Intra-Cardiac versus Transesophageal Echocardiographic Guidance for Left Atrial Appendage Occlusion with a Watchman FLX Device

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Device and Implantation Procedure
2.3. Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Patient Population
3.2. Procedural Results and In-Hospital Outcomes
3.3. Follow-Up
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CCT | Cardiac computed tomography |
| ICE | Intra-cardiac echocardiography |
| LAAO | Left atrial appendage occlusion |
| NVAF | Non-valvular atrial fibrillation |
| OACs | Oral anticoagulants |
| TIA | Transitory ischemic attacks |
| TEE | Transesophageal echocardiography |
References
- Go, A.S.; Hylek, E.M.; Phillips, K.A.; Chang, Y.; Henault, L.E.; Selby, J.V.; Singer, D.E. Prevalence of diagnosed atrial fibrillation in adults: National implications for rhythm management and stroke prevention: The anticoagulation and risk factors in atrial fibrillation (ATRIA) Study. JAMA 2001, 285, 2370–2375. [Google Scholar] [CrossRef] [PubMed]
- Zoni-Berisso, M.; Lercari, F.; Carazza, T.; Domenicucci, S. Epidemiology of atrial fibrillation: European perspective. Clin. Epidemiol. 2014, 6, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Kakkar, A.K.; Mueller, I.; Bassand, J.-P.; Fitzmaurice, D.A.; Goldhaber, S.Z.; Goto, S.; Haas, S.; Hacke, W.; Lip, G.Y.H.; Mantovani, L.G.; et al. Risk profiles and antithrombotic treatment of patients newly diagnosed with atrial fibrillation at risk of stroke: Perspectives from the international, observational, prospective GARFIELD registry. PLoS ONE 2013, 8, e6347. [Google Scholar] [CrossRef] [PubMed]
