Recurrence Patterns after Surgery in Patients with Different Endometriosis Subtypes: A Long-Term Hospital-Based Cohort Study

Abstract
1. Introduction
2. Materials and Methods
2.1. Surgical Technique
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
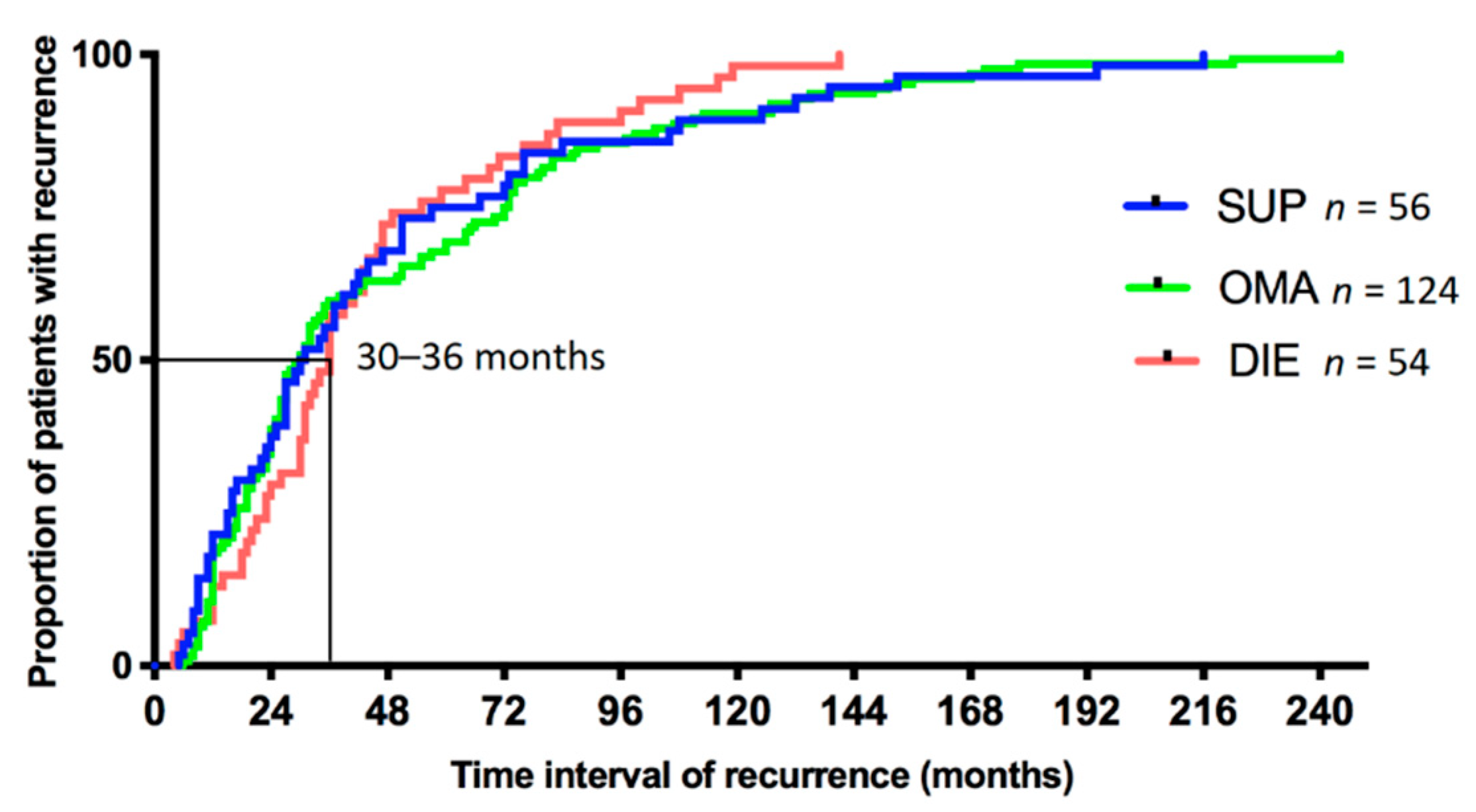
3.2. Time to Recurrence
3.3. Recurrent Endometriosis Subtype, Based on Subtype at First Surgery
3.4. Evolution of Endometriosis Subtypes over Recurrent Surgeries
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Janssen, E.B.; Rijkers, A.C.M.; Hoppenbrouwers, K.; Meuleman, C.; D’Hooghe, T.M. Prevalence of endometriosis diagnosed by laparoscopy in adolescents with dysmenorrhea or chronic pelvic pain: A systematic review. Hum. Reprod. Update 2013, 19, 570–582. [Google Scholar] [CrossRef]
- Gylfason, J.T.; Kristjansson, K.A.; Sverrisdottir, G.; Jonsdottir, K.; Rafnsson, V.; Geirsson, R.T. Pelvic endometriosis diagnosed in an entire nation over 20 years. Am. J. Epidemiol. 2010, 172, 237–243. [Google Scholar] [CrossRef]
- Bougie, O.; Yap, M.; Sikora, L.; Flaxman, T.; Singh, S. Influence of race/ethnicity on prevalence and presentation of endometriosis: A systematic review and meta-analysis. Bjog 2019, 126, 1104–1115. [Google Scholar] [CrossRef]
- Vercellini, P.; Fedele, L.; Aimi, G.; Pietropaolo, G.; Consonni, D.; Crosignani, P.G. Association between endometriosis stage, lesion type, patient characteristics and severity of pelvic pain symptoms: A multivariate analysis of over 1000 patients. Hum. Reprod. 2007, 22, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Simoens, S.; Hummelshoj, L.; Dunselman, G.; Dirksen, C.; Endocost, C.W.; D’Hooghe, T. The burden of endometriosis: Costs and quality of life of women with endometriosis and treated in referral centres. Hum. Reprod. 2012, 27, 1292–1299. [Google Scholar] [CrossRef] [PubMed]
- Duffy, J.M.N.; Arambage, K.; Correa, F.J.S.; Olive, D.; Garry, R.; Barlow, D.H.; Farquhar, C.; Jacobson, T.Z. Laparoscopic surgery for endometriosis. Cochrane Database Syst. Rev. 2014, 3, CD01103. [Google Scholar]
- Cea Soriano, L.; López-Garcia, E.; Schulze-Rath, R.; Garcia Rodríguez, L.A. Incidence, treatment and recurrence of endometriosis in a UK-based population analysis using data from The Health Improvement Network and the Hospital Episode Statistics database. Eur. J. Contracept. Reprod. Health Care 2017, 22, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.W. Recurrence of endometriosis and its control. Hum. Reprod. Update 2009, 15, 441–461. [Google Scholar] [CrossRef] [PubMed]
