
Filling the Gap: Facial Anatomy and Safe Lower Lip Injection Practices

Abstract
1. Introduction
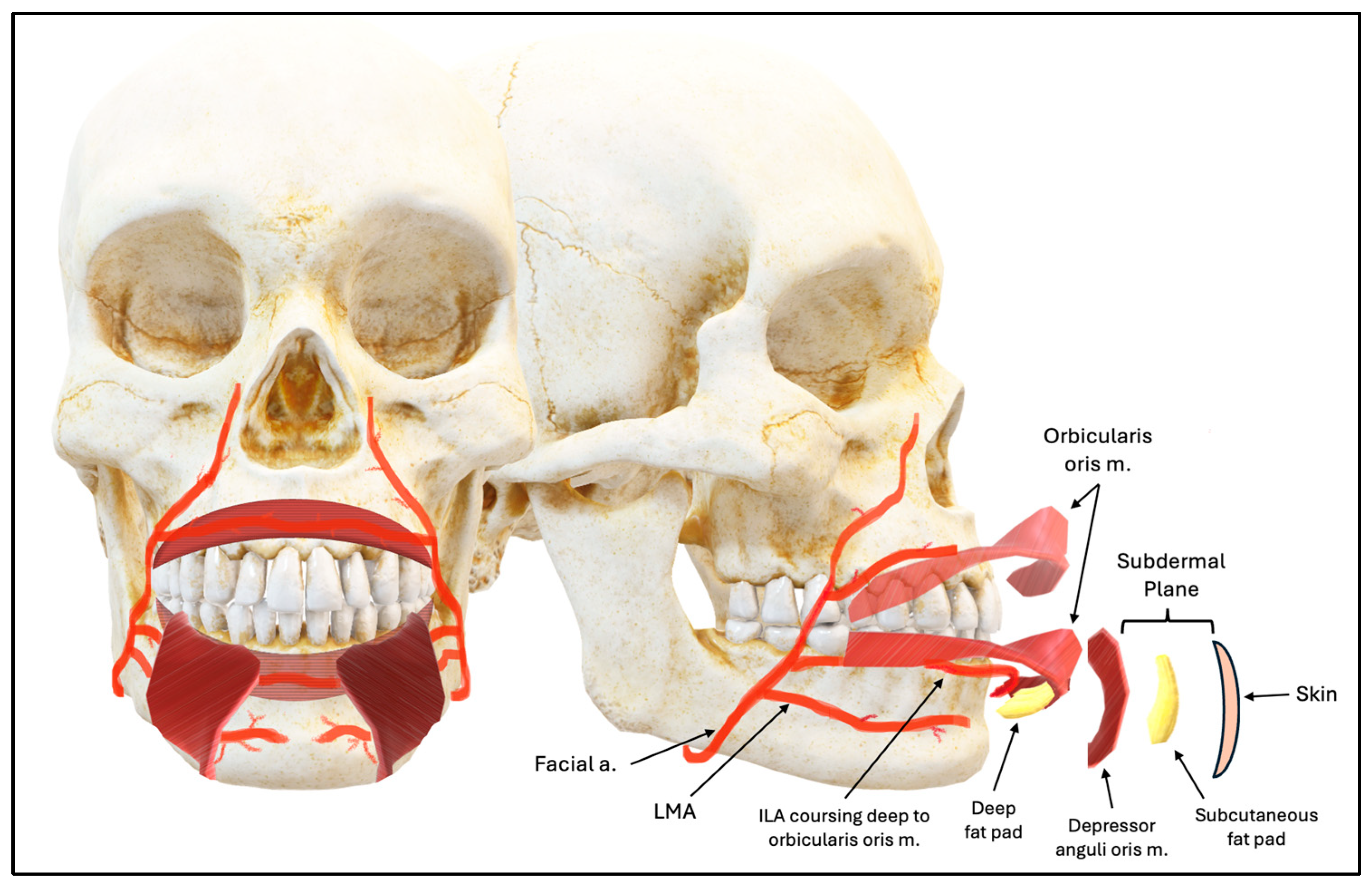
1.1. Anatomical Considerations
1.2. Complications
1.3. Purpose
2. Materials and Methods
2.1. Specimens
2.2. Dissection of the Hemifaces
2.3. Data Collection and Analysis
3. Results
3.1. Prevalence
3.2. Characterization
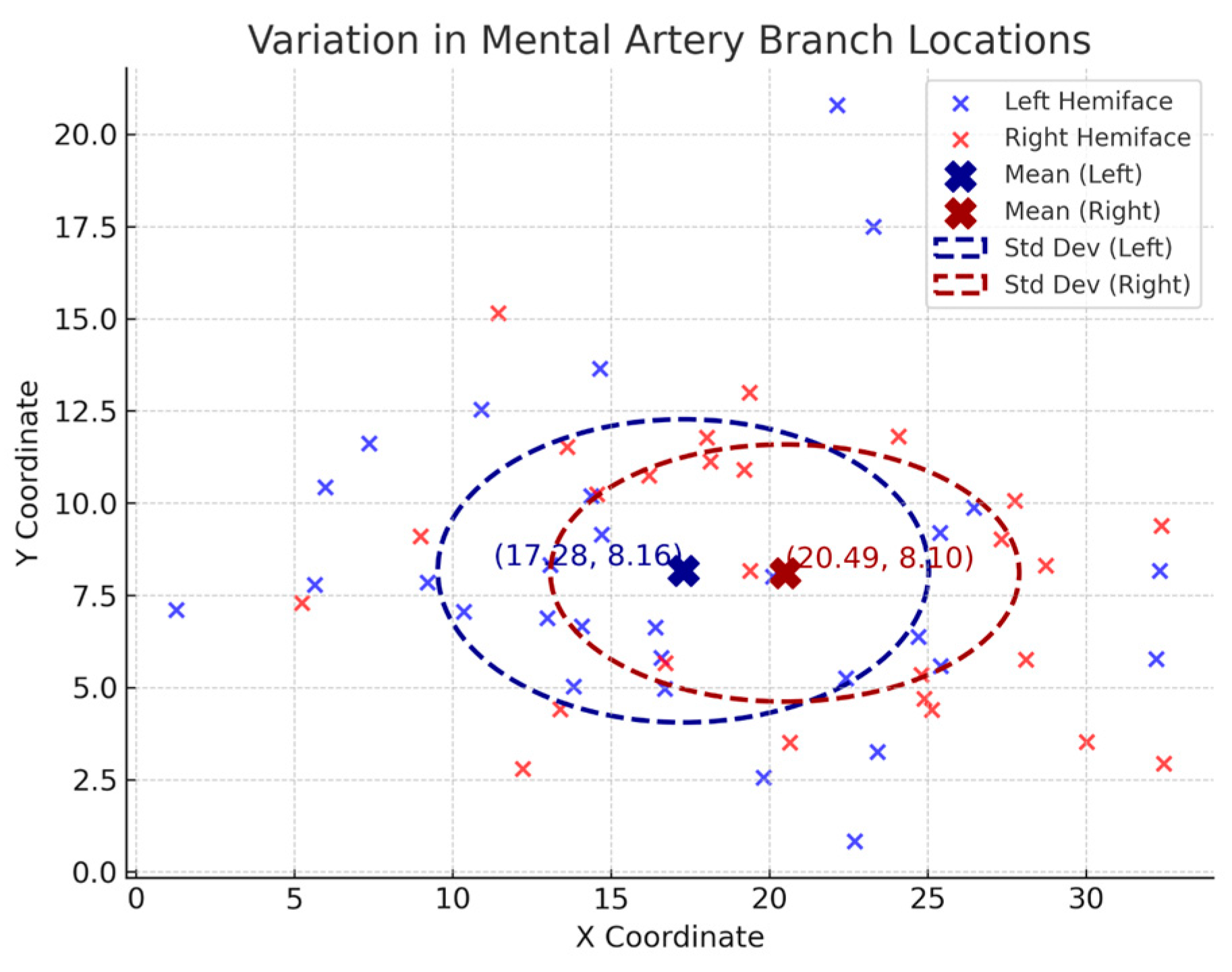
3.3. Statistical Analysis
4. Discussion
4.1. Overview
4.2. Inferior Labial Artery
4.3. Labiomental Artery
4.4. Mental Artery
4.5. Additional Safety Practices
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ILA | Inferior Labial Artery |
| FA | Facial Artery |
| LMA | Labiomental Artery |
| MA | Mental Artery |
| SLA | Superior Labial Artery |
| MF | Mental Foramen |
| M1 | Mental Artery Branch 1 (most medial) |
| M2 | Mental Artery Branch 2 |
| M3 | Mental Artery Branch 3 |
References
- American Society of Plastic Surgeons. 2020 Plastic Surgery Statistics Report; American Society of Plastic Surgeons: Arlington Heights, IL, USA, 2020; Available online: https://www.plasticsurgery.org/documents/News/Statistics/2020/plastic-surgery-statistics-full-report-2020.pdf (accessed on 9 March 2025).
