
Paradigm Shift in Inflammatory Bowel Disease Management: Precision Medicine, Artificial Intelligence, and Emerging Therapies




Abstract
1. Introduction
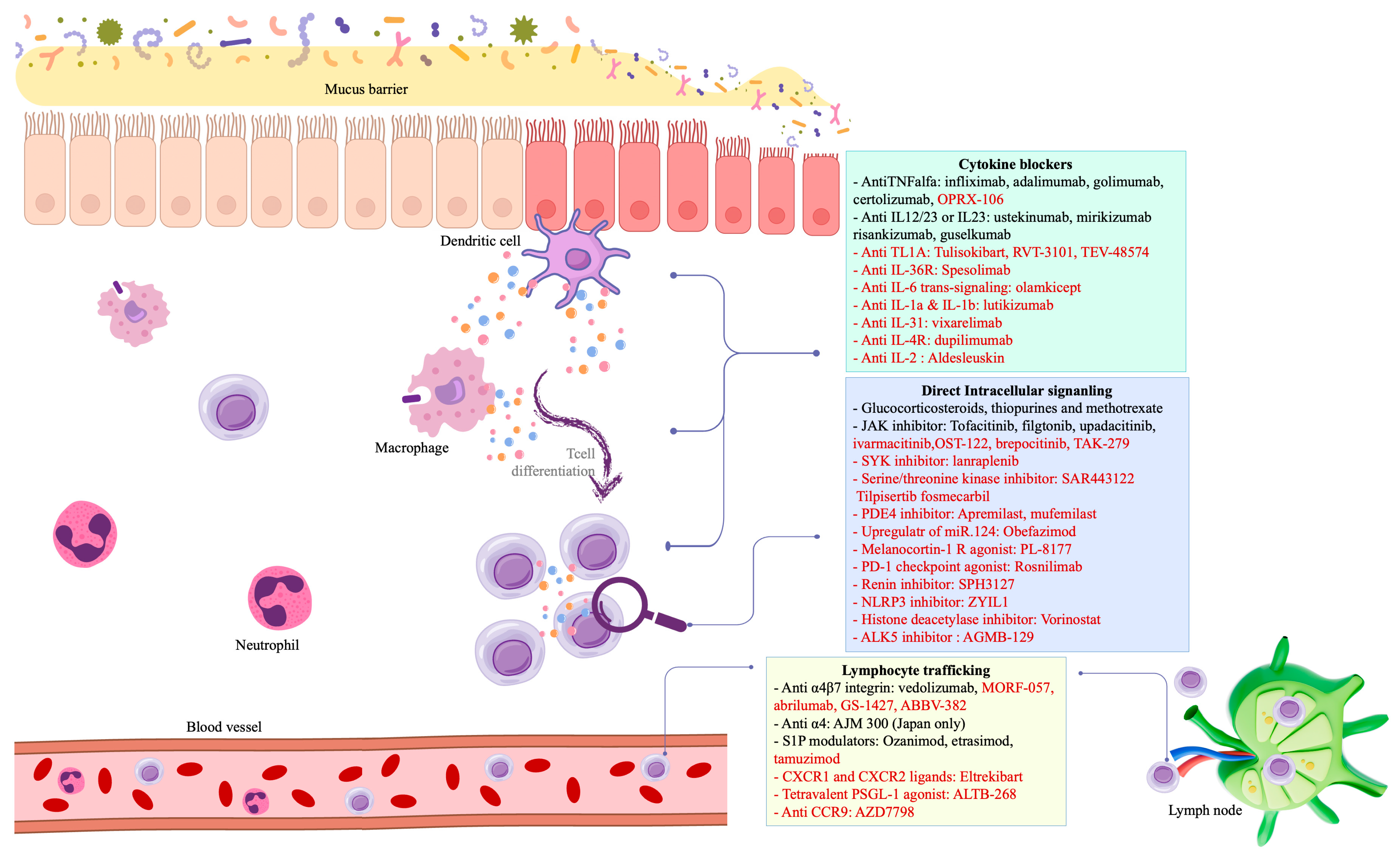
2. Novel Therapies and Emerging Targets
3. The Rise of Precision Medicine in IBD Management
4. Navigating the Financial Landscape of IBD Management
5. Ensuring Safety in IBD Treatment
6. Limitations and Future Directions
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| IBD | Inflammatory Bowel Disease |
| CD | Crohn’s Disease |
| UC | Ulcerative Colitis |
| TNF | Tumor Necrosis Factor |
| IL | Interleukin |
| JAK | Janus Kinase |
| S1P | Sphingosine-1-Phosphate |
| PDE | Phosphodiesterase |
| SYK | Spleen Tyrosine Kinase |
| TLR | Toll-Like Receptor |
| miRNA | MicroRNA |
| GWAS | Genome-Wide Association Studies |
| WES | Whole-Exome Sequencing |
| AI | Artificial Intelligence |
| CNN | Convolutional Neural Network |
| UCEIS | Ulcerative Colitis Endoscopic Index of Severity |
| EMA | European Medicines Agency |
| FDA | Food and Drug Administration |
| MAdCAM-1 | Mucosal Addressin Cell Adhesion Molecule-1 |
| CAR-T | Chimeric Antigen Receptor T-cell Therapy |
| PDE4 | Phosphodiesterase-4 |
| ALK5 | Activin-like Kinase 5 |
| PSGL-1 | P-Selectin Glycoprotein Ligand-1 |
| NLRP3 | NOD-, LRR-, and pyrin domain-containing protein 3 |
| RIPK1/2 | Receptor-Interacting Protein Kinase 1/2 |
| CXCR1/2 | C-X-C Motif Chemokine Receptor 1/2 |
| HDACi | Histone Deacetylase Inhibitor |
| CCR9 | C-C Motif Chemokine Receptor 9 |
| TYK2 | Tyrosine Kinase 2 |
| PD-1 | Programmed Death-1 |
| IPAA | Ileal Pouch-Anal Anastomosis |
| cAMP | Cyclic Adenosine Monophosphate |
| CREB | cAMP Response Element-Binding Protein |
| Treg | Regulatory T Cells |
| APC | Antigen-Presenting Cell |
References
- Feuerstein, J.D.; Cheifetz, A.S. Crohn Disease: Epidemiology, Diagnosis, and Management. Mayo Clin. Proc. 2017, 92, 1088–1103. [Google Scholar] [CrossRef] [PubMed]
- Jagirdhar, G.S.K.; Perez, J.A.; Perez, A.B.; Surani, S. Integration and implementation of precision medicine in the multifaceted inflammatory bowel disease. World J. Gastroenterol. 2023, 29, 5211–5225. [Google Scholar] [CrossRef] [PubMed]
- Zheng, D.Y.; Wang, Y.N.; Huang, Y.H.; Jiang, M.; Dai, C. Effectiveness and safety of upadacitinib for inflammatory bowel disease: A systematic review and meta-analysis of RCT and real-world observational studies. Int. Immunopharmacol. 2024, 126, 111229. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.M.; Loftus, E.V., Jr. Risankizumab to treat moderately to severely active Crohn’s disease in adults: An evaluation of trials and data. Expert. Rev. Gastroenterol. Hepatol. 2023, 17, 1169–1183. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Yassin, N.; Marley, A.; Bellato, V.; Foppa, C.; Pellino, G.; Myrelid, P.; Millan, M.; Gros, B.; Avellaneda, N.; et al. Crossing barriers: The burden of inflammatory bowel disease across Western Europe. Ther. Adv. Gastroenterol. 2023, 16, 17562848231218615. [Google Scholar] [CrossRef]
- Bretto, E.; Ribaldone, D.G.; Caviglia, G.P.; Saracco, G.M.; Bugianesi, E.; Frara, S. Inflammatory Bowel Disease: Emerging Therapies and Future Treatment Strategies. Biomedicines 2023, 11, 2249. [Google Scholar] [CrossRef]
- Neurath, M.F. Strategies for targeting cytokines in inflammatory bowel disease. Nat. Rev. Immunol. 2024, 24, 559–576. [Google Scholar] [CrossRef]
