

Passive Blood-Flow-Restriction Exercise’s Impact on Muscle Atrophy Post-Total Knee Replacement: A Randomized Trial
 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Methods
- 1.
- Control group (CON, Primary TKA: 11, Revision TKA: 2):
- 2.
- Intervention group (INT, Primary TKA: 10, Revision TKA: 3):
2.2. Study Design
2.3. Sample Size Calculation
2.4. Standard Operative and Postoperative Treatment
2.4.1. Surgery
2.4.2. Daily Physical Therapy
2.4.3. Rehabilitation
2.5. Interventions
2.5.1. Limb Occlusion Pressure and Blood Flow Restriction
2.5.2. In-Hospital Rehabilitation Protocol
2.6. Outcome Measures
2.7. Statistics
3. Results
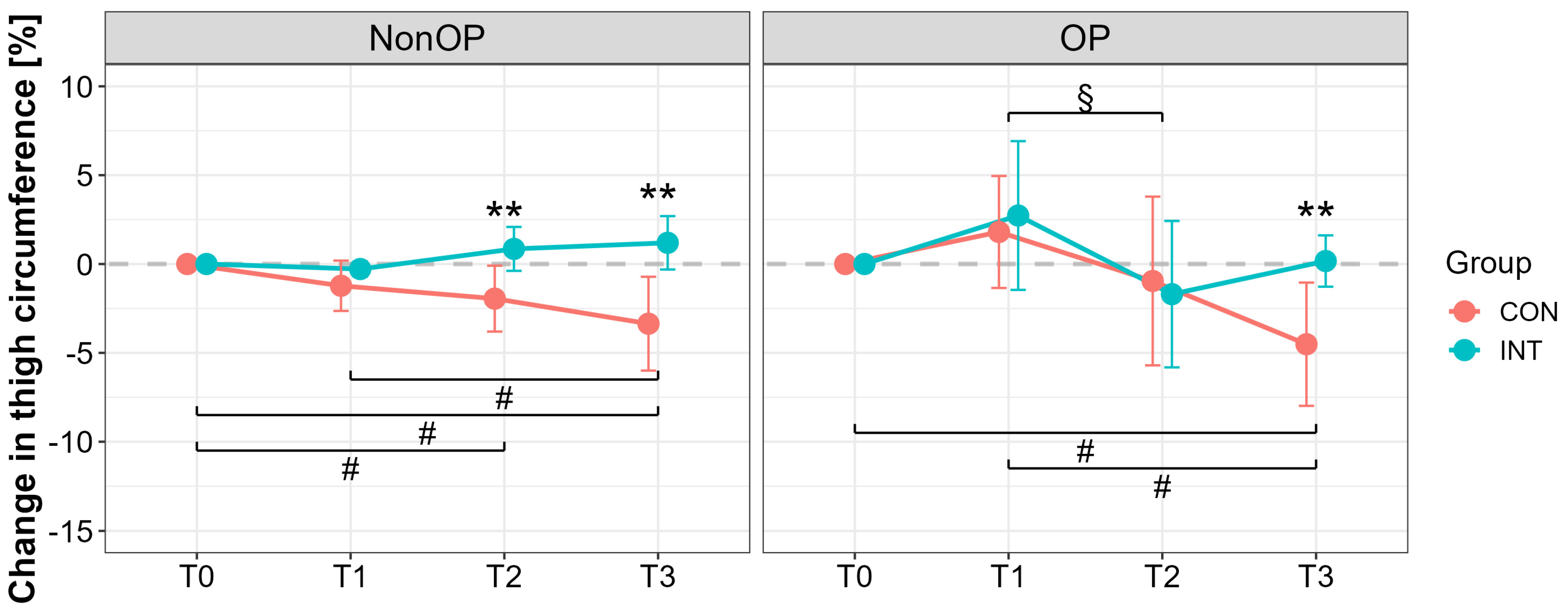
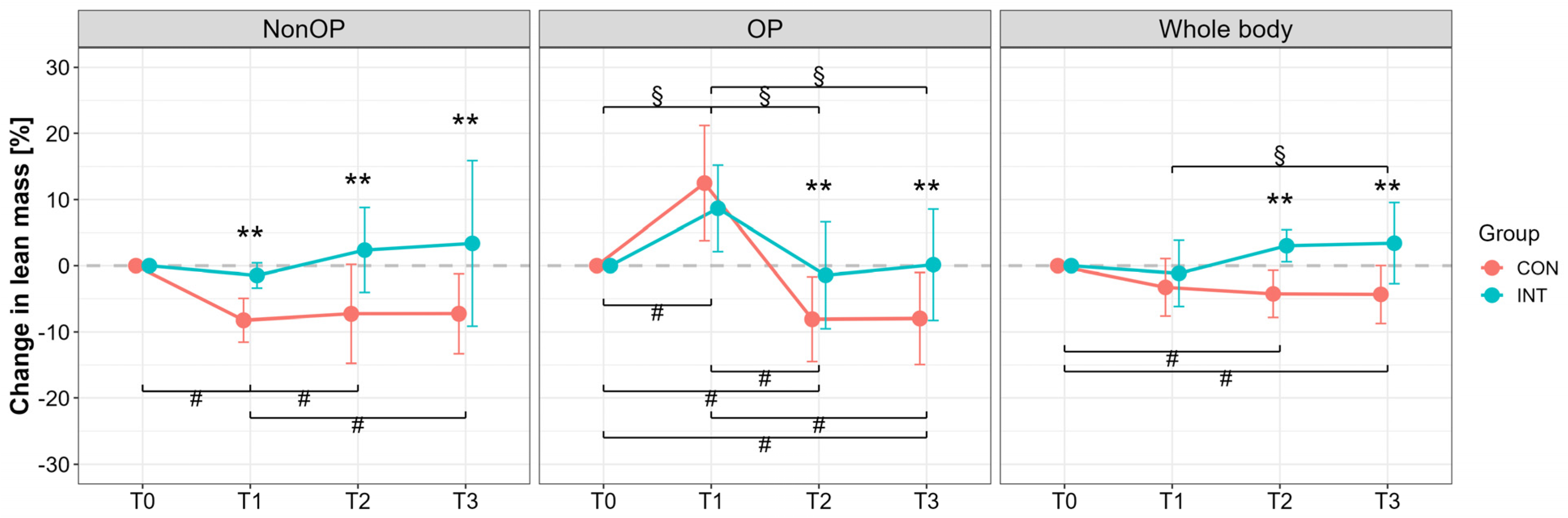
3.1. Quadriceps and Thigh Muscle Assessment
3.2. Functional Assessments
3.3. Questionnaires
4. Discussion
4.1. Muscle Atrophy After Total Knee Arthroplasty
4.2. Impact of Passive Blood Flow Restriction Training on Muscle Swelling
4.3. Impact of Passive Blood Flow Restriction on Functional Outcomes and Quality of Life
5. Summary and Clinical Impact
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACL | Anterior Cruciate Ligament |
| BFR | Blood Flow Restriction |
| CON | Control Group |
| CPM | Continuous Passive Motion |
| CRT | Chair Rising Test |
| DXA | Dual-Energy X-Ray Absorptiometry |
| INT | Intervention Group |
| KOOS | Knee Injury and Osteoarthritis Outcome Score |
| LOP | Limb Occlusion Pressure |
| MCIDs | Minimal clinically important differences |
| MURF-1 | Muscle RING-finger protein-1 |
| NMES | Neuromuscular electrical stimulation |
| pBFR | Passive Blood Flow Restriction |
| PJI | Periprosthetic Joint Infection |
| QoL | Quality of Life |
| rTKA | Revision Total Knee Arthroplasty |
| SF-36 | Short-Form 36 Score |
| TKA | Total Knee Arthroplasty |
| VAS | Visual Analog Scale |
| 6 MWT | Six-Minute Walking Test |
References
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef] [PubMed]
- LaStayo, P.C.; Meier, W.; Marcus, R.L.; Mizner, R.; Dibble, L.; Peters, C. Reversing muscle and mobility deficits 1 to 4 years after TKA: A pilot study. Clin. Orthop. Relat. Res. 2009, 467, 1493–1500. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.C.; Stevens-Lapsley, J.E. Importance of attenuating quadriceps activation deficits after total knee arthroplasty. Exerc. Sport Sci. Rev. 2012, 40, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Petersen, K.K.; Simonsen, O.; Laursen, M.B.; Nielsen, T.A.; Rasmussen, S.; Arendt-Nielsen, L. Chronic postoperative pain after primary and revision total knee arthroplasty. Clin. J. Pain 2015, 31, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Zech, A.; Hendrich, S.; Pfeifer, K. Association Between Exercise Therapy Dose and Functional Improvements in the Early Postoperative Phase After Hip and Knee Arthroplasty: An Observational Study. PM&R 2015, 7, 1064–1072. [Google Scholar] [CrossRef] [PubMed]