- Marini, C.; De Santis, F.; Sacco, S.; Russo, T.; Olivieri, L.; Totaro, R.; Carolei, A. Contribution of Atrial Fibrillation to Incidence and Outcome of Ischemic Stroke: Results From a Population-Based Study. Stroke 2005, 36, 1115–1119. [Google Scholar] [CrossRef] [PubMed]
- Hart, R.G.; Pearce, L.A.; Aguilar, M.I. Meta-analysis: Antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann. Intern. Med. 2007, 146, 857–867. [Google Scholar] [CrossRef] [PubMed]
- Boersma, L.V.; Ince, H.; Kische, S.; Pokushalov, E.; Schmitz, T.; Schmidt, B.; Gori, T.; Meincke, F.; Protopopov, A.V.; Betts, T.; et al. Efficacy and safety of left atrial appendage closure with WATCHMAN in patients with or without contraindication to oral anticoagulation: 1-Year follow-up outcome data of the EWOLUTION trial. Heart Rhythm 2017, 14, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Nielsen-Kudsk, J.E.; Berti, S.; De Backer, O.; Aguirre, D.; Fassini, G.; Cruz-Gonzalez, I.; Grassi, G.; Tondo, C. Use of Intracardiac Compared with Transesophageal Echocardiography for Left Atrial Appendage Occlusion in the Amulet Observational Study. JACC Cardiovasc. Interv. 2019, 12, 1030–1039. [Google Scholar] [CrossRef] [PubMed]
- Alkhouli, M.; Chaker, Z.; Alqahtani, F.; Raslan, S.; Raybuck, B. Outcomes of Routine Intracardiac Echocardiography to Guide Left Atrial Appendage Occlusion. JACC Clin. Electrophysiol. 2020, 6, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, J.M.; Teixeira, R.; Puga, L.; Costa, M.; Gonçalves, L. Comparison of intracardiac and transoesophageal echocardiography for guidance of percutaneous left atrial appendage occlusion: A meta-analysis. Echocardiography 2019, 36, 1330–1337. [Google Scholar] [CrossRef] [PubMed]
