

Relationship between Dry Eye Disease and Dyslipidemia: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
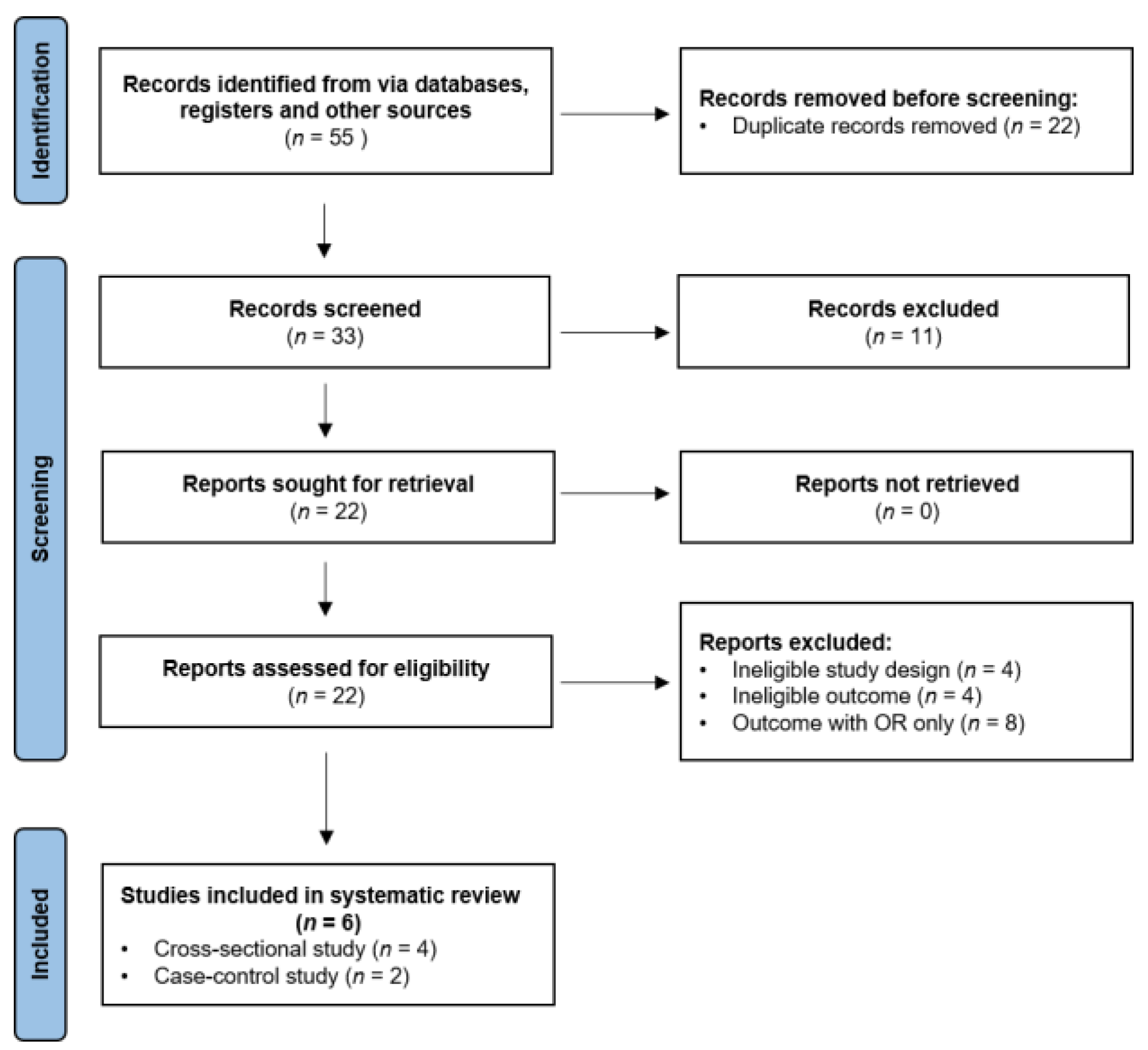
2.1. Search Strategy and Data Retrieval Protocol
2.2. Inclusion and Exclusion Criteria
3. Results
3.1. Highlights of Each Study
3.2. Quantitative Data Analysis
4. Discussion
4.1. Higher Prevalence of Dyslipidemia in Female DED Patients
4.2. Abnormal Lipid Profiles Are Not Significantly Associated with DED Patients
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gayton, J.L. Etiology, prevalence, and treatment of dry eye disease. Clin. Ophthalmol. 2009, 3, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Messmer, E.M. The pathophysiology, diagnosis, and treatment of dry eye disease. Dtsch. Arztebl. Int. 2015, 112, 71–81, quiz 82. [Google Scholar] [CrossRef] [PubMed]
- Schaumberg, D.A.; Dana, R.; Buring, J.E.; Sullivan, D.A. Prevalence of dry eye disease among US men: Estimates from the Physicians’ Health Studies. Arch. Ophthalmol. 2009, 127, 763–768. [Google Scholar] [CrossRef] [PubMed]
- Ay, İ.E.; Şenol, Y.; Gobeka, H.H.; Doğan, M. Is a Dry Eye Disorder in Firefighters an Occupational Disease? Med. Lav. 2023, 114, e2023020. [Google Scholar] [PubMed]
- Chia, E.-M.; Mitchell, P.; Rochtchina, E.; Lee, A.J.; Maroun, R.; Wang, J.J. Prevalence and associations of dry eye syndrome in an older population: The Blue Mountains Eye Study. Clin. Exp. Ophthalmol. 2003, 31, 229–232. [Google Scholar] [CrossRef] [PubMed]
- Miljanović, B.; Dana, R.; Sullivan, D.A.; Schaumberg, D.A. Impact of dry eye syndrome on vision-related quality of life. Am. J. Ophthalmol. 2007, 143, 409–415.e2. [Google Scholar] [CrossRef] [PubMed]
- Tong, L.; Waduthantri, S.; Wong, T.Y.; Saw, S.M.; Wang, J.J.; Rosman, M.; Lamoureux, E. Impact of symptomatic dry eye on vision-related daily activities: The Singapore Malay Eye Study. Eye 2010, 24, 1486–1491. [Google Scholar] [CrossRef] [PubMed]
- Lam, S.M.; Tong, L.; Yong, S.S.; Li, B.; Chaurasia, S.S.; Shui, G.; Wenk, M.R. Meibum lipid composition in Asians with dry eye disease. PLoS ONE 2011, 6, e24339. [Google Scholar] [CrossRef]
- Goto, E.; Dogru, M.; Fukagawa, K.; Uchino, M.; Matsumoto, Y.; Saiki, M.; Tsubota, K. Successful tear lipid layer treatment for refractory dry eye in office workers by low-dose lipid application on the full-length eyelid margin. Am. J. Ophthalmol. 2006, 142, 264–270.e1. [Google Scholar] [CrossRef]
- Craig, J.P.; Tomlinson, A. Importance of the lipid layer in human tear film stability and evaporation. Optom. Vis. Sci. 1997, 74, 8–13. [Google Scholar] [CrossRef]
- Bron, A.; Tiffany, J.; Gouveia, S.; Yokoi, N.; Voon, L. Functional aspects of the tear film lipid layer. Exp. Eye Res. 2004, 78, 347–360. [Google Scholar] [CrossRef] [PubMed]