- Vuyyuru, S.K.; Shackelton, L.M.; Hanzel, J.; Ma, C.; Jairath, V.; Feagan, B.G. Targeting IL-23 for IBD: Rationale and Progress to Date. Drugs 2023, 83, 873–891. [Google Scholar] [CrossRef]
- Moschen, A.R.; Tilg, H.; Raine, T. IL-12, IL-23 and IL-17 in IBD: Immunobiology and therapeutic targeting. Nat. Rev. Gastroenterol. Hepatol. 2018, 16, 185–196. [Google Scholar] [CrossRef]
- Parigi, T.L.; Iacucci, M.; Ghosh, S. Blockade of IL-23: What is in the Pipeline? J. Crohn’s Colitis 2022, 16, ii64–ii72. [Google Scholar] [CrossRef]
- Ferrante, M.; Irving, P.M.; Selinger, C.P.; D’haens, G.; Kuehbacher, T.; Seidler, U.; Gropper, S.; Haeufel, T.; Forgia, S.; Danese, S.; et al. Safety and tolerability of spesolimab in patients with ulcerative colitis. Expert Opin. Drug Saf. 2022, 22, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, S.; Aden, K.; Bernardes, J.P.; Conrad, C.; Tran, F.; Höper, H.; Volk, V.; Mishra, N.; Blase, J.I.; Nikolaus, S.; et al. Therapeutic Interleukin-6 Trans-signaling Inhibition by Olamkicept (sgp130Fc) in Patients with Active Inflammatory Bowel Disease. Gastroenterology 2021, 160, 2354–2366.e11. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Chen, B.; Wang, B.; Chen, H.; Li, Y.; Cao, Q.; Zhong, J.; Shieh, M.J.; Ran, Z.; Tang, T.; et al. Effect of Induction Therapy with Olamkicept vs Placebo on Clinical Response in Patients with Active Ulcerative Colitis: A Randomized Clinical Trial. JAMA 2023, 329, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; He, C.; Xin, S.; Liu, X.; Zhang, S.; Qiao, B.; Shang, H.; Gao, L.; Xu, J. A Deep View of the Biological Property of Interleukin-33 and Its Dysfunction in the Gut. Int. J. Mol. Sci. 2023, 24, 13504. [Google Scholar] [CrossRef]
- Cao, Z.; Li, Y.; Wang, W.; Jie, S.; Hu, X.; Zhou, J.; Wu, T.; Aili, D.; Long, Z.; Li, Y.; et al. Is Lutikizumab, an Anti-Interleukin-1α/β Dual Variable Domain Immunoglobulin, efficacious for Osteoarthritis? Results from a bayesian network meta-analysis. BioMed Res. Int. 2020, 2020, 9013283. [Google Scholar] [CrossRef]
- Furfaro, F.; Alfarone, L.; Gilardi, D.; Correale, C.; Allocca, M.; Fiorino, G.; Argollo, M.; Zilli, A.; Zacharopoulou, E.; Loy, L.; et al. TL1A: A New Potential Target in the Treatment of Inflammatory Bowel Disease. Curr. Drug Targets 2021, 22, 760–769. [Google Scholar] [CrossRef]
- Danese, S.; Klopocka, M.; Scherl, E.J.; Romatowski, J.; Allegretti, J.R.; Peeva, E.; Vincent, M.S.; Schoenbeck, U.; Ye, Z.; Hassan-Zahraee, M.; et al. Anti-TL1A Antibody PF-06480605 Safety and Efficacy for Ulcerative Colitis: A Phase 2a Single-Arm Study. Clin. Gastroenterol. Hepatol. 2021, 19, 2324–2332.e6. [Google Scholar] [CrossRef]
- Feagan, B.G.; Sands, B.; Siegel, C.A.; Dubinsky, M.; Longman, R.; Sabinho, J.; Laurent, O.O.; Luo, A.A.; Lu, J.D.; Nguyen, D.; et al. DOP87 The Anti-TL1AAntibody PRA023 Demonstrated Proof-of-Concept in Crohn’s Disease: Phase 2a APOLLO-CDStudy Results. J. Crohn’s Colitis 2023, 17, i162–i164. [Google Scholar] [CrossRef]
- Almon, E.; Shaaltiel, Y.; Sbeit, W.; Fich, A.; Schwartz, D.; Waterman, M.; Szlaifer, M.; Reuveni, H.; Amit-Cohen, B.C.; Alon, S.; et al. Novel Orally Administered Recombinant Anti-TNF Alpha Fusion Protein for the Treatment of Ulcerative Colitis: Results from a Phase 2a Clinical Trial. J. Clin. Gastroenterol. 2021, 55, 134–140. [Google Scholar] [CrossRef]
- A Six Week Efficacy, Safety and Tolerability Study of V565 in Crohn’s Disease—Full Text View—ClinicalTrials. Available online: https://clinicaltrials.gov/ct2/show/NCT02976129 (accessed on 15 January 2024).