- Eggerstedt, M.; Rhee, J.; Urban, M.J.; Mangahas, A.; Smith, R.M.; Revenaugh, P.C. Beauty is in the eye of the follower: Facial aesthetics in the age of social media. Am. J. Otolaryngol. 2020, 41, 102643. [Google Scholar] [CrossRef] [PubMed]
- Tansatit, T.; Phumyoo, T.; MCCabe, H.; Jitaree, B. Translucent and ultrasonographic studies of the inferior labial artery for improvement of filler injection techniques. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2399. [Google Scholar] [CrossRef] [PubMed]
- Al-Hoqail, R.A.; Meguid, E.M. Anatomic dissection of the arterial supply of the lips: An anatomical and analytical approach. J. Craniofacial Surg. 2008, 19, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-L.; Lee, H.-J.; Youn, K.-H.; Kim, H.-J. Positional relationship of superior and inferior labial artery by ultrasonography image analysis for safe lip augmentation procedures. Clin. Anat. 2020, 33, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Glaich, A.S.; Cohen, J.L.; Goldberg, L.H. Injection necrosis of the glabella: Protocol for prevention and treatment after use of dermal fillers. Dermatol. Surg. 2006, 32, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-J.; Won, S.-Y.; Jehoon, O.; Hu, K.-S.; Mun, S.-Y.; Yang, H.-M.; Kim, H.-J. The facial artery: A comprehensive anatomical review. Clin Anat. 2018, 31, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Kikuta, S.; Iwanaga, J.; Kusukawa, J.; Tubbs, R.S. The mental artery: Anatomical study and literature review. J Anat. 2020, 236, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Crouzet, C.; Fournier, H.; Papon, X.; Hentati, N.; Cronier, P.; Mercier, P. Anatomy of the arterial vascularization of the lips. Surg. Radiol. Anat. 1998, 20, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Funt, D.; Pavicic, T. Dermal fillers in aesthetics: An overview of adverse events and treatment approaches. Clin. Cosmet. Investig. Dermatol. 2013, 6, 295–316. [Google Scholar] [CrossRef] [PubMed]
- Hong, G.W.; Hu, H.; Chang, K.; Park, Y.; Lee, K.W.A.; Chan, L.K.W.; Yi, K.-H. Review of the adverse effects associated with dermal filler treatments: Part I Nodules, Granuloma, and Migration. Diagnostics 2024, 14, 1640. [Google Scholar] [CrossRef] [PubMed]
- Kroumpouzos, G.; Treacy, P. Hyaluronidase for dermal filler complications: Review of applications and dosage recommendations. JMIR Dermatol. 2024, 7, e50403. [Google Scholar] [CrossRef] [PubMed]
