
Clinical Application of 3D-Assisted Surgery Techniques in Treatment of Intra-Articular Distal Radius Fractures: A Systematic Review in 718 Patients

 ,
,  , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Search Strategy
2.3. Study Selection
2.4. Quality Check and Best Evidence Synthesis
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
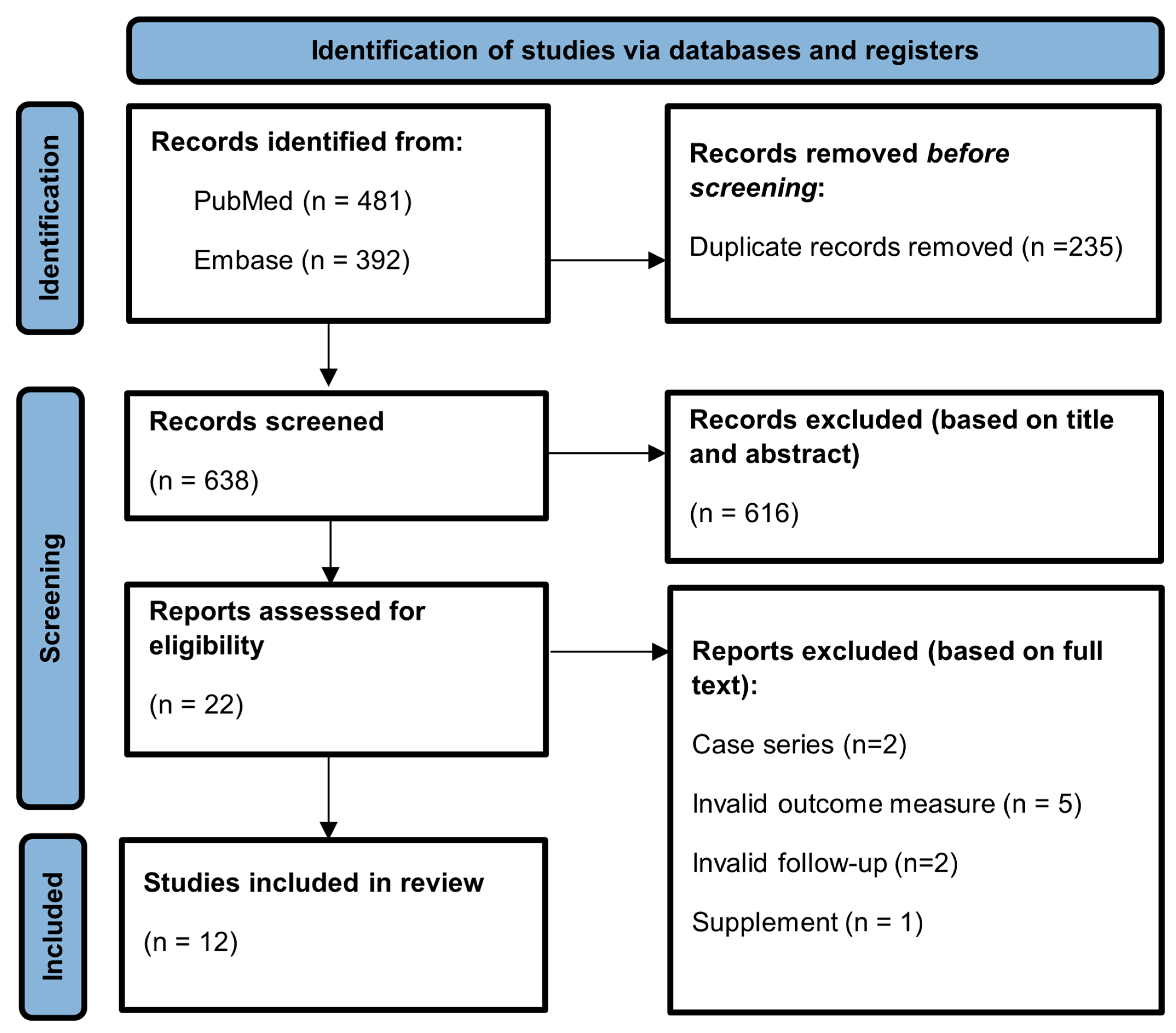
3.1. Search and Study Characteristics
3.2. Methodological Quality Assessment
3.3. Identified 3D Applications in Distal Radius Fracture Surgery
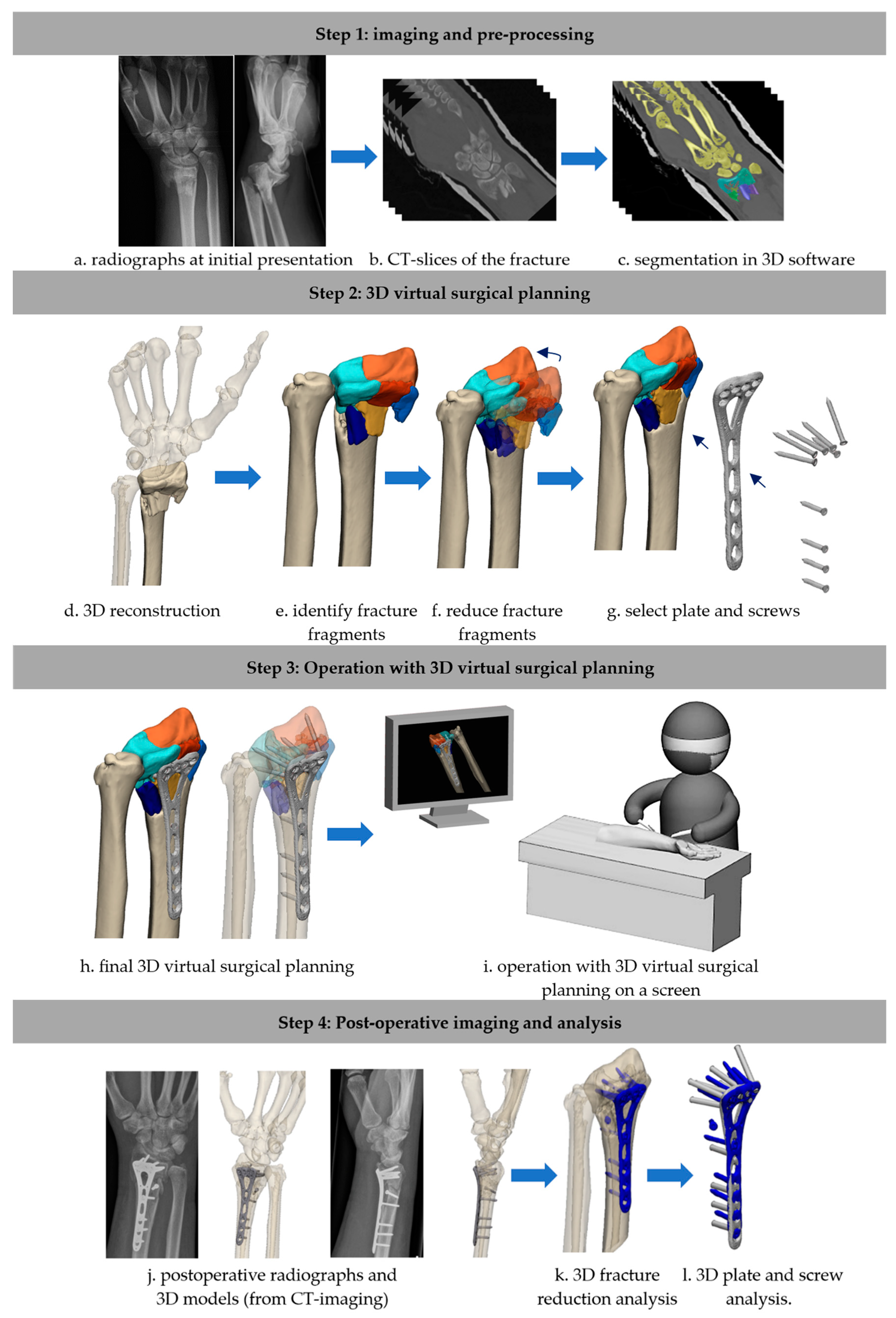
3.3.1. Three-Dimensional Virtual Surgical Planning
3.3.2. Three-Dimensional Printing
3.3.3. Three-Dimensional Intraoperative Guides
3.4. Effect of 3D-Assisted Surgery on Intraoperative Metrics
3.4.1. Operation Time
3.4.2. Fluoroscopy Frequency
3.5. Effect of 3D-Assisted Surgery on Postoperative Outcomes
3.5.1. Patient Follow-Up: PROMs
3.5.2. Patient Follow-Up: Function/Range of Motion
3.5.3. Fracture Reduction
3.5.4. Complication Rate
3.5.5. Accurate Length of Placed Screws
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations
| 2D | Two-dimensional |
| 3D | Three-dimensional |
| CCD | Case–control design |
| COH | Cohort study |
| CSD | Cross-sectional design |
| CT | Computed tomography |
| DASH | Disability of the Arm, Shoulder, and Hand |
| deg. | Degrees |
| Δdeg. | Difference in degrees |
| mm | Millimeters |
| NA | Not addressed/not applicable |
| PRISMA | Preferred Reporting Items for Systematic Reviews |
| PROMs | Patient-reported outcome measures |
| PROSPERO | International prospective register of systematic reviews |
| PRWE | Patient-Rated Wrist Evaluation |
| RCT | Randomized controlled trial |
| ROM | Range of motion |
| SD | Standard deviation |
| VAS | Visual analogue scale |
| VSP | Virtual surgical planning |
References
- Walenkamp, M.; Aydin, S.; Mulders, M.; Goslings, J.; Schep, N. Predictors of unstable distal radius fractures: A systematic review and meta-analysis. J. Hand Surg. (Eur. Vol.) 2016, 41, 501–515. [Google Scholar] [CrossRef]
- Bentohami, A.; De Burlet, K.; De Korte, N.; Van den Bekerom, M.; Goslings, J.; Schep, N. Complications following volar locking plate fixation for distal radial fractures: A systematic review. J. Hand Surg. (Eur. Vol.) 2014, 39, 745–754. [Google Scholar] [CrossRef]
- Prijs, J.; Schoolmeesters, B.; Eygendaal, D.; de Vries, J.P.M.; Jutte, P.C.; Doornberg, J.N.; Jaarsma, R.L.; IJpma, F.F.A. 3D virtual pre-operative planning may reduce the incidence of dorsal screw penetration in volar plating of intra-articular distal radius fractures. Eur. J. Trauma Emerg. Surg. Off. Publ. Eur. Trauma Soc. 2021, 48, 3911–3921. [Google Scholar] [CrossRef] [PubMed]
- Rundgren, J.; Bojan, A.; Mellstrand Navarro, C.; Enocson, A. Epidemiology, classification, treatment and mortality of distal radius fractures in adults: An observational study of 23,394 fractures from the national Swedish fracture register. BMC Musculoskelet. Disord. 2020, 21, 88. [Google Scholar] [CrossRef] [PubMed]
- Fanuele, J.; Koval, K.J.; Lurie, J.; Zhou, W.; Tosteson, A.; Ring, D. Distal radial fracture treatment: What you get may depend on your age and address. JBJS 2009, 91, 1313–1319. [Google Scholar] [CrossRef]
- Rosenauer, R.; Pezzei, C.; Quadlbauer, S.; Keuchel, T.; Jurkowitsch, J.; Hausner, T.; Leixnering, M. Complications after operatively treated distal radius fractures. Arch. Orthop. Trauma Surg. 2020, 140, 665–673. [Google Scholar] [CrossRef]
