
Tinnitus and Its Relation to Depression, Anxiety, and Stress—A Population-Based Cohort Study
 ,
,
Abstract
1. Introduction
2. Materials and Methods
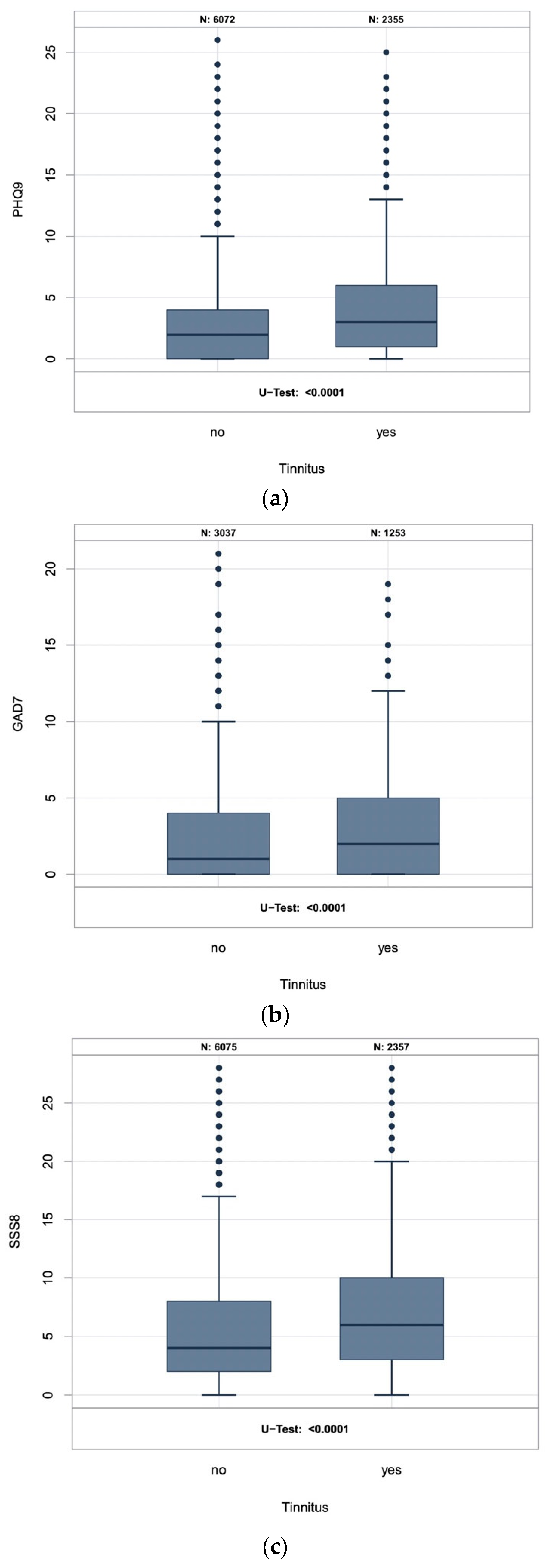
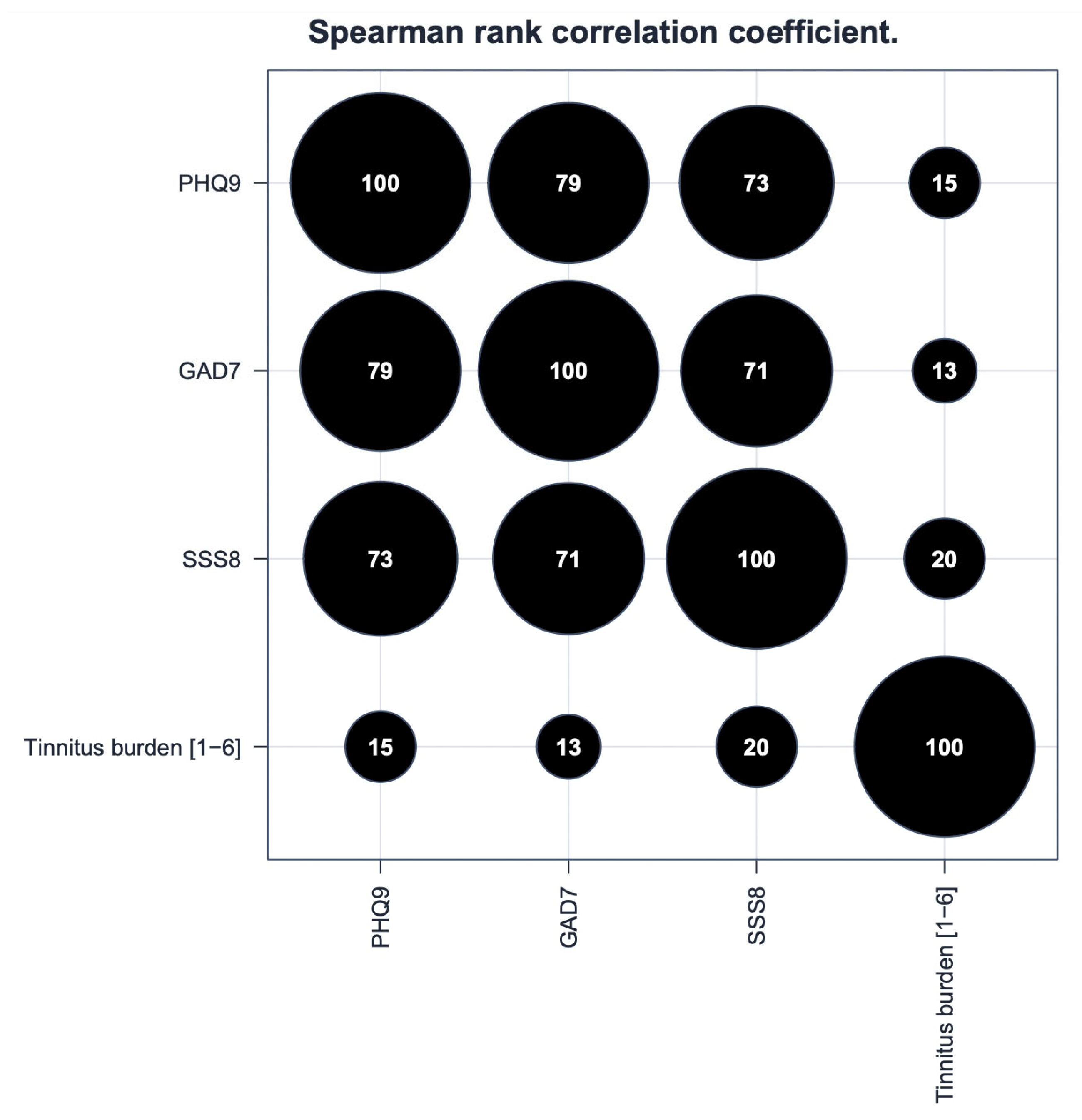
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baguley, D.; McFerran, D.; Hall, D. Tinnitus. Lancet 2013, 382, 1600–1607. [Google Scholar] [CrossRef]
- McCormack, A.; Edmondson-Jones, M.; Somerset, S.; Hall, D. A systematic review of the reporting of tinnitus prevalence and severity. Hear. Res. 2016, 337, 70–79. [Google Scholar] [CrossRef]
- Biswas, R.; Lugo, A.; Akeroyd, M.A.; Schlee, W.; Gallus, S.; Hall, D.A. Tinnitus prevalence in Europe: A multi-country cross-sectional population study. Lancet Reg. Health-Eur. 2022, 12, 100250. [Google Scholar] [CrossRef]
- Heller, A.J. Classification and epidemiology of tinnitus. Otolaryngol. Clin. N. Am. 2003, 36, 239–248. [Google Scholar] [CrossRef]
- Stobik, C.; Weber, R.K.; Münte, T.F.; Walter, M.; Frommer, J. Evidence of psychosomatic influences in compensated and decompensated tinnitus. Int. J. Audiol. 2005, 44, 370–378. [Google Scholar] [CrossRef]
- Hiller, W.; Goebel, G. Komorbidität psychiatrischer Störungen beim chronischen Tinnitus. In Ohrgeräusche. Psychosomatische Aspekte des chronischen Tinnitus; Goebel, G., Ed.; Urban & Vogel: München, Germany, 2001; pp. 47–68. [Google Scholar]
- Geocze, L.; Mucci, S.; Abranches, D.C.; Marco, M.A.; Penido Nde, O. Systematic review on the evidences of an association between tinnitus and depression. Braz. J. Otorhinolaryngol. 2013, 79, 106–111. [Google Scholar] [CrossRef]
