

An Analysis of Post-Adrenalectomy Dynamics in MACS (Mild Autonomous Cortisol Secretion)-Positive Adrenal Tumours: The Biomarkers and Clinical Impact



Abstract
1. Introduction
Objective
2. Methods
3. Results
3.1. Hormonal Biomarkers upon Unilateral Adrenalectomy
3.2. Impact of Adrenalectomy on Cardio-Metabolic Status
3.3. Impact of Adrenalectomy on Bone Status
3.4. Cognitive Impairement and Quality of Life
4. Discussion
4.1. MACS: From General Health Aspects to Various Biomarkers
4.2. General Management: From Surgery to Post-Operative Medication
4.3. Current Limitations and Future Research
5. Conclusions
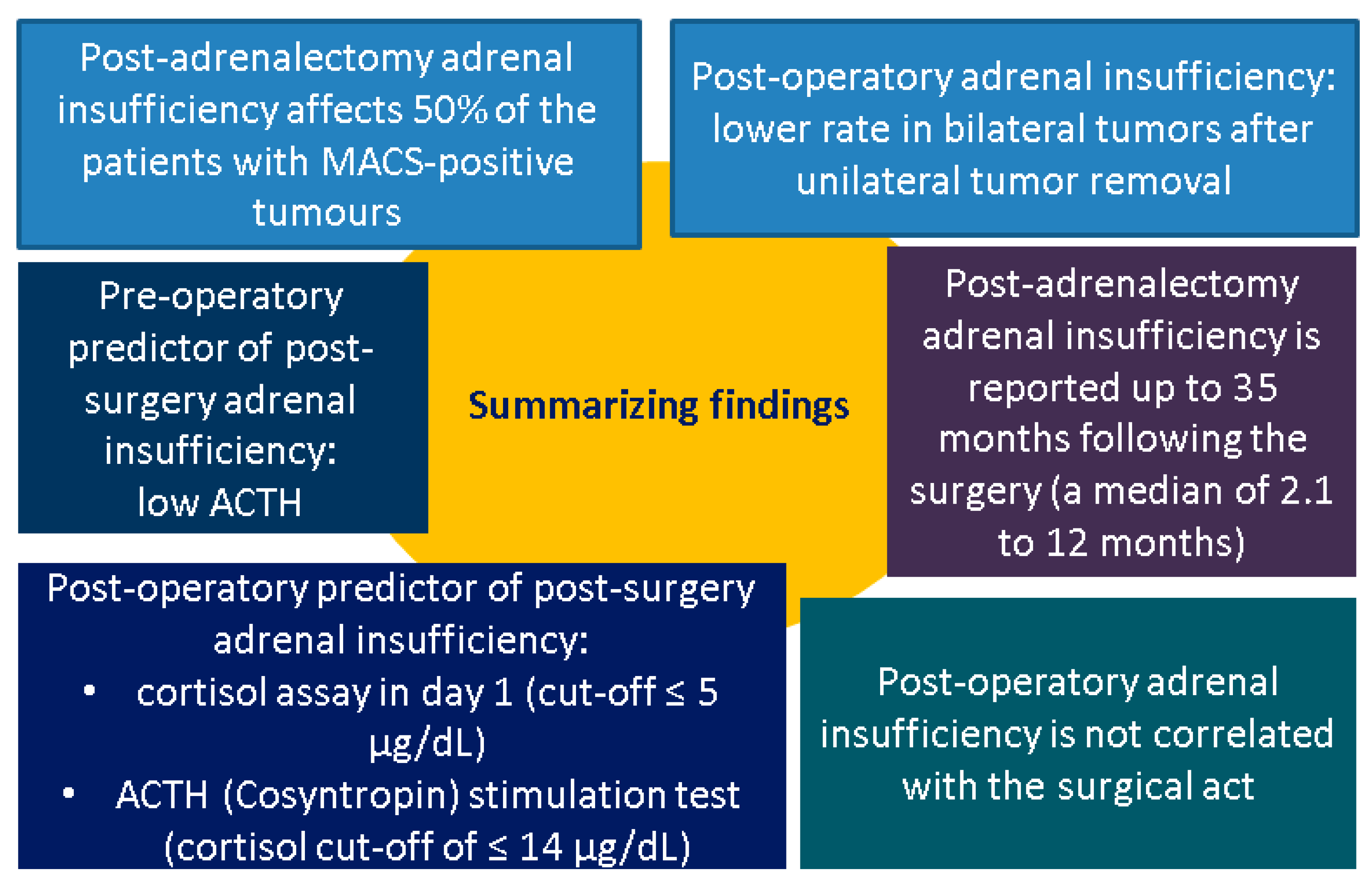
- A stratified strategy is encouraged for post-unilateral adrenalectomy in MACS, while post-operative adrenal insufficiency should be expected in almost half of the patients.
- A potential long-term improvement in hypertension, and even the glucose profile, is expected after tumour removal.
- Patients with bilateral adrenal tumours who are referred for unilateral adrenalectomy display a lower risk of adrenal insufficiency, but, in this distinct instance, additional imaging surveillance of the adrenal tumour is required, as well as considering genetic testing.
- Serum cortisol assays serve as the most useful biomarker as a pre-operatory predictor of adrenal post-surgery function (specifically, amid DST, and, potentially, in addition to baseline ACTH assessment). Post-surgery basal cortisol ( ± CST) helps inform the decision to employ glucocorticoids replacement from the first post-operative day and during follow-up. Serial testing every 3 months is a useful tool for up to 35 months post-surgery.
- Routinely prescribing glucocorticoid replacement for all patients who underwent a unilateral adrenalectomy may lead to over-prescription and potential negative effects, since not all MACS patients display post-adrenalectomy adrenal insufficiency. Hence, a personalized strategy is encouraged.
- The operation does not seem to be correlated with the post-surgery outcome regarding the biomarkers, including endocrine profile, cardio-metabolic, and osseous outcomes.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AI | adrenal incidentalomas |
| ACTH | adrenocorticotropic hormone |
| ACS | autonomous cortisol secretion |
| CS | Cushing’s syndrome |
| CTX | C-terminal telopeptide |
| CI | confidence interval |
| CST | cosyntropin stimulation test |
| DST | dexamethasone suppression test |
| DDD | defined daily dose |
| F/M | female-to-male ratio |
| IQR | interquartile interval |
| HPA | hypothalamic–pituitary–adrenal |
| LDDST | low dose dexamethasone suppression test |
| LDL | low-density lipoprotein |
| LH | luteinizing hormone |
| MACS | mild autonomous cortisol secretion |
| MSC | midnight serum cortisol |
| NFA | non-functioning adrenal tumours |
| N | number of patients |
| NA | not available |
| OR | odds ratio |
| PA | primary aldosteronism |
| P1NP | type 1 procollagen amino terminal peptide |
| PACS | possible autonomous cortisol secretion |
| PSH | postsurgical (unilateral adrenalectomy) hypocortisolism |
| POD1 | postoperative day 1 cortisol |
| ROC | receiver operating characteristic |
| SD | standard deviation |
| y | years |
| UFC | urinary free cortisol |
| vs. | versus |
Appendix A

| Reference | Perioperative Characteristics | Perioperative Hormonal Assessment |
|---|---|---|
| [32] | Laparoscopic or laparotomic adrenalectomy was decided depending on the size (N = 31 for adenoma size > 4 cm and N = 29 for evidence of hypercortisolism) There were no perioperative complications following surgery N1 vs. N2 Hydrocortisone dose during substitutive therapy period (mg/day): 20.9 ± 2.6 vs. 20.9 ± 2.3, p = 0.932 Hydrocortisone replacement = all patients Hydrocortisone dose = 100 mg intravenously, during surgery Cortisone acetate = 25–37.5 mg/day orally Postsurgical hypocortisolism = 39 patients were retested at 6, 12, 18, 24, and 36 months by low-dose corticotropin stimulation test in 6, 15, 9, 7, and 2 patients. | N1 vs. N2 ACTH pg/mL: 9.6 ± 5.7 (1.9–26.9) vs. 9.0 ± 4.4 (5.0–23.8), p = 0.665 ACTH > 26.9 pg/mL: 0 (0.0) vs. 1 (1.7), p = 0.650 1 mg-DST (µg/dL): 4.6 ± 3.5 (1.2–13.7) vs. 3.2 ± 2.1 (0.9–9.0), p = 0.098 1 mg-DST < 1.2 µg/dL: 0 (0.0) vs. 9 (42.9), p < 0.0001 UFC (µg/24 h): 68.2 ± 45.2 (10.4–189.6) vs. 51.3 ± 32.4 (10.0–120.0), p = 0.136 UFC < 10.4 µg/24 h: 0 (0.0) vs. 2 (9.5), p = 0.119 MSC (µg/dL): 6.0 ± 3.1 (1.2–12.5) vs. 3.4 ± 2.0 (1.0–8.0), p = 0.001 MSC < 1.2 µg/dL: 0 (0.0) vs. 1 (4.8), p = 0.350 1 mg DST cortisol < 1.2 µg/dL had lower rates of dyslipidemia and a better metabolic profile |
| [33] | N1 vs. N2 Glucocorticoid replacement was lower in N1 < N2: 59% vs. 89%, p = 0.003 Treatment durations were shorter in N1 < N2: 4.4 ± 3.8 vs. 10.7 ± 18.0 months, p = 0.04 | N1 vs. N2 Postoperative serum cortisol levels had greater values N1 > N2: 8.0 ± 5.7 vs. 5.0 ± 2.6 µg/dL, p = 0.03 |
| [34] | N1 vs. N2 vs. N3 Postoperative length of hospital (days), median (IQR): 3 (2–5) vs. 3 (2–3) vs. 2 (2–4) Postoperative treatment due to adrenal insufficiency, postoperatively: 72.8% vs. 59.5% vs. 10.5% Postoperative treatment due to adrenal insufficiency, first follow-up: 71.9% vs. 50% vs. 14.4% Surgical technique open/endoscopic: 5.6%/94.4% vs. 8.9%/91.1% vs. 14.3/85.7 | NA |
| [35] | Glucocorticoid replacement was started in patients who developed adrenal insufficiency. Prevalence of postoperative adrenal insufficiency = 25.9% | N1 vs. N2 At the time of diagnosis, both groups had similar cortisol metabolism. However, differences were observed after surgery: Basal cortisol (µg/dL): 12.8 (0.8–24.7) vs. 18.15 (12.1–25.5), p = 0.07 1 mg DST (µg/dL): 1.1 (0.5–8.7) vs. 2.9 (2.1–4.9), p = 0.003 ACTH (pg/mL): 20 (9–53) vs. 6 (1–9), p = 0.001 24 h UFC (nmol/24 h): 77 (28–121) vs. 85.5 (53–173), p = 0.41 Salivary cortisol (µg/dL): 0.15 (0.06–0.54) vs. 0.2 (0.09–0.31), p = 0.53 DHEA-S (µg/dL): 120 (15–129) vs. 72 (22–89), p = 0.62 |
| [36] | N1 vs. N2 vs. N3 vs. N4 Need for postoperative glucocorticoid replacement: 57% vs. 74% vs. 5% vs. 50%, p = 0.001 Duration glucocorticoid replacement, months: 2.1 (0.8–4.6) vs. 6.0 (1.4–17.1) vs. 1 vs. 0.8 (0.7–2.2), p = 0.010 All patients who had abnormal POD1-CST were given replacement glucocorticoids. Hydrocortisone daily dose = 30 mg | N1 vs. N2 vs. N3 vs. N4 Abnormal POD1: 55% vs. 67% vs. 14% vs. 42%, p < 0.001 POD1-CST identifies patients with hypercortisolism who are at risk of adrenal insufficiency after unilateral adrenalectomy, allowing for selective glucocorticoid replacement. |
| [38] | Laparoscopic adrenalectomy = all patients There were no perioperative complications following surgery Hydrocortisone replacement = all patients, 2 months, and then adrenal function was regularly evaluated by corticotropin test Prevalence of adrenal insufficiency = 40% The mean duration of impaired adrenal function was 12.3 ± 9.0 (6–35) months | Follow-up: 6 months N1 vs. N2 ACTH (pg/mL): 26.0 ± 10.6 vs. 11.6 ± 4.9, p < 0.0001 1 mg DST (nmol/L): 19.3 ± 5.5 vs. 85.6 ± 27.6, p < 0.0001 UFC (nmol/24 h): 48.8 ± 27.6 vs. 60.2 ± 32.3, p = 0.22 UFC/UFC ratio: 0.22 ± 0.10 vs. 0.26 ± 0.15, p = 0.61 Patients with hypoadrenalism showed baseline 1 mg DST levels comparable to patients without (3.7 ± 0.7 vs. 3.0 ± 1, p = 0.107). |
| [39] | N1′ vs. N2′ vs. N3′ Duration of inpatient hospital stay (days): 6 ± 12 vs. 5 ± 20 vs. 5.5 ± 10, p = 0.465 Complications: 30% vs. 20% vs. 7.1%, p = 0.275 Postoperative adrenal insufficiency: 4.5% vs. 42.9% vs. 64.3%, p < 0.001 Duration of adrenal insufficiency (months): 47 vs. 4.5 ± 40 vs. 17 ± 130, p = 0.310 Minimally invasive surgery (N,%): 86.4% vs. 89.5% vs. 91.7%, p = 0.539 N’ Laparoscopic surgery = 71.7% Median postoperative follow-up = 72 (6–214) months. Low-grade postoperative complications = 20.4% Acute pancreatitis = 2 Allergic reaction = 4 Hypokalemia = 2 Hypoxia = 2 Intestinal atony = 2 Large hematoma = 2 Lymph fistula = 4 Pneumonia = 2 Wound infection = 2 | NA |
