Lidocaine vs. Other Local Anesthetics in the Development of Transient Neurologic Symptoms (TNS) Following Spinal Anesthesia: A Meta-Analysis of Randomized Controlled Trials


Abstract
1. Introduction
2. Materials and Methods
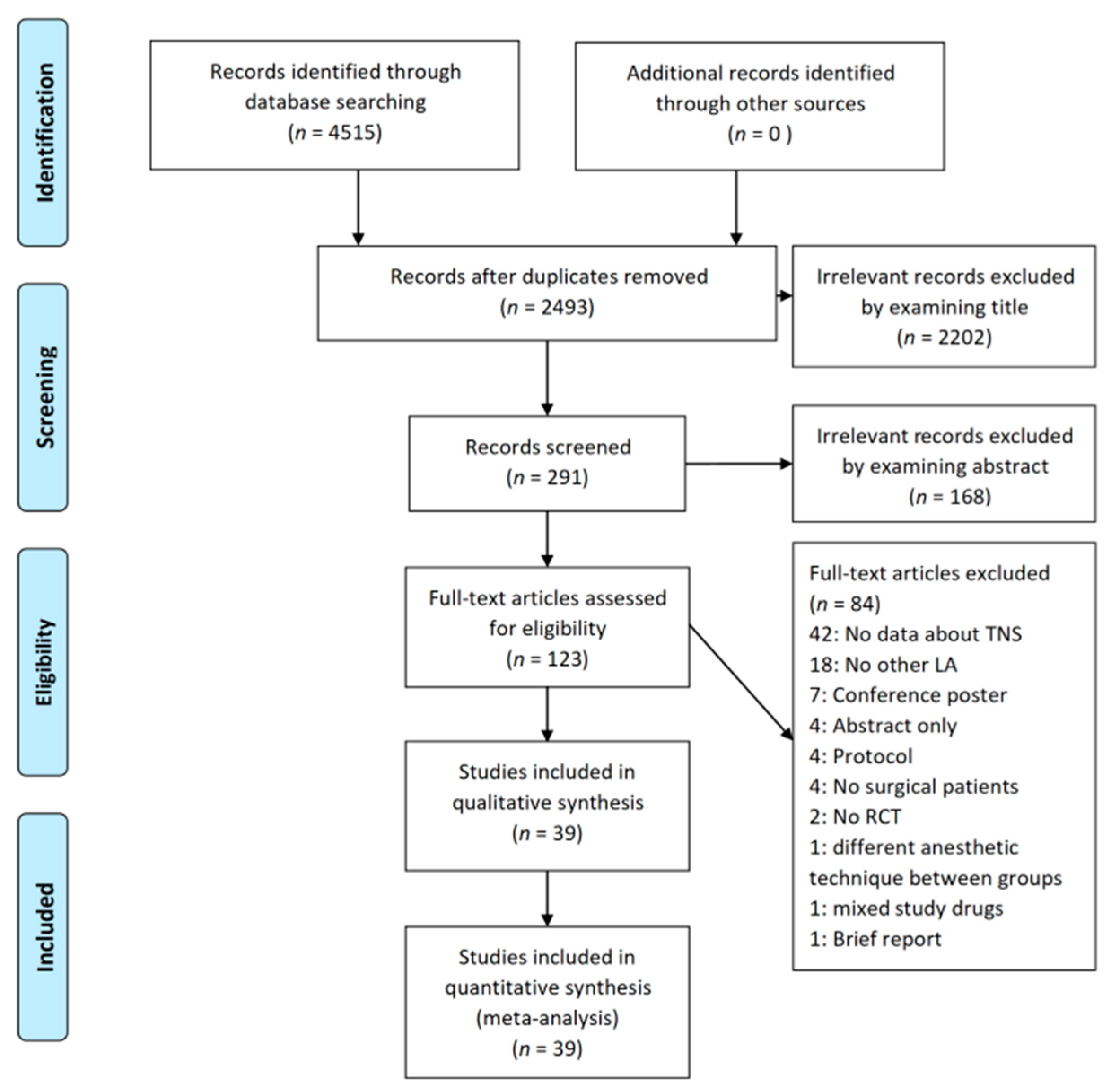
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
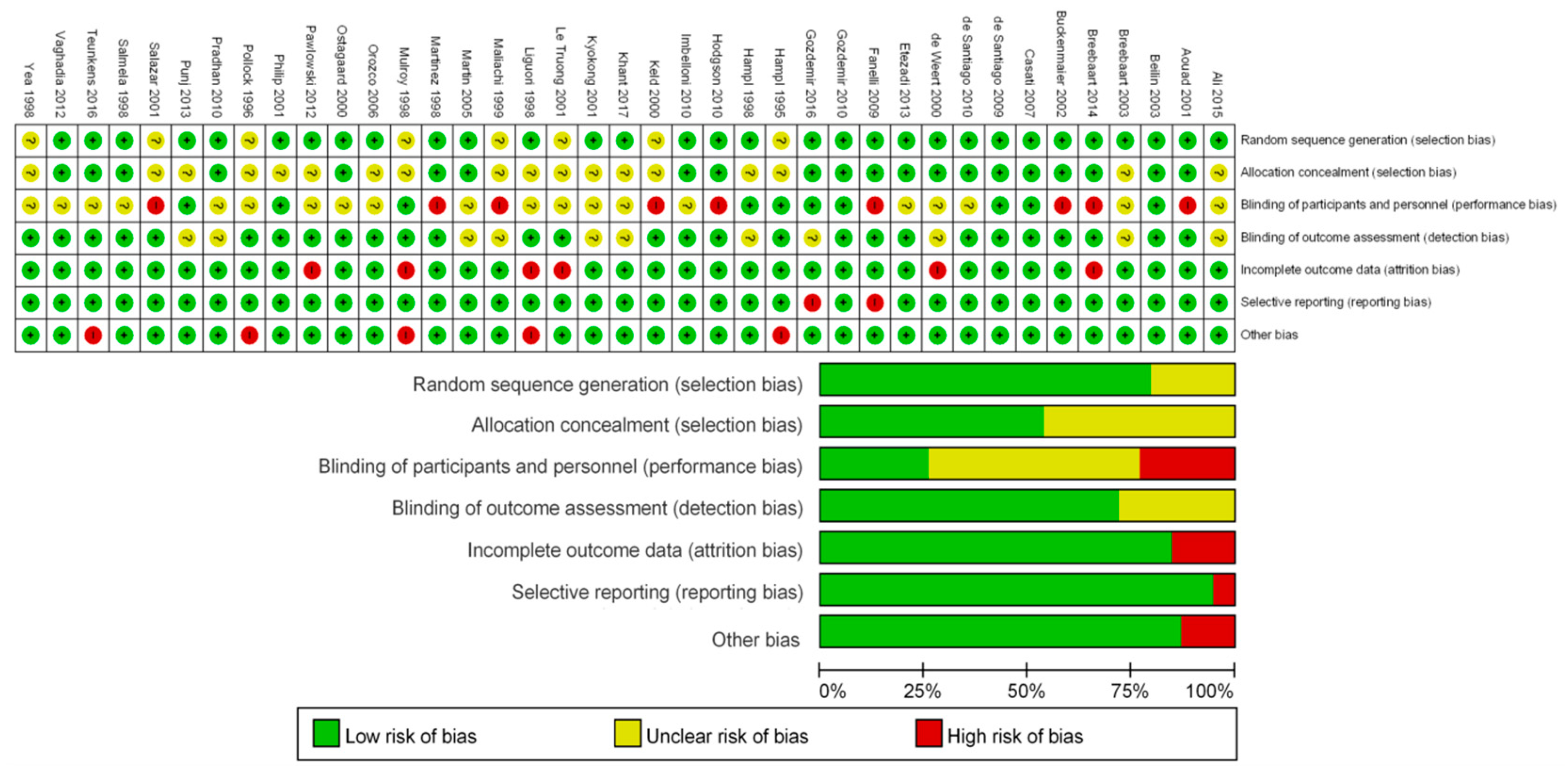
2.4. Risk of Bias Assessment
2.5. Data Synthesis and Statistical Analysis
3. Results
3.1. Descriptions of Trials
3.2. Methodology Quality and Risk of Bias
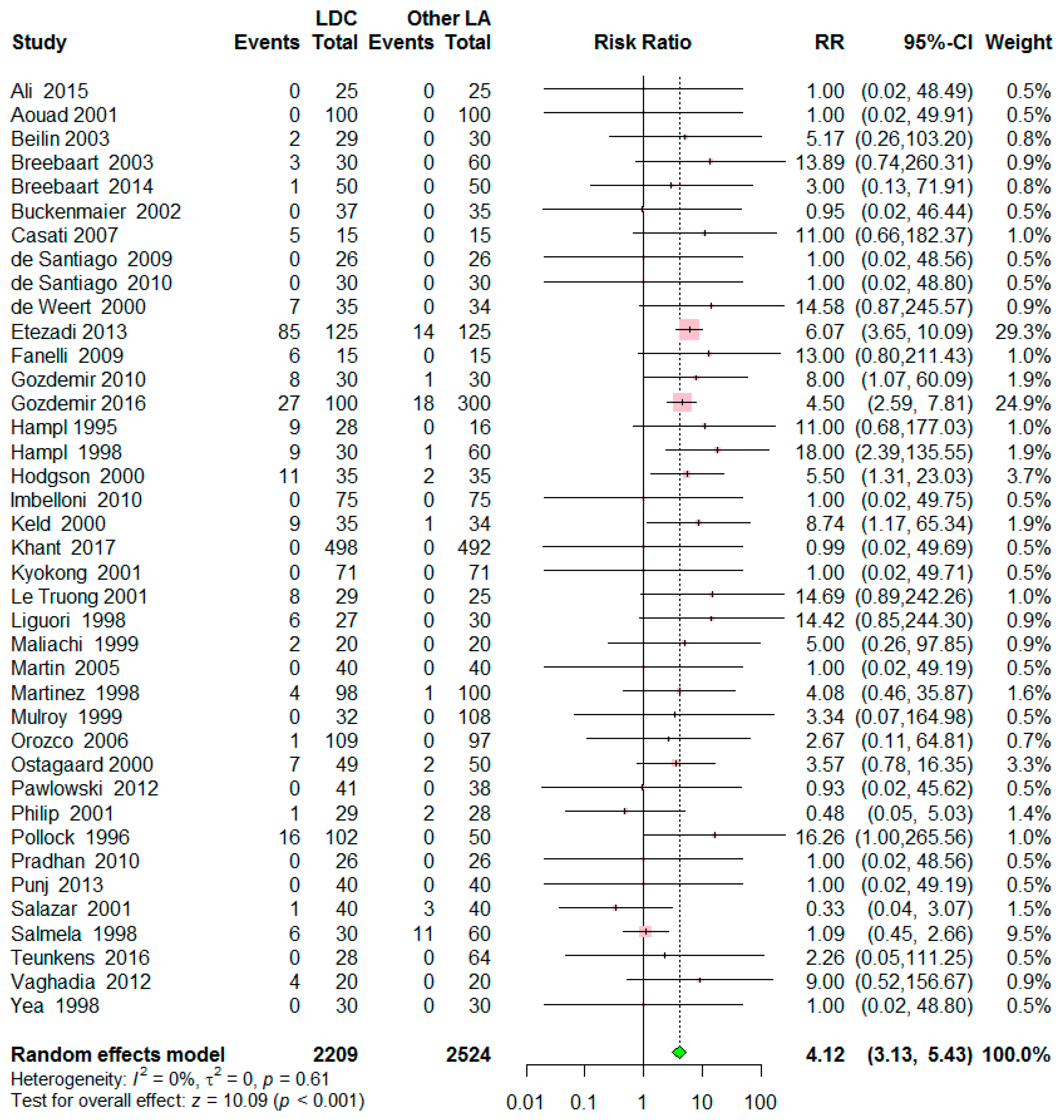
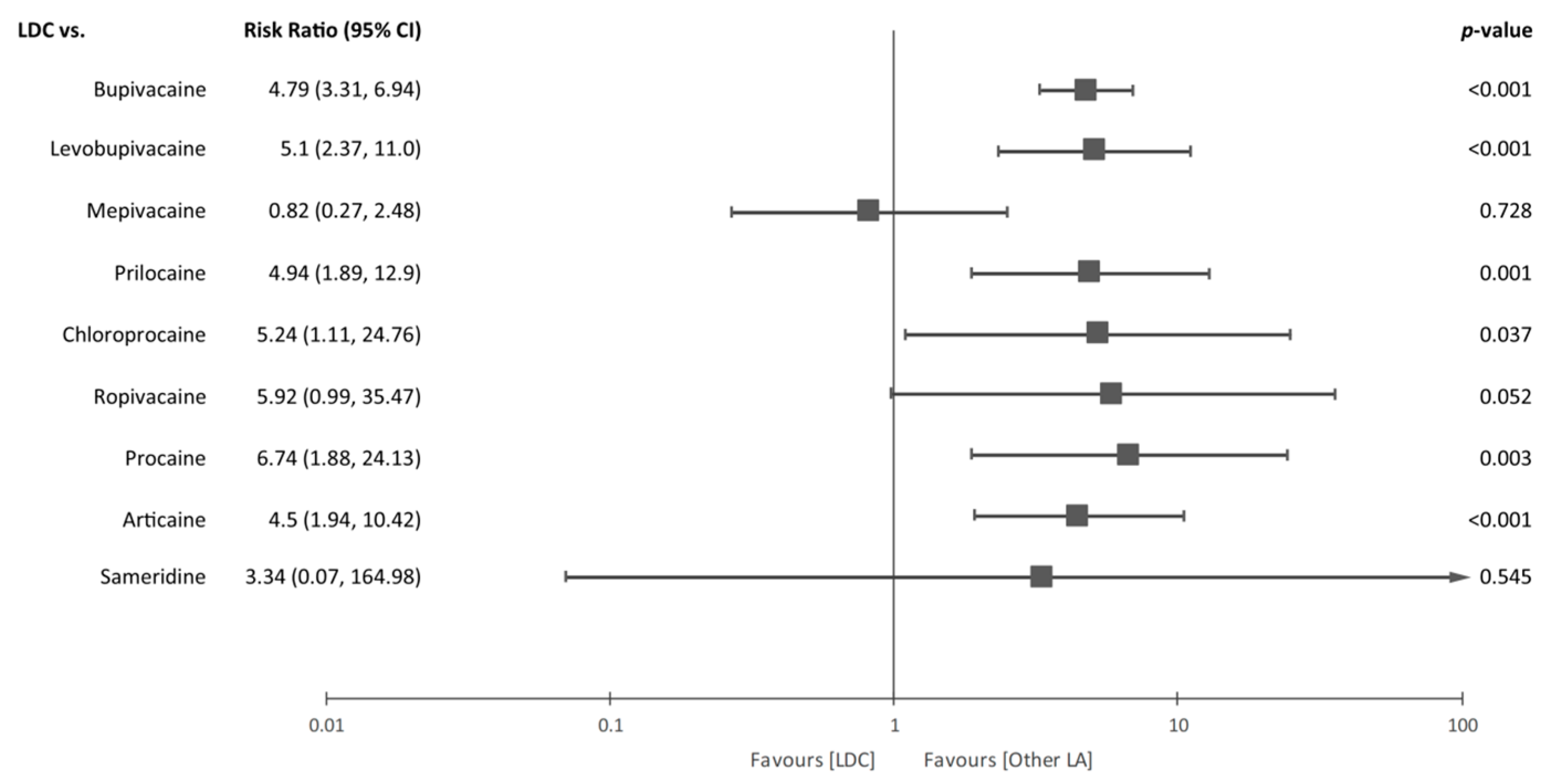
3.3. Outcome Synthesis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Liam, B.L.; Yim, C.F.; Chong, J.L. Dose response study of lidocaine 1% for spinal anaesthesia for lower limb and perineal surgery. Can. J. Anaesth. 1998, 45, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Zaric, D.; Pace, N.L. Transient neurologic symptoms (TNS) following spinal anaesthesia with lidocaine versus other local anaesthetics. Cochrane Database Syst. Rev. 2009, 15, CD003006. [Google Scholar] [CrossRef] [PubMed]
- Forget, P.; Borovac, J.A.; Thackeray, E.M.; Pace, N.L. Transient neurological symptoms (TNS) following spinal anaesthesia with lidocaine versus other local anaesthetics in adult surgical patients: A network meta-analysis. Cochrane Database Syst. Rev. 2019, 12, CD003006. [Google Scholar] [CrossRef]
- Ali Hassan, H.I. Comparison between two different selective spinal anesthesia techniques in ambulatory knee arthroscopy as fast-track anesthesia. Anesth. Essays Res. 2015, 9, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Aouad, M.T.; Siddik, S.S.; Jalbout, M.I.; Baraka, A.S. Does pregnancy protect against intrathecal lidocaine-induced transient neurologic symptoms? Anesth. Analg. 2001, 92, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Buckenmaier, C.C., 3rd; Nielsen, K.C.; Pietrobon, R.; Klein, S.M.; Martin, A.H.; Greengrass, R.A.; Steele, S.M. Small-dose intrathecal lidocaine versus ropivacaine for anorectal surgery in an ambulatory setting. Anesth. Analg. 2002, 95, 1253–1257. [Google Scholar] [CrossRef]
- de Santiago, J.; Santos-Yglesias, J.; Giron, J.; de Oca, F.M.; Jimenez, A.; Diaz, P. Low-Dose 3 mg Levobupivacaine Plus 10 microg Fentanyl Selective Spinal Anesthesia for Gynecological Outpatient Laparoscopy. Anesth. Analg. 2009, 109, 1456–1461. [Google Scholar] [CrossRef] [PubMed]
- de Santiago, J.; Santos-Yglesias, J.; Giron, J.; Jiménez, A.; Errando, C.L. Low-dose hypobaric spinal anesthesia for anorectal surgery in jackknife position: Levobupivacaine-fentanyl compared to lidocaine-fentanyl. Rev. Espaola Anestesiol. Reanim. 2010, 57, 565–570. [Google Scholar] [CrossRef]
- Imbelloni, L.E.; Gouveia, M.A.; Cordeiro, J.A. Hypobaric 0.15% bupivacaine versus hypobaric 0.6% lidocaine for posterior spinal anesthesia in outpatient anorectal surgery. Braz. J. Anestesiol. 2010, 60, 113–120. [Google Scholar] [CrossRef][Green Version]
- Khant, S.R.; Chaudhari, R.; Kore, R.A.; Bhagwat, S.; Jakhalekar, R.P. Low dose lignocaine + butorphanol vs. low dose bupivacaine for spinal anaesthesia in day care urological surgeries: A prospective randomized control trial. Turk. J. Urol. 2017, 43, 189–195. [Google Scholar] [CrossRef][Green Version]