- Hiller, W.; Janca, A.; Burke, K.C. Association between tinnitus and somatoform disorders. J. Psychosom. Res. 1997, 43, 613–624. [Google Scholar] [CrossRef]
- Heidemann, C.; Scheidt-Nave, C.; Beyer, A.-K.; Baumert, J.; Thamm, R.; Maier, B.; Neuhauser, H.; Fuchs, J.; Kuhnert, R.; Hapke, U. Gesundheitliche Lage von Erwachsenen in Deutschland—Ergebnisse zu ausgewählten Indikatoren der Studie GEDA 2019/2020-EHIS. J. Health Monit. 2021, 6, 9. [Google Scholar] [CrossRef]
- Jacobi, F.; Höfler, M.; Siegert, J.; Mack, S.; Gerschler, A.; Scholl, L.; Busch, M.A.; Hapke, U.; Maske, U.; Seiffert, I.; et al. Twelve-month prevalence, comorbidity and correlates of mental disorders in Germany: The Mental Health Module of the German Health Interview and Examination Survey for Adults (DEGS1-MH). Int. J. Methods Psychiatr. Res. 2014, 23, 304–319. [Google Scholar] [CrossRef]
- Rouche, A.; Erhart, M.; von Stillfried, D.G. Epidemiologie somatoformer Störungen in der vertragsärztlichen Versorgung—Deutschland 2011. In Proceedings of the DGPPN Kongress 2014 Deutsche Gesellschaft für Psychiatrie und Psychotherapie, Psychosomatik und Nervenheilkunde, Berlin, Germany, 26–29 November 2014. [Google Scholar]
- Langguth, B.; Landgrebe, M.; Kleinjung, T.; Sand, G.P.; Hajak, G. Tinnitus and depression. World J. Biol. Psychiatry 2011, 12, 489–500. [Google Scholar] [CrossRef]
- Czornik, M.; Malekshahi, A.; Mahmoud, W.; Wolpert, S.; Birbaumer, N. Psychophysiological treatment of chronic tinnitus: A review. Clin. Psychol. Psychother. 2022, 29, 1236–1253. [Google Scholar] [CrossRef]
- Langguth, B.; Kreuzer, P.M.; Kleinjung, T.; De Ridder, D. Tinnitus: Causes and clinical management. Lancet Neurol. 2013, 12, 920–930. [Google Scholar] [CrossRef]
