

One-Year Echocardiographic Follow-Up in Transthyretin Cardiac Amyloidosis: Impact of Tafamidis Treatment

 ,
,
Abstract
1. Introduction
2. Research Protocol and Methods
2.1. Study Population
2.2. Data Collected at Diagnosis
2.2.1. Clinical and Instrumental Data
2.2.2. Echocardiographic Data
2.2.3. Tafamidis Eligibility
2.2.4. Patient Follow-Up
2.3. Statistical Analyses
3. Results
3.1. Description of the Population at Baseline
3.2. Clinical Data
3.3. Echocardiographic Data
- Follow-Up Echocardiography
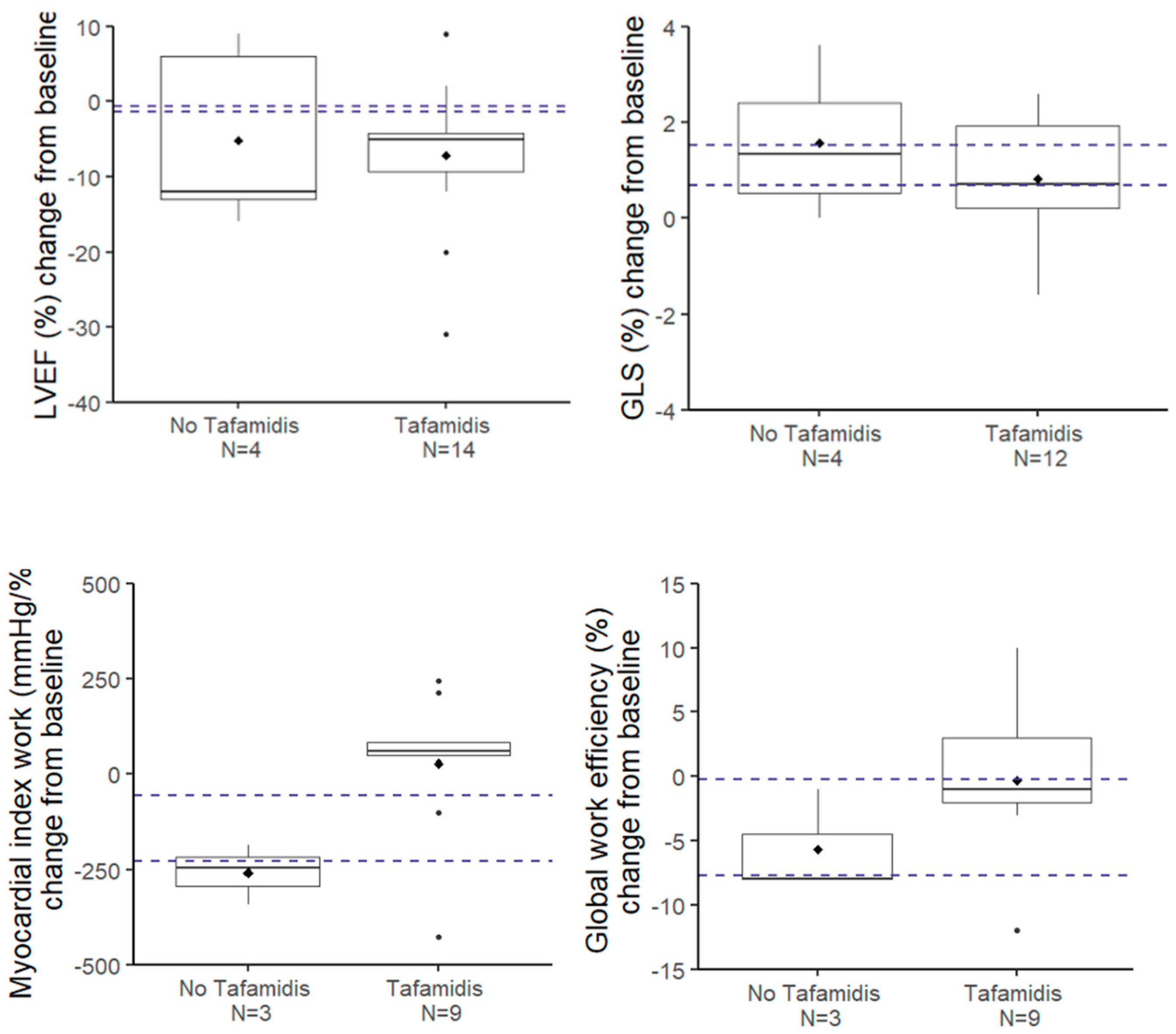
3.4. Evolution of LV Systolic Function Parameters
3.5. Comparison of Our Results with Reference Studies
3.6. Evolution of Other Echocardiographic Parameters
4. Discussion
4.1. Baseline Characteristics of Untreated and Treated Groups
4.2. Stability of Echocardiographic Parameters in Treated Patients
4.3. Safety Profile of Tafamidis Treatment
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aimo, A.; Merlo, M.; Porcari, A.; Georgiopoulos, G.; Pagura, L.; Vergaro, G.; Sinagra, G.; Emdin, M.; Rapezzi, C. Redefining the epidemiology of cardiac amyloidosis. A systematic review and meta-analysis of screening studies. Eur. J. Heart Fail. 2022, 24, 2342–2351. [Google Scholar] [CrossRef]
- Garcia-Pavia, P.; Sultan, M.B.; Gundapaneni, B.; Sekijima, Y.; Perfetto, F.; Hanna, M.; Witteles, R. Tafamidis Efficacy Among Octogenarian Patients in the Phase 3 ATTR-ACT and Ongoing Long-Term Extension Study. JACC Heart Fail. 2024, 12, 150–160. [Google Scholar] [CrossRef] [PubMed]
- de Marneffe, N.; Dulgheru, R.; Ancion, A.; Moonen, M.; Lancellotti, P. Cardiac amyloidosis: A review of the literature. Acta Cardiol. 2022, 77, 683–692. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Pavia, P.; Rapezzi, C.; Adler, Y.; Arad, M.; Basso, C.; Brucato, A.; Burazor, I.; Caforio, A.L.; Damy, T.; Eriksson, U.; et al. Diagnosis and treatment of cardiac amyloidosis: A position statement of the ESC Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2021, 42, 1554–1568. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Naharro, A.; Hawkins, P.N.; Fontana, M. Cardiac amyloidosis. Clin. Med. 2018, 18 (Suppl. 2), s30–s35. [Google Scholar] [CrossRef]