- Kyokong, O.; Charuluxananan, S.; Pothimamaka, S.; Leerapun, R. Hypotension in spinal anesthesia for cesarean section: A comparison of 0.5% hyperbaric bupivacaine and 5% hyperbaric lidocaine. J. Med. Assoc. Thai 2001, 84 (Suppl. 1), S256–S262. [Google Scholar]
- Martin, M.A.; Olle, G.; Oferil, F.; Opisso, L.l.; Serra-Prat, M.; Hidalgo, L. Recovery time and patient satisfaction in ambulatory knee arthroscopy: Prospective study comparing three anaesthetic methods. Ambul. Surg. 2005, 12, 75–79. [Google Scholar] [CrossRef]
- Mulroy, M.F.; Greengrass, R.; Ganapathy, S.; Chan, V.; Heierson, A. Sameridine is safe and effective for spinal anesthesia: A comparative dose-ranging study with lidocaine for inguinal hernia repair. Anesth. Analg. 1999, 88, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Pawlowski, J.; Orr, K.; Kim, K.M.; Pappas, A.L.; Sukhani, R.; Jellish, W.S. Anesthetic and recovery profiles of lidocaine versus mepivacaine for spinal anesthesia in patients undergoing outpatient orthopedic arthroscopic procedures. J. Clin. Anesth. 2012, 24, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, B. Spinal anesthesia for cesarean section: Comparison of 5.0% lignocaine and 0.5% bupivacaine. Nepal Med. Coll. J. 2010, 12, 30–33. [Google Scholar] [PubMed]
- Punj, J.; Khan, R.M. Spinal anaesthesia for pelvic surgery: Low concentrations of lignocaine and bupivacaine are effective with less adverse events. Middle E. J. Anaesthesiol. 2013, 22, 71–77. [Google Scholar]
- Teunkens, A.; Vermeulen, K.; Van Gerven, E.; Fieuws, S.; Van de Velde, M.; Rex, S. Comparison of 2-Chloroprocaine, Bupivacaine, and Lidocaine for Spinal Anesthesia in Patients Undergoing Knee Arthroscopy in an Outpatient Setting: A Double-Blind Randomized Controlled Trial. Reg. Anesth. Pain Med. 2016, 41, 576–583. [Google Scholar] [CrossRef]
- Yea, K.H.; Lee, S.C.; Kim, J.S.; Chung, C.J. Spinal Anesthesia with Hyperbaric 1.5% Lidocaine and 1.5% Mepivacaine. Korean J. Anesthesiol. 1998, 35, 1095–1099. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Friedrich, J.O.; Adhikari, N.K.; Beyene, J. Inclusion of zero total event trials in meta-analyses maintains analytic consistency and incorporates all available data. BMC Med. Res. Methodol. 2007, 7, 5. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Intervetions Version 5.1.0; The Cochrane Collaboration: Chichester, UK, 2011. [Google Scholar]
- Beilin, Y.; Zahn, J.; Abramovitz, S.; Bernstein, H.H.; Hossain, S.; Bodian, C. Subarachnoid small-dose bupivacaine versus lidocaine for cervical cerclage. Anesth. Analg. 2003, 97, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Breebaart, M.B.; Teune, A.; Sermeus, L.A.; Vercauteren, M.P. Intrathecal chloroprocaine vs. lidocaine in day-case surgery: Recovery, discharge and effect of pre-hydration on micturition. Acta Anaesthesiol. Scand. 2014, 58, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Breebaart, M.B.; Vercauteren, M.P.; Hoffmann, V.L.; Adriaensen, H.A. Urinary bladder scanning after day-case arthroscopy under spinal anaesthesia: Comparison between lidocaine, ropivacaine, and levobupivacaine. Br. J. Anaesth. 2003, 90, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Casati, A.; Fanelli, G.; Danelli, G.; Berti, M.; Ghisi, D.; Brivio, M.; Putzu, M.; Barbagallo, A. Spinal anesthesia with lidocaine or preservative-free 2-chlorprocaine for outpatient knee arthroscopy: A prospective, randomized, double-blind comparison. Anesth. Analg. 2007, 104, 959–964. [Google Scholar] [CrossRef] [PubMed]