- Noreña, A.J.; Eggermont, J.J. Changes in spontaneous neural activity immediately after an acoustic trauma: Implications for neural correlates of tinnitus. Hear. Res. 2003, 183, 137–153. [Google Scholar] [CrossRef]
- Wallhäusser-Franke, E.; D’Amelio, R.; Glauner, A.; Delb, W.; Servais, J.J.; Hörmann, K.; Repik, I. Transition from Acute to Chronic Tinnitus: Predictors for the Development of Chronic Distressing Tinnitus. Front. Neurol. 2017, 8, 605. [Google Scholar] [CrossRef]
- Biehl, R.; Boecking, B.; Brueggemann, P.; Grosse, R.; Mazurek, B. Personality Traits, Perceived Stress, and Tinnitus-Related Distress in Patients With Chronic Tinnitus: Support for a Vulnerability-Stress Model. Front. Psychol. 2019, 10, 3093. [Google Scholar] [CrossRef]
- Beutel, M.E.; Tibubos, A.N.; Michal, M.; Wiltink, J.; Otten, D.; Werner, A.; Wild, P.S.; Münzel, T.; Lackner, K.J.; Pfeiffer, N.; et al. Psychosomatic medicine in the Gutenberg Health Study (GHS)–Research questions, measurement instruments, selected results. Z. Fur Psychosom. Med. Und Psychother. 2020, 66, 355–375. [Google Scholar] [CrossRef]
- Wild, P.S.; Zeller, T.; Beutel, M.; Blettner, M.; Dugi, K.A.; Lackner, K.J.; Pfeiffer, N.; Münzel, T.; Blankenberg, S. The Gutenberg Health Study. Bundesgesundheitsblatt Gesundh. Gesundh. 2012, 55, 824–829. [Google Scholar] [CrossRef]
- Hackenberg, B.; Döge, J.; Lackner, K.J.; Beutel, M.E.; Münzel, T.; Pfeiffer, N.; Nagler, M.; Schmidtmann, I.; Wild, P.S.; Matthias, C.; et al. Hearing Loss and Its Burden of Disease in a Large German Cohort-Hearing Loss in Germany. Laryngoscope 2021, 132, 1843–1849. