Efficacy and Safety of Injectable and Oral Antibiotics in Treating Gonorrhea: A Systematic Review and Network Meta-Analysis


Abstract
1. Introduction
2. Methods
2.1. Reporting Guideline and Certainty of Evidence
2.2. Search Strategies and Inclusion Criteria
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
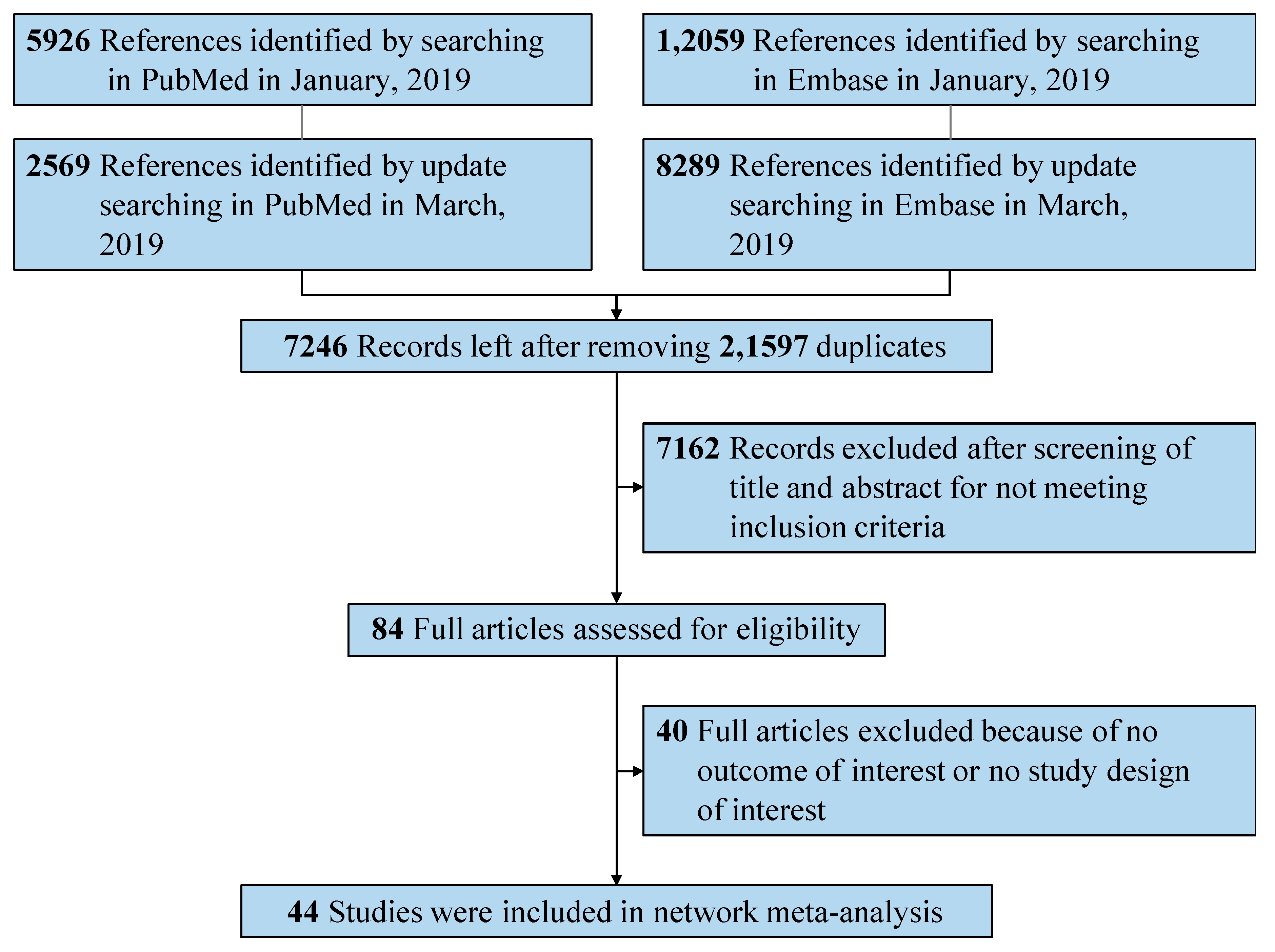
3.1. Literature Search Process and Study Characteristics
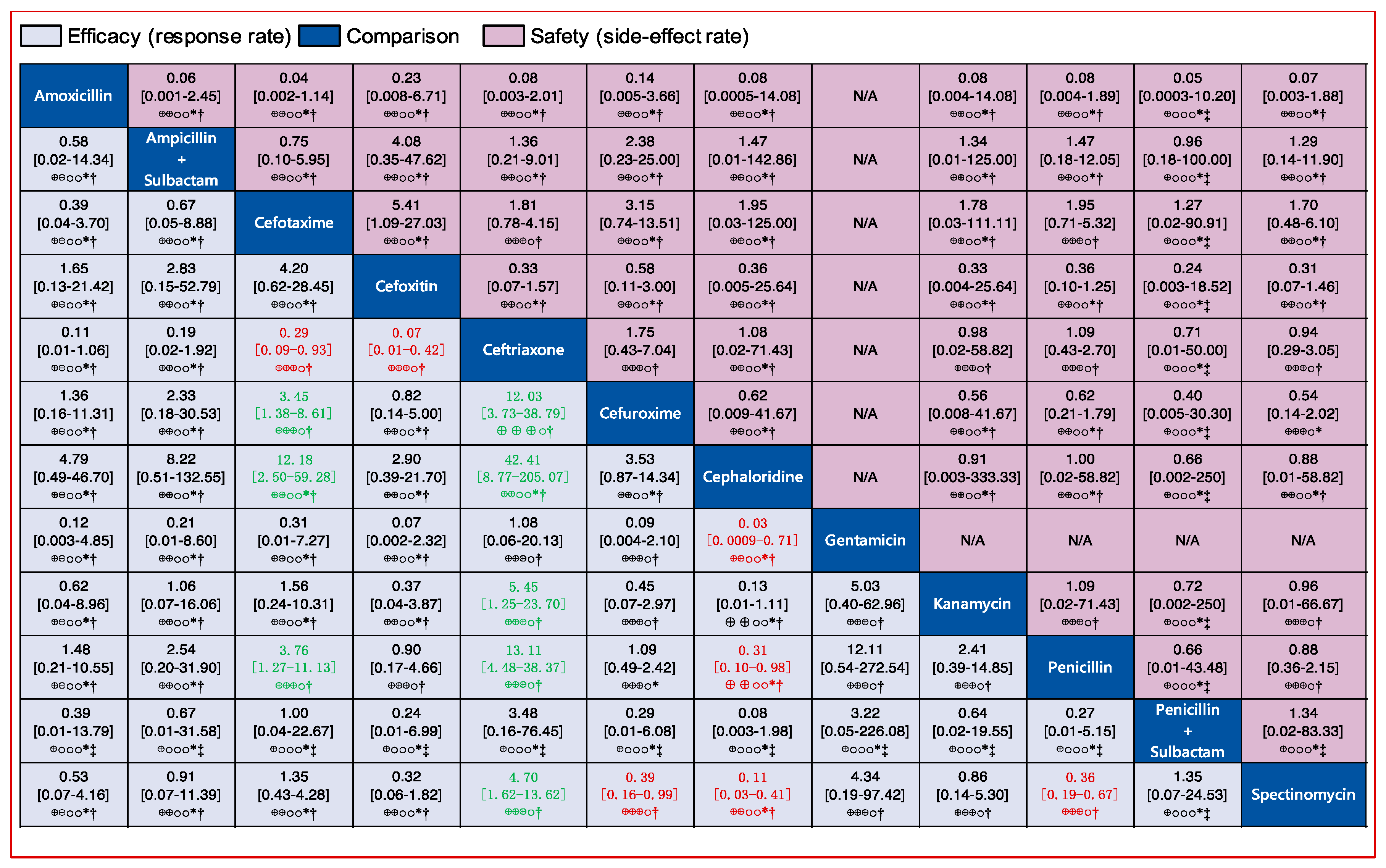
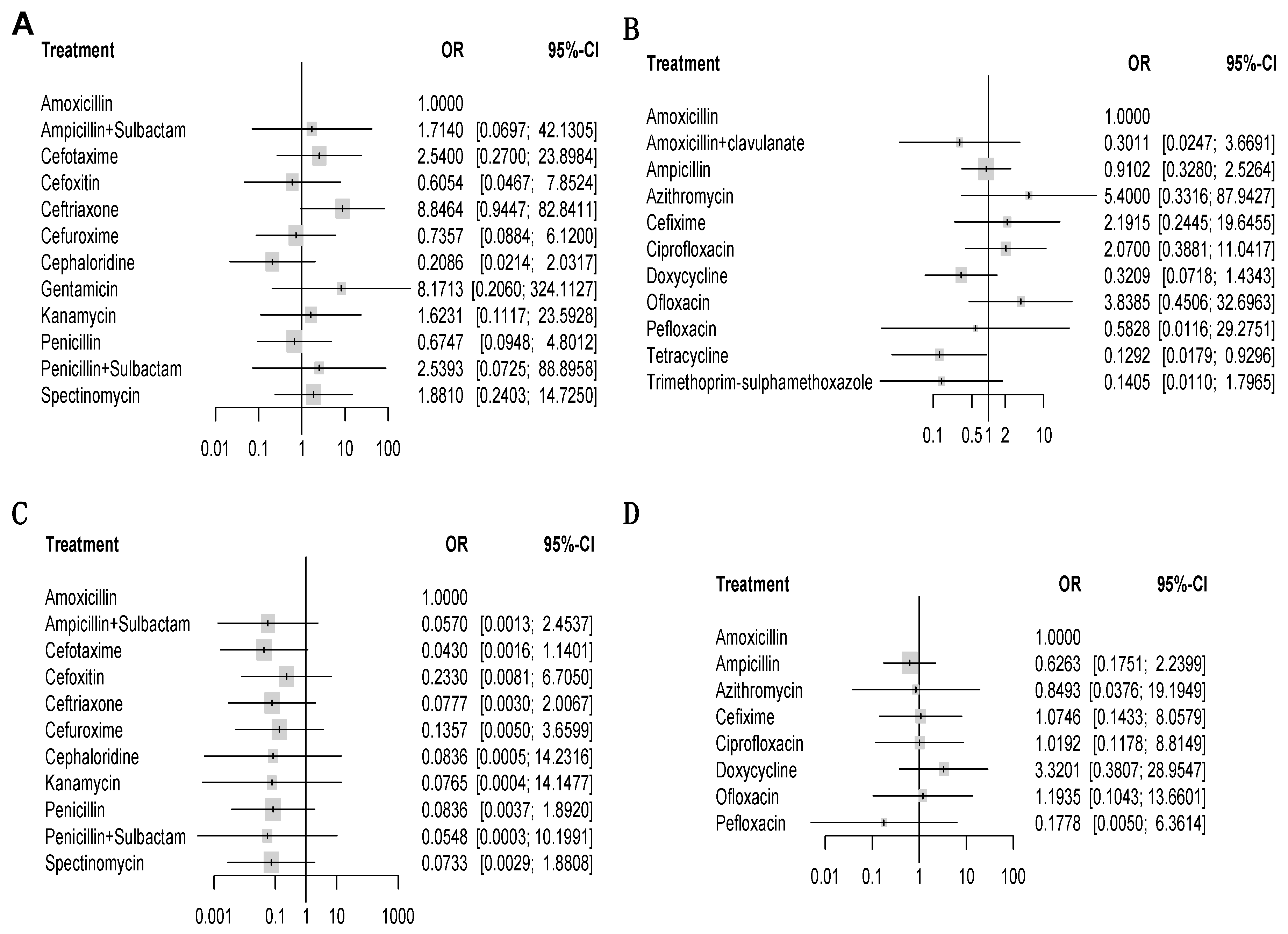
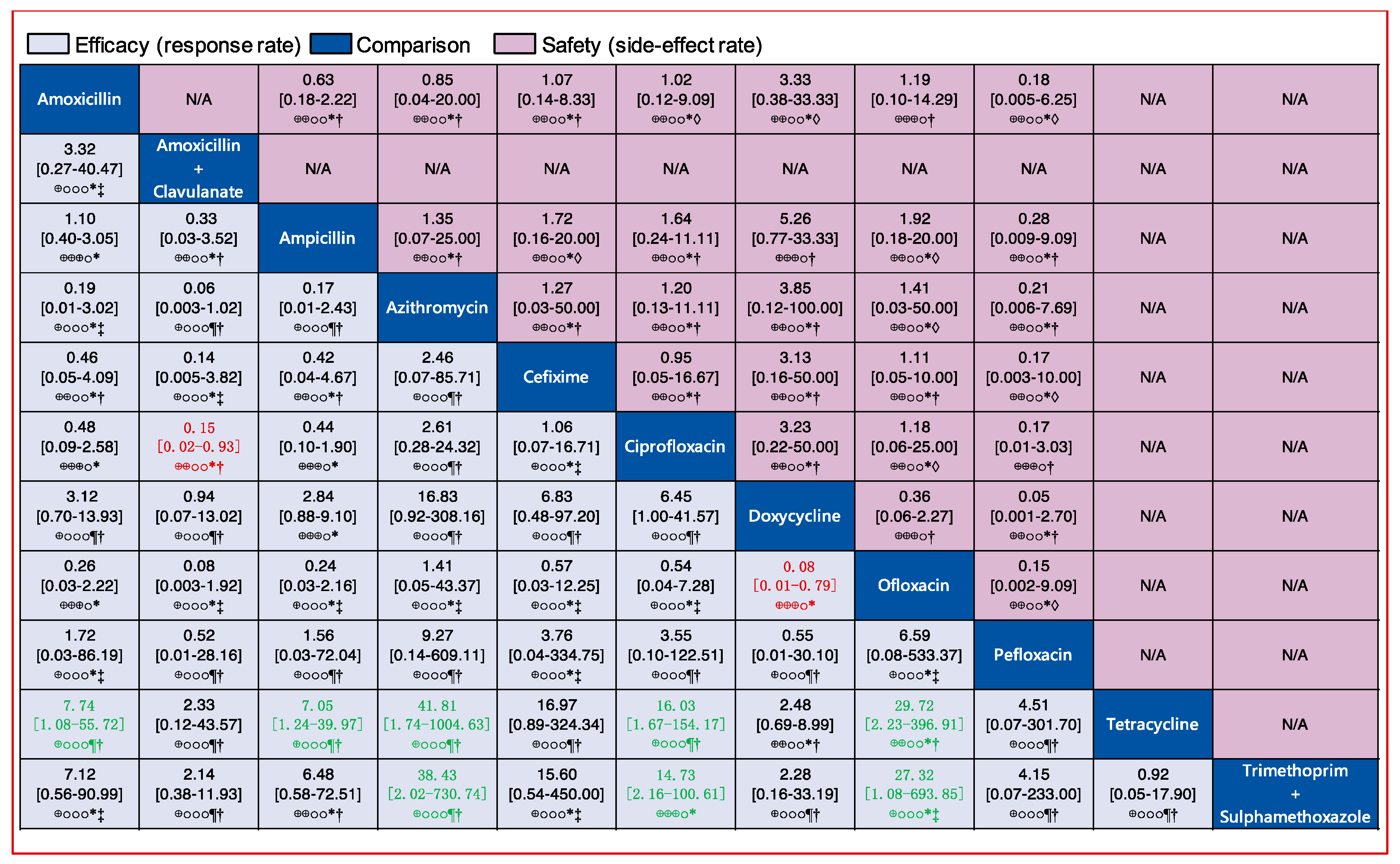
3.2. Pairwise Efficacy of Antibiotics
3.3. Safety of Antibiotics
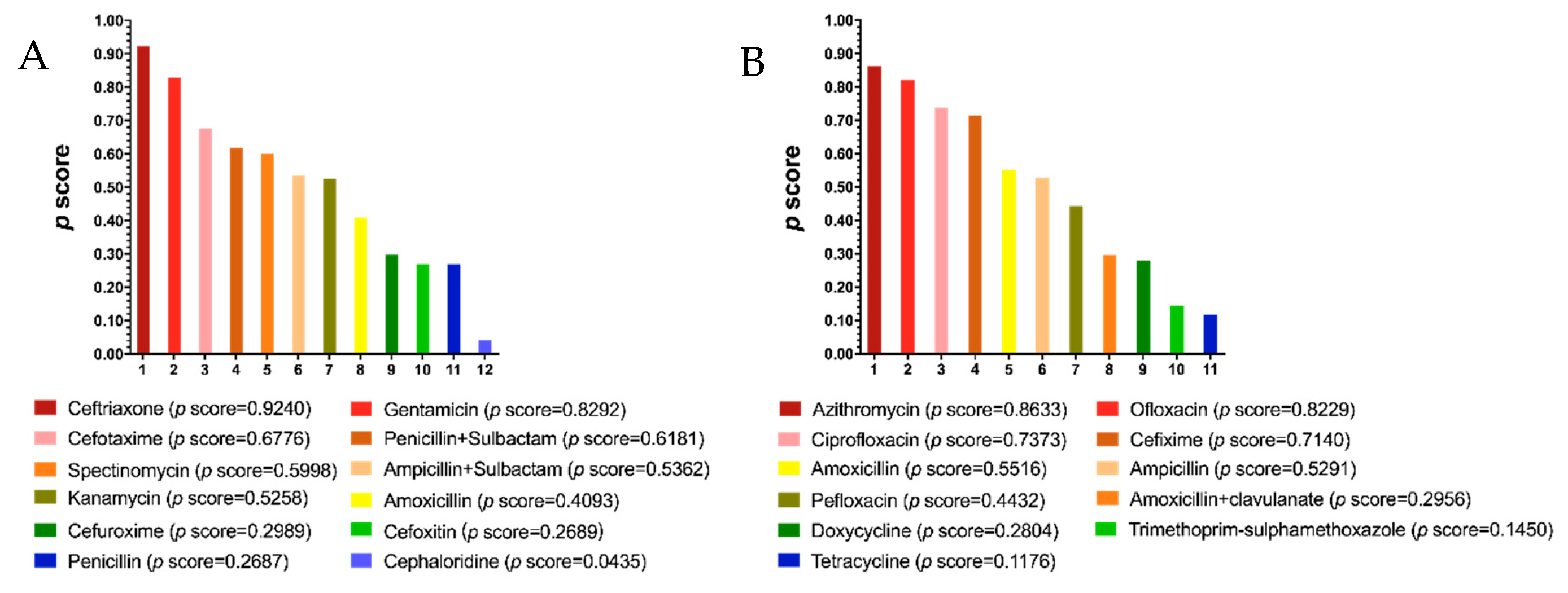
3.4. Ranking of Antibiotic Efficacy against Gonorrhea
3.5. Antibiotic Efficacy Based on Gonorrhea Infection Sites
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Unemo, M.; Jensen, J.S. Antimicrobial-resistant sexually transmitted infections: Gonorrhoea and Mycoplasma genitalium. Nat. Rev. Urol. 2017, 14, 139. [Google Scholar] [CrossRef] [PubMed]
- Suay-Garcia, B.; Perez-Gracia, M.T. Future Prospects for Neisseria gonorrhoeae Treatment. Antibiotics 2018, 7, 49. [Google Scholar] [CrossRef] [PubMed]
- Escobar, A.; Rodas, P.I.; Acuna-Castillo, C. Macrophage-Neisseria gonorrhoeae Interactions: A Better Understanding of Pathogen Mechanisms of Immunomodulation. Front. Immunol. 2018, 9, 3044. [Google Scholar] [CrossRef] [PubMed]
- Costa-Lourenco, A.; Barros Dos Santos, K.T.; Moreira, B.M.; Fracalanzza, S.E.L.; Bonelli, R.R. Antimicrobial resistance in Neisseria gonorrhoeae: History, molecular mechanisms and epidemiological aspects of an emerging global threat. Braz. J. Microbiol. 2017, 48, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Skerlev, M.; Culav-Koscak, I. Gonorrhea: New challenges. Clin. Derm. 2014, 32, 275–281. [Google Scholar] [CrossRef]
- Fifer, H.; Natarajan, U.; Jones, L.; Alexander, S.; Hughes, G.; Golparian, D.; Unemo, M. Failure of dual antimicrobial therapy in treatment of gonorrhea. N. Engl. J. Med. 2016, 374, 2504–2506. [Google Scholar] [CrossRef]
- Singh, A.E.; Gratrix, J.; Martin, I.; Friedman, D.S.; Hoang, L.; Lester, R.; Metz, G.; Ogilvie, G.; Read, R.; Wong, T. Gonorrhea Treatment Failures With Oral and Injectable Expanded Spectrum Cephalosporin Monotherapy vs Dual Therapy at 4 Canadian Sexually Transmitted Infection Clinics, 2010-2013. Sex. Transm. Dis. 2015, 42, 331. [Google Scholar] [CrossRef]