- Kamp, T.; Brouwer, S.; Seeber, G.H.; Overgaard, S.; Gademan, M.G.J.; Stevens, M. Return to work policies and practices after total hip or knee arthroplasty in Denmark, Germany, and the Netherlands: An exploratory study. Disabil. Rehabil. 2024, 46, 5313–5322. [Google Scholar] [CrossRef] [PubMed]
- Rak, D.; Nedopil, A.J.; Sayre, E.C.; Masri, B.A.; Rudert, M. Postoperative Inpatient Rehabilitation Does Not Increase Knee Function after Primary Total Knee Arthroplasty. J. Pers. Med. 2022, 12, 1934. [Google Scholar] [CrossRef] [PubMed]
- Meier, W.A.; Marcus, R.L.; Dibble, L.E.; Foreman, K.B.; Peters, C.L.; Mizner, R.L.; LaStayo, P.C. The long-term contribution of muscle activation and muscle size to quadriceps weakness following total knee arthroplasty. J. Geriatr. Phys. Ther. 2009, 32, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Bailey, A.N.; Hocker, A.D.; Vermillion, B.R.; Smolkowski, K.; Shah, S.N.; Jewett, B.A.; Dreyer, H.C. MAFbx, MuRF1, and the stress-activated protein kinases are upregulated in muscle cells during total knee arthroplasty. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2012, 303, R376–R386. [Google Scholar] [CrossRef] [PubMed]
- Ratchford, S.M.; Bailey, A.N.; Senesac, H.A.; Hocker, A.D.; Smolkowski, K.; Lantz, B.A.; Jewett, B.A.; Gilbert, J.S.; Dreyer, H.C. Proteins regulating cap-dependent translation are downregulated during total knee arthroplasty. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2012, 302, R702–R711. [Google Scholar] [CrossRef] [PubMed]
- Franz, A.; Queitsch, F.P.; Behringer, M.; Mayer, C.; Krauspe, R.; Zilkens, C. Blood flow restriction training as a prehabilitation concept in total knee arthroplasty: A narrative review about current preoperative interventions and the potential impact of BFR. Med. Hypotheses 2018, 110, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Ferraz, R.B.; Gualano, B.; Rodrigues, R.; Kurimori, C.O.; Fuller, R.; Lima, F.R.; Sá-Pinto, A.L.d.; Roschel, H. Benefits of Resistance Training with Blood Flow Restriction in Knee Osteoarthritis. Med. Sci. Sports Exerc. 2018, 50, 897–905. [Google Scholar] [CrossRef] [PubMed]
- Franz, A.; Ji, S.; Bittersohl, B.; Zilkens, C.; Behringer, M. Impact of a Six-Week Prehabilitation with Blood-Flow Restriction Training on Pre- and Postoperative Skeletal Muscle Mass and Strength in Patients Receiving Primary Total Knee Arthroplasty. Front. Physiol. 2022, 13, 881484. [Google Scholar] [CrossRef] [PubMed]