- Yamamoto, M.; Fujihara, Y.; Fujihara, N.; Hirata, H. A systematic review of volar locking plate removal after distal radius fracture. Injury 2017, 48, 2650–2656. [Google Scholar] [CrossRef] [PubMed]
- Tack, P.; Victor, J.; Gemmel, P.; Annemans, L. 3D-printing techniques in a medical setting: A systematic literature review. Biomed. Eng. Online 2016, 15, 115. [Google Scholar] [CrossRef] [PubMed]
- Meesters, A.M.; Assink, N.; Ten Duis, K.; Fennema, E.M.; Kraeima, J.; Witjes, M.J.; de Vries, J.-P.P.M.; Stirler, V.M.A.; IJpma, F.F.A. Accuracy of patient-specific drilling guides in acetabular fracture surgery: A human cadaver study. J. Pers. Med. 2021, 11, 763. [Google Scholar] [CrossRef] [PubMed]
- Meesters, A.; Kraeima, J.; Banierink, H.; Slump, C.; De Vries, J.; Ten Duis, K.; Witjes, M.J.H.; Ijpma, F.F.A. Introduction of a three-dimensional computed tomography measurement method for acetabular fractures. PLoS ONE 2019, 14, e0218612. [Google Scholar] [CrossRef]
- Banierink, H.; Meesters, A.M.; Ten Duis, K.; Doornberg, J.N.; El Moumni, M.; Heineman, E.; Reininga, I.H.F.; IJpma, F.F.A. Does 3D-Assisted Operative Treatment of Pelvic Ring Injuries Improve Patient Outcome?—A Systematic Review of the Literature. J. Pers. Med. 2021, 11, 930. [Google Scholar] [CrossRef] [PubMed]
- Assink, N.; Kraeima, J.; Slump, C.H.; ten Duis, K.; de Vries, J.P.P.M.; Meesters, A.M.L.; van Ooijen, P.; Witjes, M.J.H.; Ijpma, F.F.A. Quantitative 3D measurements of tibial plateau fractures. Sci. Rep. 2019, 9, 14395. [Google Scholar] [CrossRef]
- Neijhoft, J.; Sterz, J.; Rüsseler, M.; Britz, V.; Bepler, L.; Freund, V.; Janko, M. Evaluation of a 3D-printed hands-on radius fracture model during teaching courses. Eur. J. Trauma Emerg. Surg. 2024, 50, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Zhang, G.; He, Z.; Zhong, S.; Chen, Y.; Wei, C.; Zheng, Y.; Lin, H.; Li, W.; Huang, W. Anatomical reduction and precise internal fixation of intra-articular fractures of the distal radius with virtual X-ray and 3D printing. Australas. Phys. Eng. Sci. Med. 2019, 43, 35–47. [Google Scholar] [CrossRef] [PubMed]
- Zhu, D.; Zhang, Z.; Zhang, J.; Chen, D.; Shan, Y.; Xie, B.; Liu, P.; Yan, L. The efficacy of 3D printing-assisted surgery in treating distal radius fractures: Systematic review and meta-analysis. J. Comp. Eff. Res. 2020, 9, 919–931. [Google Scholar] [CrossRef]
- Souer, J.S.; Wiggers, J.; Ring, D. Quantitative 3-dimensional computed tomography measurement of volar shearing fractures of the distal radius. J. Hand Surg. Am. 2011, 36, 599–603. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhang, Y.; Fan, J.; Yuan, F.; Tang, Q.; Xian, C.J. Analyses of fracture line distribution in intra-articular distal radius fractures. La Radiol. Medica 2019, 124, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zhang, Y.-Q.; Wang, G.-H.; Li, K.; Wang, J.; Ni, M. Melone’s concept revisited in comminuted distal radius fractures: The three-dimensional CT mapping. J. Orthop. Surg. Res. 2020, 15, 222. [Google Scholar] [CrossRef]
- Kong, L.; Zhang, Z.; Lu, J.; Zhang, B.; Zhou, Y.; Tian, D. Clinical Utility of 3-Dimensional Reconstruction Images to Predict Conservative Treatment Outcomes of Intra-Articular Distal Radius Fractures. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e926894. [Google Scholar] [CrossRef] [PubMed]