- Denesh, D.; Carbonell, J.; Kane, J.S.; Gracie, D.; Selinger, C.P. Patients with inflammatory bowel disease (IBD) prefer oral tablets over other modes of medicine administration. Expert. Rev. Gastroenterol. Hepatol. 2021, 15, 1091–1096. [Google Scholar] [CrossRef]
- Myers, J.; Nguyen, S.; Patel, N.; Imran, M.; Hashim, M.A.; Dhalla, A.K. An orally administered robotic pill (RP) reliably and safely delivers an ustekinumab biosimilar with high bioavailability relative to subcutaneous (SC) ustekinumab in healthy human participants. Gastroenterology 2024, 166 (Suppl. S5), 492b–492c. [Google Scholar] [CrossRef]
- Bissonnette, R.; Pinter, A.; Ferris, L.K.; Gerdes, S.; Rich, P.; Vender, R.; Miller, M.; Shen, Y.K.; Kannan, A.; Li, S.; et al. An Oral Interleukin-23-Receptor Antagonist Peptide for Plaque Psoriasis. N. Engl. J. Med. 2024, 390, 510–521. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, K.; Watanabe, M.; Ohmori, T.; Nakajima, K.; Ishida, T.; Ishiguro, Y.; Kanke, K.; Kobayashi, K.; Hirai, F.; Watanabe, K.; et al. AJM300 Study Group. AJM300 (carotegrast methyl), an oral antagonist of α4-integrin, as induction therapy for patients with moderately active ulcerative colitis: A multicentre, randomised, double-blind, placebo-controlled, phase 3 study. Lancet Gastroenterol. Hepatol. 2022, 7, 648–657. [Google Scholar] [CrossRef] [PubMed]
- D’Haens, G.R.; Reinisch, W.; Lee, S.D.; Tarabar, D.; Louis, E.; Kłopocka, M.; Klaus, J.; Schreiber, S.; Park, D.I.; Hébuterne, X.; et al. Long-Term Safety and Efficacy of the Anti-Mucosal Addressin Cell Adhesion Molecule-1 Monoclonal Antibody Ontamalimab (SHP647) for the Treatment of Crohn’s Disease: The OPERA II Study. Inflamm. Bowel Dis. 2022, 28, 1034–1044. [Google Scholar] [CrossRef]
- Hibi, T.; Motoya, S.; Ashida, T.; Sai, S.; Sameshima, Y.; Nakamura, S.; Maemoto, A.; Nii, M.; Sullivan, B.A.; Gasser, R.A., Jr.; et al. Efficacy and safety of abrilumab, an 4 7 integrin inhibitor, in Japanese patients with moderate-to-severe ulcerative colitis: A phase II study. Intest. Res. 2019, 17, 375–386. [Google Scholar] [CrossRef]
- Kitsou, K.; Kokkotis, G.; Rivera-Nieves, J.; Bamias, G. Targeting the Sphingosine-1-Phosphate Pathway: New Opportunities in Inflammatory Bowel Disease Management. Drugs 2024, 84, 1179–1197. [Google Scholar] [CrossRef]
- Danese, S.; Panaccione, R.; Abreu, M.T.; Rubin, D.T.; Ghosh, S.; Dignass, A.; Afzali, A.; Wolf, D.C.; Chiorean, M.V.; Vermeire, S.; et al. Efficacy and Safety of Approximately 3 Years of Continuous Ozanimod in Moderately to Severely Active Ulcerative Colitis: Interim Analysis of the True North Open-label Extension. J. Crohn’s Colitis 2024, 18, 264–274. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Vermeire, S.; Peyrin-Biroulet, L.; Dubinsky, M.C.; Panes, J.; Yarur, A.; Ritter, T.; Baert, F.; Schreiber, S.; Sloan, S.; et al. Etrasimod as induction and maintenance therapy for ulcerative colitis (ELEVATE): Two randomised, double-blind, placebo-controlled, phase 3 studies. Lancet 2023, 401, 1159–1171, Erratum in Lancet 2023, 401, 1000. [Google Scholar] [CrossRef] [PubMed]
- Saba, J.; Degagne, E. S1pping fire: Sphingosine-1-phosphate signaling as an emerging target in inflammatory bowel disease and colitis-associated cancer. Clin. Exp. Gastroenterol. 2014, 7, 205–214. [Google Scholar] [CrossRef]
- Peyrin-Biroulet, L.; Dubinsky, M.C.; Sands, B.E.; Panés, J.; Schreiber, S.; Reinisch, W.; Feagan, B.G.; Danese, S.; Yarur, A.J.; D’Haens, G.R.; et al. Efficacy and Safety of Etrasimod in Patients with Moderately to Severely Active Isolated Proctitis: Results From the Phase 3 ELEVATE UC Clinical Programme. J. Crohn’s Colitis 2024, 18, 1270–1282, Erratum in J. Crohns Colitis 2024, 18, 1356. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Caballero-Mateos, A.M.; Cañadas-de la Fuente, G.A. Game changer: How Janus kinase inhibitors are reshaping the landscape of ulcerative colitis management. World J. Gastroenterol. 2024, 30, 3942–3953. [Google Scholar] [CrossRef] [PubMed]
- Sandborn, W.J.; Su, C.; Sands, B.E.; D’Haens, G.R.; Vermeire, S.; Schreiber, S.; Danese, S.; Feagan, B.G.; Reinisch, W.; Niezychowski, W.; et al. OCTAVE Induction 1, OCTAVE Induction 2, and OCTAVE Sustain Investigators. Tofacitinib as Induction and Maintenance Therapy for Ulcerative Colitis. N. Engl. J. Med. 2017, 376, 1723–1736. [Google Scholar] [CrossRef] [PubMed]
- Feagan, B.G.; Danese, S.; Loftus, E.V., Jr.; Vermeire, S.; Schreiber, S.; Ritter, T.; Fogel, R.; Mehta, R.; Nijhawan, S.; Kempiński, R.; et al. Filgotinib as induction and maintenance therapy for ulcerative colitis (SELECTION): A phase 2b/3 double-blind, randomised, placebo-controlled trial. Lancet 2021, 397, 2372–2384. [Google Scholar] [CrossRef] [PubMed]