- Hughes, L.; Rosenblatt, B.; Haddad, F.; Gissane, C.; McCarthy, D.; Clarke, T.; Ferris, G.; Dawes, J.; Paton, B.; Patterson, S.D. Comparing the Effectiveness of Blood Flow Restriction and Traditional Heavy Load Resistance Training in the Post-Surgery Rehabilitation of Anterior Cruciate Ligament Reconstruction Patients: A UK National Health Service Randomised Controlled Trial. Sports Med. 2019, 49, 1787–1805. [Google Scholar] [CrossRef] [PubMed]
- Kubota, A.; Sakuraba, K.; Koh, S.; Ogura, Y.; Tamura, Y. Blood flow restriction by low compressive force prevents disuse muscular weakness. J. Sci. Med. Sport 2011, 14, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Takarada, Y.; Takazawa, H.; Ishii, N. Applications of vascular occlusion diminish disuse atrophy of knee extensor muscles. Med. Sci. Sports Exerc. 2000, 32, 2035–2039. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Fahs, C.A.; Rossow, L.M.; Abe, T.; Bemben, M.G. The anabolic benefits of venous blood flow restriction training may be induced by muscle cell swelling. Med. Hypotheses 2012, 78, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Nyakayiru, J.; Fuchs, C.J.; Trommelen, J.; Smeets, J.S.J.; Senden, J.M.; Gijsen, A.P.; Zorenc, A.H.; van Loon, L.J.C.; Verdijk, L.B. Blood Flow Restriction Only Increases Myofibrillar Protein Synthesis with Exercise. Med. Sci. Sports Exerc. 2019, 51, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Kakehi, S.; Tamura, Y.; Kubota, A.; Takeno, K.; Kawaguchi, M.; Sakuraba, K.; Kawamori, R.; Watada, H. Effects of blood flow restriction on muscle size and gene expression in muscle during immobilization: A pilot study. Physiol. Rep. 2020, 8, e14516. [Google Scholar] [CrossRef] [PubMed]
- Segers, J.; Hermans, G.; Bruyninckx, F.; Meyfroidt, G.; Langer, D.; Gosselink, R. Feasibility of neuromuscular electrical stimulation in critically ill patients. J. Crit. Care 2014, 29, 1082–1088. [Google Scholar] [CrossRef] [PubMed]
- Deutsche Rentenversicherung. Reha-Therapiestandards Hüft- und Knie-TEP. Available online: https://www.deutsche-rentenversicherung.de/SharedDocs/Downloads/DE/Experten/infos_reha_einrichtungen/quali_rehatherapiestandards/TEP/rts_tep_download.pdf?__blob=publicationFile&v=1 (accessed on 31 July 2024).
- VanWye, W.R.; Weatherholt, A.M.; Winchester, L.J.; Owens, J.G.; Kiessling II, P.B. Perceptual Responses to Varying Levels of Blood Flow Restriction Without Exercise. J. Acute Care Phys. Ther. 2025, 16, 108–112. [Google Scholar] [CrossRef]