| [40] | The laparotomic or laparoscopic method was chosen based on the size of the adrenal adenoma and the patient’s clinical features. Postoperative adrenal insufficiency = 81.2% (N = 26 of these N1 = 3, N2 = 23) Recovery within 6 weeks = 53.8% (N = 14 of these N1 = 3, N2 = 11) Recovery within 6 months = 16.6% (N2 = 2) Recovery within 1 year after surgery = 25% (N2 = 3) Without recovery of adrenal function at the end of follow-up = 26. 9% (N2 = 7) Hydrocortisone replacement = all patients Hydrocortisone daily dose = 25–37.5 mg | ROC curve identified a 1 mg DST test threshold of ≤4.7 µg/dL predicting 6-week recovery with 89.5% sensitivity and 72.7% specificity (area under curve 0.87; 95% CI 66.9–98.7, p < 0.001)-best predicted HPA axis recovery |
| [41] | Retroperitoneoscopic adrenalectomy = all patients (partial adrenalectomy = 92.7%, total adrenalectomy = 7.3%) Perioperative complication = one patient with type 2 diabetes mellitus had a delayed healing of the surgical incision. Follow-up: 12 months Glucocorticoid replacement was not necessary during the follow-up. | NA |
| [42] | N1 vs. N2 vs. N3 vs. N4 Received perioperative dexamethasone (4–10 mg): 36% vs. 32% vs. 27% vs. 33% Median days on glucocorticoid replacement (IQR): 246 (116–530) vs. 55 (36–133) vs. 81 (74–206) vs. 26 (15–36), p < 0.01 Patients with secondary adrenal insufficiency on CST received hydrocortisone at a standard dose of 20 mg in the morning and 10 mg in the evening. | N1 vs. N2 vs. N3 vs. N4 Median POD1 ACTH (pg/mL): 8.2 (3.6–29) vs. 12.4 (3.6–29.4) vs. 7.5 (5.6–10.5) vs. 13.8 (5.8–19.6), p = 0.316 Median POD1 basal cortisol (μg/dL): 5.0 (1.3 -12.3) vs. 8.5 (3.2–13.1) vs. 5.5 (1.6–13.3) vs. 11.4 (2.4–15.1), p = 0.256 Abnormal CST: 62% vs. 50% vs. 32% vs. 14%, p = 0.043 Using POD1 CST instead of basal cortisol levels alone helped identify people who were at risk for secondary adrenal insufficiency. |
| [43] | Minimally invasive adrenalectomy = all patients Hydrocortisone replacement = all patients Hydrocortisone daily dose = 50 mg of hydrocortisone 30 min before surgery, every 8 h on the same day, on the day after every 12 h, and then reduced to 25 mg every 12 h. Post-adrenalectomy adrenal insufficiency was assessed 5 days after surgery using a 250 μg corticotropin stimulation test, with peak cortisol levels ≤ 18 µg/dL. Prevalence of adrenal insufficiency = 67.4% There were no perioperative complications following surgery | NA |
| [44] | Laparoscopic unilateral adrenalectomy = all patients Hydrocortisone replacement = all patients Hydrocortisone daily dose = at discharge, patients received 20–30 mg/day, this dose was tapered by 2.5–5 mg/day every 2–4 weeks, and HPA returned to normal within 6 months after surgery There were no perioperative complications following surgery | NA |
| Reference | Impact of Adrenalectomy on Cardiovascular and Metabolic Morbidity in Patients with MACS or NFA |
|---|---|
| [34] | Median follow-up, N1 vs. N2 vs. N3: 3 (0–9.9) y vs. 2.6 (0–9.6) y vs. 3.2 (0–9.9) y Defined daily dose (DDD) was used to calculate drug consumption per patient-year, based on dispensed prescriptions the year before adrenalectomy and annually after adrenalectomy. N1 mean DDD difference (SD), p-value Hypertension: 198.4 (728.1), p = 0.003, increased medication at one year postoperatively Diabetes: 22.8 (184.7), p = 0.166 Hyperlipidemia: −59.4 (306.6), p = 0.013, decreased medication Antibiotics: 3.5 (47.9), p = 0.412 N2 mean DDD difference (SD), p-value Hypertension: 96.4 (598.4), p = 0.286 Diabetes: −10.6 (164.7), p = 0.668 Hyperlipidemia: 81.6 (389.2), p = 0.167 Antibiotics: −2.5 (22.5), p = 0.464 N3 mean DDD difference (SD), p-value Hypertension: 184.2 (510.0), p < 0.001, increased medication Diabetes: 0.624, p = 0.624 Hyperlipidaemia: 29.2 (268.3), p = 0.281 Antibiotics: 2.5 (19.8), p = 0.205 |
| [35] | N1 vs. N2 Median duration of follow-up: 21 (2–126) months vs. 48 (10–88) months, p = 0.3 Diabetes mellitus: 40.7% vs. 37.5%, p = 0.602 Improvement of diabetes mellitus: 45% vs. 0, p = 0.12 Hypertension: 70.4% vs. 87.5%, p = 0.31 Improvement of hypertension: 68.4% vs. 0, p = 0.002 Hyperlipidemia: 29.6% vs. 37.5%, p = 0.49 |
| [37] | The proportion of patients who initiated: N1′ vs. N1″ Antihypertensive treatment: 0% vs. 9.5%, p = 0.746 Hypoglycemic drugs: 0% vs. 4.7%, p = 0.586 Lipid-lowering medications: 16.7% vs. 13.6%, p = 0.833 N2′ vs. N2″ Antihypertensive treatment: 0% vs. 11.6%, p = 0.342 Hypoglycemic drugs: 0% vs. 6.8%, p = 0.315 Lipid-lowering medications: 36.4% vs. 22.4%, p = 0.317 |
| [38] | N1′ vs. N2′ Improvement of blood pressure control: 68% vs. 13.4%, p = 0.001 Worsening of blood pressure control: 4% vs. 26.7, p = 0.03 The surgical approach was independently associated with the improvement of blood pressure control (OR = 3.0, 95%CI: 3.8–108.3, p < 0.001) Improvement of glycometabolic control: 28% vs. 3.3%, p = 0.02 Worsening of glycometabolic control: 8% vs. 20%, p = 0.12 Amelioration of blood pressure and/or glycometabolic control: 68% vs. 17%, p < 0.001 Worsening blood pressure and/or glycometabolic control: 40% vs. 12%, p = 0.03 |
| [39] | Baseline, N′ vs. N″ Arterial hypertension: 77% vs. 74.9%, p = 0.731 Diabetes mellitus: 18% vs. 21.1%, p = 0.941 Dyslipidemia: 47.5% vs. 46.5%, p = 0.868 Obesity: 34.5% vs. 34.6%, p = 0.883 Last follow-up, N′ vs. N″ Arterial hypertension: 61.7% vs. 74.9%, p < 0.05 Diabetes mellitus: 26.2% vs. 30.2%, p = 0.691 Dyslipidemia: 44.3% vs. 53.8%, p = 0.442 Obesity: 35.6% vs. 38.5%, p = 0.195 |
| [41] | One year after surgery Improvement in hypertension = 71 patients (57.7%) Blood pressure returned to normal levels without antihypertensive drugs = 21 patients (17.1%) Conservative management 10 patients (5.4%) complained about worsening of their blood pressure condition, and the type/dose of antihypertensive drugs was increased |
| [43] | Median follow-up: 48 (3–66) months N1 vs. N2 Improved Weight control: 32.6% vs. 6.5%, p = 0.002 Glucose control: 45.7% vs. 15.2%, p = 0.002 Blood pressure control: 45.7% vs. 23.9%, p = 0.029 Dyslipidemia control: 26.1% vs. 19.6%, p = 0.456 Worsened Weight control: 6.5% vs. 19.6%, p = 0.063 Glucose control: 10.9% vs. 43.5%, p < 0.001 Blood pressure control: 19.6% vs. 50%, p = 0.002 Dyslipidemia control: 34.8% vs. 47.8%, p = 0.204 |
| [44] | Follow-up: 12 months N2′ vs. N2″ Overweight/obesity: 54.5% vs. 50%, p = 1.000 Impaired glucose regulation/Type 2 diabetes mellitus: 45.5% vs. 33.3%, p = 1.000 Hypertension: 45.5% vs. 66.7%, p = 0.620 Dyslipidemia: 63.6% vs. 83.3%, p = 0.600 |
| Reference | Impact of Adrenalectomy on Bone Status |
|---|---|
| [31] | Median follow-up: 37 (6–92) weeks Osteocalcin: mean differences of 8.18 ng/mL (SD = 6.74, p = 0.04) CTX: mean difference of 0.14 ng/mL (SD = 0.12, p = 0.05) PINP: mean difference of 1.78 µg/L (SD = 35.4, p = 0.75) Sclerostin: mean difference of 107 pg/mL (SD = 181, p = 0.24) |
| [34] | Median follow-up, N1 vs. N2 vs. N3: 3 (0–9.9) y vs. 2.6 (0–9.6) y vs. 3.2 (0–9.9) y. DDD was used to calculate drug consumption per patient-year, based on dispensed prescriptions the year before adrenalectomy and annually after adrenalectomy. N1 mean DDD difference (SD), p-value Osteoporosis: -14.3 (102.7), p = 0.119 N2 mean DDD difference (SD), p-value Osteoporosis: 7.5 (51.5), p = 0.336 N3 mean DDD difference (SD), p-value Osteoporosis: 5.7 (31.0), p = 0.072 |