- Butovich, I.A. Lipidomics of human Meibomian gland secretions: Chemistry, biophysics, and physiological role of Meibomian lipids. Prog. Lipid Res. 2011, 50, 278–301. [Google Scholar] [CrossRef]
- Nicolaides, N. Skin Lipids. II. Lipid Class Composition of Samples from Various Species and Anatomical Sites. J. Am. Oil Chem. Soc. 1965, 42, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Braich, P.S.; Howard, M.K.; Singh, J.S. Dyslipidemia and its association with meibomian gland dysfunction. Int. Ophthalmol. 2016, 36, 469–476. [Google Scholar] [CrossRef]
- Wang, T.-J.; Wang, I.-J.; Hu, C.-C.; Lin, H.-C. Comorbidities of dry eye disease: A nationwide population-based study. Acta Ophthalmol. 2012, 90, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Roh, H.C.; Lee, J.K.; Kim, M.; Oh, J.H.; Chang, M.W.; Chuck, R.S.; Park, C.Y. Systemic Comorbidities of Dry Eye Syndrome: The Korean National Health and Nutrition Examination Survey V, 2010 to 2012. Cornea 2016, 35, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Vehof, J.; Snieder, H.; Jansonius, N.; Hammond, C.J. Prevalence and risk factors of dry eye in 79,866 participants of the population-based Lifelines cohort study in the Netherlands. Ocul. Surf. 2021, 19, 83–93. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Rev. Esp. Cardiol. Engl. Ed. 2021, 74, 790–799. [Google Scholar] [CrossRef]
- Schiavo, J.H. PROSPERO: An International Register of Systematic Review Protocols. Med. Ref. Serv. Q. 2019, 38, 171–180. [Google Scholar] [CrossRef]
- Chun, Y.H.; Kim, H.R.; Han, K.; Park, Y.-G.; Song, H.J.; Na, K.-S. Total cholesterol and lipoprotein composition are associated with dry eye disease in Korean women. Lipids Health Dis. 2013, 12, 84. [Google Scholar] [CrossRef]
- Park, H.W.; Park, J.W. The Association between Symptoms of Dry Eye Syndrome and Metabolic Outcome in a General Population in Korea. J. Korean Med. Sci. 2016, 31, 1121–1126. [Google Scholar] [CrossRef] [PubMed]
- Rathnakumar, K.; Ramachandran, K.; Baba, D.; Ramesh, V.; Anebaracy, V.; Vidhya, R.; Vinothkumar, R.; Poovitha, R.; Geetha, R. Prevalence of dry eye disease and its association with dyslipidemia. J. Basic Clin. Physiol. Pharmacol. 2018, 29, 195–199. [Google Scholar] [CrossRef]
- Choi, H.R.; Lee, J.H.; Lee, H.K.; Song, J.S.; Kim, H.C. Association Between Dyslipidemia and Dry Eye Syndrome Among the Korean Middle-Aged Population. Cornea 2020, 39, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Wolffsohn, J.S.; Arita, R.; Chalmers, R.; Djalilian, A.; Dogru, M.; Dumbleton, K.; Gupta, P.K.; Karpecki, P.; Lazreg, S.; Pult, H.; et al. TFOS DEWS II Diagnostic Methodology report. Ocul. Surf. 2017, 15, 539–574. [Google Scholar] [CrossRef] [PubMed]