- Vercellini, P.; Crosignani1, P.G.; Abbiati, A.; Somigliana, E.; Viganò, P.; Fedele, L. The effect of surgery for symptomatic endometriosis: The other side of the story. Hum. Reprod. Update 2009, 15, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Nisolle, M.; Donnez, J. Peritoneal endometriosis, ovarian endometriosis and adenomyotic nodules of the rectovaginal septum are three different entities. Fertil. Steril. 1997, 68, 585–596. [Google Scholar] [CrossRef]
- Cornillie, F.J.; Oosterlynck, D.; Lauweryns, J.M.; Koninckx, P.R. Deeply infiltrating pelvic endometriosis: Histology and clinical significance. Fertil. Steril. 1990, 53, 978–983. [Google Scholar] [CrossRef]
- Vercellini, P.; Trespidi, L.; De, G.O.; Cortesi, I.; Paraxxini, F.; Crosignani, P.G. Endometriosis and pelvic pain: Relation to disease stage and localization. Fertil. Steril. 1996, 65, 299–304. [Google Scholar] [CrossRef]
- Koninckx, P.R.; Lesaffre, E.; Meuleman, C.; Cornillie, F.J.; Demeyere, S. Suggestive evidence that pelvic endometriosis is a progressive disease, whereas deeply infiltrating endometriosis is associated with pelvic pain. Fertil. Steril. 1991, 55, 759–765. [Google Scholar] [CrossRef]
- Chapron, C.; Fauconnier, A.; Dubuisson, J.B.; Barakat, H.; Marco, V.; Bréart, G. Deep infiltrating endometriosis: Relation between severity of dysmenorrhoea and extent of disease. Hum. Reprod. 2003, 18, 760–766. [Google Scholar] [CrossRef]
- Fauconnier, A.; Chapron, C.; Dubuisson, J.B.; Marco, V.; Dousset, B.; Bréart, G. Relation between pain symptoms and the anatomic location of deep infiltrating endometriosis. Fertil. Steril. 2002, 78, 719–726. [Google Scholar] [CrossRef]
- Nirgianakis, K.; Gasparri, L.M.; Radan, A.P.; Villiger, A.; McKinnon, B.; Mosimann, B.; Papadia, A.; Mueller, M.D. Obstetric complications after laparoscopic excision of posterior deep infiltrating endometriosis: A case-control study. Fertil. Steril. 2018, 110, 459–466. [Google Scholar] [CrossRef]
- Brosens, I.; Gordts, S.; Benagiano, G. Endometriosis in adolescents is a hidden, progressive and severe disease that deserves attention, not just compassion. Hum. Reprod. 2013, 28, 2026–2031. [Google Scholar] [CrossRef]
- Evers, J.L.H. Is adolescent endometriosis a progressive disease that needs to be diagnosed and treated? Hum. Reprod. 2013, 28, 2023. [Google Scholar] [CrossRef]
- Unger, C.A.; Laufer, M.R. Progression of endometriosis in non-medically managed adolescents: A case series. J. Pediatr. Adolesc. Gynecol. 2011, 24, e21–e23. [Google Scholar] [CrossRef]