- Carroll, A.; Dyck, P.J.; de Carvalho, M.; Kennerson, M.; Reilly, M.M.; Kiernan, M.C.; Vucic, S. Novel approaches to diagnosis and management of hereditary transthyretin amyloidosis. J. Neurol. Neurosurg. Psychiatry 2022, 93, 668–678. [Google Scholar] [CrossRef]
- Maurer, M.S.; Schwartz, J.H.; Gundapaneni, B.; Elliott, P.M.; Merlini, G.; Waddington-Cruz, M.; Kristen, A.V.; Grogan, M.; Witteles, R.; Damy, T.; et al. Tafamidis Treatment for Patients with Transthyretin Amyloid Cardiomyopathy. N. Engl. J. Med. 2018, 379, 1007–1016. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.; Drachman, B.M.; Gottlieb, S.S.; Hoffman, J.E.; Hummel, S.L.; Lenihan, D.J.; Ebede, B.; Gundapaneni, B.; Li, B.; Sultan, M.B.; et al. Long-Term Survival with Tafamidis in Patients With Transthyretin Amyloid Cardiomyopathy. Circ. Heart Fail. 2022, 15, e008193. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Pavia, P.; Bengel, F.; Brito, D.; Damy, T.; Duca, F.; Dorbala, S.; Nativi-Nicolau, J.; Obici, L.; Rapezzi, C.; Sekijima, Y.; et al. Expert consensus on the monitoring of transthyretin amyloid cardiomyopathy. Eur. J. Heart Fail. 2021, 23, 895–905. [Google Scholar] [CrossRef]
- Ichikawa, Y.; Oota, E.; Odajima, S.; Kintsu, M.; Todo, S.; Takeuchi, K.; Yamauchi, Y.; Shiraki, H.; Yamashita, K.; Fukuda, T.; et al. Impact of Tafamidis on Echocardiographic Cardiac Function of Patients With Transthyretin Cardiac Amyloidosis. Circ. J. 2023, 87, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Giblin, G.T.; Cuddy, S.A.M.; González-López, E.; Sewell, A.; Murphy, A.; Dorbala, S.; Falk, R.H. Effect of tafamidis on global longitudinal strain and myocardial work in transthyretin cardiac amyloidosis. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 1029–1039. [Google Scholar] [CrossRef]
- Nishizawa, R.H.; Kawano, H.; Yoshimuta, T.; Eguchi, C.; Kojima, S.; Minami, T.; Sato, D.; Eguchi, M.; Okano, S.; Ikeda, S.; et al. Effects of tafamidis on the left ventricular and left atrial strain in patients with wild-type transthyretin cardiac amyloidosis. Eur. Heart J. Cardiovasc. Imaging 2024, 25, 678–686. [Google Scholar] [CrossRef] [PubMed]