| [44] | Follow-up: 12 months N2′ vs. N2″ Osteopenia/osteoporosis: 63.6% vs. 50%, p = 0.644 |
| Reference | Impact of Adrenalectomy on the Cognitive Function: Outcomes |
|---|---|
| [34] | Median follow-up, N1 vs. N2 vs. N3: 3 (0–9.9) y vs. 2.6 (0–9.6) y vs. 3.2 (0–9.9) y. DDD was used to calculate drug consumption per patient-year, based on dispensed prescriptions the year before adrenalectomy and annually after adrenalectomy. N1 mean DDD difference (SD), p-value Depressive disease: −30.3 (226.7), p = 0.134 N2 mean DDD difference (SD), p-value Depressive disease: −47.6 (153.2), p = 0.043, decreased medication N3 mean DDD difference (SD), p-value Depressive disease: 4.1 (171.5), p = 0.814 |
| [44] | Follow-up: 12 months N2′ vs. N2″ Global cognition (scores) Mini-Mental State Examination: 29.5 ± 0.9 vs. 28.5 ± 1.4, p = 0.726 Montreal Cognitive Assessment: 27.8 ± 1.8 vs. 26.2 ± 1.5, p = 0.062 Repeatable Battery for the Assessment of Neuropsychological Status: 107.0 ± 13.8 vs. 97.3 ± 10.6, p = 0.035 Visuospatial/constructional: 113.0 ± 9.2 vs. 96.2 ± 12.3, p = 0.033 Delayed memory: 104.1 ± 10.4 vs. 93.1 ± 14.5, p = 0.025 Immediate memory: 94.1 ± 18.1 vs. 84.3 ± 15.2, p =0.282 Language: 103.4 ± 11.0 vs. 100.5 ± 7.9, p = 0.666 Attention: 111.3 ± 9.7 vs. 117.7 ± 5.5, p = 0.211 Working memory: 14.8 ± 2.1 vs. 14.0 ± 2.0, p = 0.751 Executive function: 58.4 ± 23.9 vs. 59.6 ± 14.7, p = 0.579 Processing speed: 104.8 ± 62.6 vs. 75.2 ± 33.2, p = 0.596 |
References
- Mete, O.; Erickson, L.A.; Juhlin, C.C.; de Krijger, R.R.; Sasano, H.; Volante, M.; Papotti, M.G. Overview of the 2022 WHO Classification of Adrenal Cortical Tumors. Endocr. Pathol. 2022, 33, 155–196. [Google Scholar] [CrossRef] [PubMed]
- Ebbehoj, A.; Li, D.; Kaur, R.J.; Zhang, C.; Singh, S.; Li, T.; Atkinson, E.; Achenbach, S.; Khosla, S.; Arlt, W.; et al. Epidemiology of adrenal tumours in Olmsted County, Minnesota, USA: A population-based cohort study. Lancet Diabetes Endocrinol. 2020, 8, 894–902. [Google Scholar] [CrossRef] [PubMed]
- Jing, Y.; Hu, J.; Luo, R.; Mao, Y.; Luo, Z.; Zhang, M.; Yang, J.; Song, Y.; Feng, Z.; Wang, Z.; et al. Prevalence and Characteristics of Adrenal Tumors in an Unselected Screening Population: A Cross-Sectional Study. Ann. Intern. Med. 2022, 175, 1383–1391. [Google Scholar] [CrossRef] [PubMed]
- Elhassan, Y.S.; Alahdab, F.; Prete, A.; Delivanis, D.A.; Khanna, A.; Prokop, L.; Murad, M.H.; O’Reilly, M.W.; Arlt, W.; Bancos, I. Natural History of Adrenal Incidentalomas with and Without Mild Autonomous Cortisol Excess: A Systematic Review and Meta-analysis. Ann. Intern. Med. 2019, 171, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Prete, A.; Subramanian, A.; Bancos, I.; Chortis, V.; Tsagarakis, S.; Lang, K.; Macech, M.; Delivanis, D.A.; Pupovac, I.D.; Reimondo, G.; et al. Cardiometabolic Disease Burden and Steroid Excretion in Benign Adrenal Tumors: A Cross-Sectional Multicenter Study. Ann. Intern. Med. 2022, 175, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Di Dalmazi, G.; Vicennati, V.; Pizzi, C.; Mosconi, C.; Tucci, L.; Balacchi, C.; Cosentino, E.R.; Paolisso, P.; Fanelli, F.; Gambineri, A.; et al. Prevalence and Incidence of Atrial Fibrillation in a Large Cohort of Adrenal Incidentalomas: A Long-Term Study. J. Clin. Endocrinol. Metab. 2020, 105, e2770–e2777. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.D.; Li, D.; Kaur, R.J.; Ebbehoj, A.; Singh, S.; Atkinson, E.J.; Achenbach, S.J.; Young, W.F.; Arlt, W.; Rocca, W.A.; et al. Cardiometabolic Outcomes and Mortality in Patients with Adrenal Adenomas in a Population-based Setting. J. Clin. Endocrinol. Metab. 2021, 106, 3320–3330. [Google Scholar] [CrossRef] [PubMed]
- Zavatta, G.; Vicennati, V.; Altieri, P.; Tucci, L.; Colombin, G.; Coscia, K.; Mosconi, C.; Balacchi, C.; Fanelli, F.; Malagrinò, M.; et al. Mild autonomous cortisol secretion in adrenal incidentalomas and risk of fragility fractures: A large cross-sectional study. Eur. J. Endocrinol. 2023, 188, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Kaur, R.J.; Zhang, C.D.; Ebbehoj, A.; Singh, S.; Atkinson, E.J.; Achenbach, S.J.; Rocca, W.; Khosla, S.; Bancos, I. Risk of bone fractures after the diagnosis of adrenal adenomas: A population-based cohort study. Eur. J. Endocrinol. 2021, 184, 597–606. [Google Scholar] [CrossRef] [PubMed]
- Dumitru, N.; Carsote, M.; Cocolos, A.; Petrova, E.; Olaru, M.; Dumitrache, C.; Ghemigian, A. The Link Between Bone Osteocalcin and Energy Metabolism in a Group of Postmenopausal Women. Curr. Health Sci. J. 2019, 45, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Deutschbein, T.; Reimondo, G.; Di Dalmazi, G.; Bancos, I.; Patrova, J.; Vassiliadi, D.A.; Nekić, A.B.; Debono, M.; Lardo, P.; Ceccato, F.; et al. Age-dependent and sex-dependent disparity in mortality in patients with adrenal incidentalomas and autonomous cortisol secretion: An international, retrospective, cohort study. Lancet Diabetes Endocrinol. 2022, 10, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Patrova, J.; Mannheimer, B.; Lindh, J.D.; Falhammar, H. Mortality in Patients with Nonfunctional Adrenal Tumors. JAMA Intern. Med. 2023, 183, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Pelsma, I.C.M.; Fassnacht, M.; Tsagarakis, S.; Terzolo, M.; Tabarin, A.; Sahdev, A.; Newell-Price, J.; Marina, L.; Lorenz, K.; Bancos, I.; et al. Comorbidities in mild autonomous cortisol secretion and the effect of treatment: Systematic review and meta-analysis. Eur. J. Endocrinol. 2023, 189, S88–S101. [Google Scholar] [CrossRef] [PubMed]
- Yozamp, N.; Vaidya, A. Assessment of mild autonomous cortisol secretion among incidentally discovered adrenal masses. Best. Pract. Res. Clin. Endocrinol. Metab. 2021, 35, 101491. [Google Scholar] [CrossRef] [PubMed]
- Carsote, M.; Valea, A.; Dumitru, N.; Terzea, D.; Petrova, E.; Albu, S.; Buruiana, A.; Ghemigian, A. Metastases in daily endocrine practice. Arch. Balk. Med. Union. 2016, 51, 476–480. [Google Scholar]
- Hayes, G. Update on Adrenalectomy. Vet. Clin. N. Am. Small Anim. Pract. 2022, 52, 473–487. [Google Scholar] [CrossRef] [PubMed]
- Yip, L.; Duh, Q.Y.; Wachtel, H.; Jimenez, C.; Sturgeon, C.; Lee, C.; Velázquez-Fernández, D.; Berber, E.; Hammer, G.D.; Bancos, I.; et al. American Association of Endocrine Surgeons Guidelines for Adrenalectomy: Executive Summary. JAMA Surg. 2022, 157, 870–877. [Google Scholar] [CrossRef] [PubMed]
- Lewis, A.; Thant, A.A.; Aslam, A.; Aung, P.P.M.; Azmi, S. Diagnosis and management of adrenal insufficiency. Clin. Med. 2023, 23, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Broersen, L.H.A.; van Haalen, F.M.; Kienitz, T.; Dekkers, O.M.; Strasburger, C.J.; Pereira, A.M.; Biermasz, N.R. The incidence of adrenal crisis in the postoperative period of HPA axis insufficiency after surgical treatment for Cushing’s syndrome. Eur. J. Endocrinol. 2019, 181, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Hahner, S.; Ross, R.J.; Arlt, W.; Bancos, I.; Burger-Stritt, S.; Torpy, D.J.; Husebye, E.S.; Quinkler, M. Adrenal insufficiency. Nat. Rev. Dis. Primers 2021, 7, 19. [Google Scholar] [CrossRef] [PubMed]
- Husebye, E.S.; Pearce, S.H.; Krone, N.P.; Kämpe, O. Adrenal insufficiency. Lancet 2021, 397, 613–629. [Google Scholar] [CrossRef] [PubMed]
- Kubo, Y.; Sone, M.; Katabami, T.; Izawa, S.; Ichijo, T.; Tsuiki, M.; Okamura, S.; Yoshimoto, T.; Otsuki, M.; Takeda, Y.; et al. Predictor of Steroid Replacement Duration after Removal of Cortisol-producing Adenoma. Intern. Med. 2025, 64, 1476–1484. [Google Scholar] [CrossRef] [PubMed]