- Audebert, A.; Lecointre, L.; Afors, K.; Koch, A.; Wattiez, A.; Akladios, C. Adolescent Endometriosis: Report of a Series of 55 Cases with a Focus on Clinical Presentation and Long-Term Issues. J. Minim. Invas. Gyn. 2015, 22, 834–840. [Google Scholar] [CrossRef]
- Guo, S.W.; Martin, D.C. The perioperative period: A critical yet neglected time window for reducing the recurrence risk of endometriosis? Hum. Reprod. 2019, 34, 1858–1865. [Google Scholar] [CrossRef] [PubMed]
- Elm, E.V.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Chapron, C.; Lafay-Pillet, M.C.; Monceau, E.; Borghese, B.; Ngô, C.; Souza, C.; Ziegler, D.D. Questioning patients about their adolescent history can identify markers associated with deep infiltrating endometriosis. Fertil. Steril. 2011, 95, 877–881. [Google Scholar] [CrossRef] [PubMed]
- Nirgianakis, K.; McKinnon, B.; Imboden, S.; Knabben, L.; Gloor, B.; Mueller, M.D. Laparoscopic management of bowel endometriosis: Resection margins as a predictor of recurrence. Acta. Obstet. Gyn. Scan. 2014, 93, 1262–1267. [Google Scholar] [CrossRef]
- Liu, X.; Yuan, L.; Shen, F.; Zhu, Z.; Jiang, H.; Guo, S.W. Patterns of and Risk Factors for Recurrence in Women with Ovarian Endometriomas. Obstet. Gynecol. 2007, 109, 1411–1420. [Google Scholar] [CrossRef]
- Harrison, R.F.; Kinsella, B.C. Efficacy of medroxyprogesterone treatment in infertile women with endometriosis: A prospective, randomized, placebo-controlled study. Fertil. Steril. 2000, 74, 24–30. [Google Scholar] [CrossRef]
- Chen, Y.J.; Hsu, T.F.; Huang, B.S.; Tsai, H.W.; Chang, Y.H.; Wang, P.H. Postoperative maintenance levonorgestrel-releasing intrauterine system and endometrioma recurrence: A randomized controlled study. Am. J. Obstet. Gyn. 2017, 216, 582.e1–582.e9. [Google Scholar] [CrossRef]
- Ferrero, S.; Scala, C.; Racca, A.; Calanni, L.; Remorgida, V.; Venturini, P.L.; Maggiore, U.L.R. Second surgery for recurrent unilateral endometriomas and impact on ovarian reserve: A case-control study. Fertil. Steril. 2015, 103, 1236–1243. [Google Scholar] [CrossRef]
- Seracchioli, R.; Mabrouk, M.; Frascà, C.; Manuzzi, L.; Montanari, G.; Keramyda, A.; Venturoli, S. Long-term cyclic and continuous oral contraceptive therapy and endometrioma recurrence: A randomized controlled trial. Fertil. Steril. 2010, 93, 52–56. [Google Scholar] [CrossRef]
- Vercellini, P.; Matteis, S.D.E.; Somigliana, E.; Buggio, L.; Frattaruolo, M.P.; Fedele, L. Long-term adjuvant therapy for the prevention of postoperative endometrioma recurrence: A systematic review and meta-analysis. Acta. Obstet. Gyn. Scan. 2013, 92, 8–16. [Google Scholar] [CrossRef]