- Olesen, S.W.; Barnett, M.L.; MacFadden, D.R.; Brownstein, J.S.; Hernández-Díaz, S.; Lipsitch, M.; Grad, Y.H. The distribution of antibiotic use and its association with antibiotic resistance. eLife 2018, 7, e39435. [Google Scholar] [CrossRef]
- Albrich, W.C.; Monnet, D.L.; Harbarth, S. Antibiotic selection pressure and resistance in Streptococcus pneumoniae and Streptococcus pyogenes. Emerg. Infect. Dis. 2004, 10, 514. [Google Scholar] [CrossRef]
- Sánchez-Busó, L.; Golparian, D.; Corander, J.; Grad, Y.H.; Ohnishi, M.; Flemming, R.; Parkhill, J.; Bentley, S.D.; Unemo, M.; Harris, S.R. The impact of antimicrobials on gonococcal evolution. Nat. Microbiol. 2019, 4, 1941–1950. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Rind, D.; Devereaux, P.J.; Montori, V.M.; Freyschuss, B.; Vist, G.; et al. GRADE guidelines 6. Rating the quality of evidence--imprecision. J. Clin. Epidemiol. 2011, 64, 1283–1293. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Falck-Ytter, Y.; Jaeschke, R.; Vist, G.; et al. GRADE guidelines: 8. Rating the quality of evidence--indirectness. J. Clin. Epidemiol. 2011, 64, 1303–1310. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE guidelines: 7. Rating the quality of evidence--inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Montori, V.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Djulbegovic, B.; Atkins, D.; Falck-Ytter, Y.; et al. GRADE guidelines: 5. Rating the quality of evidence--publication bias. J. Clin. Epidemiol. 2011, 64, 1277–1282. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Montori, V.; Akl, E.A.; Djulbegovic, B.; Falck-Ytter, Y. GRADE guidelines: 4. Rating the quality of evidence—study limitations (risk of bias). J. Clin. Epidemiol. 2011, 64, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Puhan, M.A.; Schunemann, H.J.; Murad, M.H.; Li, T.; Brignardello-Petersen, R.; Singh, J.A.; Kessels, A.G.; Guyatt, G.H.; Group, G.W. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ 2014, 349, g5630. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Dias, S.; Welton, N.J.; Sutton, A.J.; Ades, A. Evidence synthesis for decision making 1: Introduction. Med. Decis. Mak. 2013, 33, 597–606. [Google Scholar] [CrossRef]
- Dias, S.; Welton, N.J.; Sutton, A.J.; Caldwell, D.M.; Lu, G.; Ades, A. Evidence synthesis for decision making 4: Inconsistency in networks of evidence based on randomized controlled trials. Med. Decis. Mak. 2013, 33, 641–656. [Google Scholar] [CrossRef] [PubMed]