- Tomasoni, D.; Bonfioli, G.B.; Aimo, A.; Adamo, M.; Canepa, M.; Inciardi, R.M.; Lombardi, C.M.; Nardi, M.; Pagnesi, M.; Riccardi, M.; et al. Treating amyloid transthyretin cardiomyopathy: Lessons learned from clinical trials. Front. Cardiovasc. Med. 2023, 10, 1154594. [Google Scholar] [CrossRef] [PubMed]
- Adams, D.; Gonzalez-Duarte, A.; O’Riordan, W.D.; Yang, C.C.; Ueda, M.; Kristen, A.V.; Tournev, I.; Schmidt, H.H.; Coelho, T.; Berk, J.L.; et al. Patisiran, an RNAi Therapeutic, for Hereditary Transthyretin Amyloidosis. N. Engl. J. Med. 2018, 379, 11–21. [Google Scholar] [CrossRef]
- Lohrmann, G.; Pipilas, A.; Mussinelli, R.; Gopal, D.M.; Berk, J.L.; Connors, L.H.; Vellanki, N.; Hellawell, J.; Siddiqi, O.K.; Fox, J.; et al. Stabilization of Cardiac Function With Diflunisal in Transthyretin (ATTR) Cardiac Amyloidosis. J. Card. Fail. 2020, 26, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.J.; Fine, N.; Garcia-Pavia, P.; Klein, A.L.; Fernandes, F.; Weissman, N.J.; Maurer, M.S.; Boman, K.; Gundapaneni, B.; Sultan, M.B.; et al. Effect of Tafamidis on Cardiac Function in Patients With Transthyretin Amyloid Cardiomyopathy. JAMA Cardiol. 2024, 9, 25. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Zhu, H.; Zhang, Y. Analysis of post-market adverse events of tafamidis base on the FDA adverse event reporting system. Sci. Rep. 2024, 14, 13691. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| No Tafamidis (N = 11) | Tafamidis (N = 28) | Comparison p-Value | |
|---|---|---|---|
| Gender, Male | 8 | 22 | 0.69 |
| Age (Years) | 87.4 ± 3.6 | 79.5 ± 5.9 | 0.0002 |
| ≥80 years | 11 | 15 | |
| BMI (kg/m2) | 25.7 ± 4.2 | 27.0 ± 3.5 | 0.35 |
| SBP (mmHg) | 123.6 ± 15.0 | 123.1 ± 13.3 | 0.92 |
| HR (bpm) | 72.2 ± 19.4 | 75.0 ± 15.1 | 0.63 |
| Atrial fibrillation | 7 | 17 | 1.0 |
| Smoker | 3 | 8, N = 27 | 1.0 |
| Dyslipidemia | 9 | 22 | 1.0 |
| Diabetes (Type II) | 2 | 8 | 0.69 |
| Hypertension | 6 | 16 | 1.0 |
| NYHA | 0.0016 | ||
| I | 0 | 2 | |
| II | 0 | 22 | |
| III | 7 | 4 | |
| IV | 4 | 0 | |
| Coronaropathy > 50% | 4 | 10 | 1.0 |
| Pulmonary hypertension | 6 | 13 | 0.73 |