- Danese, S.; Vermeire, S.; Zhou, W.; Pangan, A.L.; Siffledeen, J.; Greenbloom, S.; Hébuterne, X.; D’Haens, G.; Nakase, H.; Panés, J.; et al. Upadacitinib as induction and maintenance therapy for moderately to severely active ulcerative colitis: Results from three phase 3, multicentre, double-blind, randomised trials. Lancet 2022, 399, 2113–2128. [Google Scholar] [CrossRef]
- Hardwick, R.N.; Brassil, P.; Badagnani, I.; Perkins, K.; Obedencio, G.P.; Kim, A.S.; Conner, M.W.; Bourdet, D.L.; Harstad, E.B. Gut-Selective Design of Orally Administered Izencitinib (TD-1473) Limits Systemic Exposure and Effects of Janus Kinase Inhibition in Nonclinical Species. Toxicol. Sci. 2022, 186, 323–337. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chen, B.; Zhong, J.; Li, X.; Pan, F.; Ding, Y.; Zhang, Y.; Chen, H.; Liu, F.; Zhang, Z.; Zhang, L.; et al. Efficacy and Safety of Ivarmacitinib in Patients with Moderate-to-Severe, Active, Ulcerative Colitis: A Phase II Study. Gastroenterology 2022, 163, 1555–1568. [Google Scholar] [CrossRef]
- Sands, B.E.; Sandborn, W.J.; Feagan, B.G.; Lichtenstein, G.R.; Zhang, H.; Strauss, R.; Szapary, P.; Johanns, J.; Panes, J.; Vermeire, S.; et al. Peficitinib-UC Study Group. Peficitinib, an Oral Janus Kinase Inhibitor, in Moderate-to-severe Ulcerative Colitis: Results from a Randomised, Phase 2 Study. J. Crohn’s Colitis. 2018, 12, 1158–1169. [Google Scholar] [CrossRef] [PubMed]
- Atreya, R.; Reinisch, W.; Peyrin-Biroulet, L.; Scaldaferri, F.; Admyre, C.; Knittel, T.; Kowalski, J.; Neurath, M.F.; Hawkey, C. Clinical efficacy of the Toll-like receptor 9 agonist cobitolimod using patient-reported-outcomes defined clinical endpoints in patients with ulcerative colitis. Dig. Liver Dis. 2018, 50, 1019–1029. [Google Scholar] [CrossRef]
- Atreya, R.; Peyrin-Biroulet, L.; Klymenko, A.; Augustyn, M.; Bakulin, I.; Slankamenac, D.; Miheller, P.; Gasbarrini, A.; Hébuterne, X.; Arnesson, K.; et al. Cobitolimod for moderate-to-severe, left-sided ulcerative colitis (CONDUCT): A phase 2b randomised, double-blind, placebo-controlled, dose-ranging induction trial. Lancet Gastroenterol. Hepatol. 2020, 5, 1063–1075. [Google Scholar] [CrossRef]
- AlAmeel, T.; AlMutairdi, A.; Al-Bawardy, B. Emerging Therapies for Ulcerative Colitis: Updates from Recent Clinical Trials. Clin. Exp. Gastroenterol. 2023, 16, 147–167. [Google Scholar] [CrossRef]
- Danese, S.; Neurath, M.F.; Kopoń, A.; Zakko, S.F.; Simmons, T.C.; Fogel, R.; Siegel, C.A.; Panaccione, R.; Zhan, X.; Usiskin, K.; et al. Effects of Apremilast, an Oral Inhibitor of Phosphodiesterase 4, in a Randomized Trial of Patients with Active Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2020, 18, 2526–2534.e9. [Google Scholar] [CrossRef] [PubMed]
- Apolit, C.; Campos, N.; Vautrin, A.; Begon-Pescia, C.; Lapasset, L.; Scherrer, D.; Gineste, P.; Ehrlich, H.; Garcel, A.; Santo, J.; et al. ABX464 (Obefazimod) Upregulates miR-124 to Reduce Proinflammatory Markers in Inflammatory Bowel Diseases. Clin. Transl. Gastroenterol. 2023, 14, e00560. [Google Scholar] [CrossRef] [PubMed]
- Blomgren, P.; Chandrasekhar, J.; Di Paolo, J.A.; Fung, W.; Geng, G.; Ip, C.; Jones, R.; Kropf, J.E.; Lansdon, E.B.; Lee, S.; et al. Discovery of Lanraplenib (GS-9876): A Once-Daily Spleen Tyrosine Kinase Inhibitor for Autoimmune Diseases. ACS Med. Chem. Lett. 2020, 11, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Honjo, H.; Watanabe, T.; Kamata, K.; Minaga, K.; Kudo, M. RIPK2 as a New Therapeutic Target in Inflammatory Bowel Diseases. Front. Pharmacol. 2021, 12, 650403. [Google Scholar] [CrossRef]
- Luu, K.; Dahl, M.; Hare, E.; Sibley, C.; Lizzul, P.; Randazzo, B. DOP81 Rosnilimab, a novel PD-1 agonist monoclonal antibody, reduces T cell proliferation, inflammatory cytokine secretion, and PD-1high expressing CD4 and CD8 T cells: Results from a Phase 1 healthy volunteer clinical trial. J. Crohn’s Colitis 2024, 18 (Suppl. S1), i226. [Google Scholar] [CrossRef]
- Salmenkari, H.; Korpela, R.; Vapaatalo, H. Renin-angiotensin system in intestinal inflammation-Angiotensin inhibitors to treat inflammatory bowel diseases? Basic Clin. Pharmacol. Toxicol. 2021, 129, 161–172. [Google Scholar] [CrossRef]
- Xv, Y.; Feng, Y.; Lin, J. CXCR1 and CXCR2 are potential neutrophil extracellular trap-related treatment targets in ulcerative colitis: Insights from Mendelian randomization, colocalization and transcriptomic analysis. Front. Immunol. 2024, 15, 1425363. [Google Scholar] [CrossRef]
- Parmar, D.V.; Kansagra, K.A.; Momin, T.; Patel, H.B.; Jansari, G.A.; Bhavsar, J.; Shah, C.; Patel, J.M.; Ghoghari, A.; Barot, A.; et al. Safety, Tolerability, Pharmacokinetics, and Pharmacodynamics of the Oral NLRP3 Inflammasome Inhibitor ZYIL1: First-in-Human Phase 1 Studies (Single Ascending Dose and Multiple Ascending Dose). Clin. Pharmacol. Drug Dev. 2023, 12, 202–211. [Google Scholar] [CrossRef]
