

Primary and Recurrent Erysipelas—Epidemiological Patterns in a Single-Centre Retrospective Analysis
 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection Process
2.2. Eligibility Criteria
2.3. Statistical Analysis
3. Results
3.1. General Information
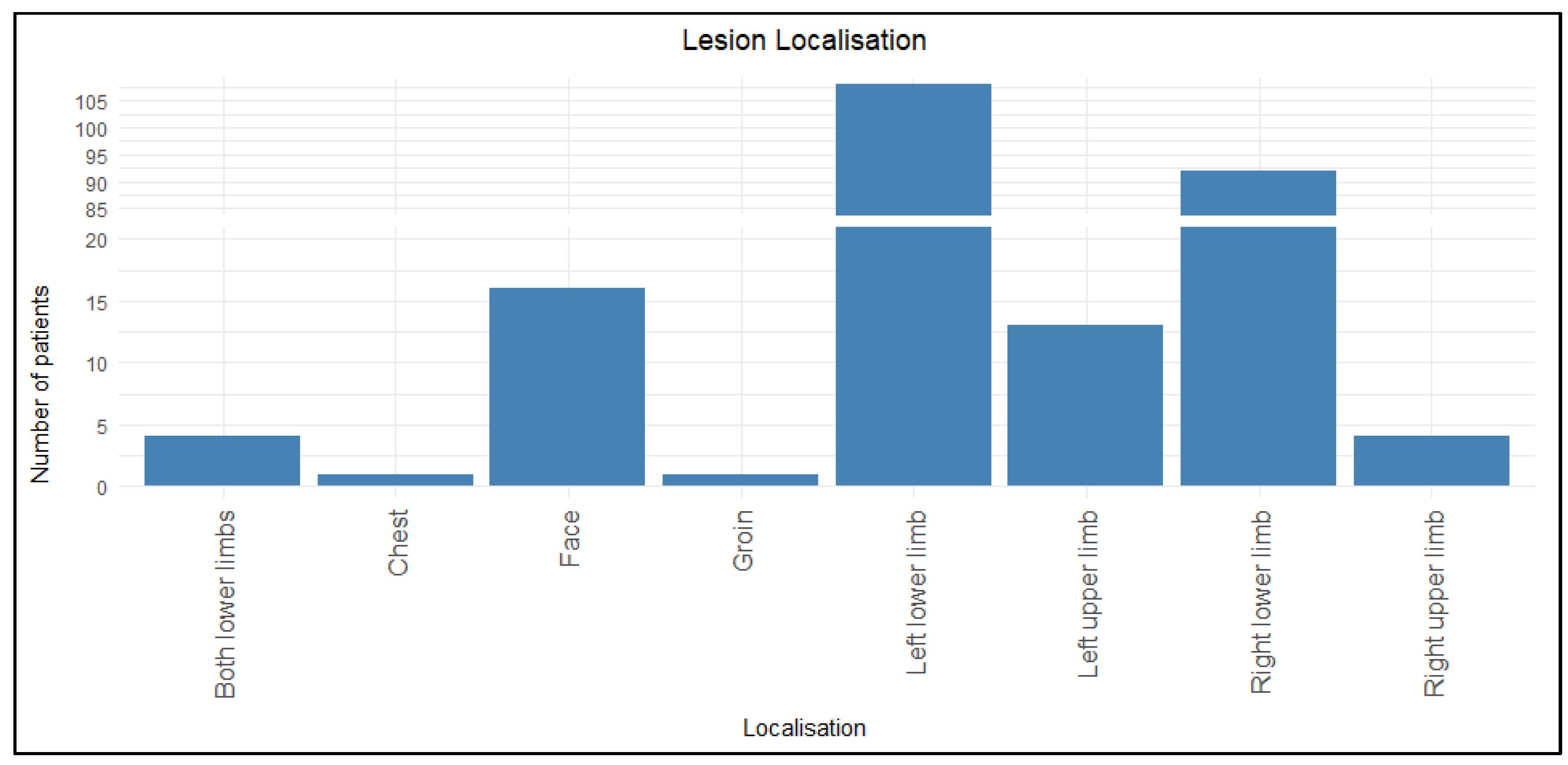
3.2. Lesion Localization
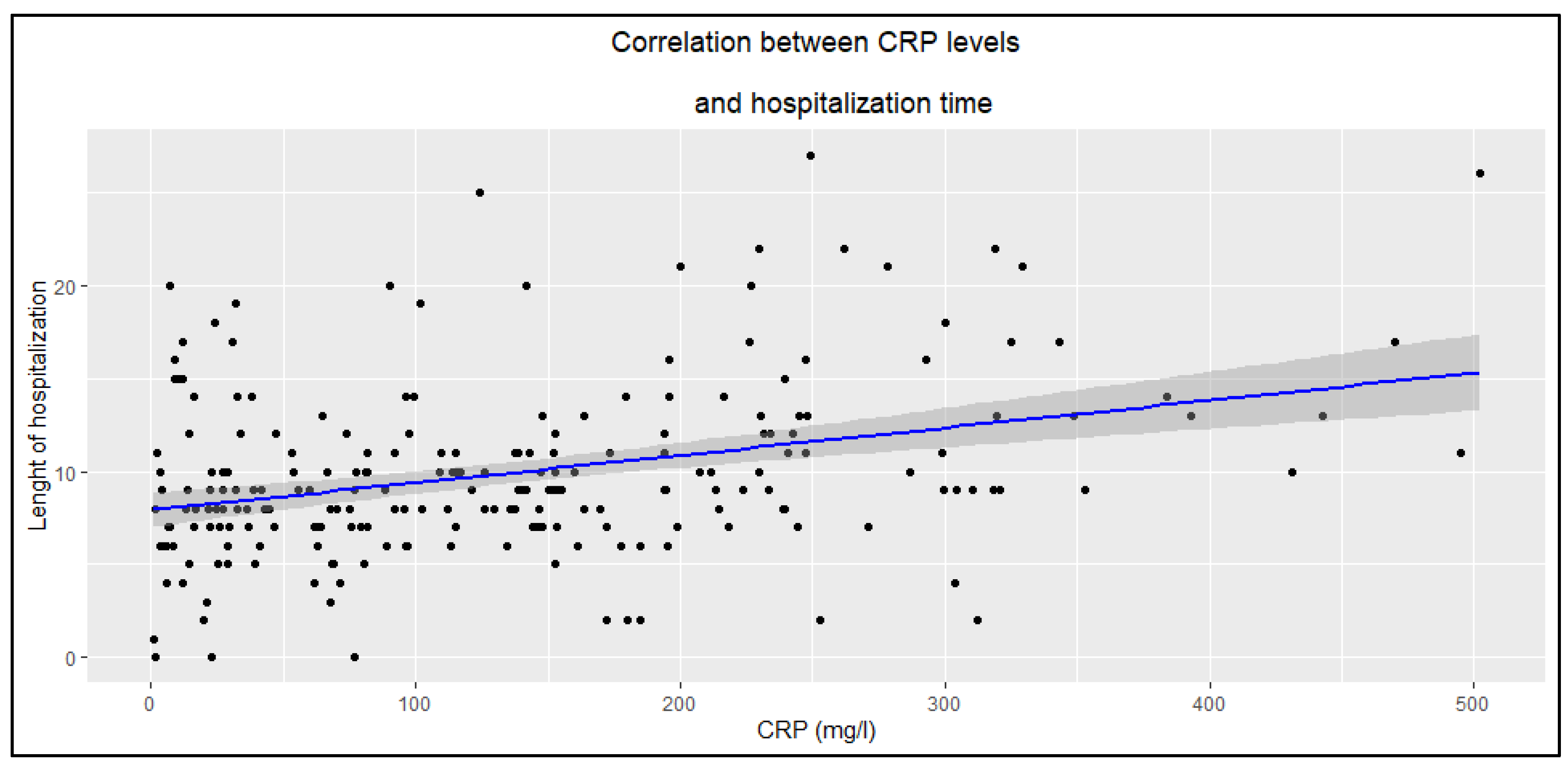
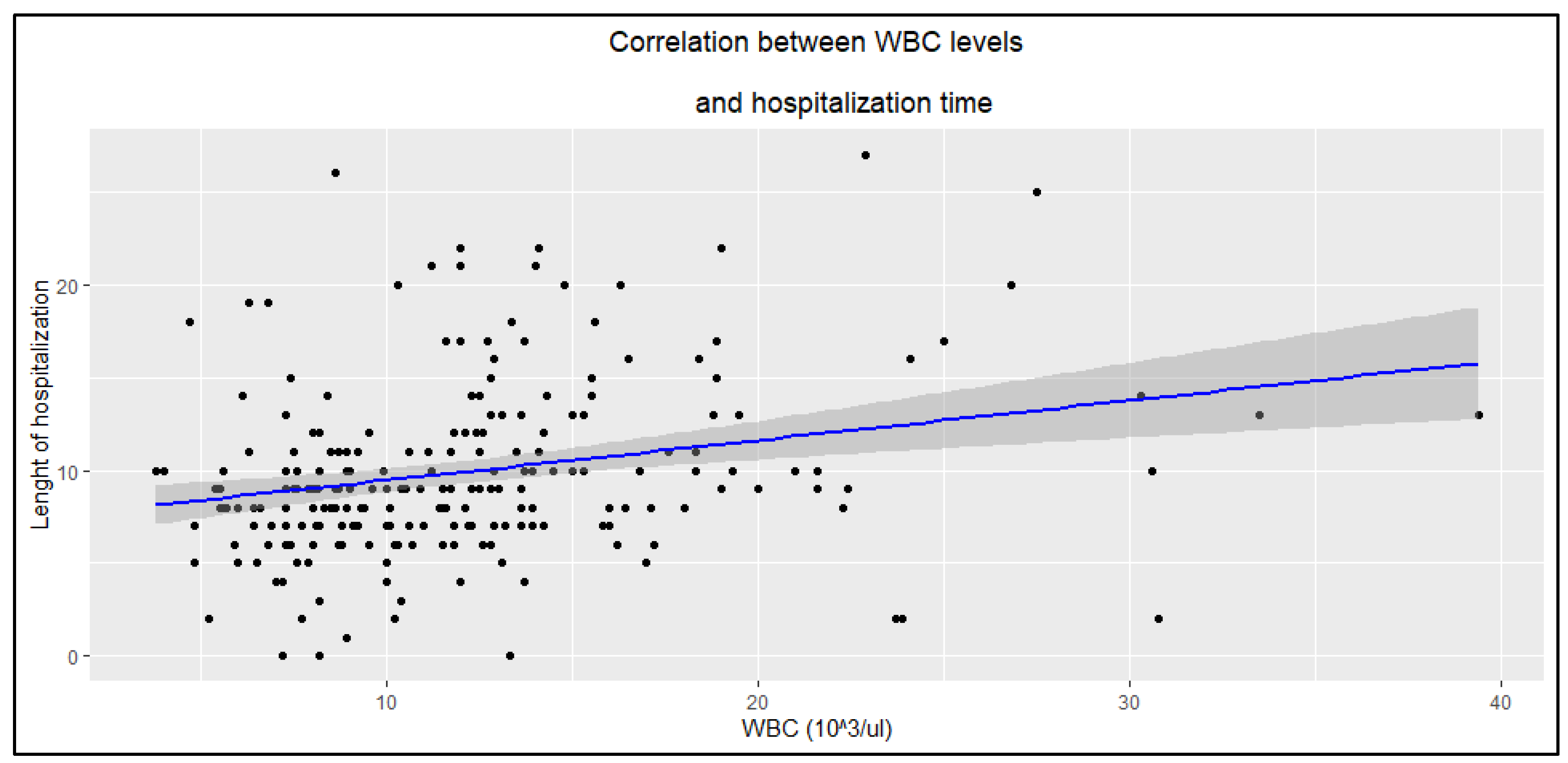
3.3. Results of Additional Tests
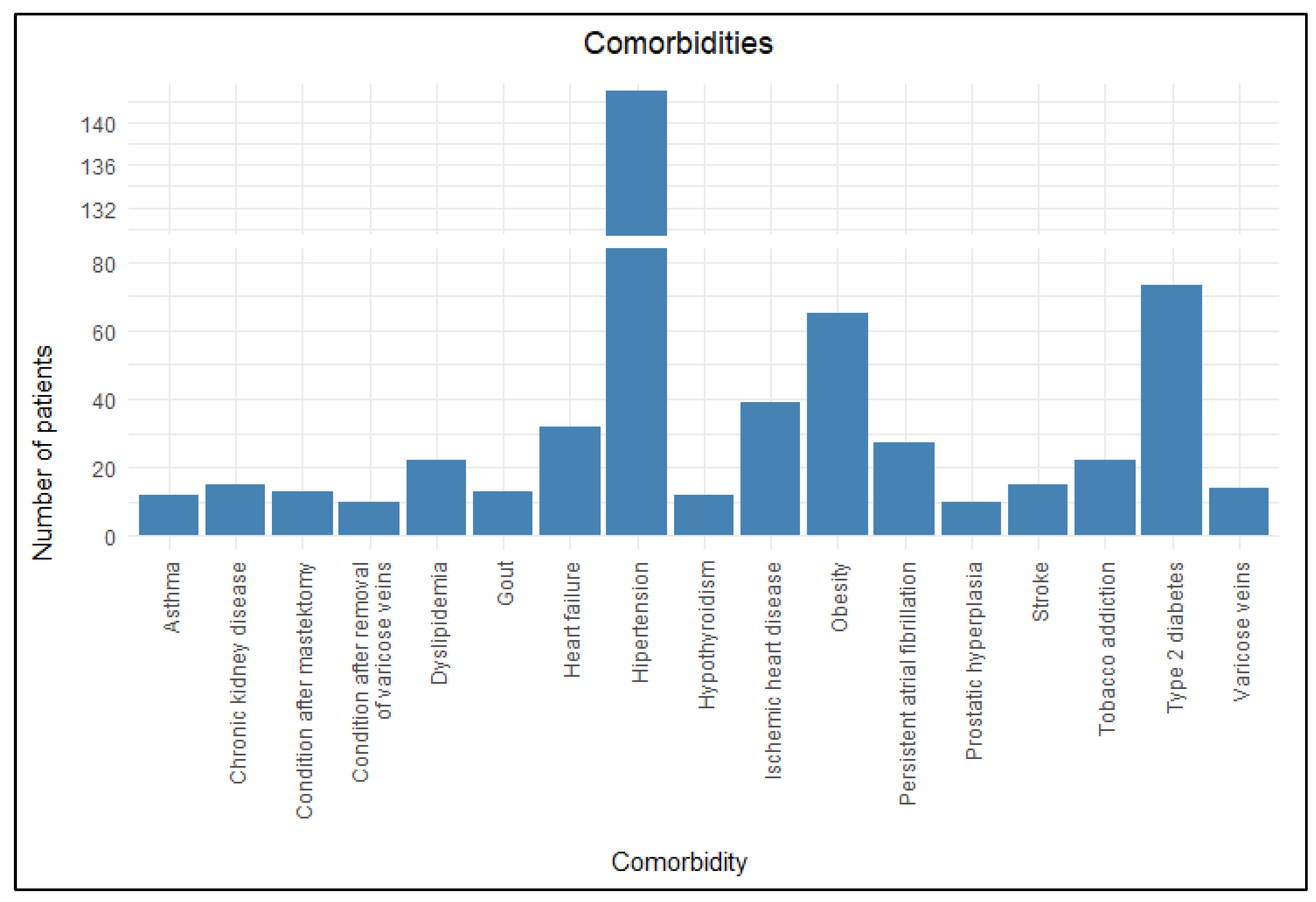
3.4. Comorbidities
3.5. Risk of Prolonged Hospitalization
4. Discussion
4.1. Demographic Characteristics of Patients
4.2. Anatomical Distribution of Erysipelas
4.3. Additional Tests
4.3.1. Inflammatory Markers
4.3.2. D-Dimer Levels
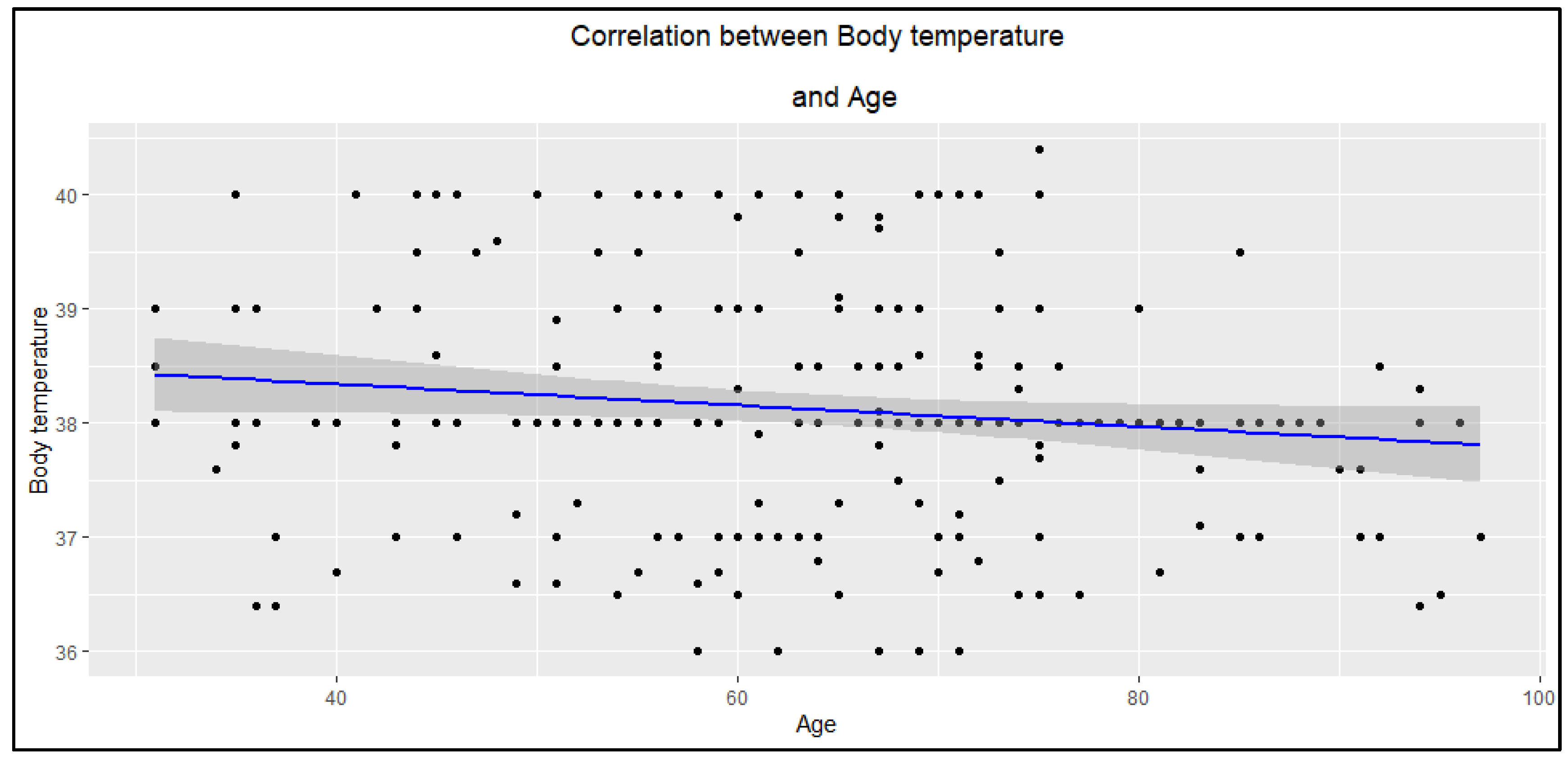
4.3.3. Body Temperature
4.4. Risk Factors of Outbreaks, Recurrences, and Prolonged Hospitalization
4.4.1. Risk Factors of Primary Erysipelas
4.4.2. Comorbidities as a Risk Factor of Recurrent Erysipelas
4.4.3. Comorbidities Influencing Hospitalization Time
4.5. Study Limitations
4.6. Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| WBC | White blood cell |
| CRP | C-reactive protein |
| PCT | Procalcitonin |
| DM2 | Diabetes mellitus type 2 |
| AF | Atrial fibrillation |
| OIL | Obesity-induced lymphedema |
| HR | Hazard ratio |
| CI | Confidence interval |
| R | Pearson’s correlation coefficient |
| SD | Standard deviation |
| U | Mann–Whitney U test |
References
- Trell, K.; Rignér, S.; Wierzbicka, M.; Nilson, B.; Rasmussen, M. Colonization of β-Hemolytic Streptococci in Patients with Erysipelas—A Prospective Study. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1901–1906. [Google Scholar] [CrossRef]
- Michael, Y.; Shaukat, N.M. Erysipelas. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- Esposito, S.; Pagliano, P.; De Simone, G.; Pan, A.; Brambilla, P.; Gattuso, G.; Mastroianni, C.; Kertusha, B.; Contini, C.; Massoli, L.; et al. Epidemiology, aetiology and treatment of skin and soft tissue infections: Final report of a prospective multicentre national registry. J. Chemother. 2022, 34, 524–533. [Google Scholar] [CrossRef]
- Li, J.; Han, X.; Zhang, X.; Wang, S. Spatiotemporal Evolution of Global Population Ageing from 1960 to 2017. BMC Public Health 2019, 19, 127. [Google Scholar] [CrossRef]
- Sørensen, T.I.A. Forecasting the Global Obesity Epidemic through 2050. Lancet 2025, 405, 756–757. [Google Scholar] [CrossRef]
- GBD 2021 Diabetes Collaborators. Global, Regional, and National Burden of Diabetes from 1990 to 2021, with Projections of Prevalence to 2050: A Systematic Analysis for the Global Burden of Disease Study 2021. Lancet 2023, 402, 203–234. [Google Scholar] [CrossRef]