- Kong, L.; Yang, G.; Yu, J.; Zhou, Y.; Li, S.; Zheng, Q.; Zhang, B. Surgical treatment of intra-articular distal radius fractures with the assistance of three-dimensional printing technique. Medicine 2020, 99, e19259. [Google Scholar] [CrossRef]
- Kaneshiro, Y.; Hidaka, N.; Yano, K.; Kawabata, A.; Fukuda, M.; Sasaoka, R.; Sakanaka, H.; Takamatsu, K. Intraoperative computed tomography with an integrated navigation system versus freehand technique under fluoroscopy in the treatment of intra-articular distal radius fractures. J. Plast. Surg. Hand Surg. 2019, 53, 255–259. [Google Scholar] [CrossRef] [PubMed]
- de Muinck Keizer, R.J.O.; Lechner, K.M.; Mulders, M.A.M.; Schep, N.W.L.; Eygendaal, D.; Goslings, J.C. Three-dimensional virtual planning of corrective osteotomies of distal radius malunions: A systematic review and meta-analysis. Strateg. Trauma Limb Reconstr. 2017, 12, 77–89. [Google Scholar]
- Cao, C.; Zhang, X.J.; Han, T. A longitudinal study of high-resolution diffusion tensor tractography in rats of middle cerebral artery occlusion. Chin. J. Contemp. Neurol. Neurosurg. 2018, 18, 47–54. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Stewart, D.; Letts, L.; Pollock, N.; Bosch, J.; Westmorland, M. Guidelines for Critical Review of Qualitative Studies; McMaster University Occupational Therapy Evidence-Based Practice Research Group: Hamilton, ON, Canada, 1998; p. 1. [Google Scholar]
- Van Tulder, M.; Furlan, A.; Bombardier, C.; Bouter, L.; Group EBotCCBR. Updated method guidelines for systematic reviews in the cochrane collaboration back review group. Spine 2003, 28, 1290–1299. [Google Scholar] [CrossRef]
- Hudak, P.L.; Amadio, P.C.; Bombardier, C.; Beaton, D.; Cole, D.; Davis, A.; Hawker, G.; Katz, J.N.; Makela, M.; Marx, R.G.; et al. Development of an upper extremity outcome measure: The DASH (disabilities of the arm, shoulder, and head). Am. J. Ind. Med. 1996, 29, 602–608. [Google Scholar] [CrossRef]
- MacDermid, J.C.; Turgeon, T.; Richards, R.S.; Beadle, M.; Roth, J.H. Patient rating of wrist pain and disability: A reliable and valid measurement tool. J. Orthop. Trauma 1998, 12, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Fricker, R.J.J.; Kastelec, M. AO Surgery Reference: Distal Forearm. 2023. Available online: https://surgeryreference.aofoundation.org/orthopedic-trauma/adult-trauma/distal-forearm (accessed on 14 August 2024).
- Federatie_Medisch_Specialisten. Distale Radiusfracturen: Richtlijnen. 2021. Available online: https://richtlijnendatabase.nl/richtlijn/distale_radiusfracturen/startpagina_-_distale_radiusfracturen.html (accessed on 14 August 2024).
- Chen, C.; Cai, L.; Zhang, C.; Wang, J.; Guo, X.; Zhou, Y. Treatment of Die-Punch Fractures with 3D Printing Technology. J. Investig. Surg. Off. J. Acad. Surg. Res. 2018, 31, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Cai, L.; Zheng, W.; Wang, J.; Guo, X.; Chen, H. The efficacy of using 3D printing models in the treatment of fractures: A randomised clinical trial. BMC Musculoskelet Disord 2019, 20, 65. [Google Scholar] [CrossRef] [PubMed]
- Grinčuk, A.; Petryla, G.; Masionis, P.; Sveikata, T.; Uvarovas, V.; Makulavičius, A. Short-term results and complications of the operative treatment of the distal radius fracture AO2R3 C type, planned by using 3D-printed models. Prospective randomized control study. J. Orthop. Surg. 2023, 31, 10225536231195127. [Google Scholar] [CrossRef] [PubMed]