- Androulakis-Korakakis, P.; Fisher, J.P.; Steele, J. The Minimum Effective Training Dose Required to Increase 1RM Strength in Resistance-Trained Men: A Systematic Review and Meta-Analysis. Sports Med. 2020, 50, 751–765. [Google Scholar] [CrossRef] [PubMed]
- Barbalho, M.; Rocha, A.C.; Seus, T.L.; Raiol, R.; Del Vecchio, F.B.; Coswig, V.S. Addition of blood flow restriction to passive mobilization reduces the rate of muscle wasting in elderly patients in the intensive care unit: A within-patient randomized trial. Clin. Rehabil. 2019, 33, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, J.A.; Ng, B.K.; Sommer, M.J.; Heymsfield, S.B. Body composition by DXA. Bone 2017, 104, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Ko, V.; Naylor, J.M.; Harris, I.A.; Crosbie, J.; Yeo, A.E.T. The six-minute walk test is an excellent predictor of functional ambulation after total knee arthroplasty. BMC Musculoskelet. Disord. 2013, 14, 145. [Google Scholar] [CrossRef] [PubMed]
- Rupp, T.; Butscheidt, S.; Jähn, K.; Simon, M.J.; Mussawy, H.; Oheim, R.; Barvencik, F.; Amling, M.; Rolvien, T. Low physical performance determined by chair rising test muscle mechanography is associated with prevalent fragility fractures. Arch. Osteoporos. 2018, 13, 71. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013; ISBN 9781134742707. [Google Scholar]
- Dreyer, H.C.; Strycker, L.A.; Senesac, H.A.; Hocker, A.D.; Smolkowski, K.; Shah, S.N.; Jewett, B.A. Essential amino acid supplementation in patients following total knee arthroplasty. J. Clin. Investig. 2013, 123, 4654–4666. [Google Scholar] [CrossRef] [PubMed]
- Valtonen, A.; Pöyhönen, T.; Heinonen, A.; Sipilä, S. Muscle deficits persist after unilateral knee replacement and have implications for rehabilitation. Phys. Ther. 2009, 89, 1072–1079. [Google Scholar] [CrossRef] [PubMed]
- Mizner, R.L.; Petterson, S.C.; Stevens, J.E.; Vandenborne, K.; Snyder-Mackler, L. Early quadriceps strength loss after total knee arthroplasty. The contributions of muscle atrophy and failure of voluntary muscle activation. J. Bone Joint Surg. Am. 2005, 87, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.H.; Cheng, C.K.; Lee, Y.T.; Lee, K.S. Muscle strength after successful total knee replacement: A 6- to 13-year followup. Clin. Orthop. Relat. Res. 1996, 328, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Kasmire, K.E.; Rasouli, M.R.; Mortazavi, S.M.J.; Sharkey, P.F.; Parvizi, J. Predictors of functional outcome after revision total knee arthroplasty following aseptic failure. Knee 2014, 21, 264–267. [Google Scholar] [CrossRef] [PubMed]