- Ambrus-Aikelin, G.; Takeda, K.; Joetham, A.; Lazic, M.; Povero, D.; Santini, A.M.; Pranadinata, R.; Johnson, C.D.; McGeough, M.D.; Beasley, F.C.; et al. JT002, a small molecule inhibitor of the NLRP3 inflammasome for the treatment of autoinflammatory disorders. Sci. Rep. 2023, 13, 13524, Erratum in Sci. Rep. 2023, 13, 20081. [Google Scholar] [CrossRef]
- Vermeire, S.; Dewint, P.; Vansteelant, M.; Peterka, M.; Štěpek, D.; Kierkuś, J.; Wiernicka, A.; Napora, P.; Wolański, Ł.; Kopoń, A.; et al. P658 Safety and efficacy of MH002, an optimized live biotherapeutic product, for the treatment of mild to moderate ulcerative colitis: A first-in-disease, double-blind, randomized clinical trial. J. Crohn’s Colitis 2024, 18 (Suppl. S1), i1254. [Google Scholar] [CrossRef]
- Kwak, M.S.; Hwang, C.-I.; Cha, J.M.; Jeon, J.W.; Yoon, J.Y.; Park, S.B. Single-Cell Network-Based Drug Repositioning for Discovery of Therapies against Anti-Tumour Necrosis Factor-Resistant Crohn’s Disease. Int. J. Mol. Sci. 2023, 24, 14099. [Google Scholar] [CrossRef] [PubMed]
- Pala, D.; Ronchi, P.; Rescigno, D.; Bertani, B.; Capelli, A.M.; Guariento, S.; Marchini, G.; Milioli, M.; Cesari, N.; Federico, G.; et al. Design, Synthesis, and Activity of a Novel Series of Pyridazine-Based ALK5 Inhibitors. ACS Med. Chem. Lett. 2024, 15, 1925–1932. [Google Scholar] [CrossRef] [PubMed]
- A Bemelman, W.; Collaborators, S.-E.; Adamina, M.; Buskens, C.; Dhoore, A.; Kotze, P.G.; Oresland, T.; Panis, Y.; Samprieto, G.; Spinelli, A.; et al. Evolving role of IBD surgery. J. Crohn’s Colitis 2018, 12, 1005–1007. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, A.; Bonovas, S.; Burisch, J.; Kucharzik, T.; Adamina, M.; Annese, V.; Bachmann, O.; Bettenworth, D.; Chaparro, M.; Czuber-Dochan, W.; et al. ECCO guidelines on therapeutics in ulcerative colitis: Surgical treatment. J. Crohn’s Colitis 2022, 16, 179–189. [Google Scholar] [CrossRef]
- Bettenworth, D.; Gustavsson, A.; Atreja, A.; Lopez, R.; Tysk, C.; van Assche, G.; Rieder, F. A pooled analysis of efficacy, safety, and long-term outcome of endoscopic balloon dilation therapy for patients with stricturing Crohn’s disease. Inflamm. Bowel Dis. 2017, 23, 133–142. [Google Scholar] [CrossRef]
- Vieujean, S.; Jairath, V.; Peyrin-Biroulet, L.; Dubinsky, M.; Iacucci, M.; Magro, F.; Danese, S. Understanding the therapeutic toolkit for inflammatory bowel disease. Nat. Rev. Gastroenterol. Hepatol. 2025. [Google Scholar] [CrossRef]
- Uhlig, H.H.; Booth, C.; Cho, J.; Dubinsky, M.; Griffiths, A.M.; Grimbacher, B.; Hambleton, S.; Huang, Y.; Jones, K.; Kammermeier, J.; et al. Precision medicine in monogenic inflammatory bowel disease: Proposed mIBD REPORT standards. Nat. Rev. Gastroenterol. Hepatol. 2023, 20, 810–828. [Google Scholar] [CrossRef]
- Iacucci, M.; Santacroce, G.; Majumder, S.; Morael, J.; Zammarchi, I.; Maeda, Y.; Ryan, D.; Di Sabatino, A.; Rescigno, M.; Aburto, M.R.; et al. Opening the doors of precision medicine: Novel tools to assess intestinal barrier in inflammatory bowel disease and colitis-associated neoplasia. Gut 2024, 73, 1749–1762. [Google Scholar] [CrossRef]
- Cannarozzi, A.L.; Latiano, A.; Massimino, L.; Bossa, F.; Giuliani, F.; Riva, M.; Ungaro, F.; Guerra, M.; Brina, A.L.D.; Biscaglia, G.; et al. Inflammatory bowel disease genomics, transcriptomics, proteomics and metagenomics meet artificial intelligence. United Eur. Gastroenterol. J. 2024, 12, 1461–1480. [Google Scholar] [CrossRef]
- D’Addabbo, A.; Latiano, A.; Palmieri, O.; Maglietta, R.; Annese, V.; Ancona, N. Regularized least squares classifiers may predict Crohn’s disease from profiles of single nucleotide polymorphisms. Ann. Hum. Genet. 2007, 71, 537–549. [Google Scholar] [CrossRef]
- Zhang, L.; Mao, R.; Lau, C.T.; Chung, W.C.; Chan, J.C.P.; Liang, F.; Zhao, C.; Zhang, X.; Bian, Z. Identification of useful genes from multiple microarrays for ulcerative colitis diagnosis based on machine learning methods. Sci. Rep. 2022, 12, 9962. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Zhang, M.; Ye, Z.; Wang, Y.; Wang, X.; Chen, Y.-G. Development of a 32-gene signature using machine learning for accurate prediction of inflammatory bowel disease. Cell Regen. 2023, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.C.; Chang, C.; Boschetti, G.; Ungaro, R.; Giri, M.; Grout, J.A.; Gettler, K.; Chuang, L.-S.; Nayar, S.; Greenstein, A.J.; et al. Single-cell analysis of Crohn’s disease lesions identifies a pathogenic cellular module associated with resistance to anti-TNF therapy. Cell 2019, 178, 1493–1508.e20. [Google Scholar] [CrossRef] [PubMed]