- Gui, X.Y.; Shi, H.F.; Xiong, J.; Chen, Y.X.; Wang, J.F.; Huang, J.; Qiu, X.; Wang, Y. A modified intrafocal pinning technique with three-dimensional planning to facilitate volar plating in dorsally comminuted AO/OTA C2 and C3 distal radius fractures. BMC Musculoskelet. Disord. 2021, 22, 379. [Google Scholar] [CrossRef]
- Kohyama, S.; Yoshii, Y.; Ikumi, A.; Ogawa, T.; Ishii, T. Is a novel fluoroscopic intraoperative reference system superior to conventional management for distal radius fracture reduction? A propensity-matched comparative study. Clin. Orthop. Relat. Res. 2024, 482, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Totoki, Y.; Yoshii, Y.; Kusakabe, T.; Akita, K.; Ishii, T. Screw Length Optimization of a Volar Locking Plate Using Three Dimensional Preoperative Planning in Distal Radius Fractures. J. Hand Surg. Asian-Pac. Vol. 2018, 23, 520–527. [Google Scholar] [CrossRef]
- Yoshii, Y.; Kusakabe, T.; Akita, K.; Tung, W.L.; Ishii, T. Reproducibility of three dimensional digital preoperative planning for the osteosynthesis of distal radius fractures. J. Orthop. Res. 2017, 35, 2646–2651. [Google Scholar] [CrossRef] [PubMed]
- Yoshii, Y.; Totoki, Y.; Tung, W.L.; Akita, K.; Ishii, T. A Comparison of Radiographic Outcomes between 3D Preoperative Planning and Conventional Planning in the Osteosynthesis of Distal Radius Fractures. J. Hand Surg. Asian-Pac. Vol. 2018, 24, 303–310. [Google Scholar] [CrossRef]
- Yoshii, Y.; Totoki, Y.; Sashida, S.; Sakai, S.; Ishii, T. Utility of an image fusion system for 3D preoperative planning and fluoroscopy in the osteosynthesis of distal radius fractures. J. Orthop. Surg. Res. 2019, 14, 342. [Google Scholar] [CrossRef]
- Yoshii, Y.; Ogawa, T.; Shigi, A.; Oka, K.; Murase, T.; Ishii, T. Three-dimensional evaluations of preoperative planning reproducibility for the osteosynthesis of distal radius fractures. J. Orthop. Surg. Res. 2021, 16, 131. [Google Scholar] [CrossRef] [PubMed]
- Franchignoni, F.; Vercelli, S.; Giordano, A.; Sartorio, F.; Bravini, E.; Ferriero, G. Minimal clinically important difference of the disabilities of the arm, shoulder and hand outcome measure (DASH) and its shortened version (QuickDASH). J. Orthop. Sports Phys. Ther. 2014, 44, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Maccagnano, G.; Noia, G.; Vicenti, G.; Baglioni, M.; Masciale, M.R.; Cassano, G.D.; Vitiello, R.; Moretti, B.; Pesce, V. Volar locking plate versus external fixation in distal radius fractures: A meta-analysis. Orthop. Rev. 2021, 13, 9147. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Database | Search String |
|---|---|
| Pubmed | (3D[tiab] OR three dimension*[tiab] OR 3 dimension*[tiab] OR ‘Printing, Three-Dimensional’ [Mesh] OR ‘Imaging, Three-Dimensional’ [Mesh]) AND (Radius*[tiab] OR ‘Radius’ [Mesh]) AND (fractur*[tiab] OR ‘Fractures, Bone’ [Mesh]) AND ‘2010/01/01’ [PDat]: ‘3000/12/31’ [PDat] |
| Embase | (‘three dimensional imaging’/exp OR ‘three dimensional printing’/exp OR ‘3 d’:ti,ab OR ‘3 dimension*’:ti,ab OR ‘three dimension*’:ti,ab) AND (‘radius’/exp OR radial*:ti,ab) AND (‘fracture’/exp OR fractur*:ti,ab) AND [embase]/lim AND [2010–2024]/py |
| Study | Year | Country | N | Population | Period | 3D Technology * | Outcome Measurements ** |
|---|---|---|---|---|---|---|---|
| Chen et al. [32] | 2018 | China | 107 | Die punch fractures | 2013–2015 | 3D prints | Primary: patient follow-up, fracture reduction Secondary: operation time, N fluoroscopy |