- Shokr, H.; Wolffsohn, J.S.; Huarte, S.T.; Scarpello, E.; Gherghel, D. Dry eye disease is associated with retinal microvascular dysfunction and possible risk for cardiovascular disease. Acta Ophthalmol. 2021, 99, e1236–e1242. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.R.; Kim, N.H.; Lee, J.-M.; Choi, D.P.; Seo, Y.; Cho, W.K.; Song, J.S.; Lee, H.K.; Kim, H.C. Risk Factors Influencing the Occurrence and Severity of Symptomatic Dry Eye Syndrome: A Cross-sectional Study. Ophthalmic Epidemiol. 2021, 28, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Ooi, K.G.; Lee, M.H.; Burlutsky, G.; Gopinath, B.; Mitchell, P.; Watson, S. Association of dyslipidaemia and oral statin use, and dry eye disease symptoms in the Blue Mountains Eye Study. Clin. Exp. Ophthalmol. 2019, 47, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Mussi, N.; Haque, W.; Robertson, D.M. The Association Between Risk Factors for Metabolic Syndrome and Meibomian Gland Disease in a Dry Eye Cohort. Clin. Ophthalmol. 2021, 15, 3821–3832. [Google Scholar] [CrossRef] [PubMed]
- Schaumberg, D.A.; Sullivan, D.A.; Buring, J.E.; Dana, M. Prevalence of dry eye syndrome among US women. Am. J. Ophthalmol. 2003, 136, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Tankó, L.B.; Bagger, Y.Z.; Qin, G.; Alexandersen, P.; Larsen, P.J.; Christiansen, C. Enlarged waist combined with elevated triglycerides is a strong predictor of accelerated atherogenesis and related cardiovascular mortality in postmenopausal women. Circulation 2005, 111, 1883–1890. [Google Scholar] [CrossRef] [PubMed]
- Hulley, S.; Grady, D.; Bush, T.; Furberg, C.; Herrington, D.; Riggs, B.; Vittinghoff, E.; Heart and Estrogen/Progestin Replacement Study (HERS) Research Group. Randomized trial of estrogen plus progestin for secondary prevention of coronary heart disease in postmenopausal women. JAMA 1998, 280, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Talbott, E.; Guzick, D.; Clerici, A.; Berga, S.; Detre, K.; Weimer, K.; Kuller, L. Coronary heart disease risk factors in women with polycystic ovary syndrome. Arter. Thromb. Vasc. Biol. 1995, 15, 821–826. [Google Scholar] [CrossRef] [PubMed]
- Hjortland, M.C.; Mcnamara, P.M.; Kannel, W.B. Some atherogenic concomitants of menopause: The Framingham Study. Am. J. Epidemiol. 1976, 103, 304–311. [Google Scholar] [CrossRef]
- Carr, M.C.; Kim, K.H.; Zambon, A.; Mitchell, E.S.; Woods, N.F.; Casazza, C.P.; Purnell, J.Q.; Hokanson, J.E.; Brunzell, J.D.; Schwartz, R.S. Changes in LDL density across the menopausal transition. J. Investig. Med. 2000, 48, 245–250. [Google Scholar] [PubMed]
- Matthews, K.A.; Meilahn, E.; Kuller, L.H.; Kelsey, S.F.; Caggiula, A.W.; Wing, R.R. Menopause and risk factors for coronary heart disease. N. Engl. J. Med. 1989, 321, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.H.; Choi, Y.-H.; Paik, H.J.; Kim, M.K.; Wee, W.R.; Kim, D.H. Sex differences in the effect of aging on dry eye disease. Clin. Interv. Aging 2017, 12, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Dao, A.H.; Spindle, J.D.; Harp, B.A.; Jacob, A.; Chuang, A.Z.; Yee, R.W. Association of dyslipidemia in moderate to severe meibomian gland dysfunction. Am. J. Ophthalmol. 2010, 150, 371–375.e1. [Google Scholar] [CrossRef] [PubMed]