- Beuschlein, F.; Else, T.; Bancos, I.; Hahner, S.; Hamidi, O.; van Hulsteijn, L.; Husebye, E.S.; Karavitaki, N.; Prete, A.; Vaidya, A.; et al. European Society of Endocrinology and Endocrine Society Joint Clinical Guideline: Diagnosis and therapy of glucocorticoid-induced adrenal insufficiency. Eur. J. Endocrinol. 2024, 190, G25–G51. [Google Scholar] [CrossRef] [PubMed]
- Utsumi, T.; Iijima, S.; Sugizaki, Y.; Mori, T.; Somoto, T.; Kato, S.; Oka, R.; Endo, T.; Kamiya, N.; Suzuki, H. Laparoscopic adrenalectomy for adrenal tumors with endocrine activity: Perioperative management pathways for reduced complications and improved outcomes. Int. J. Urol. 2023, 30, 818–826. [Google Scholar] [CrossRef] [PubMed]
- Nachawi, N.; Li, D.; Lansang, M.C. Glucocorticoid-induced adrenal insufficiency and glucocorticoid withdrawal syndrome: Two sides of the same coin. Clevel. Clin. J. Med. 2024, 91, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Theiler-Schwetz, V.; Prete, A. Glucocorticoid withdrawal syndrome: What to expect and how to manage. Curr. Opin. Endocrinol. Diabetes Obes. 2023, 30, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.D.; Li, D.; Singh, S.; Suresh, M.; Thangamuthu, K.; Nathani, R.; Achenbach, S.J.; Atkinson, E.J.; Van Gompel, J.J.; Young, W.F.; et al. Glucocorticoid withdrawal syndrome following surgical remission of endogenous hypercortisolism: A longitudinal observational study. Eur. J. Endocrinol. 2023, 188, 592–602. [Google Scholar] [CrossRef] [PubMed]
- Iriarte-Durán, M.B.; Donato, S.; Herrera, A.; Vega, A.; Jiménez Casinello, J.M.; Marazuela, M.; Araujo-Castro, M. The impact of mild autonomous cortisol secretion and proposed interventions. Expert Rev. Endocrinol Metab. 2025, 20, 251–266. [Google Scholar] [CrossRef] [PubMed]
- Ngo, B.; Liu, T.; Lau, E. Imaging of Adrenal Incidentalomas: What Actually Happens in Everyday Clinical Practice? J. Med. Imaging Radiat. Oncol. 2025, 69, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Turan Erdogan, B.; Evranos Ogmen, B.; Sacikara, M.; Aydin, C.; Topaloglu, O.; Ersoy, R.; Cakir, B. The relationship between mild autonomous cortisol secretion and metabolic diseases in cases with adrenal incidentaloma. Endokrynol. Pol. 2025, 76, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Athimulam, S.; Delivanis, D.; Thomas, M.; Young, W.F.; Khosla, S.; Drake, M.T.; Bancos, I. The Impact of Mild Autonomous Cortisol Secretion on Bone Turnover Markers. J. Clin. Endocrinol. Metab. 2020, 105, 1469–1477. [Google Scholar] [CrossRef] [PubMed]
- Eller-Vainicher, C.; Morelli, V.; Aresta, C.; Salcuni, A.S.; Falchetti, A.; Carnevale, V.; Persani, L.; Scillitani, A.; Chiodini, I. Defining Nonfunctioning Adrenal Adenomas on the Basis of the Occurrence of Hypocortisolism after Adrenalectomy. J. Endocr. Soc. 2020, 4, bvaa079. [Google Scholar] [CrossRef] [PubMed]
- Foster, T.; Bancos, I.; McKenzie, T.; Dy, B.; Thompson, G.; Lyden, M. Early assessment of postoperative adrenal function is necessary after adrenalectomy for mild autonomous cortisol secretion. Surgery 2021, 169, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Thompson, L.H.; Ranstam, J.; Almquist, M.; Nordenström, E.; Bergenfelz, A. Impact of Adrenalectomy on Morbidity in Patients with Non-Functioning Adrenal Cortical Tumours, Mild Hypercortisolism and Cushing’s Syndrome as Assessed by National and Quality Registries. World J. Surg. 2021, 45, 3099–3107. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, N.; Tazegul, G.; Sari, R.; Avsar, E.; Altunbas, H.; Balci, M.K. Effectiveness of unilateral adrenalectomy in bilateral adrenal incidentaloma patients with subclinical hypercortisolemia. Acta Endocrinol. 2021, 17, 479–485. [Google Scholar] [CrossRef] [PubMed]
- DeLozier, O.M.; Dream, S.Y.; Findling, J.W.; Carroll, T.B.; Evans, D.B.; Wang, T.S. Selective Glucocorticoid Replacement Following Unilateral Adrenalectomy for Hypercortisolism and Primary Aldosteronism. J. Clin. Endocrinol. Metab. 2022, 107, e538–e547. [Google Scholar] [CrossRef] [PubMed]
- Araujo-Castro, M.; Mínguez Ojeda, C.; Sánchez Ramírez, M.N.; Gómez Dos Santos, V.; Pascual-Corrrales, E.; Fernández-Argüeso, M. Adrenalectomy improves blood pressure control in nonfunctioning adrenal incidentalomas and glycemic and lipid control in patients with autonomous cortisol secretion. Endocrine 2022, 78, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Morelli, V.; Frigerio, S.; Aresta, C.; Passeri, E.; Pugliese, F.; Copetti, M.; Barbieri, A.M.; Fustinoni, S.; Polledri, E.; Corbetta, S.; et al. Adrenalectomy Improves Blood Pressure and Metabolic Control in Patients with Possible Autonomous Cortisol Secretion: Results of a RCT. Front. Endocrinol. 2022, 13, 898084. [Google Scholar] [CrossRef] [PubMed]
- Remde, H.; Kranz, S.; Morell, S.M.; Altieri, B.; Kroiss, M.; Detomas, M.; Fassnacht, M.; Deutschbein, T. Clinical course of patients with adrenal incidentalomas and cortisol autonomy: A German retrospective single center cohort study. Front. Endocrinol. 2023, 14, 1123132. [Google Scholar] [CrossRef] [PubMed]
- Bonaventura, I.; Tomaselli, A.; Angelini, F.; Ferrari, D.; De Alcubierre, D.; Hasenmajer, V.; Sbardella, E.; Cozzolino, A.; Paganini, A.M.; Isidori, A.M.; et al. Predicting postoperative hypocortisolism in patients with non-aldosterone-producing adrenocortical adenoma: A retrospective single-centre study. J. Endocrinol. Investig. 2024, 47, 1751–1762. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Yang, L.; Wang, X.; Bai, X.; Tuoheti, K.; Yisha, Z.; Hu, D.; Liu, T. Impact of adrenalectomy on hypertension in patients with nonfunctional adrenal tumors: A retrospective study. World J. Urol. 2024, 42, 441. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.; Zhang, C.D.; Hangge, P.T.; Yen, T.W.F.; Shaik, T.J.; Doffek, K.; Findling, J.W.; Carroll, T.; Evans, D.B.; Dream, S.Y.; et al. Cosyntropin Stimulation Testing is More Selective than Postoperative Day 1 Basal Cortisol for Diagnosing Secondary Adrenal Insufficiency After Unilateral Adrenalectomy. Ann. Surg. Oncol. 2024, 31, 6883–6892. [Google Scholar] [CrossRef] [PubMed]
- Koh, J.M.; Song, K.; Kwak, M.K.; Suh, S.; Kim, B.J.; Sung, T.Y.; Hong, J.H.; Jeong, B.C.; Kim, J.H.; Lee, S.H. Adrenalectomy Improves Body Weight, Glucose, and Blood Pressure Control in Patients with Mild Autonomous Cortisol Secretion: Results of an Randomized Controlled Trial by the Co-work of Adrenal Research (COAR) Study. Ann. Surg. 2024, 279, 945–952. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Zhao, W.; Zhang, W.; Tian, Z.; Zhang, Z.; Lou, Y.; Zhang, Z.; Yang, F.; Zhu, D.; Li, P. Comparable cognitive impairment was detected in MACS and CS and alleviated after remission of hypercortisolism in MACS. Front. Endocrinol. 2024, 15, 1373101. [Google Scholar] [CrossRef] [PubMed]
- Al-Jalabneh, T.; Al-Shawabkeh, O.; Al-Gwairy, I.; Abu-Zeitoun, O.; Al-Njadat, I.; Al-Soudi, M.; Zarour, A. Laparoscopic Versus Open Adrenalectomy: A Retrospective Comparative Study. Med. Arch. 2021, 75, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Hurtado, M.D.; Cortes, T.; Natt, N.; Young WFJr Bancos, I. Extensive clinical experience: Hypothalamic-pituitary-adrenal axis recovery after adrenalectomy for corticotropin-independent cortisol excess. Clin Endocrinol. 2018, 89, 721–733. [Google Scholar] [CrossRef] [PubMed]
- Gavriilidis, P.; Camenzuli, C.; Paspala, A.; Di Marco, A.N.; Palazzo, F.F. Posterior Retroperitoneoscopic Versus Laparoscopic Transperitoneal Adrenalectomy: A Systematic Review by an Updated Meta-Analysis. World J. Surg. 2021, 45, 168–179. [Google Scholar] [CrossRef] [PubMed]