| Chen et al. [33] | 2019 | China | 48 | AO23C | 2014–2015 | 3D prints | Primary: patient follow-up, fracture reduction Secondary: operation time, N fluoroscopy |
| Grinčuk et al. [34] | 2023 | Lithuania | 66 | AO23C | 2021–2022 | 3D prints | Primary: patient follow-up, fracture reduction, complication rate Secondary: Operation time |
| Gui et al. [35] | 2021 | China | 41 | AO23C2 + C3 with dorsal comminution | 2017–2018 | 3D prints | Primary: patient follow-up, fracture reduction, complication rate Secondary: - |
| Kong et al. [20] | 2020 | China | 32 | AO23B + C | 2017–2018 | 3D prints | Primary: patient follow-up, fracture reduction, complication rate Secondary: operation time, N fluoroscopy |
| Kohyama et al. [36] | 2024 | Japan | 171 | AO23A3,B3 + C | 2014–2021 | 3D VSP | Primary: fracture reduction Secondary: - |
| Totoki et al. [37] | 2018 | Japan | 49 | AO23A2-A3 + C | Not reported | 3D VSP | Primary: accuracy of screw placement Secondary: operation time |
| Xu et al. [14] | 2019 | China | 21 | AO23C | 2017–2018 | 3D VSP, 3D prints, 3D guide | Primary: patient follow-up, fracture reduction, complication rate, accuracy of screw placement Secondary: - |
| Yoshii et al. [38] | 2017 | Japan | 20 | AO23A2-A3 + C | Not reported | 3D VSP | Primary: fracture reduction, accuracy of screw placement Secondary: - |
| Yoshii et al. [39] | 2018 | Japan | 60 | AO23A2-A3 + B3 + C | Not reported | 3D VSP | Primary: fracture reduction Secondary: - |
| Yoshii et al. [40] | 2019 | Japan | 42 | AO23A3 + C2-C3 | Not reported | 3D VSP, 3D guide | Primary: fracture reduction, accuracy of screw placement Secondary: - |
| Yoshii et al. [41] | 2021 | Japan | 63 | AO23A3 + C2-C3 | 2015-2019 | 3D VSP | Primary: patient follow-up, fracture reduction Secondary: - |
| Chen 2018 [32] | Chen 2019 [32] | Grinčuk 2023 [34] | Gui 2021 [35] | Kong 2020 [20] | Kohyama 2024 [36] | Totoki 2018 [37] | Xu 2020 [14] | Yoshii 2017 [38] | Yoshii 2019 [40] | Yoshii 2018 [39] | Yoshii 2021 [41] | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Study purpose | ||||||||||||
| Was the study question clearly stated? | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 |
| 2. Literature review | ||||||||||||
| Was relevant background literature reviewed? | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 |
| 3. Study design * | RCT | RCT | RCT | CSD | RCT | CCD | COH. | COH. | COH. | RCT | RCT | CSD |
| 4. Sample | ||||||||||||
| Was the sample described in detail? | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Was the sample justified? | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| Were the groups randomized? | 1 | 1 | 1 | NA | 1 | NA | NA | NA | NA | 1 | 0 | NA |
| Was randomizing appropriately done? | 0 | 0 | 1 | NA | 1 | NA | NA | NA | NA | 0 | 0 | NA |
| 5. Outcomes | ||||||||||||
| Were the outcome measures reliable? | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 |
| Were the outcome measures valid? | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 |
| 6. Intervention | ||||||||||||
| Intervention was described in detail? | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| Contamination was avoided? | 1 | 1 | 0 | NA | 1 | 0 | 1 | NA | NA | 1 | 0 | NA |
| Cointervention was avoided? | 0 | 0 | 1 | NA | 1 | 1 | 1 | NA | NA | 1 | 0 | NA |
| 7. Results | ||||||||||||