- Kuriakose, R.K.; Braich, P.S. Dyslipidemia and its Association with Meibomian Gland Dysfunction: A Systematic Review. Int. Ophthalmol. 2018, 38, 1809–1816. [Google Scholar] [CrossRef]
- Yoo, Y.-S.; Park, S.-K.; Hwang, H.-S.; Kim, H.-S.; Arita, R.; Na, K.-S. Association of Serum Lipid Level with Meibum Biosynthesis and Meibomian Gland Dysfunction: A Review. J. Clin. Med. 2022, 11, 4010. [Google Scholar] [CrossRef] [PubMed]
- Deplewski, D.; Qin, K.; Ciletti, N.; Rosenfield, R.L. Unique mode of lipogenic activation in rat preputial sebocytes. J. Nutr. Metab. 2011, 2011, 163631. [Google Scholar] [CrossRef] [PubMed]
- Yagyu, H.; Kitamine, T.; Osuga, J.-I.; Tozawa, R.-I.; Chen, Z.; Kaji, Y.; Oka, T.; Perrey, S.; Tamura, Y.; Ohashi, K.; et al. Absence of ACAT-1 attenuates atherosclerosis but causes dry eye and cutaneous xanthomatosis in mice with congenital hyperlipidemia. J. Biol. Chem. 2000, 275, 21324–21330. [Google Scholar] [CrossRef] [PubMed]
- Tsubota, K.; Yokoi, N.; Shimazaki, J.; Watanabe, H.; Dogru, M.; Yamada, M.; Kinoshita, S.; Kim, H.-M.; Tchah, H.-W.; Hyon, J.Y.; et al. New Perspectives on Dry Eye Definition and Diagnosis: A Consensus Report by the Asia Dry Eye Society. Ocul. Surf. 2017, 15, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Shimazaki, J. Definition and Diagnostic Criteria of Dry Eye Disease: Historical Overview and Future Directions. Investig. Opthalmol. Vis. Sci. 2018, 59, DES7–DES12. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Inclusion Criteria |
| Studies discussing the potential involvement of dyslipidemia in DED Studies with peer-reviewed retrospective (cross-sectional studies, case–control studies) and prospective designs Studies involving quantitative information on TC, TGs, LDL-C, and HDL-C in individuals with and without DED |
| Exclusion criteria |
| Studies in languages other than English Studies not involving human participants Clinical guidelines, consensus documents, reviews, and conference proceedings Studies focusing exclusively on MGD Studies reporting qualitative data only |
| Title | Country | Study Design | Case | Control | Diagnosis Method | Key Findings | References |
|---|---|---|---|---|---|---|---|