- Rücker, G. Network meta-analysis, electrical networks and graph theory. Res. Synth. Methods 2012, 3, 312–324. [Google Scholar] [CrossRef] [PubMed]
- Rücker, G.; Schwarzer, G. Reduce dimension or reduce weights? Comparing two approaches to multi-arm studies in network meta-analysis. Stat. Med. 2014, 33, 4353–4369. [Google Scholar] [CrossRef] [PubMed]
- Dias, S.; Welton, N.; Caldwell, D.; Ades, A. Checking consistency in mixed treatment comparison meta-analysis. Stat. Med. 2010, 29, 932–944. [Google Scholar] [CrossRef] [PubMed]
- König, J.; Krahn, U.; Binder, H. Visualizing the flow of evidence in network meta-analysis and characterizing mixed treatment comparisons. Stat. Med. 2013, 32, 5414–5429. [Google Scholar] [CrossRef]
- Rücker, G.; Schwarzer, G. Ranking treatments in frequentist network meta-analysis works without resampling methods. BMC Med. Res. Methodol. 2015, 15, 58. [Google Scholar] [CrossRef]
- Molin, L.; Nyström, B. A comparison between cephaloridine and penicillin in the treatment of gonorrhoea. Chemotherapy 1970, 15, 384–391. [Google Scholar] [CrossRef]
- Crider, S.R.; Kilpatrick, M.E.; Harrison, W.O.; Kerbs, S.; Berg, S.W. A comparison of penicillin G plus a beta-lactamase inhibitor (sulbactam) with spectinomycin for treatment of urethritis caused by penicillinase-producing Neisseria gonorrhoeae. Sex. Transm. Dis. 1984, 11, 314–317. [Google Scholar] [CrossRef]
- Veeravahu, M.; Sumathipala, A.; Clay, J. Cefoxitin v procaine penicillin in the treatment of uncomplicated gonorrhoea. Br. J. Vener. Dis. 1983, 59, 406. [Google Scholar] [CrossRef][Green Version]
- Morrison, G.D.; Evans, A.J.; Haskins, H.W.; Lewis, N.M.; Seale, G.H.; Mayall, E.; Mullinger, B.M. Cefuroxime compared with penicillin for the treatment of gonorrhea. Sex. Transm. Dis. 1980, 7, 188–190. [Google Scholar] [CrossRef]
- Judson, F.; Ehret, J.; Root, C. Comparative study of ceftriaxone and aqueous procaine penicillin G in the treatment of uncomplicated gonorrhea in women. Antimicrob. Agents Chemother. 1983, 23, 218–220. [Google Scholar] [CrossRef] [PubMed]
- Judson, F.N.; Ehret, J.M.; Handsfield, H.H. Comparative study of ceftriaxone and spectinomycin for treatment of pharyngeal and anorectal gonorrhea. JAMA 1985, 253, 1417–1419. [Google Scholar] [CrossRef] [PubMed]
- Handsfield, H.H.; Murphy, V. Comparative study of ceftriaxone and spectinomycin for treatment of uncomplicated gonorrhoea in men. Lancet 1983, 322, 67–70. [Google Scholar] [CrossRef]