| Results were reported in terms of statistical significance? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Were the analysis method/s appropriate? | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 |
| Clinical importance was reported? | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 |
| Drop-outs were reported? | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 |
| 8. Conclusion | ||||||||||||
| Conclusions were appropriate given study methods and results? | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Total n points | 9 | 9 | 9 | 10 | 14 | 9 | 13 | 8 | 9 | 9 | 8 | 8 |
| Maximum points possible | 16 | 16 | 06 | 12 | 16 | 14 | 14 | 12 | 12 | 16 | 16 | 12 |
| Quality score (%) | 56 | 56 | 56 | 83 | 88 | 64 | 93 | 67 | 75 | 56 | 50 | 67 |
| Study quality interpretation ** | M | M | M | G | G | M | E | G | G | M | M | M |
| High Quality study? *** | ✓ | ✓ | ✓ | ✓ | ✓ |
| Operation Time | |||||||
| Measure | Study | 3D Technology | Groups | Outcome ± SD | |||
| 2D (N) | 3D (N) | 2D | 3D | Sig. (p) | |||
| Operation Time (min) | Chen 2018 [32] | 3D printing | 55 | 52 | 65.7 ± 6.0 | 56.6 ± 4.7 | p < 0.001 * |
| Chen 2019 [33] | 3D printing | 25 | 23 | 75.4 ± 6.0 | 66.5 ± 5.3 | p < 0.001 * | |
| Grinčuk 2023 [34] | 3D printing | 33 | 33 | 72.1 ± 17.5 | 65.1 ± 15.2 | p = 0.072 | |
| Kong 2020 ✓ [20] | 3D printing | 16 | 16 | 63.5 ± 5.9 | 51.4 ± 6.8 | p < 0.001 * | |
| Totoki 2018 ✓ [37] | 3D VSP | 19 | 28 | 101.8 ± NA | 95.3 ± NA | p > 0.05 | |
| Sum N patients/Weighted mean (range) | 148 | 154 | 73.2 (63.5–101.8) | 66.9 (51.4–95.3) | |||
| Fluoroscopy Frequency | |||||||
| Measure | Study | 3D Technology | Groups | Outcome ± SD | |||
| 2D (N) | 3D (N) | 2D | 3D | Sig. (p) | |||
| Fluoroscopy frequency (N) | Chen 2018 [32] | 3D printing | 55 | 52 | 5.9 ± 1.6 | 4.9 ± 1.4 | p < 0.001 * |
| Chen 2019 [33] | 3D printing | 25 | 23 | 5.6 ± 1.6 | 4.4 ± 1.4 | p = 0.011 * | |
| Kong 2020 ✓ [20] | 3D printing | 16 | 16 | 5.6 ± 1.1 | 4.2 ± 1.3 | p = 0.002 * | |
| Sum N patients/Weighted mean (range) | 96 | 96 | 5.8 (5.6–5.9) | 4.7 (4.2–4.9) | |||
| Patient Follow-Up: PROMs | ||||||||
| Measure | Study | 3D Technology | Groups | Outcome ± SD | ||||
| 2D (N) | 3D (N) | 2D | 3D | Sig. (p) | ||||
| DASH ± SD | Kong 2020 ✓ [20] | 3D printing | 16 | 16 | 24.5 ± 7.0 | 23.8 ± 8.1 | p = 0.91 | |
| Grinčuk 2023 [34] | 3D printing | 33 | 33 | 23.6 ± 20.2 | 14.9 ± 13.1 | p = 0.094 | ||
| Sum N patients/Weighted mean (range) | 49 | 49 | 23.9 (23.6–24.5) | 17.8 (14.9–23.8) | ||||
| PRWE ± SD | Grinčuk 2023 [34] | 3D printing | 33 | 33 | 19.6 ± 20.8 | 13.8 ± 2.4 | p = 0.342 | |
| Sum N patients/Weighted mean (range) | 33 | 33 | 19.6 | 13.8 | ||||
| VAS ± SD | Kong 2020 ✓ [20] | 3D printing | 16 | 16 | 0.9 ± 0.3 | 0.9 ± 0.2 | p = 0.80 | |
| Grinčuk 2023 [34] | 3D printing | 33 | 33 | 1.0 ± 1.3 | 0.8 ± 0.8 | p = 0.554 | ||
| Sum N patients/Weighted mean (range) | 49 | 49 | 1.0 (0.9–1.0) | 0.8 (0.8–0.9) | ||||
| Patient Follow-Up: Function/ROM: (Difference Between Uninjured and Fractured Side for the 2D and 3D Group) | ||||||||
| Measure | Study | 3D Technology | Groups | Outcome ± SD | ||||
| 2D (N) | 3D (N) | 2D | 3D | Sig. (p) | ||||
| Gartland–Werley score ± SD (pts) | Chen 2018 [32] | 3D printing | 55 | 52 | 86.0 ± 15.2 | 86.4 ± 14.1 | p = 0.878 | |
| Chen 2019 [33] | 3D printing | 25 | 23 | 74.8 ± 16.6 | 75.7 ± 15.5 | p = 0.211 | ||
| Sum N patients/Weighted mean (range) | 80 | 75 | 82.5 (74.8–86.0) | 83.1 (75.7–86.4) | ||||