- Suntornlohanakul, O.; Mandal, S.; Saha, P.; Saygili, E.S.; Asia, M.; Arlt, W.; Elhassan, Y.S.; Prete, A.; Ronchi, C.L. Presentation and management of patients with adrenal masses: A large tertiary centre experience. Eur. J. Endocrinol. 2024, 191, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Jia, J.; Yang, Z.; Teng, Z.; Han, Z. Efficacy and safety of laparoendoscopic single-site adrenalectomy versus conventional laparoscopic adrenalectomy: An updated systematic review and meta-analysis. Wideochir Inne Tech Maloinwazyjne 2022, 17, 20–34. [Google Scholar] [CrossRef] [PubMed]
- Green, R.L.; Gao, T.P.; Hamilton, A.E.; Kuo, L.E. Older age impacts outcomes after adrenalectomy. Surgery 2023, 174, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Allahwasaya, A.; Akhund, R.; Balachandra, S.; McLeod, C.; Lindeman, B.; Fazendin, J.; Gillis, A.; Zmijewski, P.; Chen, H. Adrenal Referral Pattern: Management of Patients with an Adrenal Incidentaloma. J. Surg. Res. 2024, 302, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Ren, X.; Nan, M.; Zhang, X. Evaluating the efficacy of surgical and conservative approaches in mild autonomous cortisol secretion: A meta-analysis. Front. Endocrinol. 2024, 15, 1399311. [Google Scholar] [CrossRef] [PubMed]
- Rusu, C.C.; Anton, F.; Valea, A.; Bondor, C.I. N-Terminal Pro-Brain Natriuretic Peptide Correlates with Ghrelin and Acyl-Ghrelin in Pre-Dialysis Chronic Kidney Disease. Int. J. Mol. Sci. 2024, 25, 5696. [Google Scholar] [CrossRef] [PubMed]
- Fallo, F.; Di Dalmazi, G.; Beuschlein, F.; Biermasz, N.R.; Castinetti, F.; Elenkova, A.; Fassnacht, M.; Isidori, A.M.; Kastelan, D.; Korbonits, M.; et al. Diagnosis and management of hypertension in patients with Cushing’s syndrome: A position statement and consensus of the Working Group on Endocrine Hypertension of the European Society of Hypertension. J. Hypertens. 2022, 40, 2085–2101. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Vella, A. Glucose metabolism in Cushing’s syndrome. Curr. Opin. Endocrinol. Diabetes Obes. 2020, 27, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Adamska, A.; Ulychnyi, V.; Siewko, K.; Popławska-Kita, A.; Szelachowska, M.; Adamski, M.; Buczyńska, A.; Krętowski, A.J. Cardiovascular risk factors in mild adrenal autonomous cortisol secretion in a Caucasian population. Endocr. Connect. 2022, 11, e220074. [Google Scholar] [CrossRef] [PubMed]
- Araujo-Castro, M.; Reincke, M.; Lamas, C. Epidemiology and Management of Hypertension and Diabetes Mellitus in Patients with Mild Autonomous Cortisol Secretion: A Review. Biomedicines 2023, 11, 3115. [Google Scholar] [CrossRef] [PubMed]
- Delivanis, D.A.; Athimulam, S.; Bancos, I. Modern Management of Mild Autonomous Cortisol Secretion. Clin. Pharmacol. Ther. 2019, 106, 1209–1221. [Google Scholar] [CrossRef] [PubMed]
- Beaupere, C.; Liboz, A.; Fève, B.; Blondeau, B.; Guillemain, G. Molecular Mechanisms of Glucocorticoid-Induced Insulin Resistance. Int. J. Mol. Sci. 2021, 22, 623. [Google Scholar] [CrossRef] [PubMed]
- Salehidoost, R.; Korbonits, M. Glucose and lipid metabolism abnormalities in Cushing’s syndrome. J. Neuroendocrinol. 2022, 34, e13143. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Feng, M.; Lu, L.; Zhao, Z.; Bao, X.; Deng, K.; Yao, Y.; Zhu, H.; Wang, R. Lipid Abnormalities in Patients With Cushing’s Disease and Its Relationship With Impaired Glucose Metabolism. Front. Endocrinol. 2021, 11, 600323. [Google Scholar] [CrossRef] [PubMed]
- Chiodini, I.; Falchetti, A.; Merlotti, D.; Eller Vainicher, C.; Gennari, L. Updates in epidemiology, pathophysiology and management strategies of glucocorticoid-induced osteoporosis. Expert. Rev. Endocrinol. Metab. 2020, 15, 283–298. [Google Scholar] [CrossRef] [PubMed]
- Nica, S.; Sionel, R.; Maciuca, R.; Csutak, O.; Ciobica, M.L.; Nica, M.I.; Chelu, I.; Radu, I.; Toma, M. Gender-Dependent Associations Between Digit Ratio and Genetic Polymorphisms, BMI, and Reproductive Factors. Rom. J. Mil. Med. 2025, 128, 78–86. [Google Scholar] [CrossRef]
- Anghel, D.; Ciobica, L.M.; Negru, M.M.; Jurcut, C.; Otlocan, L.; Coca, A. Bone mineral density and vitamin D levels in patients with rheumatoid arthritis. Osteoporos. Int. 2017, 28 (Suppl. S1), S435–S436. [Google Scholar]
- Yano, C.; Yokomoto-Umakoshi, M.; Fujita, M.; Umakoshi, H.; Yano, S.; Iwahashi, N.; Katsuhara, S.; Kaneko, H.; Ogata, M.; Fukumoto, T.; et al. Coexistence of bone and vascular disturbances in patients with endogenous glucocorticoid excess. Bone Rep. 2022, 17, 101610. [Google Scholar] [CrossRef] [PubMed]
- Popa, F.L.; Diaconu, C.; Canciu, A.; Ciortea, V.M.; Iliescu, M.G.; Stanciu, M. Medical management and rehabilitation in posttraumatic common peroneal nerve palsy. Balneo PRM Res. J. 2022, 13, 496. [Google Scholar] [CrossRef]
- Favero, V.; Eller-Vainicher, C.; Morelli, V.; Cairoli, E.; Salcuni, A.S.; Scillitani, A.; Corbetta, S.; Casa, S.D.; Muscogiuri, G.; Persani, L.; et al. Increased Risk of Vertebral Fractures in Patients with Mild Autonomous Cortisol Secretion. J. Clin. Endocrinol. Metab. 2024, 109, e623–e632. [Google Scholar] [CrossRef] [PubMed]
- Šojat, A.S.; Dunjić-Kostić, B.; Marina, L.V.; Ivović, M.; Radonjić, N.V.; Kendereški, A.; Ćirković, A.; Tančić-Gajić, M.; Arizanović, Z.; Mihajlović, S.; et al. Depression: Another cortisol-related comorbidity in patients with adrenal incidentalomas and (possible) autonomous cortisol secretion. J. Endocrinol. Investig. 2021, 44, 1935–1945. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Zhang, C.D.; Saini, J.; Singh, S.; Nathani, R.; Thangamuthu, K.; Suresh, M.; Atkinson, E.J.; Achenbach, S.J.; Van Gompel, J.; et al. Determinants of muscle function and health-related quality of life in patients with endogenous hypercortisolism: A cross-sectional study. Eur. J. Endocrinol. 2023, 188, 603–612. [Google Scholar] [CrossRef] [PubMed]
- Vasiliu, O. Therapeutic management of atypical antipsychotic-related metabolic dysfunctions using GLP-1 receptor agonists: A systematic review. Exp. Ther. Med. 2023, 26, 355. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Atkinson, E.J.; Achenbach, S.J.; LeBrasseur, N.; Bancos, I. Frailty in Patients with Mild Autonomous Cortisol Secretion is Higher Than in Patients with Nonfunctioning Adrenal Tumors. J. Clin. Endocrinol. Metab. 2020, 105, e3307–e3315. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Singh, S.; Zhang, C.D.; Kaur, R.J.; Ebbehoj, A.; Atkinson, E.J.; Achenbach, S.J.; Stricker, N.H.; Mielke, M.M.; Rocca, W.; et al. Risk of dementia and psychiatric or sleep disorders after diagnosis of adrenal adenomas: A population-based cohort study. Eur. J. Endocrinol. 2023, 189, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Araujo-Castro, M.; Hanzu, F.A.; Pascual-Corrales, E.; García Cano, A.M.; Marchan, M.; Escobar-Morreale, H.F.; Valderrabano, P.; Casals, G. Is the 1 mg-dexamethasone suppression test a precise marker of glucocorticoid excess and cardiometabolic risk in patients with adrenal incidentalomas? Endocrine 2023, 82, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Al-Waeli, D.; Alidrisi, H.; Mansour, A. Utilizing dehydroepiandrosterone sulfate and its ratio for detecting mild autonomous cortisol excess in patients with adrenal incidentaloma. J. Med. Life 2023, 16, 1456–1461. [Google Scholar] [CrossRef] [PubMed]
- Carafone, L.E.; Zhang, C.D.; Li, D.; Lazik, N.; Hamidi, O.; Hurtado, M.D.; Young, W.F., Jr.; Thomas, M.A.; Dy, B.M.; Lyden, M.L.; et al. Diagnostic Accuracy of Dehydroepiandrosterone Sulfate and Corticotropin in Autonomous Cortisol Secretion. Biomedicines 2021, 9, 741. [Google Scholar] [CrossRef] [PubMed]
- Valea, A.; Ghervan, C.; Morar, A.; Pop, D.D.; Carsote, M.; Albu, S.E.; Georgescu, C.E.; Chiorean, A. Hashimoto’s thyroiditis and breast cancer: Coincidence or correlation? Arch. Balk. Med. Union 2016, 51, 129–132. [Google Scholar]