- Lee, S.R.; Yi, K.W.; Song, J.Y.; Seo, S.K.; Lee, D.Y.; Cho, S.; Kim, S.H. Efficacy and Safety of Long-Term Use of Dienogest in Women with Ovarian Endometrioma. Reprod. Sci. 2018, 25, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Koga, K.; Takamura, M.; Fujii, T.; Osuga, Y. Prevention of the recurrence of symptom and lesions after conservative surgery for endometriosis. Fertil. Steril. 2015, 104, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Vignali, M.; Bianchi, S.; Candiani, M.; Spadaccini, G.; Oggioni, G.; Busacca, M. Surgical treatment of deep endometriosis and risk of recurrence. J. Minim. Invas. Gyn. 2005, 12, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Exacoustos, C.; Zupi, E.; Amadio, A.; Amoroso, C.; Szabolcs, B.; Romanini, M.E.; Arduini, D. Recurrence of endometriomas after laparoscopic removal: Sonographic and clinical follow-up and indication for second surgery. J. Minim. Invas. Gyn. 2006, 13, 281–288. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| First Surgery | SUP | OMA | DIE | Unknown | p | |
|---|---|---|---|---|---|---|
| Characteristics | (n = 56) | (n = 124) | (n = 54) | (n = 88) | ||
| Age (y ± SD) | 27.7 ± 6.4 | 29.4 ± 5.3 | 30.1 ± 5.0 | 29.4 ± 6.6 | ns | |
| Median time to second surgery (min-max, months) | 30.5 (5–216) | 30 (6–244) | 36 (4–141) | 33.5 (5–190) | ns | |
| First surgery in external hospital | 43 (76.8%) | 109 (87.9%) | 33 (61.1%) | 85 (96.6%) | <0.001 * | |
| Second surgery in external hospital | 12 (21.4%) | 40 (32.3%) | 12 (22.2%) | 33 (37.5%) | ns | |
| One recurrence | 100% | 100% | 100% | 100% | n/a | |
| Two recurrences | 18 (32.1%) | 52 (41.9%) | 18 (33.3%) | 44 (50.0%) | ns | |
| Three recurrences | 4 (7.1%) | 16 (12.9%) | 8 (14.8%) | 22 (25.0%) | ns | |
| Four recurrences | 2 (3.6%) | 4 (3.2%) | 4 (7.4%) | 13 (14.8%) | ns | |
| Five recurrences | 0 | 0 | 1 (1.9%) | 3 (3.4%) | ns | |
| First Surgery | SUP (N = 56) Median Time to Recurrence (Min–Max) | p OR (95% CI) 1 | OMA (N = 124) Median Time to Recurrence (Min–Max) | p OR (95% CI) 2 | DIE (N = 54) Median Time to Recurrence (Min–Max) | p OR (95% CI) 3 | |
|---|---|---|---|---|---|---|---|
| Recurrent Surgery | |||||||
| SUP | 17 (30.4%) | 0.001 | 10 (8.1%) | 0.0011 | 9 (16.7%) | ns | |
| 30 (9–194) | 3.65 | 28 (7–244) | 0.28 | 31 (5–116) | |||
| (1.74, 7.51) | (0.14, 0.62) | ||||||
| OMA | 10 (17.9%) 71.5 (6–216) | 0.0036 0.34 (0.17, 0.73) | 58 (46.8%) 27 (6–222) | <0.0001 3.72 (2.04, 6.74) | 11 (20.4%) 36 (6–141) | 0.021 0.42 (0.2, 0.87) | |