- de Weert, K.; Traksel, M.; Gielen, M.; Slappendel, R.; Weber, E.; Dirksen, R. The incidence of transient neurological symptoms after spinal anaesthesia with lidocaine compared to prilocaine. Anaesthesia 2000, 55, 1020–1024. [Google Scholar] [CrossRef] [PubMed]
- Etezadi, F.; Karimi Yarandi, K.; Ahangary, A.; Shokri, H.; Imani, F.; Safari, S.; Khajavi, M.R. The effect of needle type, duration of surgery and position of the patient on the risk of transient neurologic symptoms. Anesth. Pain Med. 2013, 2, 154–158. [Google Scholar] [CrossRef]
- Fanelli, G.; Danelli, G.; Zasa, M.; Baciarello, M.; Di Cianni, S.; Leone, S. Intrathecal ropivacaine 5 mg/ml for outpatient knee arthroscopy: A comparison with lidocaine 10 mg/ml. Acta Anaesthesiol. Scand. 2009, 53, 109–115. [Google Scholar] [CrossRef]
- Gozdemir, M.; Muslu, B.; Sert, H.; Usta, B.; Demircioglu, R.I.; Karatas, O.F.; Surgit, O. Transient neurological symptoms after spinal anaesthesia with levobupivacaine 5 mg/ml or lidocaine 20 mg/ml. Acta Anaesthesiol. Scand. 2010, 54, 59–64. [Google Scholar] [CrossRef]
- Gozdemir, M.; Muslu, B.; Sert, H.; Usta, B.; Demircioglu, R.I.; Kasikara, H. Transient neurological symptoms after spinal anesthesia. Clin. Invest. Med. 2016, 39, 27512. [Google Scholar] [CrossRef]
- Hampl, K.F.; Heinzmann-Wiedmer, S.; Luginbuehl, I.; Harms, C.; Seeberger, M.; Schneider, M.C.; Drasner, K. Transient neurologic symptoms after spinal anesthesia: A lower incidence with prilocaine and bupivacaine than with lidocaine. Anesthesiology 1998, 88, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Hampl, K.F.; Schneider, M.C.; Thorin, D.; Ummenhofer, W.; Drewe, J. Hyperosmolarity does not contribute to transient radicular irritation after spinal anesthesia with hyperbaric 5% lidocaine. Reg. Anesth. 1995, 20, 363–368. [Google Scholar]
- Hodgson, P.S.; Liu, S.S.; Batra, M.S.; Gras, T.W.; Pollock, J.E.; Neal, J.M. Procaine compared with lidocaine for incidence of transient neurologic symptoms. Reg. Anesth. Pain Med. 2000, 25, 218–222. [Google Scholar] [PubMed]
- Keld, D.B.; Hein, L.; Dalgaard, M.; Krogh, L.; Rodt, S.A. The incidence of transient neurologic symptoms (TNS) after spinal anaesthesia in patients undergoing surgery in the supine position. Hyperbaric lidocaine 5% versus hyperbaric bupivacaine 0.5%. Acta Anaesthesiol. Scand. 2000, 44, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Le Truong, H.H.; Girard, M.; Drolet, P.; Grenier, Y.; Boucher, C.; Bergeron, L. Spinal anesthesia: A comparison of procaine and lidocaine. Can. J. Anaesth. 2001, 48, 470–473. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Liguori, G.A.; Zayas, V.M.; Chisholm, M.F. Transient neurologic symptoms after spinal anesthesia with mepivacaine and lidocaine. Anesthesiology 1998, 88, 619–623. [Google Scholar] [CrossRef] [PubMed]