- Araujo-Castro, M.; Casals, G.; Hanzu, F.A.; Pascual-Corrales, E.; García Cano, A.M.; Lanza, V.F.; Luis Del Rey Mejías, Á.; Marchan, M.; Escobar-Morreale, H.F.; Valderrabano, P. Characterisation of the urinary steroid profile of patients with nonfunctioning adrenal incidentalomas: A matched controlled cross-sectional study. Clin. Endocrinol. 2023, 98, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Berke, K.; Constantinescu, G.; Masjkur, J.; Kimpel, O.; Dischinger, U.; Peitzsch, M.; Kwapiszewska, A.; Dobrowolski, P.; Nölting, S.; Reincke, M.; et al. Plasma Steroid Profiling in Patients With Adrenal Incidentaloma. J. Clin. Endocrinol. Metab. 2022, 107, e1181–e1192. [Google Scholar] [CrossRef] [PubMed]
- Bancos, I.; Taylor, A.E.; Chortis, V.; Sitch, A.J.; Jenkinson, C.; Davidge-Pitts, C.J.; Lang, K.; Tsagarakis, S.; Macech, M.; Riester, A.; et al. Urine steroid metabolomics for the differential diagnosis of adrenal incidentalomas in the EURINE-ACT study: A prospective test validation study. Lancet Diabetes Endocrinol. 2020, 8, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Valea, A.; Carsote, M.; Moldovan, C.; Georgescu, C. Chronic autoimmune thyroiditis and obesity. Arch. Balk. Med. Union. 2018, 53, 64–69. [Google Scholar]
- Masjkur, J.; Gruber, M.; Peitzsch, M.; Kaden, D.; Di Dalmazi, G.; Bidlingmaier, M.; Zopp, S.; Langton, K.; Fazel, J.; Beuschlein, F.; et al. Plasma Steroid Profiles in Subclinical Compared with Overt Adrenal Cushing Syndrome. J. Clin. Endocrinol. Metab. 2019, 104, 4331–4340. [Google Scholar] [CrossRef] [PubMed]
- Ku, E.J.; Lee, C.; Shim, J.; Lee, S.; Kim, K.A.; Kim, S.W.; Rhee, Y.; Kim, H.J.; Lim, J.S.; Chung, C.H.; et al. Metabolic Subtyping of Adrenal Tumors: Prospective Multi-Center Cohort Study in Korea. Endocrinol. Metab. 2021, 36, 1131–1141. [Google Scholar] [CrossRef] [PubMed]
- Huayllas, M.K.P.; Smith, L.M.; Gallagher, J.C.; Netzel, B.C.; Singh, R.J.; Kater, C.E. Steroidogenesis in patients with adrenal incidentalomas: Extended steroid profile measured by liquid chromatography-mass spectrometry after ACTH stimulation and dexamethasone suppression. Clin. Endocrinol. 2021, 95, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Fassnacht, M.; Tsagarakis, S.; Terzolo, M.; Tabarin, A.; Sahdev, A.; Newell-Price, J.; Pelsma, I.; Marina, L.; Lorenz, K.; Bancos, I.; et al. European Society of Endocrinology clinical practice guidelines on the management of adrenal incidentalomas, in collaboration with the European Network for the Study of Adrenal Tumors. Eur. J. Endocrinol. 2023, 189, G1–G42. [Google Scholar] [CrossRef] [PubMed]
- Faillot, S.; Foulonneau, T.; Néou, M.; Espiard, S.; Garinet, S.; Vaczlavik, A.; Jouinot, A.; Rondof, W.; Septier, A.; Drougat, L.; et al. Genomic classification of benign adrenocortical lesions. Endocr. Relat. Cancer 2021, 28, 79–95. [Google Scholar] [CrossRef] [PubMed]
- Di Dalmazi, G.; Altieri, B.; Scholz, C.; Sbiera, S.; Luconi, M.; Waldman, J.; Kastelan, D.; Ceccato, F.; Chiodini, I.; Arnaldi, G.; et al. RNA Sequencing and Somatic Mutation Status of Adrenocortical Tumors: Novel Pathogenetic Insights. J. Clin. Endocrinol. Metab. 2020, 105, e4459–e4473. [Google Scholar] [CrossRef] [PubMed]
- Jouinot, A.; Armignacco, R.; Assié, G. Genomics of benign adrenocortical tumors. J. Steroid Biochem. Mol. Biol. 2019, 193, 105414. [Google Scholar] [CrossRef] [PubMed]
- Juhlin, C.C.; Bertherat, J.; Giordano, T.J.; Hammer, G.D.; Sasano, H.; Mete, O. What Did We Learn from the Molecular Biology of Adrenal Cortical Neoplasia? From Histopathology to Translational Genomics. Endocr. Pathol. 2021, 32, 102–133. [Google Scholar] [CrossRef] [PubMed]
- Little, D.W., 3rd; Dumontet, T.; LaPensee, C.R.; Hammer, G.D. β-catenin in adrenal zonation and disease. Mol. Cell. Endocrinol. 2021, 522, 111120. [Google Scholar] [CrossRef] [PubMed]
- Bouys, L.; Vaczlavik, A.; Jouinot, A.; Vaduva, P.; Espiard, S.; Assié, G.; Libé, R.; Perlemoine, K.; Ragazzon, B.; Guignat, L.; et al. Identification of predictive criteria for pathogenic variants of primary bilateral macronodular adrenal hyperplasia (PBMAH) gene ARMC5 in 352 unselected patients. Eur. J. Endocrinol. 2022, 187, 123–134. [Google Scholar] [CrossRef] [PubMed]
- Bertherat, J.; Bourdeau, I.; Bouys, L.; Chasseloup, F.; Kamenický, P.; Lacroix, A. Clinical, Pathophysiologic, Genetic, and Therapeutic Progress in Primary Bilateral Macronodular Adrenal Hyperplasia. Endocr. Rev. 2023, 44, 567–628. [Google Scholar] [CrossRef] [PubMed]
- Higgs, J.A.; Quinn, A.P.; Seely, K.D.; Richards, Z.; Mortensen, S.P.; Crandall, C.S.; Brooks, A.E. Pathophysiological Link between Insulin Resistance and Adrenal Incidentalomas. Int. J. Mol. Sci. 2022, 23, 4340. [Google Scholar] [CrossRef] [PubMed]
- Sydney, G.I.; Ioakim, K.J.; Paschou, S.A. Insulin resistance and adrenal incidentalomas: A bidirectional relationship. Maturitas 2019, 121, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Manea, M.M.; Dragos, D.; Ghenu, M.I.; Enache, I.I.; Stoican, I.C.; Ciulavu, C.; Vasiliu, O.; Sirbu, C.A.; Tuta, S. The Neurocardiogenic Impact of Ischemic Stroke: Intricacies of Cardiac Enzymes and the Vegetative System. Rom. J. Mil. Med. 2025, CXXVIII, 36–42. [Google Scholar] [CrossRef]
- Marina, L.V.; Ivović, M.; Tančić-Gajić, M.; Arizanović, Z.; Raković, D.; Milin-Lazović, J.; Kendereški, A.; Micić, D.; Vujović, S. Luteinizing hormone and insulin resistance in menopausal patients with adrenal incidentalomas: The cause-effect relationship? Clin. Endocrinol. 2018, 88, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Lazúrová, I.; Jochmanová, I.; Sotak, Š.; Špaková, I.; Mareková, M. Is there a role for the IGF system and epidermal growth factor (EGF) in the pathogenesis of adrenocortical adenomas? A preliminary case-control study. Physiol. Res. 2020, 69, 1085–1094. [Google Scholar] [CrossRef] [PubMed]
- Abdellatif, A.B.; Fernandes-Rosa, F.L.; Boulkroun, S.; Zennaro, M.C. Vascular and hormonal interactions in the adrenal gland. Front. Endocrinol. 2022, 13, 995228. [Google Scholar] [CrossRef] [PubMed]
- Vega-Beyhart, A.; Iruarrizaga, M.; Pané, A.; García-Eguren, G.; Giró, O.; Boswell, L.; Aranda, G.; Flores, V.; Casals, G.; Alonso, C.; et al. Endogenous cortisol excess confers a unique lipid signature and metabolic network. J. Mol. Med. 2021, 99, 1085–1099. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.T.; Ramesh, T.; Toh, X.R.; Nguyen, L.N. Emerging roles of lysophospholipids in health and disease. Prog. Lipid Res. 2020, 80, 101068. [Google Scholar] [CrossRef] [PubMed]
- Morze, J.; Wittenbecher, C.; Schwingshackl, L.; Danielewicz, A.; Rynkiewicz, A.; Hu, F.B.; Guasch-Ferré, M. Metabolomics and Type 2 Diabetes Risk: An Updated Systematic Review and Meta-analysis of Prospective Cohort Studies. Diabetes Care 2022, 45, 1013–1024. [Google Scholar] [CrossRef] [PubMed]
- Green, C.D.; Maceyka, M.; Cowart, L.A.; Spiegel, S. Sphingolipids in metabolic disease: The good, the bad, and the unknown. Cell Metab. 2021, 33, 1293–1306. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.; Hatch, G.M.; Wang, Y.; Yu, F.; Wang, M. The relationship between phospholipids and insulin resistance: From clinical to experimental studies. J. Cell. Mol. Med. 2019, 23, 702–710. [Google Scholar] [CrossRef] [PubMed]
- Hasenmajer, V.; Sbardella, E.; Sciarra, F.; Minnetti, M.; Isidori, A.M.; Venneri, M.A. The Immune System in Cushing’s Syndrome. Trends Endocrinol. Metab. 2020, 31, 655–669. [Google Scholar] [CrossRef] [PubMed]