- Apaya, J. Comparison of amoxycillin and procaine penicillin in the treatment of uncomplicated gonorrhoea. Br. J. Vener. Dis. 1984, 60, 274. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zajdowicz, T.; Sanches, P.; Berg, S.; Kerbs, S.; Newquist, R.; Harrison, W. Comparison of ceftriaxone with cefoxitin in the treatment of penicillin-resistant gonococcal urethritis. Sex. Transm. Infect. 1983, 59, 176–178. [Google Scholar] [CrossRef] [PubMed]
- Lossick, J.G.; Thompson, S.E.; Smeltzer, M.P. Comparison of cefuroxime and penicillin in the treatment of uncomplicated gonorrhea. Antimicrob. Agents Chemother. 1982, 22, 409–413. [Google Scholar] [CrossRef]
- Duanćić, A.; Fiumara, N.J.; Alpert, S.; Lee, Y.-H.; Tarr, P.I.; Rosner, B.; McCormack, W.M. Comparison of spectinomycin hydrochloride and aqueous procaine penicillin G in the treatment of uncomplicated gonorrhea. Antimicrob. Agents Chemother. 1974, 6, 512–515. [Google Scholar] [CrossRef][Green Version]
- Baddour, L.M.; Busby, L.; Shapiro, E.; Cox, K.B.; Glassco, S.; Johnson, J.K. Evaluation of treatment with single-dose ampicillin/sulbactam with probenecid or ceftriaxone in patients with uncomplicated gonorrhea. Sex. Transm. Dis. 1992, 19, 341–345. [Google Scholar] [CrossRef]
- McCormack, W.M.; Mogabgab, W.J.; Jones, R.B.; Wendel, J.G.; Handsfield, H. Multicenter, comparative study of cefotaxime and ceftriaxone for treatment of uncomplicated gonorrhea. Sex. Transm. Dis. 1993, 20, 269–273. [Google Scholar] [CrossRef]
- Panikabutra, K.; Ariyarit, C.; Chitwarakorn, A.; Saensanoh, C.; Wongba, C. Randomised comparative study of ceftriaxone and spectinomycin in gonorrhoea. Sex. Transm. Infect. 1985, 61, 106–108. [Google Scholar] [CrossRef]
- Dixon, C.; Bittiner, J.; Shahidullah, M.; Slack, R.; Sulaiman, M. Randomised observer blind comparative trial of ceftriaxone and penicillin in treating uncomplicated gonorrhoea in men and women. Sex. Transm. Infect. 1986, 62, 78–81. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.W.; Robson, H.G. Single-dose treatment of gonococcal urethritis in males: Evaluation of procaine penicillin, ampicillin and spectinomycin. Can. Med. Assoc. J. 1974, 110, 165. [Google Scholar] [PubMed]