- Brandt, F.S.; Cazzaniga, A. Hyaluronic acid gel fillers in the management of facial aging. Clin. Interv. Aging 2008, 3, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Lee, H.J.; Kim, Y.S.; Kim, H.J.; Hu, K.S. What is the difference between the inferior labial artery and the horizontal labiomental artery? Surg. Radiol. Anat. 2015, 37, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Thanasarnaksorn, W.; Thanyavuthi, A.; Prasertvit, P.; Rattanakuntee, S.; Jitaree, B.; Suwanchinda, A. Case series of tongue necrosis from vascular complications after chin augmentation with hyaluronic acid: Potential pathophysiology and management. J. Cosmet. Dermatol. 2023, 22, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Clark, N.W.; Pan, D.R.; Barrett, D.M. Facial fillers: Relevant anatomy, injection techniques, and complications. World J. Otorhinolaryngol. Head Neck Surg. 2023, 9, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Tansatit, T.; Apinuntrum, P.; Phetudom, T. A dark side of the cannula injections: How arterial wall perforations and emboli occur. Aesthetic Plast. Surg. 2017, 41, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Tansatit, T.; Phumyoo, T.; Sawatwong, W.; McCabe, H.; Jitaree, B. Implication of location of the ascending mental artery at the chin injection point. Plast. Reconstr. Surg. 2020, 145, 51e–57e. [Google Scholar] [CrossRef] [PubMed]
- Goodman, G.J.; Magnusson, M.R.; Callan, P.; Roberts, S.; Hart, S.; Lin, F.; Rahman, E.; McDonald, C.B.; Liew, S.; Porter, C.; et al. Aspiration before tissue filler-an exercise in futility and unsafe practice. Aesthetic Surg. J. 2022, 42, 89–101. [Google Scholar] [CrossRef] [PubMed]
- Beiu, C.; Popa, L.G.; Bălăceanu-Gurău, B.; Iliescu, C.A.; Racoviță, A.; Popescu, M.N.; Mihai, M.M. Personalization of minimally-invasive aesthetic procedures with the use of ultrasound compared to alternative imaging modalities. Diagnostics 2023, 13, 3512. [Google Scholar] [CrossRef] [PubMed]
- Li, A.; Yan, J.; Zhao, Y.; Yu, Z.; Tian, S.; Khan, A.H.; Zhu, Y.; Wu, A.; Zhang, C.; Tian, X.-L. Vascular aging: Assessment and intervention. Clin. Interv. Aging 2023, 18, 1373–1395. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Artery | Prevalence Amongst Hemifaces | Prevalence Supplying Lower Lip | ||
|---|---|---|---|---|
| n | Percentage (%) | n | Percentage (%) | |
| ILA | 43 | 90 | 42 | 88 |
| LMA | 36 | 75 | 15 | 43 |