| Hospitalization for acute heart failure | 4 | 8 | 0.71 |
| Length of stay (days) | 6.5 (6; 9) | 5.5 (4; 7) | 0.26 |
| Carpal tunnel | 2 | 8 | 0.69 |
| Lower limb oedema | 1 | 3 | 1.0 |
| Orthostatic hypotension | 1 | 6 | 0.65 |
| No Tafamidis (N = 11) | Tafamidis (N = 28) | Comparison | |||
|---|---|---|---|---|---|
| N Non Missing | Results | N Non Missing | Results | p-Value | |
| Telediastolic volume (mL) | 11 | 73 (60; 100) | 28 | 92 (68; 107) | 0.26 |
| SVi (mL/m2) | 9 | 34 (28; 43) | 26 | 35 (30; 41) | 0.79 |
| LVEF (%) | 11 | 54 (48; 60) | 28 | 56 (51;62) | 0.16 |
| GLS average (%) | 9 | −10.2 (−12.3; −10.1) | 27 | −13.9 (−15.9; −11.2) | 0.019 |
| Global work index (mmHg/%) | 7 | 1037 (780; 1160) | 25 | 1219 (963; 1347) | 0.16 |
| Global work efficiency (%) | 7 | 90 (85; 92) | 25 | 92 (87; 95) | 0.14 |
| LA Volume (mL/m2) | 8 | 38 (32; 53) | 22 | 48 (41;61) | 0.15 |
| LA GLS S-CT (%) | 6 | −2.5 (−7; −2) | 14 | −4 (−5; −2) | 0.83 |
| LA GLS S-R (%) | 6 | 13 (10; 21) | 14 | 10 (8; 13) | 0.51 |
| IVSd (mm) | 11 | 16.0 (15.7; 18.0) | 28 | 15.5 (13.5; 17.3) | 0.20 |
| LVEDD (mm) | 11 | 45 (33; 50) | 28 | 45 (39; 49) | 0.79 |
| LV mass index (g/m2) | 11 | 166 (137; 183) | 28 | 138 (120; 169) | 0.055 |
| E Velocity (cm/s) | 10 | 84 (72; 94) | 28 | 89 (71; 120) | 0.26 |
| E/A | 6 | 1.2 (0.74; 1.9) | 18 | 1.5 (0.80; 2.2) | 0.35 |
| e’ septal (cm/s) | 9 | 4 (4; 5) | 27 | 6 (5; 6) | 0.041 |
| e’ lateral (cm/s) | 9 | 5 (4; 7) | 27 | 7 (6; 9) | 0.012 |
| E/e’ mean | 9 | 18.8 (11.0; 22.0) | 27 | 14.0 (11.5; 16.5) | 0.19 |
| Vmax TR (m/s) | 10 | 3.2 (2.9; 3.5) | 21 | 2.9 (2.8; 3.0) | 0.12 |
| sPAP (mmHg) | 10 | 53 (37; 60) | 21 | 42 (36; 50) | 0.19 |
| RVEDD (mm) | 11 | 38 (32; 46) | 26 | 39 (36; 43) | 0.91 |
| TAPSE (mm) | 10 | 15 (15; 18) | 28 | 20 (16; 24) | 0.024 |
| S’ tricuspid (cm/s) | 7 | 8 (7; 14) | 24 | 11 (9; 13) | 0.19 |
| RA surface (cm2) | 10 | 18.2 (15.8; 21.8) | 28 | 20.5 (16.2; 24.0) | 0.47 |
| GLS RV G (%) | 8 | −9.7 (−15.6; −8.7) | 17 | −13.8 (−15.5; −11.1) | 0.27 |
| GLS RV FW (%) | 8 | −12.9 (−19.6; −11.9) | 17 | −16.4 (−19.9; −12.8) | 0.56 |
| AR—Grade | 11 | 27 | 0.016 | ||
| Trace | 3 | 20 | |||
| Mild | 7 | 5 | |||