- Chamli, A.; Jaber, K.; Ben Lagha, I.; Ben Slimane, M.; Rabhi, F.; Doss, N.; Dhaoui, M.R. Factors Associated with Acute and Recurrent Erysipelas in a Young Population: A Retrospective of 147 Cases. Tunis. Med. 2021, 99, 886–889. [Google Scholar]
- Brindle, R.J.; O’Neill, L.A.; Williams, O.M. Risk, Prevention, Diagnosis, and Management of Cellulitis and Erysipelas. Curr. Derm. Rep. 2020, 9, 73–82. [Google Scholar] [CrossRef]
- Alexander, H.; Paller, A.S.; Traidl-Hoffmann, C.; Beck, L.A.; De Benedetto, A.; Dhar, S.; Girolomoni, G.; Irvine, A.D.; Spuls, P.; Su, J.; et al. The Role of Bacterial Skin Infections in Atopic Dermatitis: Expert Statement and Review from the International Eczema Council Skin Infection Group. Br. J. Dermatol. 2020, 182, 1331–1342. [Google Scholar] [CrossRef]
- Leung, A.K.; Barankin, B.; Lam, J.M.; Leong, K.F.; Hon, K.L. Tinea Pedis: An Updated Review. Drugs Context 2023, 12, 1–16. [Google Scholar] [CrossRef]
- Higashi, Y.; Imafuku, S.; Tsuruta, N.; Murotani, K.; Western Japan Inflammatory Skin Disease Research Group. Systemic Therapy for Psoriasis and the Risk of Cutaneous Infections. J. Dermatol. 2024, 51, 939–949. [Google Scholar] [CrossRef]
- Sukumaran, V.; Senanayake, S. Bacterial Skin and Soft Tissue Infections. Aust. Prescr. 2016, 39, 159–163. [Google Scholar] [CrossRef]
- Savage, M.W.; Pottinger, J.M.; Chiang, H.-Y.; Yohnke, K.R.; Bowdler, N.C.; Herwaldt, L.A. Surgical Site Infections and Cellulitis after Abdominal Hysterectomy. Am. J. Obstet. Gynecol. 2013, 209, 108.e1–108.e10. [Google Scholar] [CrossRef]
- Bui, U.T.; Finlayson, K.; Edwards, H. Risk Factors for Infection in Patients with Chronic Leg Ulcers: A Survival Analysis. Int. J. Clin. Pract. 2018, 72, e13263. [Google Scholar] [CrossRef]
- Sapuła, M.; Krankowska, D.; Wiercińska-Drapało, A. In Search of Risk Factors for Recurrent Erysipelas and Cellulitis of the Lower Limb: A Cross-Sectional Study of Epidemiological Characteristics of Patients Hospitalized Due to Skin and Soft-Tissue Infections. Interdiscip. Perspect. Infect. Dis. 2020, 2020, 1–5. [Google Scholar] [CrossRef]
- Li, A.; Wang, N.; Ge, L.; Xin, H.; Li, W. Risk Factors of Recurrent Erysipelas in Adult Chinese Patients: A Prospective Cohort Study. BMC Infect. Dis. 2021, 21, 26. [Google Scholar] [CrossRef]
- Sugimoto, H.; Furukawa, K. Milian’s Ear Sign: Erysipelas. IDCases 2018, 14, e00449. [Google Scholar] [CrossRef]