- Abreu, M.T.; Davies, J.M.; A Quintero, M.; Delmas, A.; Diaz, S.; Martinez, C.D.; Venables, T.; Reich, A.; Crynen, G.; Deshpande, A.R.; et al. Transcriptional behavior of regulatory T cells predicts IBD patient responses to vedolizumab therapy. Inflamm. Bowel Dis. 2022, 28, 1800–1812. [Google Scholar] [CrossRef]
- Boardman, D.A.; Wong, M.Q.; Rees, W.D.; Wu, D.; Himmel, M.E.; Orban, P.C.; Vent-Schmidt, J.; Zachos, N.C.; Steiner, T.S.; Levings, M.K. Levings, Flagellin-specific human CAR Tregs for immune regulation in IBD. J. Autoimmun. 2023, 134, 102961. [Google Scholar] [CrossRef]
- Manandhar, I.; Alimadadi, A.; Aryal, S.; Munroe, P.B.; Joe, B.; Cheng, X. Gut microbiome-based supervised machine learning for clinical diagnosis of inflammatory bowel diseases. Am. J. Physiol. Gastrointest. Liver Physiol. 2021, 320, G328–G337. [Google Scholar] [CrossRef]
- Cannarozzi, A.L.; Massimino, L.; Latiano, A.; Parigi, T.L.; Giuliani, F.; Bossa, F.; Di Brina, A.L.; Ungaro, F.; Biscaglia, G.; Danese, S.; et al. Artificial intelligence: A new tool in the pathologist’s armamentarium for the diagnosis of IBD. Comput. Struct. Biotechnol. J. 2024, 23, 3407–3417. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cai, C.; Shi, Q.; Li, J.; Jiao, Y.; Xu, A.; Zhou, Y.; Wang, X.; Peng, C.; Zhang, X.; Cui, X.; et al. Pathologist-level diagnosis of ulcerative colitis inflammatory activity level using an automated histological grading method. Int. J. Med. Inform. 2024, 192, 105648. [Google Scholar] [CrossRef] [PubMed]
- Omori, T.; Yamamoto, T.; Murasugi, S.; Koroku, M.; Yonezawa, M.; Nonaka, K.; Nagashima, Y.; Nakamura, S.; Tokushige, K. Comparison of Endoscopic and Artificial Intelligence Diagnoses for Predicting the Histological Healing of Ulcerative Colitis in a Real-World Clinical Setting. Crohns Colitis 360 2024, 6, otae005. [Google Scholar] [CrossRef]
- Ruan, G.; Qi, J.; Cheng, Y.; Liu, R.; Zhang, B.; Zhi, M.; Chen, J.; Xiao, F.; Shen, X.; Fan, L.; et al. Development and Validation of a Deep Neural Network for Accurate Identification of Endoscopic Images from Patients with Ulcerative Colitis and Crohn’s Disease. Front. Med. 2022, 9, 854677. [Google Scholar] [CrossRef]
- Marin-Santos, D.; Contreras-Fernandez, J.A.; Perez-Borrero, I.; Pallares-Manrique, H.; Gegundez-Arias, M.E. Automatic detection of crohn disease in wireless capsule endoscopic images using a deep convolutional neural network. Appl. Intell. 2023, 53, 12632–12646. [Google Scholar] [CrossRef]
- Wang, C.; Li, S.; Lin, N.; Zhang, X.; Han, Y.; Wang, X.; Liu, D.; Tan, X.; Pu, D.; Li, K.; et al. Application of Large Language Models in Medical Training Evaluation-Using ChatGPT as a Standardized Patient: Multimetric Assessment. J. Med. Internet Res. 2025, 27, e59435. [Google Scholar] [CrossRef]
- Sciberras, M.; Farrugia, Y.; Gordon, H.; Furfaro, F.; Allocca, M.; Torres, J.; Arebi, N.; Fiorino, G.; Iacucci, M.; Verstockt, B.; et al. Accuracy of Information given by ChatGPT for Patients with Inflammatory Bowel Disease in Relation to ECCO Guidelines. J. Crohn’s Colitis 2024, 18, 1215–1221. [Google Scholar] [CrossRef] [PubMed]
- Murthy, S.K.; Weizman, A.V.; Kuenzig, M.E.; Windsor, J.W.; Kaplan, G.G.; Benchimol, E.I.; Bernstein, C.N.; Bitton, A.; Coward, S.; Jones, J.L.; et al. The 2023 Impact of Inflammatory Bowel Disease in Canada: Treatment Landscape. J. Can. Assoc. Gastroenterol. 2023, 6 (Suppl. S2), S97–S110. [Google Scholar] [CrossRef] [PubMed]
- Catalán-Serra, I.; Ricanek, P.; Grimstad, T. “Out of the box” new therapeutic strategies for Crohn’s disease: Moving beyond biologics. Rev. Esp. Enferm. Dig. 2023, 115, 614–634. [Google Scholar] [CrossRef] [PubMed]
- Saruta, M.; Kawaguchi, I.; Ogawa, Y.; Sanchez Gonzalez, Y.; Numajiri, N.; Tang, X.; Miller, R. Assessing the economics of biologic and small molecule therapies for the treatment of moderate to severe ulcerative colitis in Japan: A cost per responder analysis of upadacitinib. J. Med. Econ. 2024, 27, 566–574. [Google Scholar] [CrossRef]
- Burisch, J.; Vardi, H.; Schwartz, D.; Friger, M.; Kiudelis, G.; Kupčinskas, J.; Fumery, M.; Gower-Rousseau, C.; Lakatos, L.; Lakatos, P.L.; et al. Health-care costs of inflammatory bowel disease in a pan-European, community-based, inception cohort during 5 years of follow-up: A population-based study. Lancet Gastroenterol. Hepatol. 2020, 5, 454–464. [Google Scholar] [CrossRef]
- D’Amico, F.; Solitano, V.; Magro, F.; Olivera, P.A.; Halfvarson, J.; Rubin, D.; Dignass, A.; Al Awadhi, S.; Kobayashi, T.; Queiroz, N.S.F.; et al. Practical Management of Biosimilar Use in Inflammatory Bowel Disease (IBD): A Global Survey and an International Delphi Consensus. J. Clin. Medicine 2023, 12, 6350. [Google Scholar] [CrossRef]
- Jensen, T.B.; Kim, S.C.; Jimenez-Solem, E.; Bartels, D.; Christensen, H.R.; Andersen, J.T. Shift From Adalimumab Originator to Biosimilars in Denmark. JAMA Intern. Med. 2020, 180, 902–903. [Google Scholar] [CrossRef]