- Habte-Gabr, E.; Geyid, A.; Serdo, D.; Biddle, J.; Perine, P.L. Single-dose treatment of uncomplicated acute gonococcal urethritis in Ethiopian men: Comparison of rosoxacin, spectinomycin, penicillin, and ampicillin. Sex. Transm. Dis. 1987, 14, 153–155. [Google Scholar] [CrossRef]
- Pedersen, A.H.; Wiesner, P.J.; Holmes, K.K.; Johnson, C.J.; Turck, M. Spectinomycin and penicillin G in the treatment of gonorrhea: A comparative evaluation. JAMA 1972, 220, 205–208. [Google Scholar] [CrossRef]
- Chitwarakorn, A.; Ariyarit, C.; Panikabutra, K.; Buateing, A.; Biddle, J.; Thompson, S.; Brown, S. Treating gonococcal infections resistant to penicillin in Bangkok: Comparison of cefuroxime and spectinomycin. Sex. Transm. Infect. 1985, 61, 306–310. [Google Scholar] [CrossRef]
- Simpson, M.; Khan, M.; Siddiqui, Y.; Gruninger, R.; Wigren, D. Treatment of gonorrhea: Comparison of cefotaxime and penicillin. Antimicrob. Agents Chemother. 1981, 19, 798–800. [Google Scholar] [CrossRef]
- Stolz, E.; Ong, L.; van Joost, T.; Michel, M.F. Treatment of non-complicated urogenital, rectal and oropharyngeal gonorrhoea with intramuscular cefotaxime 1.0 g or cefuroxime 1.5 g. J. Antimicrob. Chemother. 1984, 14, 295–299. [Google Scholar] [CrossRef]
- Hira, S.K.; Attili, V.R.; Kamanga, J.; Mkandawire, O.; Patel, J.S.; Patel, M.I. Efficacy of gentamicin and kanamycin in the treatment of uncomplicated gonococcal urethritis in Zambia. Sex. Transm. Dis. 1985, 12, 52–54. [Google Scholar] [CrossRef]
- Rajan, V.; Sng, E.; Thirumoorthy, T.; Goh, C. Ceftriaxone in the treatment of ordinary and penicillinase-producing strains of Neisseria gonorrhoeae. Sex. Transm. Infect. 1982, 58, 314–316. [Google Scholar] [CrossRef]
- Mogabgab, W.J.; Lutz, F.B. Randomized study of cefotaxime versus ceftriaxone for uncomplicated gonorrhea. South. Med. J. 1994, 87, 461–464. [Google Scholar] [CrossRef]
- Judson, F.N.; Allaman, J.; Dans, P.E. Treatment of gonorrhea: Comparison of penicillin G procaine, doxycycline, spectinomycin, and ampicillin. JAMA 1974, 230, 705–708. [Google Scholar] [CrossRef]
- Boslego, J.W.; Hicks, C.B.; Greenup, R.; Thomas, R.J.; Wiener, H.A.; Ciak, J.; Tramont, E.C. A prospective randomized trial of ofloxacin vs. doxycycline in the treatment of uncomplicated male urethritis. Sex. Transm. Dis. 1988, 15, 186–191. [Google Scholar] [CrossRef]
- Lassus, A.; Karppinen, L.; Ingervo, L.; Jeskanen, L.; Reitamo, S.; Happonen, H.-P.; Karkulahti, R. Ciprofloxacin versus amoxycillin and probenecid in the treatment of uncomplicated gonorrhoea. Scand. J. Infect. Dis Suppl. 1989, 60, 58–61. [Google Scholar] [PubMed]