| Total cholesterol and lipoprotein composition are associated with dry eye disease in Korean women | South Korea | Cross-sectional study | 531 cases (116 men, 415 women; age >19 years) | 5096 controls (2292 men, 2804 women; age >19 years) | DED questionnaire survey | No statistically significant gender-related differences were observed in the values of TC, LDL-C, HDL-C, and TGs between individuals with and without DED. The prevalence of abnormal TC was significantly higher in women with DED than in their male counterparts. The prevalence of abnormal LDL-C was significantly higher in women aged over 65 with DED than in their male counterparts. The prevalence of low HDL-C was significantly lower in women with DED than in the control group. | Chun et al. [20] (June 2013) |
| The Association between Symptoms of Dry Eye Syndrome and Metabolic Outcome in a General Population in Korea | South Korea | Cross-sectional study | 2704 cases (744 men, 1960 women; age >19 years) | 12,590 controls (5782 men, 6808 women; age >19 years) | Delphi consensus method by a panel of 17 dry-eye experts | No statistically significant gender-related differences were observed in the values of TGs and HDL-C between individuals with and without DES. The prevalence of elevated TG was significantly higher in women with DES than in their male counterparts. | Park et al. [21] (April 2016) |
| Prevalence of dry eye disease and its association with dyslipidemia | India | Case-control study | 60 cases (23 men, 37 women; age: 25–70 years) | 60 controls (matched age and sex) | Questionnaire and clinical examinations | Compared with individuals without DED, individuals with DED (both men and women) demonstrated a statistically significant association with dyslipidemia (TGs, TC, HDL-C, and LDL-C values). The prevalence of dyslipidemia was significantly higher in women than in men. | Rathnakumar et al. [22] (November 2017) |
| Association Between Dyslipidemia and Dry Eye Syndrome Among the Korean Middle-Aged Population | South Korea | Cross-sectional study | 1117 cases (332 men, 785 women) | 1155 controls (522 men, 633 women) | OSDI | The prevalence of hypercholesterolemia was significantly higher in individuals with DES than in those without. The values of HDL-C were significantly higher in individuals with DES than in those without. A significant independent relationship was observed between dyslipidemia and DES in men after adjustment. No significant association between DES and dyslipidemia was observed in either premenopausal or postmenopausal women after adjustment. | Choi et al. [23] (July 2019) |
| Dry eye disease is associated with retinal microvascular dysfunction and possible risk for cardiovascular disease | United Kingdom | Case–control study | 25 cases (12 men, 15 women; age: 35–50 years) | 25 controls (15 men, 10 women; age: 35–50 years) | TFOS DEWS II criteria [24] | Compared with the control group, patients with DED had significantly higher values of TC and lower values of HDL-C. | Shokr et al. [25] (January 2021) |