- Krasagakis, K.; Valachis, A.; Maniatakis, P.; Krüger-Krasagakis, S.; Samonis, G.; Tosca, A.D. Report: Analysis of Epidemiology, Clinical Features and Management of Erysipelas. Int. J. Dermatol. 2010, 49, 1012–1017. [Google Scholar] [CrossRef]
- Wańczyk-Dręczewska, B.; Owczarczyk-Saczonek, A.B.; Placek, W.J. Erysipelas in an Atypical Location. Przegląd Dermatol. 2020, 107, 378–384. [Google Scholar] [CrossRef]
- Cervellin, G.; Longobardi, U.; Lippi, G. One Holy Man, One Eponym, Three Distinct Diseases. St. Anthony’s Fire Revisited. Acta Biomed. Atenei Parm. 2020, 92, e2021008. [Google Scholar] [CrossRef]
- Miró, E.M.; Sánchez, N.P. Cutaneous Manifestations of Infectious Diseases. In Atlas of Dermatology in Internal Medicine; Sánchez, N.P., Ed.; Springer: New York, NY, USA, 2012; pp. 77–119. [Google Scholar] [CrossRef]
- Bailey, E.; Kroshinsky, D. Cellulitis: Diagnosis and Management: Cellulitis. Dermatol. Ther. 2011, 24, 229–239. [Google Scholar] [CrossRef]
- Noh, S.H.; Park, S.D.; Kim, E.J. Serum Procalcitonin Level Reflects the Severity of Cellulitis. Ann. Dermatol. 2016, 28, 704. [Google Scholar] [CrossRef]
- Brindle, R.; Williams, O.M.; Barton, E.; Featherstone, P. Assessment of Antibiotic Treatment of Cellulitis and Erysipelas: A Systematic Review and Meta-Analysis. JAMA Dermatol. 2019, 155, 1033. [Google Scholar] [CrossRef]
- Shu, Z.; Cao, J.; Li, H.; Chen, P.; Cai, P. Efficacy and Safety of First- and Second-Line Antibiotics for Cellulitis and Erysipelas: A Network Meta-Analysis of Randomized Controlled Trials. Arch. Dermatol. Res. 2024, 316, 603. [Google Scholar] [CrossRef]
- Brishkoska-Boshkovski, V.; Kondova-Topuzovska, I.; Damevska, K.; Petrov, A. Comorbidities as Risk Factors for Acute and Recurrent Erysipelas. Open Access Maced. J. Med. Sci. 2019, 7, 937–942. [Google Scholar] [CrossRef] [PubMed]
- Inghammar, M.; Rasmussen, M.; Linder, A. Recurrent Erysipelas—Risk Factors and Clinical Presentation. BMC Infect. Dis. 2014, 14, 270. [Google Scholar] [CrossRef]
- Xu, S.; Chen, M.; Feng, T.; Zhan, L.; Zhou, L.; Yu, G. Use Ggbreak to Effectively Utilize Plotting Space to Deal With Large Datasets and Outliers. Front. Genet. 2021, 12, 774846. [Google Scholar] [CrossRef]
- Kozłowska, D.; Myśliwiec, H.; Kiluk, P.; Baran, A.; Milewska, A.J.; Flisiak, I. Clinical and epidemiological assessment of patients hospitalized for primary and recurrent erysipelas. Przegl. Epidemiol. 2016, 70, 575–584. [Google Scholar]
- McNamara, D.R. A Predictive Model of Recurrent Lower Extremity Cellulitis in a Population-Based Cohort. Arch. Intern. Med. 2007, 167, 709. [Google Scholar] [CrossRef]