| MA | 48 | 100 | 46 | 96 |
| Variable | n | Percentage (%) | |
|---|---|---|---|
| Characterization Type | A | 5 | 10 |
| B | 43 | 90 | |
| C | 0 | 0 | |
| Bifurcation point in relation to oral commissure | Superior | 0 | 0 |
| In line with | 1 | 2.1 | |
| Inferior | 42 | 88 | |
| Relationship to orbicularis oris muscle | Superficial | 0 | 0 |
| Deep | 43 | 90 | |
| Intermediate | 5 | 10 | |
| Relationship to depressor anguli oris muscle | Superficial | 3 | 6.4 |
| Deep | 40 | 83 | |
| Indeterminate | 5 | 10 | |
| Relationship to depressor labii inferioris muscle | Superficial | 15 | 31 |
| Deep | 28 | 58 | |
| Indeterminate | 5 | 10 | |
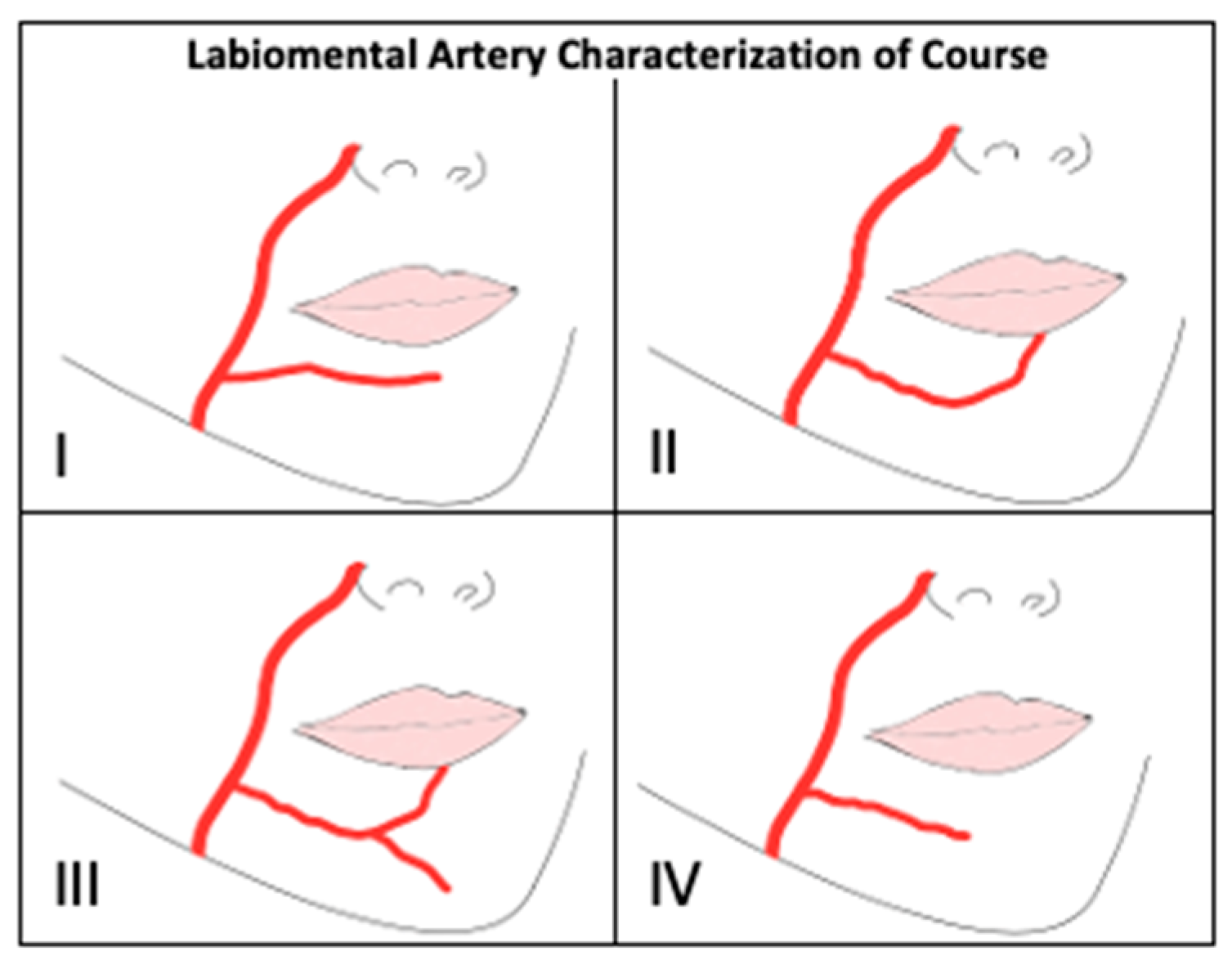
| Variable | n | Percentage (%) | |
|---|---|---|---|
| Characterization Type | I | 0 | 0 |
| II | 11 | 3.1 | |
| III | 0 | 0 | |
| IV | 21 | 58 | |
| II and IV | 4 | 11 | |
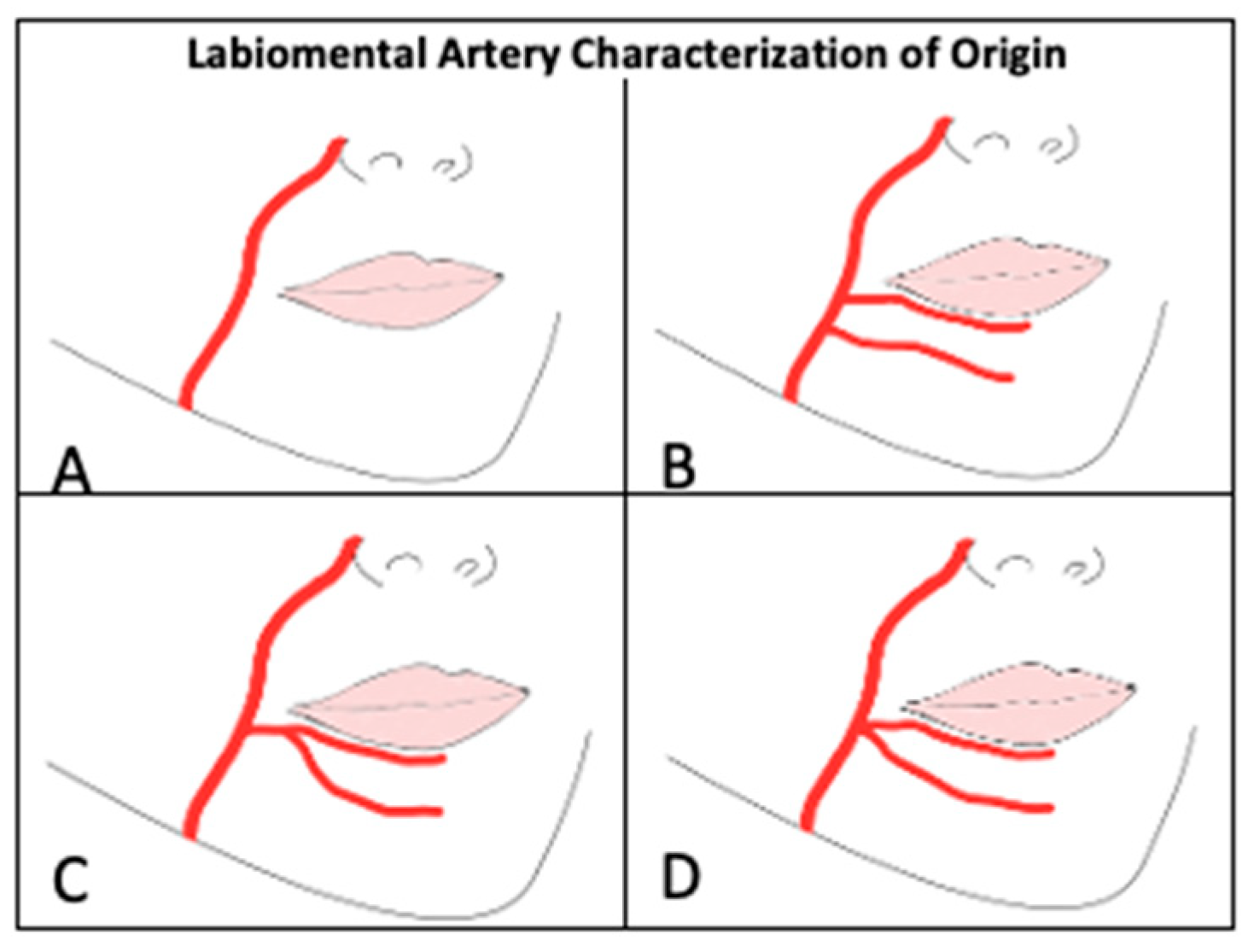
| Characterization of Origin | A | 11 | 23 |
| B | 30 | 63 | |
| C | 4 | 8.3 | |
| D | 3 | 6.3 | |
| Relationship to orbicularis oris muscle | Superficial | 0 | 0 |
| Deep | 36 | 75 | |
| Intermediate | 12 | 25 | |
| Relationship to depressor anguli oris muscle | Superficial | 0 | 0 |