- Maliachi Revuelta, R.; Calzada Grijalva, J.F.; Gonzalez, A.; Dosta Herrera, J.J.; Flores Lopez, D. Syndrome of transient radicular irritation secondary to spinal blockade in pelvis traumatologic surgery. Anest. Mex. 1999, 11, 109–114. [Google Scholar]
- Martínez-Bourio, R.; Arzuaga, M.; Quintana, J.M.; Aguilera, L.; Aguirre, J.; Saez-Eguilaz, J.L.; Arizaga, A. Incidence of transient neurologic symptoms after hyperbaric subarachnoid anesthesia with 5% lidocaine and 5% prilocaine. Anesthesiology 1998, 88, 624–628. [Google Scholar] [CrossRef]
- Orozco, E.G.; Arguelles, R.A.F.; Ortega, A.D.; Bastanzuri, M.C.L. Cost-effectiveness evaluation of 5% lidocaine and 0,5% bupivacaine in spinal anesthesia. Rev. Cubana Farm. 2006, 40. [Google Scholar]
- Østgaard, G.; Hallaråker, O.; Ulveseth, O.K.; Flaatten, H. A randomised study of lidocaine and prilocaine for spinal anaesthesia. Acta Anaesthesiol. Scand. 2000, 44, 436–440. [Google Scholar] [CrossRef]
- Philip, J.; Sharma, S.K.; Gottumukkala, V.N.; Perez, B.J.; Slaymaker, E.A.; Wiley, J. Transient neurologic symptoms after spinal anesthesia with lidocaine in obstetric patients. Anesth. Analg. 2001, 92, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Pollock, J.E.; Neal, J.M.; Stephenson, C.A.; Wiley, C.E. Prospective study of the incidence of transient radicular irritation in patients undergoing spinal anesthesia. Anesthesiology 1996, 84, 1361–1367. [Google Scholar] [CrossRef] [PubMed]
- Salazar, F.; Bogdanovich, A.; Adalia, R.; Chabás, E.; Gomar, C. Transient neurologic symptoms after spinal anaesthesia using isobaric 2% mepivacaine and isobaric 2% lidocaine. Acta Anaesthesiol. Scand. 2001, 45, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Salmela, L.; Aromaa, U. Transient radicular irritation after spinal anesthesia induced with hyperbaric solutions of cerebrospinal fluid-diluted lidocaine 50 mg/ml or mepivacaine 40 mg/ml or bupivacaine 5 mg/ml. Acta Anaesthesiol. Scand. 1998, 42, 765–769. [Google Scholar] [CrossRef]
- Vaghadia, H.; Neilson, G.; Lennox, P.H. Selective spinal anesthesia for outpatient transurethral prostatectomy (TURP): Randomized controlled comparison of chloroprocaine with lidocaine. Acta Anaesthesiol. Scand. 2012, 56, 217–223. [Google Scholar] [CrossRef]
- Liu, S.S.; McDonald, S.B. Current issues in spinal anesthesia. Anesthesiology 2001, 94, 888–906. [Google Scholar] [CrossRef]
- Goldblum, E.; Atchabahian, A. The use of 2-chloroprocaine for spinal anaesthesia. Acta Anaesthesiol. Scand. 2013, 57, 545–552. [Google Scholar] [CrossRef]
- Hampl, K.F.; Schneider, M.C.; Pargger, H.; Gut, J.; Drewe, J.; Drasner, K. A similar incidence of transient neurologic symptoms after spinal anesthesia with 2% and 5% lidocaine. Anesth. Analg. 1996, 83, 1051–1054. [Google Scholar] [CrossRef] [PubMed]
- Pollock, J.E.; Liu, S.S.; Neal, J.M.; Stephenson, C.A. Dilution of spinal lidocaine does not alter the incidence of transient neurologic symptoms. Anesthesiology 1999, 90, 445–450. [Google Scholar] [CrossRef]