- Ueland, G.Å.; Methlie, P.; Heie, A.; Meling Stokland, A.E.; Dahle, A.L.; Sævik, Å.B.; Løvås, K.; Husebye, E.S. Substantial changes in inflammatory and cardiovascular biomarkers in patients with autonomous cortisol secretion. Eur. J. Endocrinol. 2023, 189, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Favero, V.; Prete, A.; Mangone, A.; Elhassan, Y.S.; Pucino, V.; Asia, M.; Hardy, R.; Chiodini, I.; Ronchi, C.L. Inflammation-based scores in benign adrenocortical tumours are linked to the degree of cortisol excess: A retrospective single-centre study. Eur. J. Endocrinol. 2023, 189, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Araujo-Castro, M.; Paja Fano, M.; Pla Peris, B.; González Boillos, M.; Pascual-Corrales, E.; García-Cano, A.M.; Parra Ramírez, P.; Rojas-Marcos, P.M.; Ruiz-Sanchez, J.G.; Vicente, A.; et al. Autonomous cortisol secretion in patients with primary aldosteronism: Prevalence and implications on cardiometabolic profile and on surgical outcomes. Endocr. Connect. 2023, 12, e230043. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Horikoshi, H.; Omura, M.; Tsurutani, Y.; Saito, J.; Nishikawa, T. Association Between Aldosterone and Hypertension Among Patients With Overt and Subclinical Hypercortisolism. J. Endocr. Soc. 2022, 7, bvac167. [Google Scholar] [CrossRef] [PubMed]
- Hung, K.; Lee, B.C.; Chen, P.T.; Liu, K.L.; Chang, C.C.; Wu, V.C.; Lin, Y.H. Influence of autonomous cortisol secretion in patients with primary aldosteronism: Subtype analysis and postoperative outcome. Endocr. Connect. 2023, 12, e230121. [Google Scholar] [CrossRef] [PubMed]
- Caetano, C.M.; Malchoff, C.D. Daily Glucocorticoid Replacement Dose in Adrenal Insufficiency, a Mini Review. Front. Endocrinol. 2022, 13, 897211. [Google Scholar] [CrossRef] [PubMed]
- Nowotny, H.; Ahmed, S.F.; Bensing, S.; Beun, J.G.; Brösamle, M.; Chifu, I.; Claahsen van der Grinten, H.; Clemente, M.; Falhammar, H.; Hahner, S.; et al. Therapy options for adrenal insufficiency and recommendations for the management of adrenal crisis. Endocrine 2021, 71, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, M.; Imamura, Y.; Kawamura, K.; Yamamoto, S.; Sazuka, T.; Nakamura, K.; Sakamoto, S.; Nagano, H.; Koide, H.; Tanaka, T.; et al. Contralateral adrenal width predicts the duration of prolonged post-surgical steroid replacement for subclinical Cushing syndrome. Int. J. Urol. 2018, 25, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.; Lin, J.; Hu, X.; Liu, Y.; Zhang, J.; Zhang, L.; Jiang, J.; Li, X.; Guo, J. Preoperative prognostic nomogram for prophylactic steroid treatment of patients with subclinical Cushing’s syndrome. Transl. Androl. Urol. 2021, 10, 426–437. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.S.; Auchus, R.J. Evaluation and Treatment of Patients with Hypercortisolism: A Review. JAMA Surg. 2020, 155, 1152–1159. [Google Scholar] [CrossRef] [PubMed]
- Ueland, G.Å.; Methlie, P.; Jøssang, D.E.; Sagen, J.V.; Viste, K.; Thordarson, H.B.; Heie, A.; Grytaas, M.; Løvås, K.; Biermann, M.; et al. Adrenal Venous Sampling for Assessment of Autonomous Cortisol Secretion. J. Clin. Endocrinol. Metab. 2018, 103, 4553–4560. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.C.; Thompson, S.M.; Adamo, D.; Fleming, C.J.; Bancos, I.; McKenzie, T.J.; Cheville, J.; Young, W.F.; Andrews, J.C. Adrenal venous sampling for lateralization of cortisol hypersecretion in patients with bilateral adrenal masses. Clin. Endocrinol. 2023, 98, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, L.B.; Mackinney, E.; Wang, T.S. When to Intervene for Subclinical Cushing’s Syndrome. Surg. Clin. N. Am. 2019, 99, 747–758. [Google Scholar] [CrossRef] [PubMed]
- van Helden, E.V.; van Uitert, A.; Albers, K.I.; Steegers, M.A.H.; Timmers, H.J.L.M.; d’Ancona, F.C.H.; van der Wal, S.E.I.; Scheffer, G.J.; Keijzer, C.; Warlé, M.C.; et al. Chronic postsurgical pain after minimally invasive adrenalectomy: Prevalence and impact on quality of life. BMC Anesthesiol. 2022, 22, 153. [Google Scholar] [CrossRef] [PubMed]
- Zubair, A.B.; Arif, M.H.; Razzaq, M.T.; Zaman, M.; Haider, Z.; Fajar, I.E.; Saleem, S.; Khalil, A.; Sabir, M.; Kaneez, M. The Spectrum of Postoperative Complications and Outcomes After Open Adrenalectomy: An Experience from a Developing Country. Cureus 2022, 14, e31357. [Google Scholar] [CrossRef] [PubMed]
- Fouche, D.; Chenais, G.; Haissaguerre, M.; Bouriez, D.; Gronnier, C.; Collet, D.; Tabarin, A.; Najah, H. Risk factors for intraoperative complications, postoperative complications, and prolonged length of stay after laparoscopic adrenalectomy by transperitoneal lateral approach: A retrospective cohort study of 547 procedures. Surg. Endosc. 2023, 37, 7573–7581. [Google Scholar] [CrossRef] [PubMed]
- Mihai, I.; Boicean, A.; Teodoru, C.A.; Grigore, N.; Iancu, G.M.; Dura, H.; Bratu, D.G.; Roman, M.D.; Mohor, C.I.; Todor, S.B.; et al. Laparoscopic Adrenalectomy: Tailoring Approaches for the Optimal Resection of Adrenal Tumors. Diagnostics 2023, 13, 3351. [Google Scholar] [CrossRef] [PubMed]
- Pirzada, F.M.; Kumar, R. Minimally invasive adrenalectomy for adrenocortical cancers: A systematic review. Indian J. Urol. 2025, 41, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Mihai, I.; Dura, H.; Teodoru, C.A.; Todor, S.B.; Ichim, C.; Grigore, N.; Mohor, C.I.; Mihetiu, A.; Oprinca, G.; Bacalbasa, N.; et al. Intraoperative Ultrasound: Bridging the Gap between Laparoscopy and Surgical Precision during 3D Laparoscopic Partial Nephrectomies. Diagnostics 2024, 14, 942. [Google Scholar] [CrossRef] [PubMed]
- Sholklapper, T.; Omil-Lima, D.; Kutikov, A. Adrenal Surgery: Open, Laparoscopic, and Robotic Approaches. Urol. Clin. N. Am. 2025, 52, 261–273. [Google Scholar] [CrossRef] [PubMed]
- Esposito, G.; Mullineris, B.; Colli, G.; Curia, S.; Piccoli, M. Robotic Versus Laparoscopic Adrenalectomy for Adrenal Tumors: An Up-to-Date Meta-Analysis on Perioperative Outcomes. Cancers 2025, 17, 150. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Pei, Y.; Zhi, Y.; Sun, F.; Song, N. Comparative study of single-port single-channel and single-port multi-channel adrenalectomy in various maximum tumor diameters. BMC Surg. 2025, 25, 6. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, B.; Karunakaran, D.; Touma, N.J. Perioperative outcomes of adrenal surgery Does surgical specialty matter? Can. Urol. Assoc. J. 2025, 19, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Feciche, B.O.; Barbos, V.; Big, A.; Porav-Hodade, D.; Cumpanas, A.A.; Latcu, S.C.; Zara, F.; Barb, A.C.; Dumitru, C.S.; Cut, T.G.; et al. Posterior Retroperitoneal Laparoscopic Adrenalectomy: An Anatomical Essay and Surgical Update. Cancers 2024, 16, 3841. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.H.; Wong, C. Time to Flip the Approach: Retroperitoneoscopic Adrenalectomy. J. Surg. Res. 2024, 296, 189–195. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| First Author Year of Publication Reference | Study Design | Number of Patients (Study Population) Sex Ratio (F/M) Age (Years) |
|---|---|---|
| 2020 [31] | Cross-sectional, prospective study | N = 213 patients with adrenal adenomas; F/M = 143/7; age [mean (ranges)] = 58 (18–93) y N1 = 22 patients with CS; F/M = 18/4; age [mean (ranges)] = 41.5 (18–61) y N2 = 92 patients with MACS; F/M = 57/35; age [mean (ranges)] = 41.5 (18–61) y N3 = 99 patients with NFA; F/M = 67/32; age [mean (ranges)] = 59 (28–93) y Post-adrenalectomy N1′ = 2 patients with CS N2′ = 6 patients with MACS N3′ = 8 patients with NFA |
| 2020 [32] | Cohort study | N = 60 patients with AI who underwent adrenalectomy (31 patients for adenoma size > 4 cm, 29 patients for presence of hypercortisolism) N1 = 39 patients with postsurgical hypocortisolism; F/M = 31/8; age [mean ± SD (ranges)] = 55.3 ± 12.0 (24–74) y N2 = 21 patients without postsurgical hypocortisolism; F/M = 15/6; age [mean ± SD (ranges)] = 57.2 ± 8.3 (33–75) y |