| Extension ± SD (Δdeg.) | Chen 2018 [32] | 3D printing | 55 | 52 | 4.6 ± 3.7 | 4.6 ± 3.8 | p = 0.993 | |
| Chen 2019 [33] | 3D printing | 25 | 23 | 3.8 ± 3.1 | 4.1 ± 3.5 | p = 0.765 | ||
| Sum N patients/Weighted mean (range) | 80 | 75 | 4.3 (3.8–4.6) | 4.4 (4.1–4.6) | ||||
| Flexion ± SD (Δdeg.) | Chen 2018 [32] | 3D printing | 55 | 52 | 4 ± 3.7 | 3.6 ± 3.2 | p = 0.606 | |
| Chen 2019 [33] | 3D printing | 25 | 23 | 3.6 ± 2.7 | 3.1 ± 2.7 | p = 0.511 | ||
| Grinčuk 2023 [34] | 3D printing | 33 | 33 | 12.1 ± 10.1 | 7.5 ± 5.9 | p = 0.06 | ||
| Sum N patients/Weighted mean (range) | 113 | 108 | 6.6 (3.6–12.1) | 4.7 (3.1–7.5) | ||||
| Pronation ± SD (Δdeg.) | Chen 2018 [32] | 3D printing | 55 | 52 | 5.5 ± 3.9 | 5.5 ± 3.4 | p = 0.906 | |
| Chen 2019 [33] | 3D printing | 25 | 23 | 4.5 ± 3.7 | 5.1 ± 3.2 | p = 0.548 | ||
| Grinčuk 2023 [34] | 3D printing | 33 | 33 | 1.7 ± 5.1 | 1.0 ± 2.9 | p = 0.926 | ||
| Sum N patients/Weighted mean (range) | 113 | 108 | 4.1 (1.7–5.6) | 4.0 (1–5.5) | ||||
| Supination (Δdeg.) | Chen 2018 [32] | 3D printing | 55 | 52 | 5.6 ± 4.3 | 5.3 ± 4.7 | p = 0.671 | |
| Chen 2019 [33] | 3D printing | 25 | 23 | 4.9 ± 3.3 | 4.4 ± 3.3 | p = 0.613 | ||
| Grinčuk 2023 [34] | 3D printing | 33 | 33 | 2.0 ± 5.3 | 1.3 ± 4.5 | p = 0.692 | ||
| Sum N patients/Weighted mean (range) | 113 | 108 | 4.4 (2.0–5.6) | 3.9 (1.3–5.3) | ||||
| Radial deviation ± SD (deg.) | Kong 2020 ✓ [20] | 3D printing | 16 | 16 | 23.2 ± 4.9 | 24.8 ± 5.1 | p = 0.38 | |
| Sum N patients/Weighted mean (range) | 16 | 16 | 23.2 | 24.8 | ||||
| Ulnar deviation ± SD (deg.) | Kong 2020 ✓ [20] | 3D printing | 16 | 16 | 19.8 ± 5.8 | 22.0 ± 6.9 | p = 0.35 | |
| Grinčuk 2023 [34] | 3D printing | 33 | 33 | 13.8 ± 10.4 | 9.5 ± 7.1 | p = 0.12 | ||
| Sum N patients/Weighted mean (range) | 49 | 49 | 15.7 (13.6–19.8) | 13.6 (9.5–22.0) | ||||
| Fracture Reduction (Difference Between Postoperative Fractures Side and Contralateral, or Direct Measurement of Reduced Fracture) | ||||||||
| Measure | Study | 3D Technology | Groups | Outcome ± SD | ||||
| 2D (N) | 3D (N) | 2D | 3D | Sig. (p) | ||||
| Satisfying Intra-articular fracture reduction rate (%) | Kong 2020 ✓ [20] | 3D printing | 16 | 16 | 94 | 94 | p > 0.05 | |
| Sum N patients/Weighted mean (range) | 16 | 16 | 94 | 94 | ||||
| Ulnar deviation (deg.) | Chen 2018 [32] | 3D printing | 55 | 52 | 20.7 ± 1.8 | 20.6 ± 1.8 | p = 0.868 | |
| Chen 2019 [33] | 3D printing | 25 | 23 | 20.4 ± 1.5 | 20.9 ± 1.7 | p = 0.309 | ||
| Sum N patients/Weighted mean (range) | 80 | 75 | 20.6 (20.4–20.8) | 20.7 (20.6–20.9) | ||||
| Ulnar deviation (Δdeg.) | Grinčuk 2023 [34] | 3D printing | 33 | 33 | 1.2 ± 2.3 | 0.3 ± 1.8 | p = 0.254 | |
| Kohyama 2024 [36] | 3D VSP | 108 | 63 | 1.4 ± 1.4 | 1.3 ± 1.0 | p = 0.71 | ||
| Yoshii 2019 [40] | 3D VSP, 3D guide | 21 | 21 | 1.6 ± 1.6 | 1.7 ± 1.1 | NA | ||
| Sum N patients/Weighted mean (range) | 162 | 117 | 1.4 (1.2–1.6) | 1.1 (0.3–1.7) | ||||
| Palmar tilt (deg.) | Chen 2018 [32] | 3D printing | 55 | 52 | 12.7 ± 1.6 | 12.4 ± 1.4 | p = 0.467 | |
| Chen 2019 [33] | 3D printing | 25 | 23 | 12.7 ± 1.9 | 12.2 ± 1.5 | p = 0.359 | ||
| Sum N patients/Weighted mean (range) | 80 | 75 | 12.7 (12.7–12.7) | 12.3 (12.2–12.4) | ||||
| Palmar tilt (Δdeg.) | Yoshii 2019 [40] | 3D VSP, 3D guide | 21 | 21 | 2.5 ± 2.3 | 2.2 ± 1.7 | NA | |
| Yoshii 2018 [39] | 3D VSP | 30 | 30 | 4.0 ± 3.1 | 2.5 ± 1.8 | p = 0.03 * | ||
| Grinčuk 2023 [34] | 3D printing | 33 | 33 | 4.3 ± 8.7 | 3.7 ± 4.9 | p = 0.158 | ||