- Sočan, K.; Sočan, M. Trends in the Epidemiology of Erysipelas in Slovenia. Acta Dermatovenerol. Alp. Pannonica Adriat. 2018, 27, 1–4. [Google Scholar]
- Bläckberg, A.; Trell, K.; Rasmussen, M. Erysipelas, a Large Retrospective Study of Aetiology and Clinical Presentation. BMC Infect. Dis. 2015, 15, 402. [Google Scholar] [CrossRef]
- Chen, L.; Zheng, Y.; Zheng, D.; Li, Z.; Chen, H.; Chen, C.; Yu, S. Research Trends on Lymphedema after Mastectomy for Breast Cancer Patients from 2000 to 2023: A Scientometric Analysis. Front. Oncol. 2025, 15, 1440966. [Google Scholar] [CrossRef]
- Taniyama, D.; Maruki, T.; Maeda, T.; Yoshida, H.; Takahashi, T. Repetitive Cellulitis Caused by Streptococcus Agalactiae Isolates with Different Genotypic and Phenotypic Features in a Patient Having Upper Extremity with Lymphedema after Mastectomy and Axillary Lymph Node Dissection. IDCases 2020, 20, e00793. [Google Scholar] [CrossRef]
- Krueger, E.A.; Hong, C.; Cunningham, N.J.; Berteau, L.K.; Cordero, L.; Wu, E.S.C.; Holloway, I.W. Prevalence of Nicotine and Tobacco Product Use by Sexual Identity, Gender Identity, and Sex Assigned at Birth Among Emerging Adult Tobacco Users in California, United States. Nicotine Tob. Res. 2023, 25, 1378–1385. [Google Scholar] [CrossRef]
- Koceva, A.; Herman, R.; Janez, A.; Rakusa, M.; Jensterle, M. Sex- and Gender-Related Differences in Obesity: From Pathophysiological Mechanisms to Clinical Implications. Int. J. Mol. Sci. 2024, 25, 7342. [Google Scholar] [CrossRef]
- Krokosz, D.; Lipowski, M. “No Risk No Fun?”: Determinants of Satisfaction with Life in People Who Engage in Extreme and High-Risk Sports. Int. J. Environ. Res. Public Health 2022, 19, 13328. [Google Scholar] [CrossRef]
- Rossaneis, M.A.; Haddad, M.d.C.F.L.; Mathias, T.A.d.F.; Marcon, S.S. Differences in Foot Self-Care and Lifestyle between Men and Women with Diabetes Mellitus. Rev. Lat. Am. Enferm. 2016, 24, e2761. [Google Scholar] [CrossRef]
- Maze, M.J.; Skea, S.; Pithie, A.; Metcalf, S.; Pearson, J.F.; Chambers, S.T. Prevalence of Concurrent Deep Vein Thrombosis in Patients with Lower Limb Cellulitis: A Prospective Cohort Study. BMC Infect. Dis. 2013, 13, 141. [Google Scholar] [CrossRef]
- Norman, D.C. Fever in the Elderly. Clin. Infect. Dis. 2000, 31, 148–151. [Google Scholar] [CrossRef]
- Limpawattana, P.; Phungoen, P.; Mitsungnern, T.; Laosuangkoon, W.; Tansangworn, N. Atypical Presentations of Older Adults at the Emergency Department and Associated Factors. Arch. Gerontol. Geriatr. 2016, 62, 97–102. [Google Scholar] [CrossRef]