| Deep | 36 | 75 | |
| Indeterminate | 12 | 25 | |
| Relationship to depressor labii inferioris muscle | Superficial | 1 | 2.1 |
| Deep | 35 | 73 | |
| Indeterminate | 12 | 25 | |
| Variable | n | Percentage (%) | |
|---|---|---|---|
| Characterization Type | 1 | 2 | 4.2 |
| 2 | 27 | 56 | |
| 3 | 18 | 38 | |
| 4 | 1 | 2.1 | |
| Branches Supplying Inferior Lip | 0 | 1 | 2.1 |
| 1 | 20 | 42 | |
| 2 | 22 | 46 | |
| 3 | 3 | 6.3 | |
| Indeterminate | 2 | 4.2 | |
| Artery | Mean ± SD (mm) | Range (mm) |
|---|---|---|
| ILA | 1.5 ± 0.49 | 0.35–2.5 |
| LMA | 1.2 ± 0.53 | 0.23–2.5 |
| All MAs | 1.6 ± 0.51 | 0.62–2.7 |
| M1 | 1.7 ± 0.48 | 0.65–2.7 |
| M2 | 1.4 ± 0.48 | 0.62–2.3 |
| M3 | 1.1 ± 0.50 | 0.66–1.6 |
| Artery | Left Hemifaces Included (n) | Left Hemiface Diameter Mean ± SD (mm) | Right Hemifaces Included (n) | Right Hemiface Diameter Mean ± SD (mm) | Statistical Significance |
|---|---|---|---|---|---|
| ILA | 15 | 1.4 ± 0.48 | 16 | 1.5 ± 0.53 | p = 0.57 |
| LMA | 14 | 1.3 ± 0.62 | 11 | 1.4 ± 0.56 | p = 0.72 |
| MAs Combined | 30 | 1.6 ± 0.50 | 26 | 1.6 ± 0.59 | p = 0.83 |
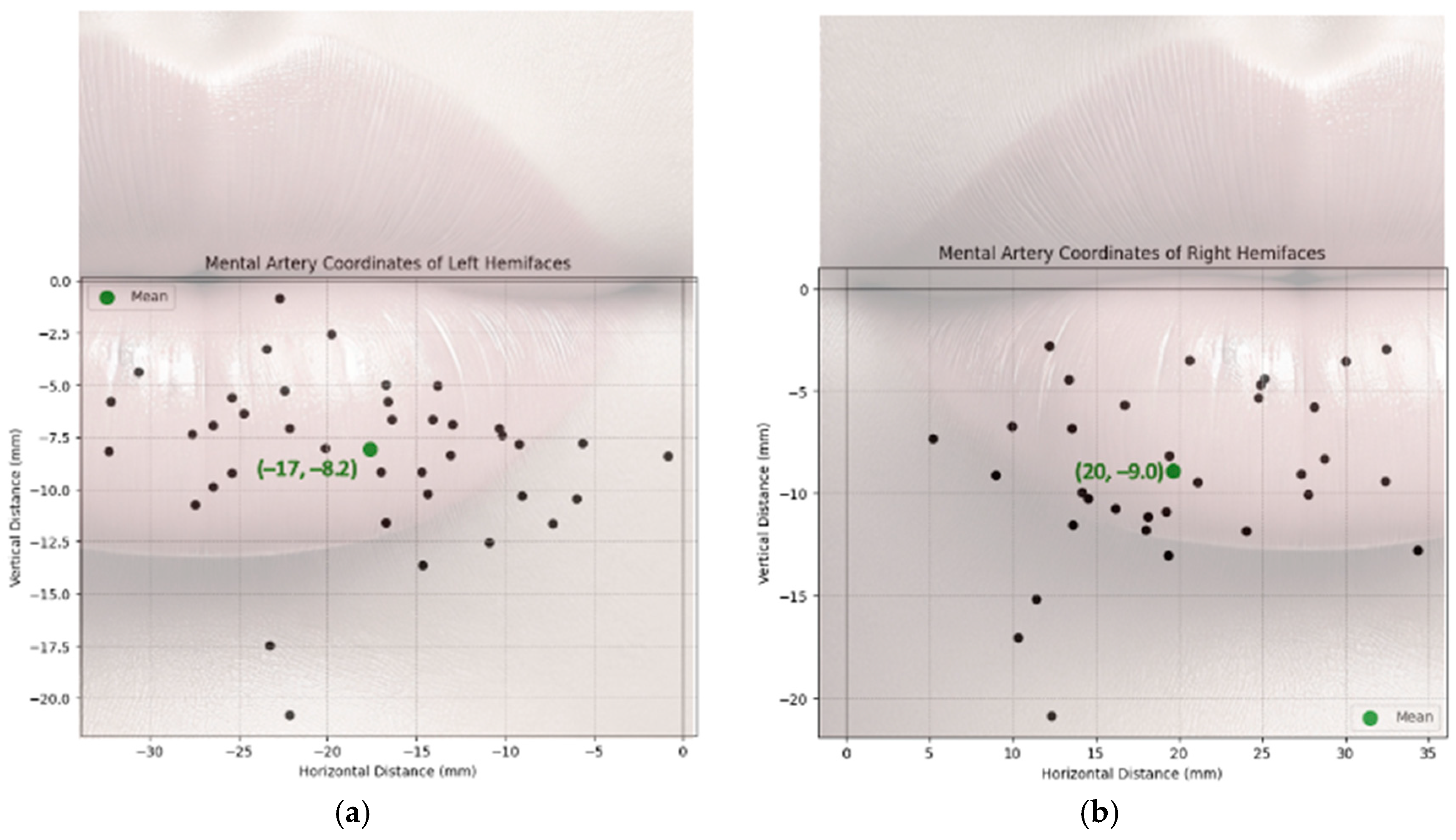
| Bilaterality | Branches Include (n) | Mean | Horizontal (X) Variation | Vertical (Y) Variation | Overall Variation |