- Greidanus, N.V.; Peterson, R.C.; Masri, B.A.; Garbuz, D.S. Quality of life outcomes in revision versus primary total knee arthroplasty. J. Arthroplast. 2011, 26, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Nham, F.H.; Patel, I.; Zalikha, A.K.; El-Othmani, M.M. Epidemiology of primary and revision total knee arthroplasty: Analysis of demographics, comorbidities and outcomes from the national inpatient sample. Arthroplasty 2023, 5, 18. [Google Scholar] [CrossRef] [PubMed]
- Roof, M.A.; Sharan, M.; Merkow, D.; Feng, J.E.; Long, W.J.; Schwarzkopf, R.S. High-volume revision surgeons have better outcomes following revision total knee arthroplasty. Bone Joint J. 2021, 103-B, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Caron, É.; Gabrion, A.; Ehlinger, M.; Verdier, N.; Rubens-Duval, B.; Neri, T.; Martz, P.; Putman, S.; Pasquier, G. Complications and failures of non-tumoral hinged total knee arthroplasty in primary and aseptic revision surgery: A review of 290 cases. Orthop. Traumatol. Surg. Res. 2021, 107, 102875. [Google Scholar] [CrossRef] [PubMed]
- Laurence, P.; Hanney, W.J.; Purita, J.; Graham, A.; Kolber, M. Blood Flow Restriction Training. Bio Orthop. J. 2022, 4, e142–e163. [Google Scholar] [CrossRef]
- Fuchs, C.J.; Hermans, W.J.H.; Nyakayiru, J.; Weijzen, M.E.G.; Smeets, J.S.J.; Aussieker, T.; Senden, J.M.; Wodzig, W.K.H.W.; Snijders, T.; Verdijk, L.B.; et al. Daily blood flow restriction does not preserve muscle mass and strength during 2 weeks of bed rest. J. Physiol. 2024; ahead of print. [Google Scholar] [CrossRef]
- Slysz, J.T.; Boston, M.; King, R.; Pignanelli, C.; Power, G.A.; Burr, J.F. Blood Flow Restriction Combined with Electrical Stimulation Attenuates Thigh Muscle Disuse Atrophy. Med. Sci. Sports Exerc. 2021, 53, 1033–1040. [Google Scholar] [CrossRef] [PubMed]
- Iversen, E.; Røstad, V.; Larmo, A. Intermittent blood flow restriction does not reduce atrophy following anterior cruciate ligament reconstruction. J. Sport Health Sci. 2016, 5, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Hughes, L.; Swain, P.M.; Lai, T.; McEwen, J.A. It’s time to regulate—The importance of accurate surgical-grade tourniquet autoregulation in blood flow restriction exercise applications. Phys. Ther. Sport 2024, 67, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Noble, P.C.; Conditt, M.A.; Cook, K.F.; Mathis, K.B. The John Insall Award: Patient expectations affect satisfaction with total knee arthroplasty. Clin. Orthop. Relat. Res. 2006, 452, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Kurien, T.; Kerslake, R.W.; Graven-Nielsen, T.; Arendt-Nielsen, L.; Auer, D.P.; Edwards, K.; Scammell, B.E.; Petersen, K.K.-S. Chronic postoperative pain after total knee arthroplasty: The potential contributions of synovitis, pain sensitization and pain catastrophizing-An explorative study. Eur. J. Pain 2022, 26, 1979–1989. [Google Scholar] [CrossRef] [PubMed]