- Roujeau, J.-C.; Sigurgeirsson, B.; Korting, H.-C.; Kerl, H.; Paul, C. Chronic Dermatomycoses of the Foot as Risk Factors for Acute Bacterial Cellulitis of the Leg: A Case-Control Study. Dermatology 2004, 209, 301–307. [Google Scholar] [CrossRef]
- Dupuy, A.; Benchikhi, H.; Roujeau, J.-C.; Bernard, P.; Vaillant, L.; Chosidow, O.; Sassolas, B.; Guillaume, J.-C.; Grob, J.-J.; Bastuji-Garin, S. Risk Factors for Erysipelas of the Leg (Cellulitis): Case-Control Study. BMJ 1999, 318, 1591–1594. [Google Scholar] [CrossRef]
- Toschi, A.; Giannella, M.; Viale, P. Recurrence of Skin and Soft Tissue Infections: Identifying Risk Factors and Treatment Strategies. Curr. Opin. Infect. Dis. 2025, 38, 71–77. [Google Scholar] [CrossRef]
- Yosipovitch, G.; Nedorost, S.T.; Silverberg, J.I.; Friedman, A.J.; Canosa, J.M.; Cha, A. Stasis Dermatitis: An Overview of Its Clinical Presentation, Pathogenesis, and Management. Am. J. Clin. Dermatol. 2023, 24, 275–286. [Google Scholar] [CrossRef]
- Bilancini, S.; Lucchi, M.; Ciacciarelli, M. Stasis Microangiopathy: From Pathogenesis to Treatment. Vessel Plus 2021, 5, 39. [Google Scholar] [CrossRef]
- Gibran, N.S.; Jang, Y.-C.; Isik, F.F.; Greenhalgh, D.G.; Muffley, L.A.; Underwood, R.A.; Usui, M.L.; Larsen, J.; Smith, D.G.; Bunnett, N.; et al. Diminished Neuropeptide Levels Contribute to the Impaired Cutaneous Healing Response Associated with Diabetes Mellitus. J. Surg. Res. 2002, 108, 122–128. [Google Scholar] [CrossRef]
- Pozzilli, P.; Leslie, R.D.G. Infections and Diabetes: Mechanisms and Prospects for Prevention. Diabet. Med. 1994, 11, 935–941. [Google Scholar] [CrossRef]
- Delamaire, M.; Maugendre, D.; Moreno, M.; Le Goff, M.-C.; Allannic, H.; Genetet, B. Impaired Leucocyte Functions in Diabetic Patients. Diabet. Med. 1997, 14, 29–34. [Google Scholar] [CrossRef]
- Factor, S.H.; Levine, O.S.; Schwartz, B.; Harrison, L.H.; Farley, M.M.; McGeer, A.; Schuchat, A. Invasive Group A Streptococcal Disease: Risk Factors for Adults. Emerg. Infect. Dis. 2003, 9, 970–977. [Google Scholar] [CrossRef]
- David, P.; Singh, S.; Ankar, R. A Comprehensive Overview of Skin Complications in Diabetes and Their Prevention. Cureus 2023, 15, e38961. [Google Scholar] [CrossRef]
- Sudduth, C.L.; Greene, A.K. Lymphedema and Obesity. Cold Spring Harb. Perspect. Med. 2022, 12, a041176. [Google Scholar] [CrossRef]
- Taira, K.G.; Wang, M.; Guo, W.; Kam, O.; Kaufmann, T. Association of Cellulitis with Obesity: Systematic Review and Meta-Analysis. JMIR Dermatol. 2024, 7, e54302. [Google Scholar] [CrossRef]