|---|---|---|---|---|---|
| Left Hemifaces | 30 | (−17, −8.2) | 60 | 17 | 34 |
| Right Hemifaces | 26 | (20, −8.1) | 55 | 12 | 33 |
| Levene’s Test | W = 0.03 | W = 0.03 | |||
| p = 0.86 | p = 0.86 | ||||
| F-Test for Variance | F = 1.1 | F = 1.4 | |||
| p = 0.82 | p = 0.41 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Swancutt, M.M.; Allard, A.J.; Ho, A.; Sloan, S. Filling the Gap: Facial Anatomy and Safe Lower Lip Injection Practices. J. Clin. Med. 2025, 14, 3214. https://doi.org/10.3390/jcm14093214
Swancutt MM, Allard AJ, Ho A, Sloan S. Filling the Gap: Facial Anatomy and Safe Lower Lip Injection Practices. Journal of Clinical Medicine. 2025; 14(9):3214. https://doi.org/10.3390/jcm14093214
Chicago/Turabian StyleSwancutt, Makayla M., Aaron J. Allard, Alex Ho, and Sara Sloan. 2025. "Filling the Gap: Facial Anatomy and Safe Lower Lip Injection Practices" Journal of Clinical Medicine 14, no. 9: 3214. https://doi.org/10.3390/jcm14093214
APA StyleSwancutt, M. M., Allard, A. J., Ho, A., & Sloan, S. (2025). Filling the Gap: Facial Anatomy and Safe Lower Lip Injection Practices. Journal of Clinical Medicine, 14(9), 3214. https://doi.org/10.3390/jcm14093214