| 2021 [33] | Retrospective study | N = 121 patients who underwent adrenalectomy N1 = 68 patients with 1 mg DST cortisol 1.8–5 µg/dL; of these 56 had indeterminate nodule which included MACS F/M = 43/25; age (mean ± SD) = 58.5 ± 11.3 y N2 = 53 patients with 1 mg DST cortisol > 5 µg/dL; of these 30 had indeterminate nodule which includes MACS F/M = 43/10; age (mean ± SD) = 52.4 ± 15.8 y |
| 2021 [34] | Cohort study | N = 271 with adrenal adenomas undergoing adrenalectomy N1 = 127 patients with CS; F/M = 104/23; age (mean ± SD) = 56.9 ±12.6 y N2 = 45 patients with ACS *; F/M = 31/14; age (mean ± SD) = 65.0 ± 10.4 y N3 = 99 with NFA;F/M = 59/40; age (mean ± SD) = 60.5 ± 12.1y |
| 2021 [35] | Retrospective study | N = 35 patients with bilateral adenoma with subclinical hypercortisolemia N1 = 27 patients with unilateral adrenalectomy, of these 21 had PACS * and 6 ACS *; F/M = 22/5; age [mean (range)] = 57 (34–75) y N2 = 8 patients with conservative management, of these 7 had PACS * and 1 ACS *; F/M = 4/4; age [mean (range)] = 65 (46–75) y |
| 2022 [36] | Prospective cohort | N = 108 patients who underwent adrenalectomy N1 = 47 patients with MACS; F/M = 38/9; age [mean (range)] = 59 (54–66) y N2 = 27 patients with CS; F/M = 26/1; age [mean (range)] = 55 (45–60) y N3 = 22 patients with PA; F/M = 6/16; age [mean (range)] = 51 (38–55) y N4 = 12 with both PA/CS *; F/M = 4/8; age [mean (range)] = 58 (44–65) y |
| 2022 [37] | Retrospective study | N = 745 patients with adrenal adenomas N1 = 486 patients with NFA; F/M = 273/213; age (mean ± SD) = 62.6 ± 10.72 y N2 = 259 patients (47 with confirmed ACS * and 212 with PACS *); F/M = 151/108; age (mean ± SD) = 64.7 ± 10.50 y N1′ = 16 patients with adrenalectomy N1″ = 470 patients with conservative management N2′ = 42 patients with adrenalectomy N2″ = 217 patients with conservative management |
| 2022 [38] | Cohort study | N = 55 AI patients with PACS 6-month follow-up: N1 = 25 patients with adrenalectomy; F/M =17/8; age [mean (range)] = 63.2 ± 10.3 (41–76) y N2 = 30 patients with conservative management; F/M = 22/8; age [mean (range)] = 66.5 ± 9.1 (42–76) y |
| 2023 [39] | Cohort study | N = 260 patients adrenal adenomas; F/M = 147/113; age [mean (range)] = 59.5 (20–82) y N1 = 123 patients with NFA; F/M = 69/54; age (mean ± SD) = 57 ± 62 y N2 = 96 patients with PACS *; F/M = 53/43; age (mean ± SD) = 63 ± 48 y N3 = 41 patients with ACS *; F/M = 25/16; age (mean ± SD) = 56 ± 51 y Post-adrenalectomy: N’ = 61 patients N1′ = 22 patients with NFA N2′ = 23 patients with PACS * N3′ = 16 patients with ACS * Conservative management: N″ = 199 patients N1″ = 101 patients with NFA N2″ = 73 patients with PACS * N3″ = 25 patients with ACS * |
| 2023 [40] | Retrospective cohort study | N = 32 patients with AI undergoing unilateral adrenalectomy; F/M = 19/13; age [mean (range)] = 61 (51–66) y N1 = 7 patients with NFA; F/M = 5/2; age [mean (range)] = 66 (64–67) y N2 = 25 patients with MACS; F/M =14/11; age [mean (range)] = 58 (49–66) y |
| 2024 [41] | Cohort study | N = 309 patients with NFA; F/M = 138/171; age (mean ± SD) = 54.9 ± 10.1 y N1 = 123 patients with adrenalectomy; F/M = 54/69; age (mean ± SD) = 54.2 ± 10.5 y N2 = 186 patients with conservative management; F/M = 84/102; age (mean ± SD) = 55.3 ± 9.8 y |
| 2024 [42] | Cohort study | N = 207 patients who underwent adrenalectomy; F/M = 126/81; age [mean (range)] = 54.7 (45.9 –63.2) y N1 = 42 patients with CS; F/M = 39/3; age [mean (range)] = 52.0 (44.5–58.8) y N2 = 70 patients with MACS; F/M = 57/13; age [mean (range)] = 59.4 (51.9–68.2) y N3 = 22 patients with mixed PA/hypercortisolism *; F/M = 8/14; age [mean (range)] = 63.6 (53.7–65.9) y N4 = 73 patients with PA; F/M = 22/51; age [mean (range)] = 50.9 (40.3–57.9) y |
| 2024 [43] | Prospective, multicenter study randomized | N = 92 patients with MACS N1 = 46 patients with adrenalectomy; F/M = 29/17; age (mean ± SD) = 53.6 ± 8.1 y N2 = 46 patients with conservative management; F/M = 29/17; age (mean ± SD) = 54.0 ± 7.4 y |
| 2024 [44] | Prospective study | N = 115 patients with AI N1 = 59 patients with NFA; F/M = 31/28; age (mean ± SD) = 45.9 ± 10.4 y N2 = 36 patients with MACS; F/M = 25/11; age (mean ± SD) = 48.0 ± 8.5 y N3 = 20 patients with CS; F/M = 18/2; age (mean ± SD) = 41.9 ± 12.1 y N2′ = 11 patients with adrenalectomy N2″ = 6 conservative management |
| Reference | Criteria for MACS/NFA Diagnosis |
|---|---|
| [31] | MACS: 1 mg DST cortisol > 1.8 µg/dL |
| [32] | Presence of hypercortisolism ≥ 3 out of: 1 mg DST cortisol > 3 µg/dL UFC > 60 mg/24 h ACTH < 10 pg/mL MSC > 5.4 mg/dL Postsurgical hypocortisolism (PSH) diagnosis and rule-out involve cut-offs of 16 µg/dL and 22 µg/dL. |
| [33] | MACS: 1 mg DST cortisol > 1.8 µg/dL |
| [34] | NFA: 1 mg DST cortisol ≤ 1.8 µg/dL ACS: 1 mg DST cortisol > 5 µg/dL, without clinical signs of CS |
| [35] | ACS: 1 mg DST cortisol > 5 µg/dL PACS: 1 mg DST cortisol: 1.9–5 µg/dL |
| [36] | MACS: 1 mg DST cortisol > 1.8 µg/dL CS: 1 mg DST cortisol ≥ 5 µg/dL PA: elevated plasma aldosterone, suppressed plasma renin activity, and aldosterone/renin ratio > 20, confirmatory testing with oral sodium loading or saline infusion test Abnormal POD1-CST: cortisol ≤ 14 (≤18 prior to April 2017). |
| [37] | NFA: 1 mg DST cortisol < 1.8 µg/dL PACS: 1 mg DST cortisol 1.9–5 µg/dL ACS: 1 mg DST cortisol > 5 µg/dL |
| [38] | PACS: 1 mg DST cortisol 1.9–5 µg/dL |
| [39] | NFA: 1 mg DST ≤ 1.8 µg/dL PACS: 1 mg DST 1.9–5 µg/dL ACS: 1 mg DST > 5 µg/dL |
| [40] | NFA: 1 mg DST cortisol ≤ 1.8 µg/dL MACS: 1 mg DST cortisol ≥ 1.8 µg/dL |
| [41] | NFA: 1 mg DST cortisol ≤ 1.8 µg/dL |
| [42] | CS: 1 mg DST > 5 µg/dL MACS:1 mg DST cortisol 1.8–4.9 μg/dL PA: increased plasma aldosterone levels, decreased plasma renin activity aldosterone/renin ratio > 20 Secondary adrenal insufficiency: POD1 basal cortisol level of ≤5 μg/dL, or a cortisol level of ≤14 μg/dL 60 min after CST Abnormal CST based on POD1 basal cortisol levels at thresholds between 5 and 15 μg/dL |
| [43] | MACS: 1 mg DST cortisol > 1.8 µg/dL |
| [44] | NFA: 1 mg DST ≤ 1.8 µg/dL MACS: 1 mg DST > 1.8 µg/dL CS: LDDST serum cortisol ≥ 1.8 µg/dL, elevated MSC and 24 h UFC, suppressed morning plasma ACTH |
| Reference | Analyzed Outcomes |
|---|---|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [40] |
|
| [41] |
|
| [43] |
|
| [44] |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trandafir, A.-I.; Carsote, M.; Florescu, A.-F. An Analysis of Post-Adrenalectomy Dynamics in MACS (Mild Autonomous Cortisol Secretion)-Positive Adrenal Tumours: The Biomarkers and Clinical Impact. J. Clin. Med. 2025, 14, 5217. https://doi.org/10.3390/jcm14155217
Trandafir A-I, Carsote M, Florescu A-F. An Analysis of Post-Adrenalectomy Dynamics in MACS (Mild Autonomous Cortisol Secretion)-Positive Adrenal Tumours: The Biomarkers and Clinical Impact. Journal of Clinical Medicine. 2025; 14(15):5217. https://doi.org/10.3390/jcm14155217
Chicago/Turabian StyleTrandafir, Alexandra-Ioana, Mara Carsote, and Alexandru-Florin Florescu. 2025. "An Analysis of Post-Adrenalectomy Dynamics in MACS (Mild Autonomous Cortisol Secretion)-Positive Adrenal Tumours: The Biomarkers and Clinical Impact" Journal of Clinical Medicine 14, no. 15: 5217. https://doi.org/10.3390/jcm14155217
APA StyleTrandafir, A.-I., Carsote, M., & Florescu, A.-F. (2025). An Analysis of Post-Adrenalectomy Dynamics in MACS (Mild Autonomous Cortisol Secretion)-Positive Adrenal Tumours: The Biomarkers and Clinical Impact. Journal of Clinical Medicine, 14(15), 5217. https://doi.org/10.3390/jcm14155217