| DIE | 27 (48.2%) | ns | 49 (39.5%) | ns | 29 (53.7%) | ns | |
| 27 (5–139) | 51 (8–135) | 39 (18–119) | |||||
| Unknown subtype | 2 (3.6%) | ns | 5 (4.0%) | ns | 5 (9.3%) | ns | |
| 31.5 (12.51) | 30 (12–156) | 24 (4–31) | |||||
| (a) | |||||||||
| Location of OMA at 1st Surgery | Bilateral n = 13 (22.4%) | Unilateral Left n = 21 (36.2%) | Unilateral Right n = 14 (24.1%) | Unknown n = 10 (17.2%) | |||||
| Location of OMA at 2nd Surgery | |||||||||
| Bilateral | 6 (46.2%) | 9 (42.9%) | 4 (28.6%) | 4 (40.0%) | |||||
| Unilateral left | 3 (23.1%) | 8 (38.1%) | 3 (21.4%) | 1 (10.0%) | |||||
| Unilateral right | 4 (30.8%) | 4 (19.0%) | 7 (50.0%) | 3 (30.0%) | |||||
| Unknown | 0 (0%) | 0 (0%) | 0 (0%) | 2 (20.0%) | |||||
| (b) | |||||||||
| First Surgery | DIE | SUP n = 27 | OMA n = 49 | ||||||
| Uterosacral Ligament n = 3/29 | Vagina n = 11/29 | Intestine n = 10/29 | Bladder n = 1/29 | Others * n = 4/29 | |||||
| DIE Location at Second Surgery | |||||||||
| Uterosacral ligament | 0 | 1 (3.4%) | 1 (3.4%) | 1 (3.4%) | 1 (3.4%) | 7 (25.9%) | 9 (18.4%) | ||
| Vagina | 0 | 8 (27.6%) | 5 (17.2%) | 0 | 0 | 10 (37.0%) | 23 (46.9%) | ||
| Intestine | 1 (3.4%) | 4 (13.8%) | 4 (13.8%) | 0 | 2 (6.9%) | 12 (44.4%) | 15 (30.6%) | ||
| Bladder | 0 | 0 | 0 | 0 | 0 | 2 (7.4%) | 3 (6.1%) | ||
| Others * | 2 (6.9%) | 1 (3.4%) | 1 (3.4%) | 0 | 1 (3.4%) | 1 (3.7%) | 5 (10.2%) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nirgianakis, K.; Ma, L.; McKinnon, B.; Mueller, M.D. Recurrence Patterns after Surgery in Patients with Different Endometriosis Subtypes: A Long-Term Hospital-Based Cohort Study. J. Clin. Med. 2020, 9, 496. https://doi.org/10.3390/jcm9020496
Nirgianakis K, Ma L, McKinnon B, Mueller MD. Recurrence Patterns after Surgery in Patients with Different Endometriosis Subtypes: A Long-Term Hospital-Based Cohort Study. Journal of Clinical Medicine. 2020; 9(2):496. https://doi.org/10.3390/jcm9020496
Chicago/Turabian StyleNirgianakis, Konstantinos, Lijuan Ma, Brett McKinnon, and Michael D. Mueller. 2020. "Recurrence Patterns after Surgery in Patients with Different Endometriosis Subtypes: A Long-Term Hospital-Based Cohort Study" Journal of Clinical Medicine 9, no. 2: 496. https://doi.org/10.3390/jcm9020496
APA StyleNirgianakis, K., Ma, L., McKinnon, B., & Mueller, M. D. (2020). Recurrence Patterns after Surgery in Patients with Different Endometriosis Subtypes: A Long-Term Hospital-Based Cohort Study. Journal of Clinical Medicine, 9(2), 496. https://doi.org/10.3390/jcm9020496