| Moderate | 1 | 2 | |||
| Severe | 0 | 0 | |||
| AS Grade | 11 | 27 | 0.070 | ||
| Trace | 7 | 23 | |||
| Mild | 0 | 4 | |||
| Moderate | 3 | 0 | |||
| Severe | 1 | 0 | |||
| Peak velocity (m/s) | 10 | 2.0 (1.6; 3.1) | 27 | 1.4 (1.2; 1.6) | 0.021 |
| Aortic Max gradient (mmHg) | 10 | 18.5 (10.0; 39.0) | 27 | 7.0 (5.0; 9.6) | 0.013 |
| Aortic Mean gradient (mmHg) | 10 | 9 (6; 20) | 27 | 4 (3; 5) | 0.0076 |
| TVI aortic valve (cm) | 10 | 41.0 (31.9; 57.5) | 26 | 28.0 (23.0; 32.7) | 0.0094 |
| Velocity ratio | 9 | 0.40 (0.29; 0.57) | 26 | 0.70 (0.55; 0.76) | 0.030 |
| Aortic valve area (cm2) | 9 | 1.8 (1.1; 2.6) | 26 | 2.4 (2.1; 2.7) | 0.15 |
| No Tafamidis | Tafamidis | Comparison | |||
|---|---|---|---|---|---|
| N | Median (Q1; Q3) | N | Median (Q1; Q3) | p-Value b | |
| LVEF (%) | |||||
| D0 | 5 | 55.0 (54.0; 61.0) | 14 | 60.5 (55.0; 64.0) | |
| D360 | 5 | 48.0 (39.0; 60.0) | 14 | 52.5 (45.0; 58.0) | |
| Change from baseline | 5 | −12.0 (−13.0; 6.0) | 14 | −5.0 (−10.0; −4.0) | 0.85 |
| p-value evolution a | 0.31 | 0.0084 | |||
| GLS average (%) | |||||
| D0 | 4 | −11.2 (−12.3; −9.0) | 12 | −12.9 (−15.6; −10.7) | |
| D360 | 4 | −9.1 (−11.0; −7.2) | 12 | −13.0 (−14.0; −10.7) | |
| Change from baseline | 4 | 1.3 (0.35; 2.8) | 12 | 0.7 (0.00; 2.0) | 0.36 |
| p-value evolution a | 0.25 | 0.054 | |||
| Global work index (mmHg/%) | |||||
| D0 | 3 | 1078 (1023; 1174) | 9 | 1113 (963; 1301) | |
| D360 | 3 | 831 (680; 988) | 9 | 1208 (850; 1420) | |
| Change from baseline | 3 | −247 (−343; −186) | 9 | 60 (48; 84) | - |
| p-value evolution a | - | 0.054 | |||
| Global work efficiency (%) | |||||
| D0 | 3 | 90 (78; 92) | 9 | 94 (88; 95) | |
| D360 | 3 | 82 (77; 84) | 9 | 94 (89; 95) | |
| Change from baseline | 3 | −8 (−8; −1) | 9 | −1 (−2; 3) | - |
| p-value evolution a | - | 0.91 | |||
| Effect | Coeff. ± SE | p-Value | |
|---|---|---|---|
| LVEF (%) | Intercept | 50.6 ± 2.5 | - |
| Time | −0.0020 ± 0.0094 | 0.83 | |
| Tafamidis | 5.6 ± 3.0 | 0.064 | |
| Time × Tafamidis | −0.0098 ± 0.011 | 0.38 | |
| GLS average (%) | Intercept | −10.7 ± 0.94 | - |
| Time | 0.0014 ± 0.0036 | 0.70 | |
| Tafamidis | −2.7 ± 1.1 | 0.012 | |