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Wiltink, J.; Beutel, M.E.; Till, Y.; Ojeda, F.M.; Wild, P.S.; Münzel, T.; Blankenberg, S.; Michal, M. Prevalence of distress, comorbid conditions and well being in the general population. J. Affect. Disord. 2011, 130, 429–437. [Google Scholar] [CrossRef]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef]
- Gierk, B.; Kohlmann, S.; Kroenke, K.; Spangenberg, L.; Zenger, M.; Brähler, E.; Löwe, B. The somatic symptom scale-8 (SSS-8): A brief measure of somatic symptom burden. JAMA Intern. Med. 2014, 174, 399–407. [Google Scholar] [CrossRef]
- Al-Rawashdeh, B.M.; Saleh, M.Y.N.; Mustafa, R.B.; Alkhoujah, M.F.; Elkhatib, A.H.; Alsghaireen, H.; Hubaishy, L.Z. Prevalence of depression and anxiety among otolaryngology outpatients at Jordan University Hospital. Perspect. Psychiatr. Care 2019, 55, 383–395. [Google Scholar] [CrossRef]
- Park, M.; Kang, S.H.; Nari, F.; Park, E.C.; Jang, S.I. Association between tinnitus and depressive symptoms in the South Korean population. PLoS ONE 2021, 16, e0261257. [Google Scholar] [CrossRef]
- Williams, A.P.; Gourishetti, S.C.; Flaherty, M.A.; Eisenman, D.J. Anxiety, Depression, and Symptom Severity in Patients with Pulsatile and Non-Pulsatile Tinnitus. Laryngoscope 2022. early view. [Google Scholar] [CrossRef]
- Boecking, B.; Biehl, R.; Brueggemann, P.; Mazurek, B. Health-Related Quality of Life, Depressive Symptoms, Anxiety, and Somatization Symptoms in Male and Female Patients with Chronic Tinnitus. J. Clin. Med. 2021, 10, 2798. [Google Scholar] [CrossRef]
- World Health Organization. World Report on Hearing. Available online: https://www.who.int/publications/i/item/world-report-on-hearing (accessed on 7 August 2021).
