
| Steps | 8430 (6522/10398) (2026–26439) | 11390 (8261/13680) (4427–23139) | 0.048 |
| Sedentary behavior (min) (≥1.1 to ≤1.8 METs) | 705 (624/765) (189–868) | 647 (557/732) (386–853) | 0.118 |
| Light PA (min) (>1.8 and <3 METs) | 105 (73/204) (41–530) | 55 (42/88) (14–303) | <0.001 |
| Moderate PA (min) (≥3 to <6 METs) | 77.0 (44.3/114.2) (3.0–268.0) | 121.5 (82.3/188.2) (25.0–302.0) | 0.009 |
| Vigorous PA (min) (≥6 METs) | 2.0 (0.0/10.2) (0.0–212.0) | 2.0 (0.4/15.8) (0.0–55.0) | 0.697 |
| Participant Characteristics and PA | AN (First Study Assessment) (n = 25) | AN (Follow-Up) (n = 25) | Healthy Controls (n = 20) |
|---|---|---|---|
| Age, years | 16.49 (15.08/17.38) (12.44–17.85) | 16.90 (15.49/17.82) b (12.88–18.20) | 15.02 (13.59/15.84) 2 (12.07–17.86) |
| Height, centimeters | 165.4 ± 5.5 (156.3–183.0) | 164.9 ± 5.1 a (156.6–181.3) | 165.1 ± 7.1 (153.0–178.0) |
| Weight, kilograms | 41.9 ± 4.4 (35.3– 53.0) | 48.3 ± 3.8 b (41.1–56.6) | 57.3 ± 9.4 II 2 (38.8–70.8) |
| BMI, kilogram/meter2 | 15.34 ±1.72 (12.80–20.40) | 17.87 ± 1.56 b (14.50–21.80) | 20.96 ± 2.88 II 2 (16.00–27.60) |
| BMI, percentile | 2.8 ± 8.9 (0.0–43.0) | 13.2 ± 13.7 b (0.0–61.0) | 51.8 ± 25.5 II 2 (7.0–93.0) |
| Steps | 7821 (5948/9296) (2753–23923) | 10475 (8612/14975) a (646–23273) | 11390 (8261/13680) (4427–23139) |
| Sedentary behavior (min) (≥1.1 to ≤ 1.8 METs) | 712 (634/760) (483–868) | 681 (636/747) (499–848) | 647 (557/732) (386–853) |
| Light PA (min) (>1.8 and < 3 METs) | 103.0 (89.7/155.7) (41.0–293.0) | 90.0 (64.0/117.7) a (49.0–162.0) | 55.0 (41.8/88.1) II 2 (14.0–303.0) |
| Moderate PA (min) (≥3 to < 6 METs) | 73.0 (35.7/108.7) (22.0–268.0) | 96.0 (73.0/132.3) (3.0–275.0) | 121.5 (82.3/188.2) (25.0–302.0) |
| Vigorous PA (min) (≥6 METs) | 1.0 (0.0/3.3) (0.0–23.0) | 13.0 (5.0/33.3) b (0.0–116.0) | 2.0 (0.4/15.8) 1 (0.0–55.0) |
| Weight Trajectory in PA Subgroups | Low Light PA (n = 13) | High Light PA (n = 12) | p-value | Low HLPA (n = 14) | High HLPA (n = 11) | p-value |
|---|---|---|---|---|---|---|
| Inpatient BMI percentage change (admission to discharge) | 12.0 ± 9.7 (−3.6–33.6) | 18.2 ± 10.0 (−0.5–38.6) | 0.037 | 21.3 ± 9.7 (7.7–38.6) | 13.43 ± 8.50 (−0.52–25.83) | 0.045 |
| Outpatient BMI percentage change (discharge to follow-up) | 0.80 ± 3.61 (−3.70–9.42) | −2.28 ± 3.63 (−7.59–4.49) | 0.045 | −0.91 ± 3.90 (−6.25–9.42) | −0.38 ± 4.02 (−7.59–5.96) | 0.740 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kemmer, M.; Correll, C.U.; Hofmann, T.; Stengel, A.; Grosser, J.; Haas, V. Assessment of Physical Activity Patterns in Adolescent Patients with Anorexia Nervosa and Their Effect on Weight Gain. J. Clin. Med. 2020, 9, 727. https://doi.org/10.3390/jcm9030727
Kemmer M, Correll CU, Hofmann T, Stengel A, Grosser J, Haas V. Assessment of Physical Activity Patterns in Adolescent Patients with Anorexia Nervosa and Their Effect on Weight Gain. Journal of Clinical Medicine. 2020; 9(3):727. https://doi.org/10.3390/jcm9030727
Chicago/Turabian StyleKemmer, Miriam, Christoph U. Correll, Tobias Hofmann, Andreas Stengel, Julia Grosser, and Verena Haas. 2020. "Assessment of Physical Activity Patterns in Adolescent Patients with Anorexia Nervosa and Their Effect on Weight Gain" Journal of Clinical Medicine 9, no. 3: 727. https://doi.org/10.3390/jcm9030727
APA StyleKemmer, M., Correll, C. U., Hofmann, T., Stengel, A., Grosser, J., & Haas, V. (2020). Assessment of Physical Activity Patterns in Adolescent Patients with Anorexia Nervosa and Their Effect on Weight Gain. Journal of Clinical Medicine, 9(3), 727. https://doi.org/10.3390/jcm9030727