- Scott, G.; McMillan, A.; Young, H. Ciprofloxacin versus ampicillin and probenecid in the treatment of uncomplicated gonorrhoea in men. J. Antimicrob. Chemother. 1987, 20, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Dubois, J.; St-Pierre, C.; Olivier, C.; Clecner, B.; Austin, T.; Phillips, R. Comparative Double-Blind Multicentre Study of Single-Dose Pefloxacin and Amoxicillin Plus Probenecid for Treatment of Acute Uncomplicated Gonorrhoea. Drug Investig. 1990, 2, 203–207. [Google Scholar] [CrossRef]
- Karney, W.W.; Turck, M.; Holmes, K.K. Comparative therapeutic and pharmacological evaluation of amoxicillin and ampicillin plus probenecid for the treatment of gonorrhea. Antimicrob. Agents Chemother. 1974, 5, 114–118. [Google Scholar] [CrossRef][Green Version]
- Gruber, F.; Brajac, I.; Jonjic, A.; Grubisic-Greblo, H.; Lenkovic, M.; Stasic, A. Comparative trial of azithromycin and ciprofloxacin in the treatment of gonorrhea. J. Chemother. 1997, 9, 263–266. [Google Scholar] [CrossRef]
- Roddy, R.; Handsfield, H.; Hook, E. Comparative trial of single-dose ciprofloxacin and ampicillin plus probenecid for treatment of gonococcal urethritis in men. Antimicrob. Agents Chemother. 1986, 30, 267–269. [Google Scholar] [CrossRef]
- Mitchell, R.W.; Robson, H.G. Comparison of amoxicillin and ampicillin in single-dose oral treatment of males with gonococcal urethritis. Can. Med. Assoc. J. 1974, 111, 1198. [Google Scholar]
- Felman, Y.M.; William, D.C.; Corsaro, M.C. Comparison of ampicillin plus probenecid with amoxicillin plus probenecid for treatment of uncomplicated gonorrhea. Sex. Transm. Dis. 1979, 6, 72–74. [Google Scholar] [CrossRef]
- Enfors, W.; Eriksson, G. Comparison of oral ampicillin and doxycycline in the treatment of uncomplicated gonorrhoea. Sex. Transm. Infect. 1975, 51, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Brathwaite, A. Double-blind trial of amoxycillin and ampicillin plus probenecid in the treatment of gonorrhoea in men. Sex. Transm. Infect. 1979, 55, 340–342. [Google Scholar] [CrossRef] [PubMed]
- Jordan, W.C. Doxycycline vs. Tetracycline in the Treatment of Men with Gonorrhea: The Compliance Factor; LWW: Philadelphia, PA, USA, 1981. [Google Scholar]