- Berti, S.; Pastormerlo, L.E.; Santoro, G.; Brscic, E.; Montorfano, M.; Vignali, L.; Danna, P.; Tondo, C.; Rezzaghi, M.; D’Amarigo, G.; et al. Intracardiac Versus Transesophageal Echocardiographic Guidance for Left Atrial Appendage Occlusion: The LAAO Italian Multicenter Registry. JACC Cardiovasc. Interv. 2018, 11, 1086–1092. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The euro heart survey on atrial fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Pisters, R.; Lane, D.A.; Nieuwlaat, R.; de Vos, C.B.; Crijns, H.J.; Lip, G.Y. A novel user friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: The Euro Heart Survey. Chest 2010, 138, 1093–1100. [Google Scholar] [CrossRef] [PubMed]
- Schulman, S.; Kearon, C. Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar] [PubMed]
- Reddy, V.Y.; Doshi, S.K.; Kar, S.; Gibson, D.N.; Price, M.J.; Huber, K.; Horton, R.P.; Buchbinder, M.; Neuzil, P.; Gordon, N.T.; et al. 5-Year Outcomes After Left Atrial Appendage Closure: From the PREVAIL and PROTECT AF Trials. J. Am. Coll. Cardiol. 2017, 70, 2964–2975. [Google Scholar] [CrossRef]
- Lennon, M.J.; Gibbs, N.M.; Weightman, W.M.; Leber, J.; Ee, H.C.; Yusoff, I.F. Transesophageal echocardiographyrelated gastrointestinal complications in cardiac surgical patients. J. Cardiothorac. Vasc. Anesth. 2005, 19, 135–141. [Google Scholar] [CrossRef]
- Korsholm, K.; Jensen, J.M.; Nielsen-Kudsk, J.E. Intracardiac echocardiography from the Left Atrium for Procedural Guidance of Transcatheter Left Atrial Appendage Occlusion. JACC Cardiovasc. Interv. 2017, 10, 2198–2206. [Google Scholar] [CrossRef]