| Time × Tafamidis | 0.0036 ± 0.0041 | 0.39 | |
| Global work index (mmHg/%) | Intercept | 952 ± 108 | - |
| Time | −0.37 ± 0.49 | 0.46 | |
| Tafamidis | 183 ± 121 | 0.14 | |
| Time × Tafamidis | 0.52 ± 0.56 | 0.35 | |
| Global work efficiency (%) | Intercept | 88.1 ± 1.9 | - |
| Time | −0.0082 ± 0.0087 | 0.35 | |
| Tafamidis | 2.9 ± 2.1 | 0.19 | |
| Time × Tafamidis | 0.010 ± 0.0098 | 0.30 |
| No Tafamidis | Tafamidis | Comparison | |||
|---|---|---|---|---|---|
| N | Median (Q1; Q3) | N | Median (Q1; Q3) | p-Value b | |
| LV mass index (g/m2) | |||||
| D0 | 6 | 157.0 (137.0; 176.0) | 15 | 135.0 (118.0; 167.0) | |
| D360 | 6 | 160.0 (148.0; 170.0) | 15 | 148.0 (128.0; 173.0) | |
| Change from baseline | 6 | −5.5 (−25.0; 10.0) | 15 | 4.0 (−4.0; 14.0) | 0.24 |
| p-value evolution a | 0.62 | 0.25 | |||
| TAPSE (mm) | |||||
| D0 | 4 | 15.0 (12.5; 16.5) | 13 | 19.0 (17.0; 24.0) | |
| D360 | 4 | 17.5 (12.0; 23.0) | 13 | 20.0 (14.0; 21.0) | |
| Change from baseline | 4 | 4.5 (−0.50; 6.5) | 13 | −2.0 (−3.0; 0.0) | 0.099 |
| p-value evolution a | 0.38 | 0.077 | |||
| A Velocity (cm/s) | |||||
| D0 | 3 | 68 (38; 99) | 6 | 73 (69; 87) | |
| D360 | 3 | 40 (32; 99) | 6 | 74 (64; 87) | |
| Change from baseline | 3 | −6 (−28; 0) | 6 | 3 (−19; 17) | - |
| p-value evolution a | - | 1.0 | |||
| e’ septal (cm/s) | |||||
| D0 | 3 | 4.0 (3.0; 6.0) | 12 | 6.0 (5.5; 7.5) | |
| D360 | 3 | 3.0 (3.0; 4.0) | 12 | 5.0 (5.0; 6.5) | |
| Change from baseline | 3 | −1.0 (−3.0; 1.0) | 12 | −1.0 (−1.0; 0.0) | - |
| p-value evolution a | - | 0.055 | |||
| e’ lateral (cm/s) | |||||
| D0 | 4 | 4.5 (3.5; 6.5) | 13 | 7.0 (7.0; 9.0) | |
| D360 | 4 | 3.5 (3.0; 5.0) | 13 | 7.0 (6.5; 9.0) | |
| Change from baseline | 4 | 0.0 (−1.0; 1.0) | 13 | 0.0 (−1.0; 1.0) | 0.23 |
| p-value evolution a | 0.25 | 0.73 | |||
| TRPG (mmHg) | |||||
| D0 | 5 | 45 (32; 50) | 11 | 37 (31; 44) | |
| D360 | 5 | 41 (36; 41) | 11 | 33 (23; 43) | |
| Change from baseline | 5 | −1 (−11; 9) | 11 | −3 (−20; 1) | 0.50 |
| p-value evolution a | 0.63 | 0.11 | |||
| Effect | Coeff. ± SE | p-Value | |
|---|---|---|---|
| Intercept | 172 ± 13.5 | - | |
| LV mass index (g/m2) | Time | −0.040 ± 0.050 | 0.84 |