- Tong, D.; Wong, J.; Chung, F.; Friedlander, M.; Bremang, J.; Mezei, G.; Streiner, D. Prospective study on incidence and functional impact of transient neurologic symptoms associated with 1% versus 5% hyperbaric lidocaine in short urologic procedures. Anesthesiology 2003, 98, 485–494. [Google Scholar] [CrossRef]
- Ben-David, B.; Maryanovsky, M.; Gurevitch, A.; Lucyk, C.; Solosko, D.; Frankel, R.; Volpin, G.; DeMeo, P.J. A comparison of minidose lidocaine-fentanyl and conventional-dose lidocaine spinal anesthesia. Anesth. Analg. 2000, 91, 865–870. [Google Scholar] [CrossRef] [PubMed]
- Nair, G.S.; Abrishami, A.; Lermitte, J.; Chung, F. Systematic review of spinal anaesthesia using bupivacaine for ambulatory knee arthroscopy. Br. J. Anaesth. 2009, 102, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Freedman, J.M.; Li, D.K.; Drasner, K.; Jaskela, M.C.; Larsen, B.; Wi, S. Transient neurologic symptoms symptoms after spinal anesthesia: An epidemiologic study of 1,863 patients. Anesthesiology 1998, 89, 633–641. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Language | Anesthesia | Type of Operation | Number of Groups | Local Anesthetics (Control Group) | Needle | Position during Surgery | Follow-up Periods |
|---|---|---|---|---|---|---|---|---|---|
| Ali | 2015 | English | SA a | Knee arthroscopy | 2 | Bupivacaine | 25G Quincke | Supine | 24,72,168 h |
| Aouad | 2001 | English | SA a | Cesarean section | 2 | Bupivacaine | 25G Whitacre | Supine | 24,48,72 h |
| Beilin | 2003 | English | CSE b | Cervical cerclage | 2 | Bupivacaine | 25G Sprotte | Lithotomy | 24 h |
| Breebaart | 2003 | English | SA a | Knee arthroscopy | 3 | G1: Levobupivacaine G2: Ropivacaine | 27G Whitacre | Supine | 48 h |
| Breebaart | 2014 | English | SA a | Knee arthroscopy | 4 | Chloroprocaine | 27G Whitacre | Supine | 168 h |
| Buckenmaier | 2003 | English | SA a | Anorectal surgery | 2 | Ropivacaine | 25G Pencan | Jackknife | 24,48,72,168 h |
| Casati | 2007 | English | SA a | Knee arthroscopy | 2 | Chloroprocaine | 25G Whitacre | Not described | 24, 168 h |
| de Santiago | 2009 | English | SA a | Tubal sterilization | 2 | Levobupivacaine | 27G Whitacre | Trendelenburg | 168 h |
| de Santiago | 2010 | Spanish | SA a | Anorectal surgery | 2 | Levobupivacaine | 27G Whitacre | Jackknife | 72, 168 h |
| de Weert | 2000 | English | SA a | Short surgery of the lower body | 2 | Prilocaine | 25G pencil-point | Supine | 24 h |
| Etezadi | 2013 | English | SA a | Varicocele, surgical fixation of lower extremities, transurethral resection of prostate, transurethral lithotripsy, herniorrhaphy | 4 | Bupivacaine | 25G Sprotte or Quincke | Supine or lithotomy | 8, 16, 24, 32, 40, 48, 72 h |
| Fanelli | 2009 | English | SA a | Knee arthroscopy | 2 | Ropivacaine | 25G Whitacre | Supine | 24, 168 h |
| Gozdemir | 2010 | English | SA a | Minor orthopedic, varicose vein, inguinal hernia, appendectomy | 2 | Levobupivacaine | 25G Quincke | Supine | 48, 168 h |
| Gozdemir | 2016 | English | SA a | Minor orthopedic, cesarean section, varicose vein, inguinal hernia, appendectomy | 4 | G1: Levobupivacaine G2: Bupivacaine G3: Articaine | 27G pencil-point | Not described | 24,48,72 h |
| Hampl | 1995 | English | SA a | Short gynecological procedure | 3 | Bupivacaine | 25G pencil-point | Lithotomy | 24 h |