- Şaylık, F.; Çınar, T.; Akbulut, T.; Hayıroğlu, M.İ. Comparison of catheter ablation and medical therapy for atrial fibrillation in heart failure patients: A meta-analysis of randomized controlled trials. Heart Lung 2023, 57, 69–74. [Google Scholar] [CrossRef]
- Michiels, K.; Heffinck, E.; Astudillo, P.; Wong, I.; Mortier, P.; Bavo, A.M. Automated MSCT Analysis for Planning Left Atrial Appendage Occlusion Using Artificial Intelligence. J. Interv. Cardiol. 2022, 2022, 5797431. [Google Scholar] [CrossRef]
- Hayıroğlu, M.İ.; Altay, S. The Role of Artificial Intelligence in Coronary Artery Disease and Atrial Fibrillation. Balkan Med. J. 2023, 40, 151–152. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Patient | ALL (n = 772) | ICE (n = 149) | TEE (623) | p |
|---|---|---|---|---|
| Age | 76.5 ± 8.3 | 77 ± 7.5 | 76.3 ± 8 | ns |
| Male, % | 509 (65%) | 97 (65%) | 407 (65%) | ns |
| CHA2DS2VASC | 4.14 ± 1.47 | 4.2 ± 1.8 | 4.1 ± 1.4 | ns |
| HASBLED | 3.69 ± 1.1 | 3.5 ± 1.4 | 3.7 ± 1.1 | ns |
| Creatinine | 1.4 ± 1 | 1.3 ± 1.1 | 1.44 ± 1.2 | ns |
| eGFR | 59 ± 30 | 60 ± 28 | 58.4 ± 28 | ns |
| LVEF | 52 ± 10 | 54 ± 11 | 51 ± 11 | ns |
| BMI | 26.5 ± 3 | 26 ± 4 | 26.7 ± 4.4 | ns |
| Permanent AF, % | 376 (48%) | 72 (48%) | 304 (48%) | ns |
| Diabetes | 264 (33%) | 45 (30%) | 219 (34%) | ns |
| Arterial hypertension | 606 (78%) | 115 (77%) | 491 (78%) | ns |
| Previous stroke | 106 (13%) | 19 (12%) | 87 (13%) | ns |
| GI bleeding | 240 (30%) | 40 (26%) | 200 (31%) | ns |