- Tallon, D.; Chard, J.; Dieppe, P. Exploring the priorities of patients with osteoarthritis of the knee. Arthritis Care Res. 2000, 13, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Bai, D.; Cheng, C.; Tian, G. The effectiveness and safety of blood flow restriction training for the post-operation treatment of distal radius fracture. Ann. Med. 2023, 55, 2240329. [Google Scholar] [CrossRef] [PubMed]
- Žargi, T.; Drobnič, M.; Stražar, K.; Kacin, A. Short-Term Preconditioning with Blood Flow Restricted Exercise Preserves Quadriceps Muscle Endurance in Patients After Anterior Cruciate Ligament Reconstruction. Front. Physiol. 2018, 9, 1150. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, S.L.; Mechlenburg, I. Effects of Low-Load Blood-Flow Restricted Resistance Training on Functional Capacity and Patient-Reported Outcome in a Young Male Suffering From Reactive Arthritis. Front. Sports Act. Living 2021, 3, 798902. [Google Scholar] [CrossRef] [PubMed]
- Bade, M.J.; Kohrt, W.M.; Stevens-Lapsley, J.E. Outcomes before and after total knee arthroplasty compared to healthy adults. J. Orthop. Sports Phys. Ther. 2010, 40, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Mizner, R.L.; Petterson, S.C.; Stevens, J.E.; Axe, M.J.; Snyder-Mackler, L. Preoperative quadriceps strength predicts functional ability one year after total knee arthroplasty. J. Rheumatol. 2005, 32, 1533–1539. [Google Scholar] [PubMed]
- King, L.K.; Hawker, G.A.; Stanaitis, I.; Woodhouse, L.; Jones, C.A.; Waugh, E.J. Minimal clinically important difference for improvement in six-minute walk test in persons with knee osteoarthritis after total knee arthroplasty. BMC Musculoskelet. Disord. 2022, 23, 307. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.; Hely, R.; Page, R.S.; Hely, A.; Harrison, B.; Landers, S. Thirty second chair stand test: Test-retest reliability, agreement and minimum detectable change in people with early-stage knee osteoarthritis. Physiother. Res. Int. 2022, 27, e1957. [Google Scholar] [CrossRef] [PubMed]
- Migliorini, F.; Maffulli, N.; Schäfer, L.; Simeone, F.; Bell, A.; Hofmann, U.K. Minimal clinically important difference (MCID), substantial clinical benefit (SCB), and patient-acceptable symptom state (PASS) in patients who have undergone total knee arthroplasty: A systematic review. Knee Surg. Relat. Res. 2024, 36, 3. [Google Scholar] [CrossRef] [PubMed]