- Pavlotsky, F.; Amrani, S.; Trau, H. Recurrent Erysipelas: Risk Factors: Risikofaktoren Für Rezidiverysipele. J. Der Dtsch. Dermatol. Ges. 2004, 2, 89–95. [Google Scholar] [CrossRef]
- Lim, H.Y.; Rutkowski, J.M.; Helft, J.; Reddy, S.T.; Swartz, M.A.; Randolph, G.J.; Angeli, V. Hypercholesterolemic Mice Exhibit Lymphatic Vessel Dysfunction and Degeneration. Am. J. Pathol. 2009, 175, 1328–1337. [Google Scholar] [CrossRef]
- Collado, A.; Domingo, E.; Piqueras, L.; Sanz, M.-J. Primary Hypercholesterolemia and Development of Cardiovascular Disorders: Cellular and Molecular Mechanisms Involved in Low-Grade Systemic Inflammation and Endothelial Dysfunction. Int. J. Biochem. Cell Biol. 2021, 139, 106066. [Google Scholar] [CrossRef]
- Bernardi, S.; Marcuzzi, A.; Piscianz, E.; Tommasini, A.; Fabris, B. The Complex Interplay between Lipids, Immune System and Interleukins in Cardio-Metabolic Diseases. Int. J. Mol. Sci. 2018, 19, 4058. [Google Scholar] [CrossRef]
- Norimatsu, Y.; Norimatsu, Y. Malnutrition, Hypertension, and Hyperlipidemia as Risk Factors for Recurrent Cellulitis. J. Vasc. Surg. Cases Innov. Tech. 2021, 7, 343. [Google Scholar] [CrossRef]
- Norimatsu, Y.; Ohno, Y. Predictors for Readmission Due to Cellulitis among Japanese Patients. J. Dermatol. 2021, 48, 681–684. [Google Scholar] [CrossRef]
- Li, P.; Zhao, Z.; Sun, Y.; Xia, S.; Shen, W. The Prognostic Effect and Mechanism of Erysipelas in Cancer-Associated Lymphedema. Sci. Rep. 2025, 15, 5518. [Google Scholar] [CrossRef]
- Karppelin, M.; Syrjänen, J.; Siljander, T.; Vuopio-Varkila, J.; Kere, J.; Huhtala, H.; Vuento, R.; Jussila, T. Factors Predisposing to Acute and Recurrent Bacterial Non-Necrotizing Cellulitis in Hospitalized Patients: A Prospective Case–Control Study. Clin. Microbiol. Infect. 2010, 16, 729–734. [Google Scholar] [CrossRef]
- Shantsila, E.; Choi, E.-K.; Lane, D.A.; Joung, B.; Lip, G.Y.H. Atrial Fibrillation: Comorbidities, Lifestyle, and Patient Factors. Lancet Reg. Health Eur. 2024, 37, 100784. [Google Scholar] [CrossRef]
- Zhang, M.; Zhou, J. Systematic Review and Meta-Analysis of Stroke and Thromboembolism Risk in Atrial Fibrillation with Preserved vs. Reduced Ejection Fraction Heart Failure. BMC Cardiovasc. Disord. 2024, 24, 495. [Google Scholar] [CrossRef]
- Grupper, M.; Nicolau, D.P. Obesity and Skin and Soft Tissue Infections: How to Optimize Antimicrobial Usage for Prevention and Treatment? Curr. Opin. Infect. Dis. 2017, 30, 180–191. [Google Scholar] [CrossRef]
- Castro-Balado, A.; Varela-Rey, I.; Mejuto, B.; Mondelo-García, C.; Zarra-Ferro, I.; Rodríguez-Jato, T.; Fernández-Ferreiro, A. Updated Antimicrobial Dosing Recommendations for Obese Patients. Antimicrob. Agents Chemother. 2024, 68, e0171923. [Google Scholar] [CrossRef]