| Intra-cranial/subdural bleeding | 115 (14%) | 25 (16%) | 90 (14%) | ns |
| Severe CKD | 126 (16%) | 18 (12%) | 108 (17%) | ns |
| Hematologic disorder | 102 (13%) | 28 (18%) | 74 (11%) | 0.038 |
| Ischemic stroke in OACs | 54 (7%) | 8 (5.5%) | 46 (7.3%) | ns |
| DAPT+OACs | 7 (0.9%) | 2 (1.3%) | 5 (0.8%) | ns |
| Very high bleeding risk | 122 (15%) | 25 (16%) | 97 (15%) | ns |
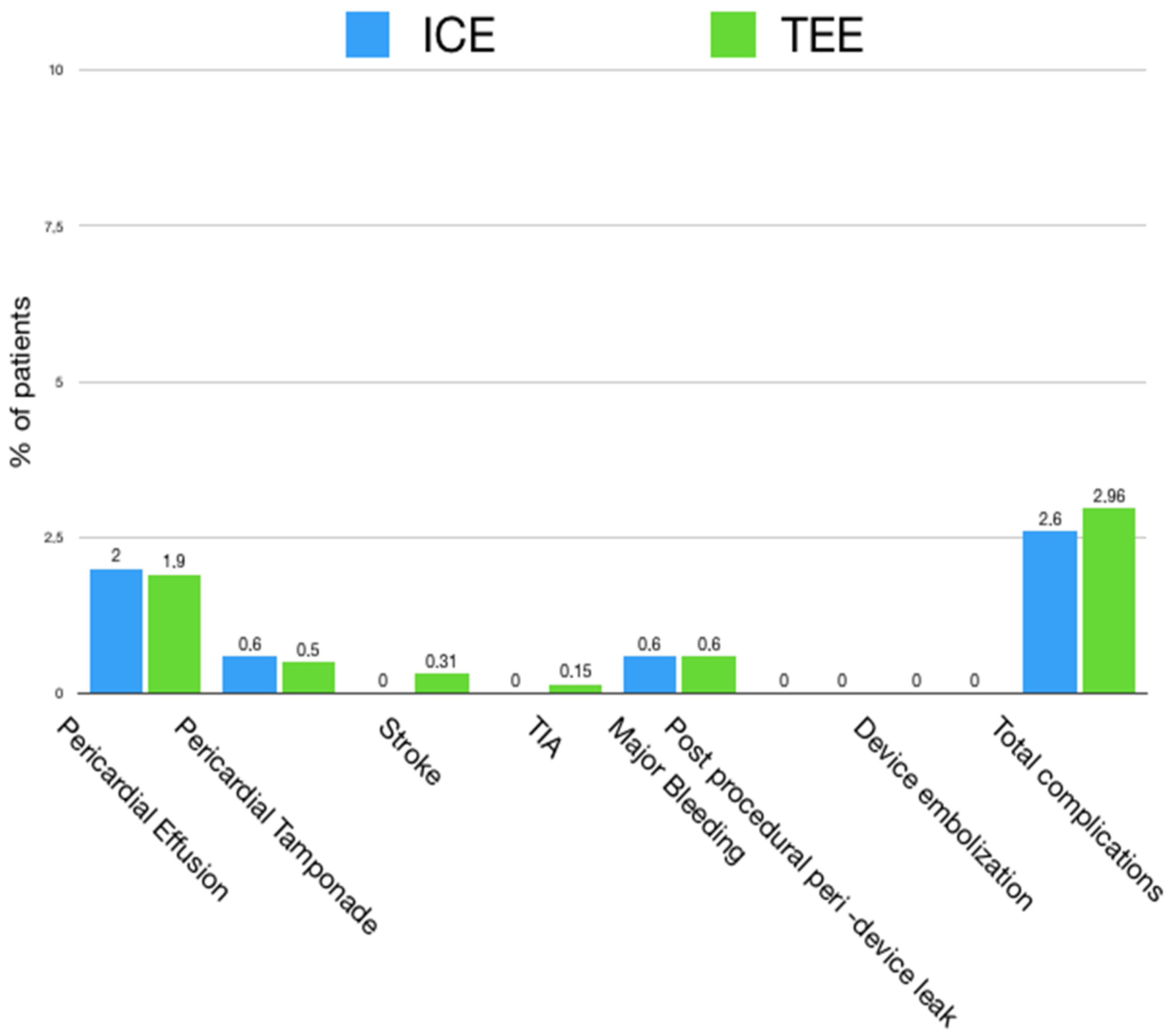
| ALL | ICE | TEE | p | |
|---|---|---|---|---|
| Patients | 772 | 149 | 623 | |
| Pericardial effusion | 15 (1.9%) | 3 (2%) | 12 (1.9%) | NS |
| Pericardial tamponade | 4 (0.5%) | 1 (0.55%) | 3 (0.47%) | NS |
| Stroke | 2 (0.25%) | 0 (0%) | 2 (0.31%) | NS |
| TIA | 1 (0.13%) | 0 (0%) | 1 (0.15%) | NS |
| Device embolization | 0 (0%) | 0 (0%) | 0 (0%) | NS |
| Peri-device leak > 5 mm | 0 (0%) | 0 (0%) | 0 (0%) | NS |
| Major bleeding | 5 (0.6%) | 1 (0.6%) | 4 (0.63%) | NS |
| Death | 0 (0%) | 0 (0%) | 0 (0%) | NS |
| Technical success | 772 (100%) | 149 (100%) | 623 (100%) | NS |
| Procedural success | 763 (98.5%) | 147 (98.7%) | 616 (98.5%) | NS |
| Fluoroscopy time | 18.7 ± 14 | 24 ± 15 | 17 ± 13 | 0.031 |
| Procedure time | 63.8 ± 34 | 73 ± 31 | 61.9 ± 36 | 0.042 |
| Contrast volume | 92.11 ± 58 | 107 ± 53 | 88 ± 59 | 0.071 |
| In-hospital stay (days) | 5.6 ± 5 | 5.3 ± 4 | 5.8 ± 6 | 0.028 |
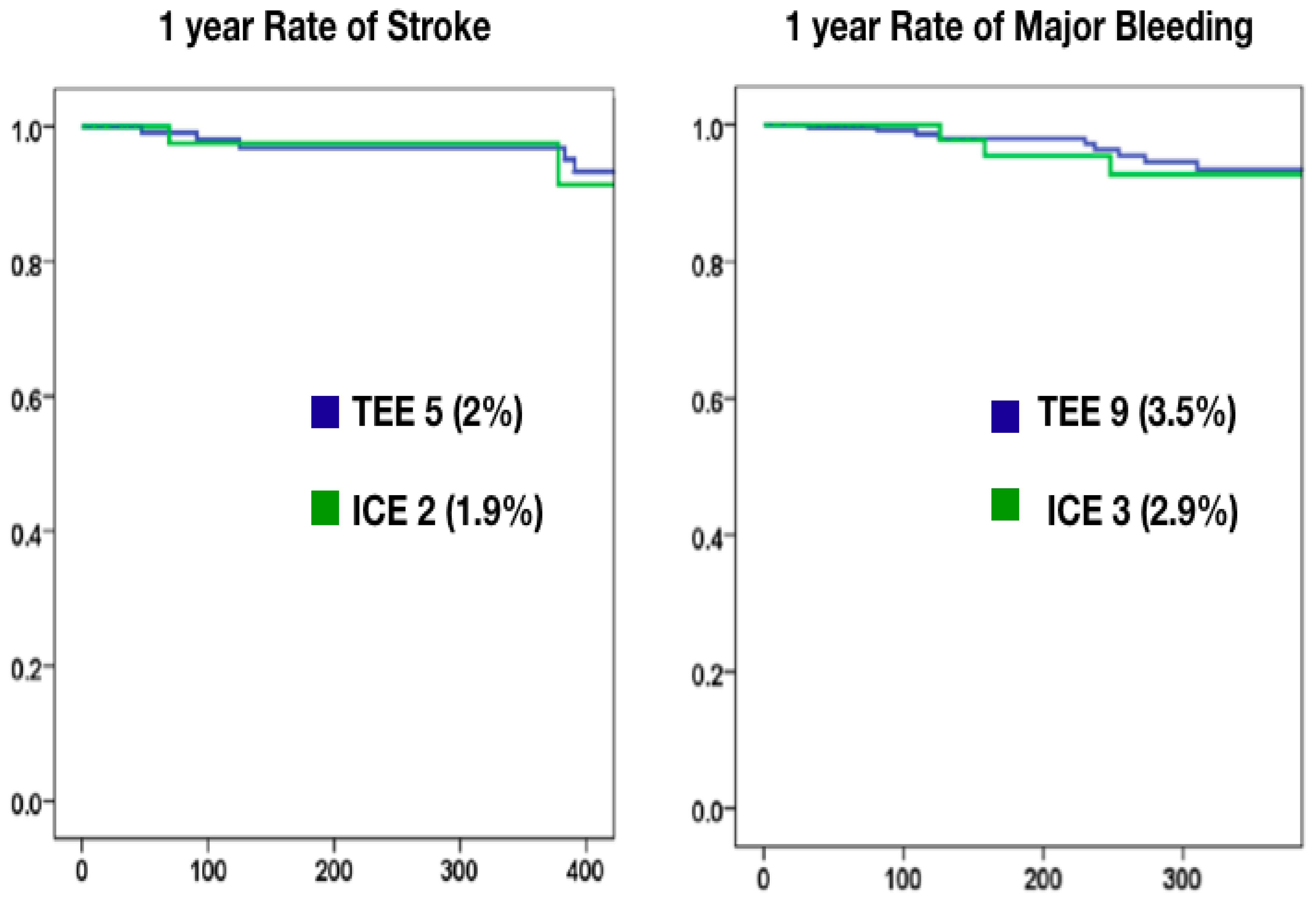
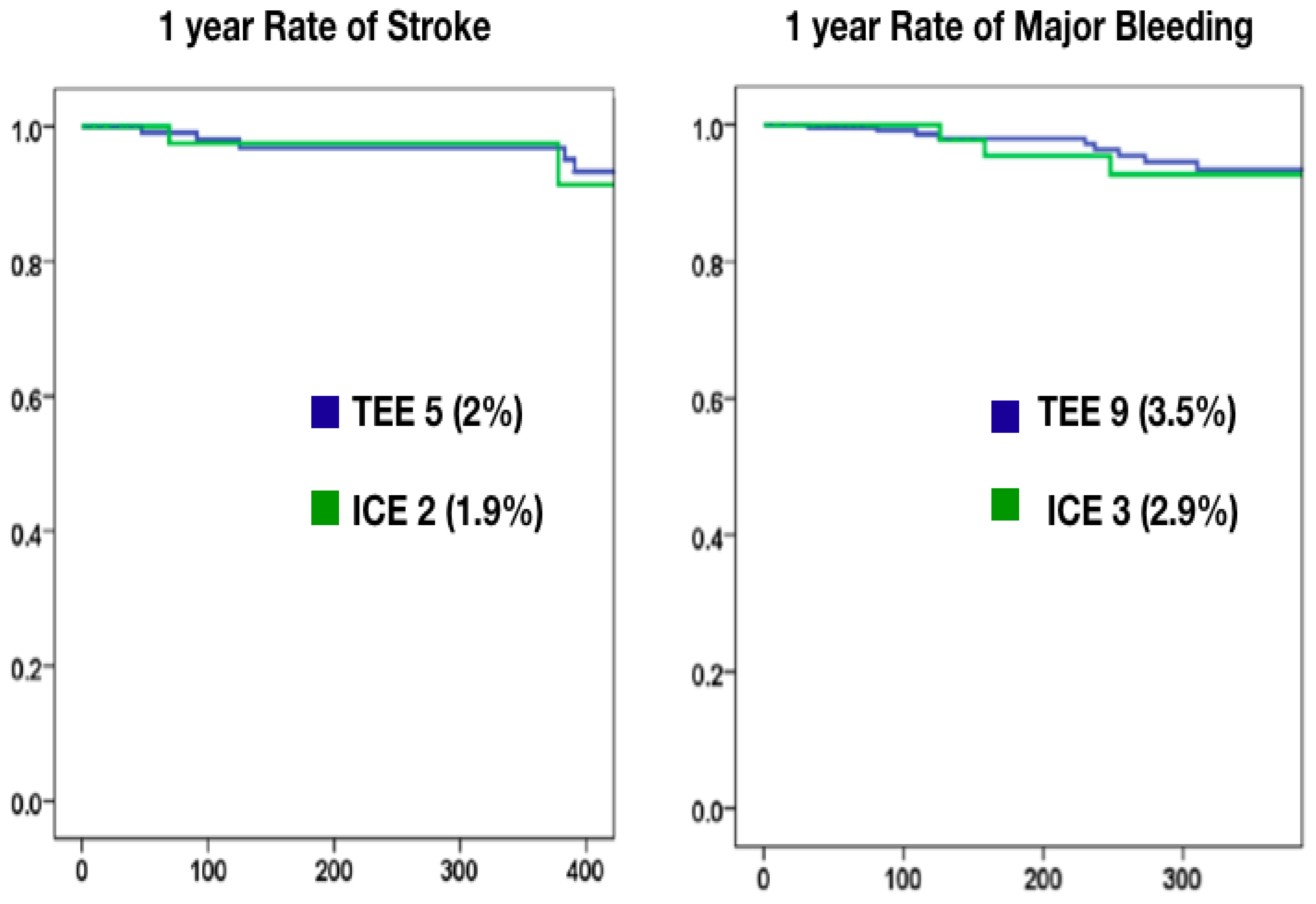
| ALL (n = 342) | ICE (n = 102) | TEE (n = 240) | p | |
|---|---|---|---|---|
| Stroke | 7 (2%) | 2 (1.9%) | 5 (2%) | NS |
| TIA | 2 (0.5%) | 0 (0%) | 2 (0.8%) | NS |
| Death | 11 (3.2%) | 3 (2.9%) | 8 (3.3%) | NS |