- Burisch, J.; Zhao, M.; Odes, S.; De Cruz, P.; Vermeire, S.; Bernstein, C.N.; Kaplan, G.G.; Duricova, D.; Greenberg, D.; Melberg, H.O.; et al. The cost of inflammatory bowel disease in high-income settings: A Lancet Gastroenterology & Hepatology Commission. Lancet Gastroenterol. Hepatol. 2023, 8, 458–492. [Google Scholar] [CrossRef]
- Caballero-Mateos, A.M. Gut Feelings: The Psychological Impact of Inflammatory Bowel Disease. J. Clin. Med. 2023, 12, 3867. [Google Scholar] [CrossRef] [PubMed]
- Burisch, J.; Claytor, J.; Hernandez, I.; Hou, J.K.; Kaplan, G.G. The Cost of Inflammatory Bowel Disease Care: How to Make it Sustainable. Clin. Gastroenterol. Hepatol. 2025, 23, 386–395. [Google Scholar] [CrossRef] [PubMed]
- Din, S.; Segal, J.; Blackwell, J.; Gros, B.; Black, C.J.; Ford, A.C. Harms with placebo in trials of biological therapies and small molecules as induction therapy in inflammatory bowel disease: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2024, 9, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- Chupin, A.; Perduca, V.; Meyer, A.; Bellanger, C.; Carbonnel, F.; Dong, C. Systematic review with meta-analysis: Comparative risk of lymphoma with anti-tumour necrosis factor agents and/or thiopurines in patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2020, 52, 1289–1297. [Google Scholar] [CrossRef]
- Marafini, I.; Troncone, E.; Rocchetti, I.; Monteleone, G. Respiratory tract infections in inflammatory bowel disease patients taking vedolizumab: A systematic review and meta-analysis of randomized controlled trials. Front. Pharmacol. 2020, 11, 585732. [Google Scholar] [CrossRef]
- Bhat, S.; Click, B.; Regueiro, M. Safety and Monitoring of Inflammatory Bowel Disease Advanced Therapies. Inflamm. Bowel Dis. 2024, 30, 829–843. [Google Scholar] [CrossRef]
- Fuller, M.K. Pediatric Inflammatory Bowel Disease: Special Considerations. Surg. Clin. N. Am. 2019, 99, 1177–1183. [Google Scholar] [CrossRef]
- Noel, D.D.; Marinella, P.; Mauro, G.; Tripodi, S.I.; Pin, A.; Serena, A.; Matteo, B.; Giuseppe, F.M.; Patrizia, A.; Stefano, C.; et al. Genetic Variants Assessing Crohn’s Disease Pattern in Pediatric Inflammatory Bowel Disease Patients by a Clinical Exome Survey. Bioinform. Biol. Insights 2021, 15, 11779322211055285. [Google Scholar] [CrossRef]
- Centanni, L.; Cicerone, C.; Fanizzi, F.; D’Amico, F.; Furfaro, F.; Zilli, A.; Parigi, T.L.; Peyrin-Biroulet, L.; Danese, S.; Allocca, M. Advancing Therapeutic Targets in IBD: Emerging Goals and Precision Medicine Approaches. Pharmaceuticals 2025, 18, 78. [Google Scholar] [CrossRef]
- Arnold, C. Autoimmune disease is the next frontier for CAR T cell therapy. Nat. Med. 2024, 30, 6–9. [Google Scholar] [CrossRef]
- Zhao, M.; Gönczi, L.; Lakatos, P.L.; Burisch, J. The Burden of Inflammatory Bowel Disease in Europe in 2020. J. Crohn’s Colitis 2021, 15, 1573–1587. [Google Scholar] [CrossRef] [PubMed]
- Oka, A.; Sartor, R.B. Microbial-Based and Microbial-Targeted Therapies for Inflammatory Bowel Diseases. Dig. Dis. Sci. 2020, 65, 757–788. [Google Scholar] [CrossRef] [PubMed]
- Caballero-Mateos, A.M. Methodological considerations and prevalence trends in disorders of gut-brain interaction: Lessons from comparative studies. Neurogastroenterol. Motil. 2023, 35, e14662. [Google Scholar] [CrossRef] [PubMed]
- Boldyreva, L.V.; Evtushenko, A.A.; Lvova, M.N.; Morozova, K.N.; Kiseleva, E.V. Underneath the Gut–Brain Axis in IBD—Evidence of the Non-Obvious. Int. J. Mol. Sci. 2024, 25, 12125. [Google Scholar] [CrossRef]
- Bar-Mashiah, A.S.; Mason, K.; Marsiglio, M.; Lukin, D.J. Forecasting IBD Activity Using Wearable Devices. Gastroenterology 2025. Online ahead of print. [Google Scholar] [CrossRef]

{kind=link}
| Drug | Mechanism of Action | Indication | Phase or Approval | Identification Number |
|---|---|---|---|---|
| Infliximab | Anti-TNFα | CD and UC | Approved by EMA and FDA | |
| Adalimumab | Anti-TNFα | CD and UC | Approved by EMA and FDA | |
| Certolizumab | Anti-TNFα | CD | Approved by FDA | |
| Golimumab | Anti-TNFα | UC | Approved by EMA and FDA | |
| Vedolizumab | Anti-α4β7 Integrin | CD and UC | Approved by EMA and FDA | |
| Ustekinumab | Anti-IL-12/23 | CD and UC | Approved by EMA and FDA | |
| Risankizumab | Anti-IL-23 | CD and UC | Approved by EMA and FDA | |
| Guselkumab | Anti-IL-23 | UC CD | Approved by FDA Ongoing phase 3 (GALAXI) | NCT05347095 NCT06408935 |
| Mirikizumab | Anti-IL-23 | UC CD | Approved by EMA and FDA Published phase 3 awaiting approval | NCT03926130 |
| Tofacitinib | JAK Inhibitor | UC | Approved by EMA and FDA | |
| Filgotinib | JAK Inhibitor | UC | Approved by EMA | |
| Upadacitinib | JAK Inhibitor | CD and UC | Approved by EMA and FDA | |