- Stenson, K.W.; Deutsch, A.; Heinemann, A.W.; Chen, D. Obesity and Inpatient Rehabilitation Outcomes for Patients with a Traumatic Spinal Cord Injury. Arch. Phys. Med. Rehabil. 2011, 92, 384–390. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| ICD-10 code A46 | Recognition other than erysipelas |
| Hospitalized adult patients | Patients treated on an outpatient basis |
| Complete patient history and follow-up history (including examination, blood tests, and body temperature) available at the Department of Dermatology, Pediatric Dermatology, and Oncology | Incomplete medical records Lack of patient’s consent for hospitalization, treatment, or early discharge upon request |
| Variable | All n = 239 | Women n = 113 (47.3%) | Men n = 126 (52.7%) | p * |
|---|---|---|---|---|
| Average age | 64 | 68 | 60 | <0.0001 |
| Relapse rate n (%) | 181 (75.7%) | 82 (72.6%) | 99 (78.6%) | 0.280 |
| Average hospitalization time | 9.82 | 9.66 | 9.98 | 0.427 |
| Localization | Men n (%) | Women n (%) | p |
|---|---|---|---|
| Primary erysipelas | |||
| Upper limb | 0 (0%) | 2 (3.4%) | 0.037 |
| Lower limb | 26 (44.8%) | 22 (37.9%) | |
| Other * | 1 (1.7%) | 7 (12.1%) | |
| Recurrent erysipelas | |||
| Upper limb | 1 (0.6%) | 14 (7.7%) | 0.0004 |
| Lower limb | 93 (51.4%) | 63 (34.8%) | |
| Other * | 5 (2.8%) | 5 (2.8%) | |
| All | |||
| Upper limb | 1 (0.4%) | 16 (6.7%) | <0.0001 |
| Lower limb | 119 (49.8%) | 85 (35.6%) | |
| Other * | 6 (2.5%) | 12 (5.0%) | |
| Surgical Treatment of Breast Cancer | Without Surgical Treatment | p * | |
|---|---|---|---|
| Upper limb | 12 | 4 | <0.0001 |
| Lower limb | 4 | 81 |
| Mean (±SD) | Minimum | Maximum | |
|---|---|---|---|
| CRP | 133.5 (±107.3) | 1.2 | 502.2 |
| WBC | 12.0 (±5.5) | 3.8 | 39.40 |
| PCT | 2.0 (±7.5) | 0.02 | 86.7 |
| D-dimer | 1710.7 (±1676.2) | 168 | 9977 |
| Comorbidity | Primary | Recurrent | p * | |
|---|---|---|---|---|
| Hypertension | With | 37 | 106 | 0.480 |
| Without | 21 | 75 | ||
| Type 2 diabetes | With | 20 | 53 | 0.454 |
| Without | 38 | 128 | ||
| Obesity | With | 15 | 50 | 0.793 |
| Without | 43 | 131 | ||
| Ischemic heart disease | With | 7 | 32 | 0.322 |
| Without | 51 | 149 | ||
| Heart failure | With | 7 | 25 | 0.737 |
| Without | 51 | 156 | ||
| Persistent atrial fibrillation | With | 9 | 18 | 0.252 |
| Without | 49 | 163 | ||
| Dyslipidemia | With | 1 | 22 | 0.024 |
| Without | 57 | 160 | ||
| Comorbidity | Number of Patients | Difference in Relapse Rate | ||