- De Renty, C.; Forelli, F.; Mazeas, J.; Kakavas, G.; Hewett, T.E.; Korakakis, V. Knee Loading with Blood Flow Restriction Can Enhance Recovery After Total Knee Arthroplasty. Cureus 2023, 15, e37895. [Google Scholar] [CrossRef] [PubMed]
- Viscay-Sanhueza, N.; Curilem Gatica, C.; Bahamondes-Avila, C. Exercise with blood flow restriction among adults undergoing total knee arthroplasty: A scoping review. J. Bodyw. Mov. Ther. 2025, 42, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Stevens-Lapsley, J.E.; Balter, J.E.; Wolfe, P.; Eckhoff, D.G.; Kohrt, W.M. Early neuromuscular electrical stimulation to improve quadriceps muscle strength after total knee arthroplasty: A randomized controlled trial. Phys. Ther. 2012, 92, 210–226. [Google Scholar] [CrossRef] [PubMed]
- Canovas, F.; Dagneaux, L. Quality of life after total knee arthroplasty. Orthop. Traumatol. Surg. Res. 2018, 104, S41–S46. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.J.; Hevesi, M.; O’Byrne, M.M.; Berry, D.J.; Lewallen, D.G.; Maradit Kremers, H. Long-Term Mortality Trends After Revision Total Knee Arthroplasty. J. Arthroplast. 2019, 34, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Boddapati, V.; Fu, M.C.; Mayman, D.J.; Su, E.P.; Sculco, P.K.; McLawhorn, A.S. Revision Total Knee Arthroplasty for Periprosthetic Joint Infection Is Associated with Increased Postoperative Morbidity and Mortality Relative to Noninfectious Revisions. J. Arthroplast. 2018, 33, 521–526. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Group | T0 | T2 | T3 | p Values from Mixed Effect Model | ||
|---|---|---|---|---|---|---|---|
| Time | Group | Time x Group | |||||
| ADL | CON | 42.5 ± 18.0 | 57.3 ± 14.2 | 66.6 ± 15.1 | <0.001 (T0 < T2 < T3) | 0.495 | 0.641 |
| INT | 49.4 ± 15.6 | 60.0 ± 11.6 | 67.5 ± 13.5 | ||||
| Pain | CON | 41.8 ± 18.7 | 52.0 ± 13.3 | 59.8 ± 15.2 | <0.001 (T0 < T2 ≈ T3) | 0.300 | 0.963 |
| INT | 48.6 ± 16.4 | 57.0 ± 12.9 | 65.0 ± 17.9 | ||||
| QOL | CON | 18.8 ± 14.1 | 30.1 ± 15.3 | 40.0 ± 17.0 | <0.001 (T0 < T2 < T3) | 0.234 | 0.984 |
| INT | 25.0 ± 16.4 | 35.1 ± 11.2 | 45.9 ± 10.5 | ||||
| SportRec | CON | 20.5 ± 23.8 | 20.6 ± 17.4 | 33.3 ± 20.2 | <0.001 (T0 ≈ T2 < T3) | 0.600 | 0.810 |
| INT | 22.0 ± 25.2 | 24.0 ± 18.1 | 40.3 ± 20.4 | ||||
| Symptoms | CON | 39.1 ± 17.1 | 50.6 ± 13.9 | 58.9 ± 20.4 | <0.001 (T0 < T2 < T3) | 0.523 | 0.721 |
| INT | 42.3 ± 11.8 | 51.4 ± 17.5 | 65.9 ± 19.4 | ||||
| Item | Group | T0 | T2 | T3 | p Values from Mixed Effect Model | ||
|---|---|---|---|---|---|---|---|
| Time | Group | Time x Group | |||||
| PF | CON | 33.2 ± 30.0 | 36.0 ± 24.1 | 57.9 ± 22.5 | <0.001 (T0 ≈ T2 < T3) | 0.766 | 0.262 |
| INT | 31.3 ± 16.4 | 47.7 ± 17.7 | 54.6 ± 15.4 | ||||
| RP | CON | 33.3 ± 40.8 | 35.8 ± 31.4 | 65.0 ± 33.8 | 0.006 (T0 ≈ T2 < T3) | 0.657 | 0.701 |