| Tafamidis | −26.0 ± 15.8 | 0.10 | |
| Time × Tafamidis | 0.050 ± 0.061 | 0.41 | |
| TAPSE (mm) | Intercept | 16.2 ± 1.5 | - |
| Time | 0.0030 ± 0.0055 | 0.58 | |
| Tafamidis | 3.5 ± 1.8 | 0.050 | |
| Time x Tafamidis | −0.0082 ± 0.0064 | 0.20 | |
| A Velocity (cm/s) | Intercept | 72.0 ± 9.0 | - |
| Time | −0.066 ± 0.036 | 0.073 | |
| Tafamidis | −3.3 ± 10.4 | 0.75 | |
| Time × Tafamidis | 0.088 ± 0.043 | 0.045 | |
| e’ septal (cm/s) | Intercept | 4.5 ± 0.55 | - |
| Time | −0.0029 ± 0.0021 | 0.18 | |
| Tafamidis | 1.5 ± 0.62 | 0.015 | |
| Time × Tafamidis | 0.0011 ± 0.0024 | 0.65 | |
| e’ lateral (cm/s) | Intercept | 5.7 ± 0.74 | - |
| Time | −0.0002 ± 0.0026 | 0.93 | |
| Tafamidis | 2.6 ± 0.85 | 0.0034 | |
| Time × Tafamidis | −0.0014 ± 0.0030 | 0.64 | |
| TRPG (mmHg) | Intercept | 40.8 ± 3.0 | - |
| Time | −0.0087 ± 0.010 | 0.40 | |
| Tafamidis | −7.7 ± 3.7 | 0.037 | |
| Time × Tafamidis | 0.00052 ± 0.013 | 0.97 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Restelli, D.; Van Wallendael, C.; De Marneffe, N.; Damas, F.; Dulgheru, R.; Lancellotti, P. One-Year Echocardiographic Follow-Up in Transthyretin Cardiac Amyloidosis: Impact of Tafamidis Treatment. J. Clin. Med. 2025, 14, 1538. https://doi.org/10.3390/jcm14051538
Restelli D, Van Wallendael C, De Marneffe N, Damas F, Dulgheru R, Lancellotti P. One-Year Echocardiographic Follow-Up in Transthyretin Cardiac Amyloidosis: Impact of Tafamidis Treatment. Journal of Clinical Medicine. 2025; 14(5):1538. https://doi.org/10.3390/jcm14051538
Chicago/Turabian StyleRestelli, Davide, Céline Van Wallendael, Nils De Marneffe, François Damas, Raluca Dulgheru, and Patrizio Lancellotti. 2025. "One-Year Echocardiographic Follow-Up in Transthyretin Cardiac Amyloidosis: Impact of Tafamidis Treatment" Journal of Clinical Medicine 14, no. 5: 1538. https://doi.org/10.3390/jcm14051538
APA StyleRestelli, D., Van Wallendael, C., De Marneffe, N., Damas, F., Dulgheru, R., & Lancellotti, P. (2025). One-Year Echocardiographic Follow-Up in Transthyretin Cardiac Amyloidosis: Impact of Tafamidis Treatment. Journal of Clinical Medicine, 14(5), 1538. https://doi.org/10.3390/jcm14051538