|---|---|---|---|---|
| With | Without | U | p * | |
| Hypertension | 143 | 96 | 6837 | 0.960 |
| Type 2 diabetes | 73 | 166 | 5909 | 0.761 |
| Obesity | 65 | 174 | 5387 | 0.574 |
| Ischemic heart disease | 39 | 200 | 3542 | 0.365 |
| Heart failure | 32 | 207 | 3134 | 0.625 |
| Persistent atrial fibrillation | 27 | 212 | 2497 | 0.249 |
| Dyslipidemia | 22 | 217 | 1577 | 0.009 |
| Predictor | HR | 95% CI | p | |
|---|---|---|---|---|
| Lower | Upper | |||
| Age | 0.99 | 0.97 | 1.02 | 0.515 |
| Number of comorbidities | 1.03 | 0.83 | 1.27 | 0.805 |
| Number of relapses | 1.15 | 0.95 | 1.40 | 0.160 |
| CRP (mg/L) | 1.000 | 0.996 | 1.003 | 0.897 |
| WBC (103/uL) | 0.91 | 0.86 | 0.97 | 0.006 |
| PCT (ng/mL) | 0.99 | 0.87 | 1.12 | 0.856 |
| D-dimer | 1.000 | 0.999 | 1.001 | 0.458 |
| Body temperature | 0.85 | 0.63 | 1.14 | 0.283 |
| Sex (F) | 1.03 | 0.47 | 2.28 | 0.933 |
| Hypertension | 1.36 | 0.65 | 2.85 | 0.417 |
| Type 2 diabetes | 0.96 | 0.40 | 2.27 | 0.919 |
| Permanent atrial fibrillation | 0.29 | 0.09 | 0.94 | 0.039 |
| Ischemic heart disease | 0.39 | 0.14 | 1.10 | 0.075 |
| Heart failure | 1.63 | 0.45 | 5.96 | 0.459 |
| Obesity (>30 BMI) | 0.39 | 0.16 | 0.98 | 0.046 |
| Tobacco addiction | 1.41 | 0.50 | 4.00 | 0.514 |
| Dyslipidemia | 2.40 | 0.59 | 9.85 | 0.222 |
| Enoxaparin | 0.53 | 0.29 | 0.95 | 0.033 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matych, M.; Ciosek, A.; Miler, K.; Noweta, M.; Brzezińska, K.; Sarzała, M.; Narbutt, J.; Lesiak, A. Primary and Recurrent Erysipelas—Epidemiological Patterns in a Single-Centre Retrospective Analysis. J. Clin. Med. 2025, 14, 5299. https://doi.org/10.3390/jcm14155299
Matych M, Ciosek A, Miler K, Noweta M, Brzezińska K, Sarzała M, Narbutt J, Lesiak A. Primary and Recurrent Erysipelas—Epidemiological Patterns in a Single-Centre Retrospective Analysis. Journal of Clinical Medicine. 2025; 14(15):5299. https://doi.org/10.3390/jcm14155299
Chicago/Turabian StyleMatych, Marta, Agata Ciosek, Karol Miler, Marcin Noweta, Karolina Brzezińska, Małgorzata Sarzała, Joanna Narbutt, and Aleksandra Lesiak. 2025. "Primary and Recurrent Erysipelas—Epidemiological Patterns in a Single-Centre Retrospective Analysis" Journal of Clinical Medicine 14, no. 15: 5299. https://doi.org/10.3390/jcm14155299
APA StyleMatych, M., Ciosek, A., Miler, K., Noweta, M., Brzezińska, K., Sarzała, M., Narbutt, J., & Lesiak, A. (2025). Primary and Recurrent Erysipelas—Epidemiological Patterns in a Single-Centre Retrospective Analysis. Journal of Clinical Medicine, 14(15), 5299. https://doi.org/10.3390/jcm14155299