- Black, J.; Long, J.; Zwickl, B.; Ray, B.; Verdon, M.; Wetherby, S.; Hook, E.; Handsfield, H. Multicenter randomized study of single-dose ofloxacin versus amoxicillin-probenecid for treatment of uncomplicated gonococcal infection. Antimicrob. Agents Chemother. 1989, 33, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Cheong, L.; Chan, R.; Nadarajah, M. Pefloxacin and ciprofloxacin in the treatment of uncomplicated gonococcal urethritis in males [corrected]. Sex. Transm. Infect. 1992, 68, 260–262. [Google Scholar] [CrossRef][Green Version]
- Megran, D.; Lefebvre, K.; Willetts, V.; Bowie, W. Single-dose oral cefixime versus amoxicillin plus probenecid for the treatment of uncomplicated gonorrhea in men. Antimicrob. Agents Chemother. 1990, 34, 355–357. [Google Scholar] [CrossRef]
- Karney, W.W.; Turck, M.; Holmes, K.K. Single-dose oral therapy for uncomplicated gonorrhea: Comparison of amoxicillin and ampicillin given with and without probenecid. J. Infect. Dis. 1974, 129, S250–S253. [Google Scholar] [CrossRef]
- Jordan, W.C. The efficacy of doxycycline vs tetracycline in treatment of gonorrhea in men. J. Natl. Med. Assoc. 1980, 72, 987. [Google Scholar]
- Lule, G.; Behets, F.; Hoffman, I.; Dallabetta, G.; Hamilton, H.; Moeng, S.; Liomba, G.; Cohen, M. STD/HIV control in Malawi and the search for affordable and effective urethritis therapy: A first field evaluation. Sex. Transm. Infect. 1994, 70, 384–388. [Google Scholar] [CrossRef]
- Baytch, H.; Rankin, D. Comparison of penicillin, tetracycline, and doxycycline in the treatment of uncomplicated gonorrhoea in men. Br. J. Vener. Dis. 1972, 48, 129. [Google Scholar] [CrossRef][Green Version]
- Kirkcaldy, R.D.; Weinstock, H.S.; Moore, P.C.; Philip, S.S.; Wiesenfeld, H.C.; Papp, J.R.; Kerndt, P.R.; Johnson, S.; Ghanem, K.G.; Hook III, E.W. The efficacy and safety of gentamicin plus azithromycin and gemifloxacin plus azithromycin as treatment of uncomplicated gonorrhea. Clin. Infect. Dis. 2014, 59, 1083–1091. [Google Scholar] [CrossRef]
- Ross, J.D.; Brittain, C.; Cole, M.; Dewsnap, C.; Harding, J.; Hepburn, T.; Jackson, L.; Keogh, M.; Lawrence, T.; Montgomery, A.A. Gentamicin compared with ceftriaxone for the treatment of gonorrhoea (G-ToG): A randomised non-inferiority trial. Lancet 2019, 393, 2511–2520. [Google Scholar] [CrossRef]
- Mann, L.M.; Kirkcaldy, R.D.; Papp, J.R.; Torrone, E.A. Susceptibility of Neisseria gonorrhoeae to Gentamicin—Gonococcal Isolate Surveillance Project, 2015–2016. Sex. Transm. Dis. 2018, 45, 96. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Injectable Drugs | Oral Drugs | Side-Effect Injectable Drugs | Side-Effect of Oral Drugs | ||||