| Major bleeding | 12 (3.5%) | 3 (2.9%) | 9 (3.7%) | NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pastormerlo, L.E.; Tondo, C.; Fassini, G.; Nicosia, A.; Ronco, F.; Contarini, M.; Giacchi, G.; Grasso, C.; Casu, G.; Romeo, M.R.; et al. Intra-Cardiac versus Transesophageal Echocardiographic Guidance for Left Atrial Appendage Occlusion with a Watchman FLX Device. J. Clin. Med. 2023, 12, 6658. https://doi.org/10.3390/jcm12206658
Pastormerlo LE, Tondo C, Fassini G, Nicosia A, Ronco F, Contarini M, Giacchi G, Grasso C, Casu G, Romeo MR, et al. Intra-Cardiac versus Transesophageal Echocardiographic Guidance for Left Atrial Appendage Occlusion with a Watchman FLX Device. Journal of Clinical Medicine. 2023; 12(20):6658. https://doi.org/10.3390/jcm12206658
Chicago/Turabian StylePastormerlo, Luigi Emilio, Claudio Tondo, Gaetano Fassini, Antonino Nicosia, Federico Ronco, Marco Contarini, Giuseppe Giacchi, Carmelo Grasso, Gavino Casu, Maria Rita Romeo, and et al. 2023. "Intra-Cardiac versus Transesophageal Echocardiographic Guidance for Left Atrial Appendage Occlusion with a Watchman FLX Device" Journal of Clinical Medicine 12, no. 20: 6658. https://doi.org/10.3390/jcm12206658
APA StylePastormerlo, L. E., Tondo, C., Fassini, G., Nicosia, A., Ronco, F., Contarini, M., Giacchi, G., Grasso, C., Casu, G., Romeo, M. R., Mazzone, P., Limite, L., Caramanno, G., Geraci, S., Pagnotta, P., Chiarito, M., Tamburino, C., & Berti, S. (2023). Intra-Cardiac versus Transesophageal Echocardiographic Guidance for Left Atrial Appendage Occlusion with a Watchman FLX Device. Journal of Clinical Medicine, 12(20), 6658. https://doi.org/10.3390/jcm12206658