| Hampl | 1998 | English | SA a | Short gynecological procedure | 3 | G1: Prilocaine G2: Bupivacaine | 25G pencil-point | Lithotomy | 24 h |
| Hodgson | 2000 | English | SA a | Knee arthroscopy | 2 | Procaine | 24 or 25G pencil-point | Supine | 72 h |
| Imbelloni | 2010 | English | SA a | Anorectal surgery | 2 | Bupivacaine | 27G Quincke | Jackknife | Until 30th day |
| Keld | 2000 | English | SA a | Inguinal hernia, femoral hernia, knee arthroscopy, removal of osteosynthetic material, fractures in the lower extremities, incision of infraumbilical abscess | 2 | Bupivacaine | 25G pencil-point | Supine | 24, 72 h |
| Khant | 2017 | English | SA a | Urologic surgery | 2 | Bupivacaine | 26G Quincke | Supine or lithotomy | Not described |
| Kyokong | 2001 | English | SA a | Cesarean section | 2 | Bupivacaine | 27G Quincke | Supine | 24 h |
| Le Truong | 2001 | English | SA a | General, gynecological, or other surgery | 2 | Procaine | 27G Whitacre | Supine or lithotomy | 48 h |
| Liguori | 1998 | English | SA a | Knee arthroscopy | 2 | Mepivacaine | 27G Whitacre | Supine | 48 h |
| Maliachi | 1999 | Portuguese | SA a | Femur surgery | 2 | Bupivacaine | 22G, not described | Supine | 24, 48, 72 h |
| Martin | 2005 | English | SA a | Knee arthroscopy | 2 | Prilocaine | 25G Whitacre | Not described | 48h |
| Martinez | 1998 | English | SA a | Orthopedic, urologic, gynecologic, vascular, general surgery | 2 | Prilocaine | 25G pencil-point | Not described | 72–120 h |
| Mulroy | 1999 | English | SA a | Inguinal hernia | 4 | Sameridine | 25G Whitacre | Supine | 24 h |
| Orozco | 2006 | Spanish | SA a | Surgery below the umbilicus | 2 | Bupivacaine | Not described | Not described | Not described |
| Ostgaard | 2000 | English | SA a | Urology surgery | 2 | Prilocaine | 25,26,27,29G Quincke | Supine or lithotomy | 24 h |
| Pawlowski | 2012 | English | CSE b | Anterior cruciate ligament repair | 2 | Mepivacaine | 27G Pencan | Supine | 24,48,72 h |
| Philip | 2001 | English | SA a | Postpartum tubal ligation | 2 | Bupivacaine | 25G Whitacre | Supine | 24,48 h |
| Pollock | 1996 | English | SA a | Knee arthroscopy or inguinal hernia | 3 | Bupivacaine | 22 or 25G Quincke or Whitacre | Supine | 72 h |
| Pradhan | 2010 | English | SA a | Cesarean section | 2 | Bupivacaine | 26G Quincke | Supine | Not described |
| Punj | 2013 | English | SA a | pelvic surgery | 4 | Bupivacaine | 24G Quincke | Supine | 120 h |
| Salazar | 2001 | English | SA a | Minor surgery of lower extremities | 2 | Mepivacaine | 26 or 27G Quincke | Supine | 24 h |
| Salmela | 1998 | English | SA a | Urologic surgery, varicose vein, hemorrhoidectomy, hernia | 3 | G1: Mepivacaine G2: Bupivacaine | 27G Quincke or Whitacre | Supine or lithotomy | 24 h |
| Teunkens | 2016 | English | SA a | Knee arthroscopy | 3 | G1: Chloroprocaine G2: Bupivacaine | 27G Whitacre | Supine | 24 h |
| Vaghadia | 2012 | English | SA a | Transurethral resection of prostate | 2 | Chloroprocaine | 25 or 27G Whitacre | Lithotomy | 96–168 h |
| Yea | 1998 | Korean | SA a | Surgery of lower body | 2 | Mepivacaine | 25G Quincke | Supine | 24 h |