| INT | 42.5 ± 42.6 | 45.8 ± 36.5 | 62.5 ± 33.9 | ||||
| BP | CON | 20.1 ± 17.1 | 37.7 ± 14.2 | 50.8 ± 21.4 | <0.001 (T0 < T2 ≈ T3) | 0.025 (CON < INT) | 0.309 |
| INT | 40.6 ± 16.2 | 54.5 ± 20.0 | 58.8 ± 21.2 | ||||
| GH | CON | 54.5 ±11.6 | 59.3 ± 10.3 | 57.4 ± 13.2 | 0.298 | 0.762 | 0.767 |
| INT | 52.1 ±22.1 | 55.2 ± 23.7 | 57.7 ± 20.5 | ||||
| VT | CON | 47.0 ± 12.3 | 49.7 ± 12.4 | 59.0 ± 17.3 | 0.002 (T0 < T3) | 0.786 | 0.843 |
| INT | 47.5 ± 26.5 | 53.7 ± 19.6 | 60.0 ± 15.8 | ||||
| SF | CON | 50.0 ± 27.0 | 61.3 ± 23.9 | 72.5 ± 29.3 | 0.014 (T0 < T3) | 0.524 | 0.923 |
| INT | 58.8 ± 31.8 | 66.3 ± 28.9 | 76.3 ± 23.9 | ||||
| RE | CON | 53.3 ± 50.2 | 76.7 ± 38.7 | 76.7 ± 38.7 | 0.005 (T0 < T2 ≈ T3) | 0.821 | 0.805 |
| INT | 46.7 ± 47.7 | 70.0 ± 39.9 | 80.0 ± 32.2 | ||||
| MH | CON | 62.0 ± 23.3 | 66.5 ± 21.0 | 69.6 ± 21.2 | 0.104 | 0.735 | 0.984 |
| INT | 65.5 ± 24.6 | 68.8 ± 21.7 | 72.7 ± 22.1 | ||||
| PCS | CON | 28.2 ±11.2 | 34.5 ± 7.6 | 41.5 ± 10.6 | <0.001 (T0 < T2 ≈ T3) | 0.167 | 0.524 |
| INT | 32.6 ± 8.98 | 41.0 ± 8.4 | 42.0 ± 10.5 | ||||
| MCS | CON | 44.4 ± 16.9 | 54.2 ± 12.5 | 54.9 ± 11.4 | <0.001 (T0 < T2 ≈ T3) | 0.906 | 0.566 |
| INT | 45.3 ± 16.7 | 52.1 ± 13.7 | 58.1 ± 12.4 | ||||
| RV | CON | 3.30 ± 1.06 | 2.50 ± 1.08 | 3.00 ± 0.67 | 0.593 | 0.963 | 0.052 |
| INT | 2.67 ± 0.71 | 3.10 ± 0.99 | 3.10 ± 0.74 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franz, A.; Heiß, L.; Schlotmann, M.; Ji, S.; Strauss, A.C.; Randau, T.; Fröschen, F.S. Passive Blood-Flow-Restriction Exercise’s Impact on Muscle Atrophy Post-Total Knee Replacement: A Randomized Trial. J. Clin. Med. 2025, 14, 5218. https://doi.org/10.3390/jcm14155218
Franz A, Heiß L, Schlotmann M, Ji S, Strauss AC, Randau T, Fröschen FS. Passive Blood-Flow-Restriction Exercise’s Impact on Muscle Atrophy Post-Total Knee Replacement: A Randomized Trial. Journal of Clinical Medicine. 2025; 14(15):5218. https://doi.org/10.3390/jcm14155218
Chicago/Turabian StyleFranz, Alexander, Luisa Heiß, Marie Schlotmann, Sanghyeon Ji, Andreas Christian Strauss, Thomas Randau, and Frank Sebastian Fröschen. 2025. "Passive Blood-Flow-Restriction Exercise’s Impact on Muscle Atrophy Post-Total Knee Replacement: A Randomized Trial" Journal of Clinical Medicine 14, no. 15: 5218. https://doi.org/10.3390/jcm14155218
APA StyleFranz, A., Heiß, L., Schlotmann, M., Ji, S., Strauss, A. C., Randau, T., & Fröschen, F. S. (2025). Passive Blood-Flow-Restriction Exercise’s Impact on Muscle Atrophy Post-Total Knee Replacement: A Randomized Trial. Journal of Clinical Medicine, 14(15), 5218. https://doi.org/10.3390/jcm14155218