| Sum N patients/Weighted mean (range) | 84 | 84 | 3.7 (2.5–4.3) | 2.9 (2.2–3.7) | ||||
| Radial height (mm.) | Chen 2018 [32] | 3D printing | 55 | 52 | 12.7 ± 1.6 | 12.4 ± 1.9 | p = 0.410 | |
| Chen 2019 [33] | 3D printing | 25 | 23 | 12.6 ± 1.8 | 12.6 ± 1.9 | p = 0.987 | ||
| Grinčuk 2023 [34] | 3D printing | 33 | 33 | 11.8 ± 2.5 | 10.8 ± 2.7 | p = 0.161 | ||
| Sum N patients/Weighted mean (range) | 113 | 108 | 12.4 (11.7–12.7) | 12.0 (10.8–12.6) | ||||
| Ulnar variance (mm) | Kohyama 2024 [36] | 3D VSP | 108 | 63 | 0.8 ± 0.8 | 0.4 ± 0.6 | p = 0.02 * | |
| Yoshii 2018 [39] | 3D VSP | 30 | 30 | 1.10 ± 0.94 | 0.92 ± 0.76 | p > 0.05 | ||
| Sum N patients/Weighted mean (range) | 138 | 93 | 0.9 (0.8–1.1) | 0.6 (0.4–0.9) | ||||
| Radial inclination (Δdeg.) | Kohyama 2024 [36] | 3D VSP | 108 | 63 | 1.3 ± 1.0 | 1.2 ± 1.2 | p = 0.69 | |
| Yoshii 2018 [39] | 3D VSP | 30 | 30 | 2.00 ± 1.58 | 3.40 ± 3.00 | p = 0.03 * | ||
| Sum N patients/Weighted mean (range) | 138 | 93 | 1.45 (1.3–2.00) | 1.91 (1.2–3.40) | ||||
| Radial inclination (deg.) | Grinčuk 2023 [34] | 3D printing | 33 | 33 | 22.56 ± 7.9 | 24.9 ± 6.2 | p = 0.17 | |
| Sum N patients/Weighted mean (range) | 33 | 33 | 22.5 | 24.9 | ||||
| Complication Rate | ||||||||
| Measure | Study | 3D Technology | Groups | Outcome ± SD | ||||
| 2D (N) | 3D (N) | 2D | 3D | Sig. (p) | ||||
| Complication rate (%) | Kong 2020 ✓ [20] | 3D printing | 16 | 16 | 12 | 7 | NA | |
| Grinčuk 2023 [34] | 3D printing | 33 | 33 | 10 | 2 | p = 0.02 * | ||
| Sum N patients/Weighted mean (range) | 49 | 49 | 10.7 (10–12) | 3.6 (2–7) | ||||
| Accuracy Screw Placement | ||||||||
| Measure | Study | 3D Technology | Groups | Outcome ± SD | ||||
| 2D (N) | 3D (N) | 2D | 3D | Sig. (p) | ||||
| Accurate length of placed screws (%) | Totoki 2018 ✓ [37] | 3D VSP | 21 | 28 | 75 | 86 | p < 0.05 * | |
| Sum N patients/Weighted mean (range) | 21 | 28 | 75 | 86 | - | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roelofs, L.J.M.; Assink, N.; Kraeima, J.; ten Duis, K.; Doornberg, J.N.; de Vries, J.-P.P.M.; Meesters, A.M.L.; IJpma, F.F.A. Clinical Application of 3D-Assisted Surgery Techniques in Treatment of Intra-Articular Distal Radius Fractures: A Systematic Review in 718 Patients. J. Clin. Med. 2024, 13, 7296. https://doi.org/10.3390/jcm13237296
Roelofs LJM, Assink N, Kraeima J, ten Duis K, Doornberg JN, de Vries J-PPM, Meesters AML, IJpma FFA. Clinical Application of 3D-Assisted Surgery Techniques in Treatment of Intra-Articular Distal Radius Fractures: A Systematic Review in 718 Patients. Journal of Clinical Medicine. 2024; 13(23):7296. https://doi.org/10.3390/jcm13237296
Chicago/Turabian StyleRoelofs, Lisanne J. M., Nick Assink, Joep Kraeima, Kaj ten Duis, Job N. Doornberg, Jean-Paul P. M. de Vries, Anne M. L. Meesters, and Frank F. A. IJpma. 2024. "Clinical Application of 3D-Assisted Surgery Techniques in Treatment of Intra-Articular Distal Radius Fractures: A Systematic Review in 718 Patients" Journal of Clinical Medicine 13, no. 23: 7296. https://doi.org/10.3390/jcm13237296
APA StyleRoelofs, L. J. M., Assink, N., Kraeima, J., ten Duis, K., Doornberg, J. N., de Vries, J.-P. P. M., Meesters, A. M. L., & IJpma, F. F. A. (2024). Clinical Application of 3D-Assisted Surgery Techniques in Treatment of Intra-Articular Distal Radius Fractures: A Systematic Review in 718 Patients. Journal of Clinical Medicine, 13(23), 7296. https://doi.org/10.3390/jcm13237296