| Ozanimod | S1P Modulator | UC CD | Approved by EMA and FDA Ongoing Phase 3 | NCT03440385 NCT03440372 |
| Etrasimod | S1P Modulator | UC CD | Approved by EMA and FDA Ongoing Phase 3 | NCT04173273 |
| Tamuzimod (VTX 0002) | S1P Modulator | UC | Terminated Phase 2 | NCT05156125 |
| Spesolimab (BI 655130) | Anti IL-36R | UC CD | Ongoing Phase 2 Ongoing Phase 2 | NCT03482635 NCT03752970 |
| Olamkicept (TJ301) | Anti IL-6 trans-signaling | UC | Completed Phase 2 No phase 3 trial registered | NCT03235752 |
| Apremilast | PDE4 inhibitor | UC | Completed Phase 2 No phase 3 trial registered | NCT02289417 |
| Obefazimod (ABX464) | Upregulator of miR-124 | UC | Ongoing Phase 3 | NCT05507203 NCT05507216 |
| PL-8177 | Melanocortin-1 receptor agonist | UC | Ongoing Phase 2 | NCT05466890 |
| Lutikizumab | Anti IL-1a and IL-1b | UC CD | Ongoing Phase 2 Ongoing Phase 2 | NCT06257875 NCT06548542 |
| Vixarelimab | Anti IL-31 and oncostatin M | UC | Ongoing Phase 2 | NCT06137183 |
| Lanraplenib (BI 3032950) | Inhibition of spleen tyrosine kinase (SYK) | UC | Ongoing Phase 2 | NCT06636656 |
| Tilpisertib fosmecarbil (GS-5290) | Serine/threonine kinase inhibitor | UC | Ongoing Phase 2 | NCT06029972 |
| SAR443122 | serine/threonine protein kinase 1 | UC | Ongoing Phase 2 | NCT05588843 |
| Rosnilimab | PD-1 checkpoint agonist | UC | Ongoing Phase 2 | NCT06127043 |
| SPH3127 | Renin inhibitor | UC | Ongoing Phase 2 | NCT05019742 NCT05770609 |
| Eltrekibart (DB19017) | CXCR1 and CXCR2 ligands | UC | Ongoing Phase 2 in association with mirikizumab | NCT06598943 |
| ALTB-268 | Tetravalent PSGL-1 agonist antibody | UC | Ongoing Phase 2 | NCT06109441 |
| ZYIL1 | NLRP3 inflammasome inhibitor | UC | Ongoing Phase 2 | NCT06398808 |
| Dupilimumab | Anti IL-4R | UC | Ongoing Phase 2 | NCT05731128 |
| Mufemilast (Hemay005) | PDE4 inhibitor | UC | Ongoing Phase 2 | NCT05486104 |
| Vorinostat | Histone deacetylase inhibitor | CD | Ongoing phase 1/2(in combination with ustekinumab) | NCT03167437 |
| Aldesleuskin | IL-2 inhibitor | CD | Ongoing Phase 1/2 | NCT04263831 |
| AGMB-129 | ALK5 inhibitor | Fibrostenotic CD | Ongoing Phase 2 | NCT05843578 |
| AZD7798 | Anti CCR9 | CD | Ongoing Phase 2 | NCT06450197 |
| Abrilumab | Anti α4β7 integrin | UC | Completed Phase 2 No phase 3 trial registered | NCT01694485 |
| GS-1427 | Anti α4β7 integrin | UC | Ongoing Phase 2 | NCT06290934 |
| AJM-300 | Anti α4 | UC | Completed Phase 3 | NCT03531892 |
| ABBV-382 | Anti α4β7 integrin | CD | Ongoing Phase 2 | NCT06548542 |
| MORF-057 | Oral anti α4β7 | UC CD | Ongoing Phase 2 Ongoing Phase 2 | NCT05611671 NCT06226883 |
| Ontamalimab (PF-00547659) | Anti-MAdCAM-1 | CD and UC | Completed Phase 3 | NCT03259334 NCT03259308 NCT03290781 NCT03559517 NCT03566823 NCT03627091 |
| Tamuzimod | S1P modulator | UC | Ongoing Phase 2 | NCT05156125 |
| Ivarmacitinib | JAK inhibitor | CD UC | Completed Phase 2 Ongoing Phase 3 | NCT03677648 NCT05181137 |
| Brepocitinib | JAK inhibitor | UC | Completed Phase 2 No Phase 3 trial registered | NCT02958865 |
| OST-122 | JAK3/TYK2/ARK5 | UC | Completed Phase 1b/2a | NCT04353791 |
| Zasocitinib (previously TAK-279) | TYK2 inhibitor | UC CD | Ongoing Phase 2 Ongoing Phase 2 | NCT06254950 NCT06233461 |
| OPRX-106 | Anti TNF | UC | Completed Phase 2 No Phase 3 trial registered | NCT02768974 |
| RVT-3101 (previously PF-06480605) | Anti TL1A | UC | Ongoing phase 2b | NCT04090411 |
| Tulisokibart (MK-7240, previously known as PRA-023) | Anti TL1A | UC CD | Ongoing Phase 3 Ongoing Phase 3 | NCT06052059 NCT06651281 NCT06430801 |
| TEV-48574 | Anti TL1A | UC CD | Ongoing Phase 2 Ongoing Phase 2 | NCT05668013 NCT05499130 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caballero Mateos, A.M.; Cañadas de la Fuente, G.A.; Gros, B. Paradigm Shift in Inflammatory Bowel Disease Management: Precision Medicine, Artificial Intelligence, and Emerging Therapies. J. Clin. Med. 2025, 14, 1536. https://doi.org/10.3390/jcm14051536
Caballero Mateos AM, Cañadas de la Fuente GA, Gros B. Paradigm Shift in Inflammatory Bowel Disease Management: Precision Medicine, Artificial Intelligence, and Emerging Therapies. Journal of Clinical Medicine. 2025; 14(5):1536. https://doi.org/10.3390/jcm14051536
Chicago/Turabian StyleCaballero Mateos, Antonio M., Guillermo A. Cañadas de la Fuente, and Beatriz Gros. 2025. "Paradigm Shift in Inflammatory Bowel Disease Management: Precision Medicine, Artificial Intelligence, and Emerging Therapies" Journal of Clinical Medicine 14, no. 5: 1536. https://doi.org/10.3390/jcm14051536
APA StyleCaballero Mateos, A. M., Cañadas de la Fuente, G. A., & Gros, B. (2025). Paradigm Shift in Inflammatory Bowel Disease Management: Precision Medicine, Artificial Intelligence, and Emerging Therapies. Journal of Clinical Medicine, 14(5), 1536. https://doi.org/10.3390/jcm14051536