| Study | Sample Size | LDC a | Control | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| LDC | Control | Concentration | Baricity | Dose | Added | Type | Concentration | Baricity | Dose | Added | |
| Ali 2015 | 25 | 25 | 0.6% | Hypobaric | 20 mg | FTN b 25 µg | Bupivacaine | 0.375% | Hyperbaric | 3 mg | FTN b 10 µg |
| Aouad 2001 | 100 | 100 | 5% | Hyperbaric | 75 mg | - | Bupivacaine | 0.75% | Hyperbaric | 12 mg | - |
| Beilin 2003 | 29 | 30 | 1% | Isobaric | 30 mg | FTN b 20 µg | Bupivacaine | 0.175% | Hyperbaric | 5.25 mg | FTN b 20 µg |
| Breebaart 2003 | 30 | G1: 30 G2: 30 | 2% | Isobaric | 60 mg | - | G1: Levobupivacaine G2: Ropivacaine | G1: 0.33% G2: 0.5% | G1:Isobaric G2:Isobaric | G1: 10 mg G2: 15 mg | - |
| Breebaart 2014 | 50 | 50 | 1.5% | Isobaric | 60 mg | - | Chloroprocaine | 1% | Isobaric | 40 mg | - |
| Buckenmaier 2003 | 37 | 35 | 2.5% | Hyperbaric | 25 mg | FTN b 20 µg | Ropivacaine | 0.5% | Hyperbaric | 4 mg | FTN b 20 µg |
| Casati 2007 | 15 | 15 | 1% | Isobaric | 50 mg | - | Chloroprocaine | 1% | Isobaric | 50 mg | |
| de Santiago 2009 | 26 | 26 | 0.3% | Hypobaric | 10 mg | FTN b 10 µg | Levobupivacaine | 0.1% | Hypobaric | 3 mg | FTN b 10 µg |
| de Santiago 2010 | 30 | 30 | 0.6% | Hypobaric | 18 mg | FTN b 10 µg | Levobupivacaine | 0.5% | Hypobaric | 3 mg | FTN b 10 µg |
| de Weert 2000 | 35 | 34 | 2% | Isobaric | 80 mg | - | Prilocaine | 2% | Isobaric | 80 mg | - |
| Etezadi 2013 | 125 | 125 | 5% | Hyperbaric | 75–100 mg | - | Bupivacaine | 0.5% | Isobaric | 12.5–15 mg | - |
| Fanelli 2009 | 15 | 15 | 1% | Isobaric | 50 mg | - | Ropivacaine | 0.5% | Isobaric | 10 mg | - |
| Gozdemir 2010 | 30 | 30 | 2% | Isobaric | 80 mg | - | Levobupivacaine | 0.5% | Isobaric | 20 mg | - |
| Gozdemir 2016 | 100 | G1: 100 G2: 100 G3: 100 | 2% | Isobaric | 60 mg | - | G1: Levobupivacaine G2: Bupivacaine G3: Articaine | G1: 0.5% G2: 0.5% G3: 2% | G1: Isobaric G2: Isobaric G3: Isobaric | G1: 15 mg G2: 15 mg G3: 60 mg | - |
| Hampl 1995 | G1: 15 G2: 13 | 16 | G1:5% (7.5% dextrose) G2:5% (2.7% dextrose) | G1:Hyperbaric G2: Hyperbaric | G1:75 mg G2: 75 mg | - | Bupivacaine | 0.5% | Hyperbaric | 7.5 mg | - |
| Hampl 1998 | 30 | G1: 30 G2: 30 | 2% | Hyperbaric | 50 mg | - | G1: Prilocaine G2: Bupivacaine | G1: 2% G2: 0.5% | G1: Hyperbaric G2: Hyperbaric | G1: 50 mg G2:12.5 mg | - |
| Hodgson 2000 | 35 | 35 | 2.5% | Hyperbaric | 50 mg | - | Procaine | 5% | Hyperbaric | 100 mg | |
| Imbelloni 2010 | 75 | 75 | 0.6% | Hypobaric | 18 mg | - | Bupivacaine | 0.15% | Hypobaric | 4.5 mg | - |
| Keld 2000 | 35 | 34 | 5% | Hyperbaric | 100 mg | - | Bupivacaine | 0.5% | Hyperbaric | 12.5 mg | - |
| Khant 2017 | 498 | 492 | 3.125% | Not described | 25 mg | Butorphanol 0.3 mg | Bupivacaine | 0.5% | Not described | 5 mg | - |
| Kyokong 2001 | 71 | 71 | 5% | Hyperbaric | 60 mg | MPc 0.2 mg EPId 0.1 mg | Bupivacaine | 0.5% | Hyperbaric | 11 mg | MPc 0.2 mg |
| Le Truong 2001 | 29 | 25 | 5% | Hyperbaric | 100 mg | - | Procaine | 5% | Isobaric | 100 mg | - |
| Liguori 1998 | 27 | 30 | 2% | Not described | 60 mg | - | Mepivacaine | 1.5% | Not described | 45 mg | - |
| Maliachi 1999 | 20 | 20 | 5% | Not described | 1 mg/kg | - | Bupivacaine | 0.5% | Not described | 7–15 mg | - |