- Vanneste, S.; Plazier, M.; der Loo, E.; de Heyning, P.V.; Congedo, M.; De Ridder, D. The neural correlates of tinnitus-related distress. Neuroimage 2010, 52, 470–480. [Google Scholar] [CrossRef]
- De Ridder, D.; Fransen, H.; Francois, O.; Sunaert, S.; Kovacs, S.; Van De Heyning, P. Amygdalohippocampal involvement in tinnitus and auditory memory. Acta Oto-Laryngol. 2006, 126, 50–53. [Google Scholar] [CrossRef]
- Schlee, W.; Weisz, N.; Bertrand, O.; Hartmann, T.; Elbert, T. Using auditory steady state responses to outline the functional connectivity in the tinnitus brain. PLoS ONE 2008, 3, e3720. [Google Scholar] [CrossRef]
- De Ridder, D.; Elgoyhen, A.B.; Romo, R.; Langguth, B. Phantom percepts: Tinnitus and pain as persisting aversive memory networks. Proc. Natl. Acad. Sci. USA 2011, 108, 8075–8080. [Google Scholar] [CrossRef]
- Blazer, D.G.; Tucci, D.L. Hearing loss and psychiatric disorders: A review. Psychol. Med. 2019, 49, 891–897. [Google Scholar] [CrossRef]
- Jastreboff, P.J.; Hazell, J.W. A neurophysiological approach to tinnitus: Clinical implications. Br. J. Audiol. 1993, 27, 7–17. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All (n) | Male (n) | Female (n) | p-Value | |
|---|---|---|---|---|
| n | 8539 | 4362 | 4177 | <0.0001 |
| Average Age years (SD) | 60.7 (13.7) | 61.4 (13.7) | 59.9 (13.5) | <0.0001 |
| Tinnitus prevalence % (n) | 28.0% (2387) | 31.7% (1.382) | 24.1% (1.005) | <0.0001 |
| Tinnitus burden 1–6 (SD) | 2.39 (1.33) | 2.35 (1.33) | 2.44 (1.34) | 0.11 |
| PHQ-9 median score (Q1/Q3) * | 2 (1/5) | 2 (0/4) | 3 (1/5) | <0.0001 |
| PHQ-9 ≥ 10% (n) | 5.5% (466) | 4.4% (191) | 6.7% (275) | <0.0001 |
| GAD-7 median score (Q1/Q3) * | 1 (0/4) | 1 (0/3) | 2 (0/5) | <0.0001 |
| GAD-7 ≥ 10% (n) | 3.9% (169) | 2.6% (57) | 5.3% (112) | <0.0001 |
| SSS-8 mean score (SD) | 5.70 (4.78) | 5.03 (4.35) | 6.40 (5.09) | <0.0001 |
| SSS-8 ≥ 8% (n) | 30.6% (2584) | 25.0% (1072) | 36.6% (1512) | <0.0001 |
| Tinnitus | Yes [95% CI] | No [95% CI] |
|---|---|---|
| Study cohort: | ||
| PHQ-9 ≥ 10 | 7.9% [6.9%; 9.1%] | 4.6% [4.1%; 5,2%] |
| GAD-7 ≥ 10 | 5.4% [4.3%; 6.9%] | 3.3% [2.7%; 4.0%] |
| SSS-8 ≥ 8 | 40.4% [38.4%; 42.4%] | 26.9% [25.8%; 28.0%] |
| European standard population 2013 *: | ||
| PHQ-9 ≥ 10 | 9.5% [8.3%; 10.9%] | 5.6% [5.0%; 6.2%] |
| GAD-7 ≥ 10 | 8.8% [7.6%; 10.1%] | 5.5% [4.9%; 6.1%] |
| SSS-8 ≥ 8 | 41.0% [38.9%; 43.1%] | 26.6% [25.5%; 27.7%] |
| German standard population 2021 *: | ||
| PHQ-9 ≥ 10 | 9.3% [8.1%; 10.6%] | 5.5% [5.0%; 6.1%] |
| GAD-7 ≥ 10 | 5.6% [4.3%; 7.3%] | 3.3% [2.7%; 4.2%] |
| SSS-8 ≥ 8 | 41.6% [39.5%; 43.7%] | 27.1% [26.0%; 28.2%] |
| WHO Hearing Impairment | All (n) | Males (n) | Females (n) | p-Value |
|---|---|---|---|---|
| No (<20 dB) | 46.6% (2418) | 41.8% (1111) | 51.7% (1307) | <0.0001 |
| Mild to moderately severe (20–64.9 dB) | 51.4% (2664) | 56.0% (1490) | 46.5% (1174) | <0.0001 |