|---|---|---|---|---|---|---|---|
| Comparison | p-Value | Comparison | p-Value | Comparison | p-Value | Comparison | p-Value |
| Penicillin vs. Spectinomycin | 0.047 | Amoxicillin vs. Ampicillin | 0.5964 | Cefotaxime vs. Ceftriaxone | 0.6689 | Amoxicillin vs. Ampicillin | 0.5016 |
| Cefuroxime vs. Spectinomycin | 0.3831 | Amoxicillin vs. Ciprofloxacin | 0.5218 | Cefotaxime vs. Penicillin | 0.6689 | Amoxicillin vs. Ciprofloxacin | 0.9755 |
| Cefuroxime vs. Penicillin | 0.4805 | Amoxicillin vs. Ofloxacin | 0.967 | Ceftriaxone vs. Penicillin | 0.8017 | Amoxicillin vs. Ofloxacin | 0.3817 |
| Ceftriaxone vs. Spectinomycin | 0.0959 | Ampicillin vs. Ciprofloxacin | 0.5218 | Ceftriaxone vs. Spectinomycin | 0.8415 | Ampicillin vs. Ciprofloxacin | 0.9755 |
| Ceftriaxone vs. Penicillin | 0.4123 | Ampicillin vs. Doxycycline | 0.967 | Cefuroxime vs. Penicillin | 0.0014 | Ampicillin vs. Doxycycline | 0.3817 |
| Cefoxitin vs. Penicillin | 0.2379 | Doxycycline vs. Ofloxacin | 0.967 | Cefuroxime vs. Spectinomycin | 0.0014 | Doxycycline vs. Ofloxacin | 0.3817 |
| Cefoxitin vs. Ceftriaxone | 0.2379 | Penicillin vs. Spectinomycin | 0.055 | ||||
| Cefotaxime vs. Penicillin | 0.5115 | ||||||
| Cefotaxime vs. Cefuroxime | 0.9661 | ||||||
| Cefotaxime vs. Ceftriaxone | 0.6748 | ||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.; Dhital, S.; Naderer, T. Efficacy and Safety of Injectable and Oral Antibiotics in Treating Gonorrhea: A Systematic Review and Network Meta-Analysis. J. Clin. Med. 2019, 8, 2182. https://doi.org/10.3390/jcm8122182
Yang J, Dhital S, Naderer T. Efficacy and Safety of Injectable and Oral Antibiotics in Treating Gonorrhea: A Systematic Review and Network Meta-Analysis. Journal of Clinical Medicine. 2019; 8(12):2182. https://doi.org/10.3390/jcm8122182
Chicago/Turabian StyleYang, Jiaru, Subhash Dhital, and Thomas Naderer. 2019. "Efficacy and Safety of Injectable and Oral Antibiotics in Treating Gonorrhea: A Systematic Review and Network Meta-Analysis" Journal of Clinical Medicine 8, no. 12: 2182. https://doi.org/10.3390/jcm8122182
APA StyleYang, J., Dhital, S., & Naderer, T. (2019). Efficacy and Safety of Injectable and Oral Antibiotics in Treating Gonorrhea: A Systematic Review and Network Meta-Analysis. Journal of Clinical Medicine, 8(12), 2182. https://doi.org/10.3390/jcm8122182