| Martin 2005 | 40 | 40 | 1.5% | Not described | 45 mg | - | Prilocaine | 1.5% | Not described | 45 mg | - |
| Martinez 1998 | 98 | 100 | 5% | Hyperbaric | 67.7 ± 8.7 mg | - | Prilocaine | 5% | Hyperbaric | 68.6±9.7 mg | - |
| Mulroy 1999 | 32 | G1: 23 G2: 43 G3: 42 | 2.5% | Hyperbaric | 100 mg | - | Sameridine | Not described | Isobaric | G1: 15 mg G2: 20 mg G3: 23 mg | - |
| Orozco 2006 | 109 | 97 | 5% | Not described | Not described | - | Bupivacaine | 0.5% | Not described | Not described | - |
| Ostgaard 2000 | 49 | 50 | 2% | Isobaric | 80 mg | - | Prilocaine | 2% | Isobaric | 80 mg | - |
| Pawlowski 2012 | 41 | 38 | 2% | Isobaric | 80 mg | - | Mepivacaine | 2% | Isobaric | 80 mg | - |
| Philip 2001 | 29 | 28 | 5% | Hyperbaric | 60–80 mg | - | Bupivacaine | 0.75% | Hyperbaric | 10.5–12 mg | - |
| Pollock 1996 | G1:51 G2:51 | 50 | G1: 5% G2: 2% | Hyperbaric or isobaric | 60 or 75 mg | EPI d or none | Bupivacaine | 0.75% | Hyperbaric | 7.5 or 9 mg | - |
| Pradhan 2010 | 26 | 26 | 5% | Hyperbaric | 75 mg | - | Bupivacaine | 0.5% | Hyperbaric | 12.5 mg | - |
| Punj 2013 | G1:20 G2:20 | G1: 20 G2: 20 | G1: 5% G2: 2.5% | Hyperbaric | Not described | - | Bupivacaine | G1: 0.5% G2: 0.25% | Hyperbaric | G1: 10 mg G2: 5 mg | - |
| Salazar 2001 | 40 | 40 | 2% | Isobaric | 40–60 mg | - | Mepivacaine | 2% | Isobaric | 40–60 mg | - |
| Salmela 1998 | 30 | G1:30 G2: 30 | 2.5% | Hyperbaric | 60–100 mg | - | G1: Mepivacaine G2: Bupivacaine | G1: 4% G2: 0.5% | G1: Hyperbaric G2: Hyperbaric | G1:40–80 mg G2:7.5–17 mg | - |
| Teunkens 2016 | 28 | G1: 30 G2: 34 | 1% | Isobaric | 40 mg | - | G1: Chloroprocaine G2: Bupivacaine | G1: 1% G2: 0.5% | G1: Isobaric G2: Isobaric | G1: 40 mg G2: 7.5 mg | |
| Vaghadia 2012 | 20 | 20 | 1.75% | Not described | 35 mg | FTN b 12.5 µg | Chloroprocaine | 1.77% | Isobaric | 40 mg | FTN b 12.5 µg |
| Yea 1998 | 30 | 30 | 1.5% | Hyperbaric | 75 mg | - | Mepivacaine | 2% | Hyperbaric | - | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koo, C.-H.; Shin, H.-J.; Han, S.-H.; Ryu, J.-H. Lidocaine vs. Other Local Anesthetics in the Development of Transient Neurologic Symptoms (TNS) Following Spinal Anesthesia: A Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2020, 9, 493. https://doi.org/10.3390/jcm9020493
Koo C-H, Shin H-J, Han S-H, Ryu J-H. Lidocaine vs. Other Local Anesthetics in the Development of Transient Neurologic Symptoms (TNS) Following Spinal Anesthesia: A Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2020; 9(2):493. https://doi.org/10.3390/jcm9020493
Chicago/Turabian StyleKoo, Chang-Hoon, Hyun-Jung Shin, Sung-Hee Han, and Jung-Hee Ryu. 2020. "Lidocaine vs. Other Local Anesthetics in the Development of Transient Neurologic Symptoms (TNS) Following Spinal Anesthesia: A Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 9, no. 2: 493. https://doi.org/10.3390/jcm9020493
APA StyleKoo, C.-H., Shin, H.-J., Han, S.-H., & Ryu, J.-H. (2020). Lidocaine vs. Other Local Anesthetics in the Development of Transient Neurologic Symptoms (TNS) Following Spinal Anesthesia: A Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine, 9(2), 493. https://doi.org/10.3390/jcm9020493