| Risk Factors Influencing the Occurrence and Severity of Symptomatic Dry Eye Syndrome: A Cross-sectional Study | South Korea | Cross-sectional study | 230 cases (77 men, 153 women; age >40 years) | 245 controls (107 men, 138 women; age >40 years) | OSDI | The prevalence of DES was significantly higher in women than in men. Hypercholesterolemia and TC were not associated with DES or correlated with the severity of DES. | Choi et al. [26] (January 2021) |
| Reviewed Article | Mean TC | Mean LDL-C | Mean HDL-C | Mean TGs |
|---|---|---|---|---|
| Chun et al. [20] | ||||
| Men | ||||
| Case | 184.5 ± 3.4 | 110.4 ± 3.3 | 51.5 ± 1.5 | 134 ± 9.7 |
| Control | 187.2 ± 1 | 112.3 ± 0.9 | 49.6 ± 0.3 | 157.4 ± 3.9 |
| p value | 0.6799 | 0.8224 | 0.6395 | 0.7210 |
| Women | ||||
| Case | 185.8 ± 2.2 | 113.4 ± 1.9 | 56.3 ± 0.7 | 106.2 ± 4 |
| Control | 186.7 ± 0.9 | 113.9 ± 0.7 | 56 ± 0.3 | 109.3 ± 2 |
| p value | 0.4302 | 0.5698 | 0.2197 | 0.1337 |
| Park et al. [21] | ||||
| Men | ||||
| Case | 49.12 ± 11.63 | 149.30 ± 107.5 | ||
| Control | 49.20 ± 11.98 | 154.90 ± 127.20 | ||
| p value | 0.850 | 0.252 | ||
| Women | ||||
| Case | 55.01 ± 12.86 | 116.5 ± 72.72 | ||
| Control | 54.98 ± 12.80 | 115.0 ± 82.33 | ||
| p value | 0.930 | 0.453 | ||
| Rathnakumar et al. [22] | ||||
| Men | ||||
| Case | 275 ± 16.58 | 152 ± 12.3 | 38 ± 6.16 | 243 ± 15.58 |
| Control | ||||
| p value | ||||
| Women | ||||
| Case | 363 ± 19.05 | 171 ± 13.07 | 29 ± 5.38 | 328 ± 18.1 |
| Control | ||||
| p value | ||||
| Choi et al. [23] | ||||
| Case | 193.5 ± 35.0 | 112.6 ± 30.8 | 55.5 ± 14.0 | 110 [82, 155] * |
| Control | 192.9 ± 35.6 | 112.7 ± 31.5 | 54.3 ± 13.4 | 115 [82, 159] * |
| p value | 0.698 | 0.946 | 0.050 | 0.397 |
| Shokr et al. [25] | ||||
| Case | 193.35 ± 6.65 | 121.81 ± 8.89 | 46.79 ± 4.22 | 89.38 ± 6.19 |
| Control | 171.69 ± 7.35 | 108.66 ± 8.89 | 61.1 ± 3.48 | 83.19 ± 6.19 |
| p value | 0.036 | 0.301 | 0.014 | 0.502 |
| Choi et al. [26] | ||||
| Case | 188.4 ± 33.0 | |||
| Control | 186.3 ± 36.6 | |||
| p value | 0.532 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, T.-H.; Tsai, Y.-J.; Wang, Y.-H.; Wu, C.-L.; Lin, I.-C. Relationship between Dry Eye Disease and Dyslipidemia: A Systematic Review. J. Clin. Med. 2023, 12, 6631. https://doi.org/10.3390/jcm12206631
Wang T-H, Tsai Y-J, Wang Y-H, Wu C-L, Lin I-C. Relationship between Dry Eye Disease and Dyslipidemia: A Systematic Review. Journal of Clinical Medicine. 2023; 12(20):6631. https://doi.org/10.3390/jcm12206631
Chicago/Turabian StyleWang, Tzu-Hao, Yuan-Jen Tsai, Yuan-Hung Wang, Chien-Liang Wu, and I-Chan Lin. 2023. "Relationship between Dry Eye Disease and Dyslipidemia: A Systematic Review" Journal of Clinical Medicine 12, no. 20: 6631. https://doi.org/10.3390/jcm12206631
APA StyleWang, T.-H., Tsai, Y.-J., Wang, Y.-H., Wu, C.-L., & Lin, I.-C. (2023). Relationship between Dry Eye Disease and Dyslipidemia: A Systematic Review. Journal of Clinical Medicine, 12(20), 6631. https://doi.org/10.3390/jcm12206631