| Severe to complete (≥65 dB) | 2.0% (104) | 2.2% (58) | 1.8% (46) | 0.37 |
| Tinnitus | Yes [95% CI] | No [95% CI] |
|---|---|---|
| Study cohort: | ||
| No (<20 dB) | 36.4% [33.8%; 39.1%] | 50.2% [48.6%; 51.8%] |
| Mild to moderately severe (20–64.9 dB) | 59.3% [56.6%; 62.0%] | 48.6% [47.0%; 50.2%] |
| Severe to complete (≥65 dB) | 4.3% [3.3%; 5.5%] | 1.2% [0.9%; 1.6%] |
| European standard population 2013 *: | ||
| No (<20 dB) | 51.3% [48.4%; 54.2%] | 66.8% [65.3%; 68.3%] |
| Mild to moderately severe (20–64.9 dB) | 45.8% [42.9%; 48.7%] | 32.5% [31.0%; 34.0%] |
| Severe to complete (≥65 dB) | 2.9% [2.0%; 4.0%] | 0.7% [0.5%; 1.0%] |
| German standard population 2021 *: | ||
| No (<20 dB) | 49.0% [46.1%; 51.9%] | 63.9% [62.3%; 65.4%] |
| Mild to moderately severe (20–64.9 dB) | 47.6% [44.8%; 50.5%] | 35.2% [33.7%; 36.8%] |
| Severe to complete (≥65 dB) | 3.4% [2.4%; 4.6%] | 0.9% [0.6%; 1.2%] |
| Tinnitus (Yes) | OR | 95% CI | p-Value |
|---|---|---|---|
| Mild to moderately severe hearing loss (vs. normal hearing), adjusted for: | |||
| PHQ-9 ≥ 10 | 1.645 | 1.400, 1.934 | <0.0001 |
| GAD-7 ≥ 10 | 1.739 | 1.392, 2.178 | <0.0001 |
| SSS-8 ≥ 8 | 1.616 | 1.373, 1.904 | <0.0001 |
| PHQ-9 ≥ 10, GAD-7 ≥ 10, and SSS-8 ≥ 8 | 1.733 | 1.384, 2.174 | <0.0001 |
| Severe to complete hearing loss (vs. normal hearing), adjusted for: | |||
| PHQ-9 ≥ 10 | 4.677 | 3.057, 7.186 | <0.0001 |
| GAD-7 ≥ 10 | 5.112 | 2.948, 8.914 | <0.0001 |
| SSS-8 ≥ 8 | 4.502 | 2.932, 6.943 | <0.0001 |
| PHQ-9 ≥ 10, GAD-7 ≥ 10, and SSS-8 ≥ 8 | 4.819 | 2.763, 8.445 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hackenberg, B.; Döge, J.; O’Brien, K.; Bohnert, A.; Lackner, K.J.; Beutel, M.E.; Michal, M.; Münzel, T.; Wild, P.S.; Pfeiffer, N.; et al. Tinnitus and Its Relation to Depression, Anxiety, and Stress—A Population-Based Cohort Study. J. Clin. Med. 2023, 12, 1169. https://doi.org/10.3390/jcm12031169
Hackenberg B, Döge J, O’Brien K, Bohnert A, Lackner KJ, Beutel ME, Michal M, Münzel T, Wild PS, Pfeiffer N, et al. Tinnitus and Its Relation to Depression, Anxiety, and Stress—A Population-Based Cohort Study. Journal of Clinical Medicine. 2023; 12(3):1169. https://doi.org/10.3390/jcm12031169
Chicago/Turabian StyleHackenberg, Berit, Julia Döge, Karoline O’Brien, Andrea Bohnert, Karl J. Lackner, Manfred E. Beutel, Matthias Michal, Thomas Münzel, Philipp S. Wild, Norbert Pfeiffer, and et al. 2023. "Tinnitus and Its Relation to Depression, Anxiety, and Stress—A Population-Based Cohort Study" Journal of Clinical Medicine 12, no. 3: 1169. https://doi.org/10.3390/jcm12031169
APA StyleHackenberg, B., Döge, J., O’Brien, K., Bohnert, A., Lackner, K. J., Beutel, M. E., Michal, M., Münzel, T., Wild, P. S., Pfeiffer, N., Schulz, A., Schmidtmann, I., Matthias, C., & Bahr, K. (2023). Tinnitus and Its Relation to Depression, Anxiety, and Stress—A Population-Based Cohort Study. Journal of Clinical Medicine, 12(3), 1169. https://doi.org/10.3390/jcm12031169