
Radial Artery Deviation and Reimplantation (RADAR) to Accelerate the Maturation of Radial-Cephalic Fistulas for Hemodialysis in Patients with End-Stage Renal Disease
 , , , ,
, , , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Description of Case 1
2.2. Procedure Description in Case 1
2.3. Description of Case 2
2.4. Procedure Description in Case 2
2.5. Description of Case 3
2.6. Procedure Description in Case 3
3. Results
4. Discussion
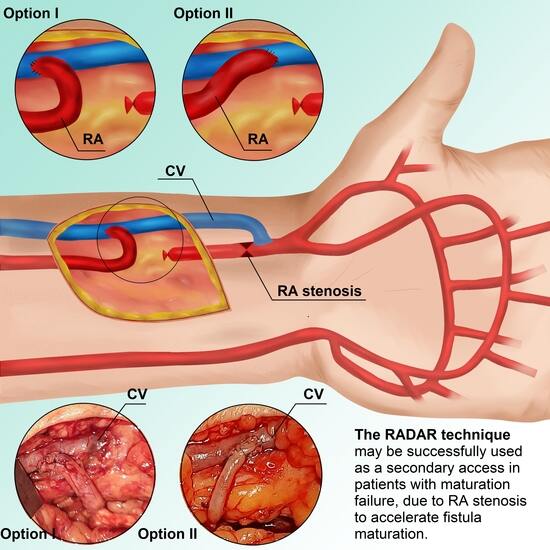
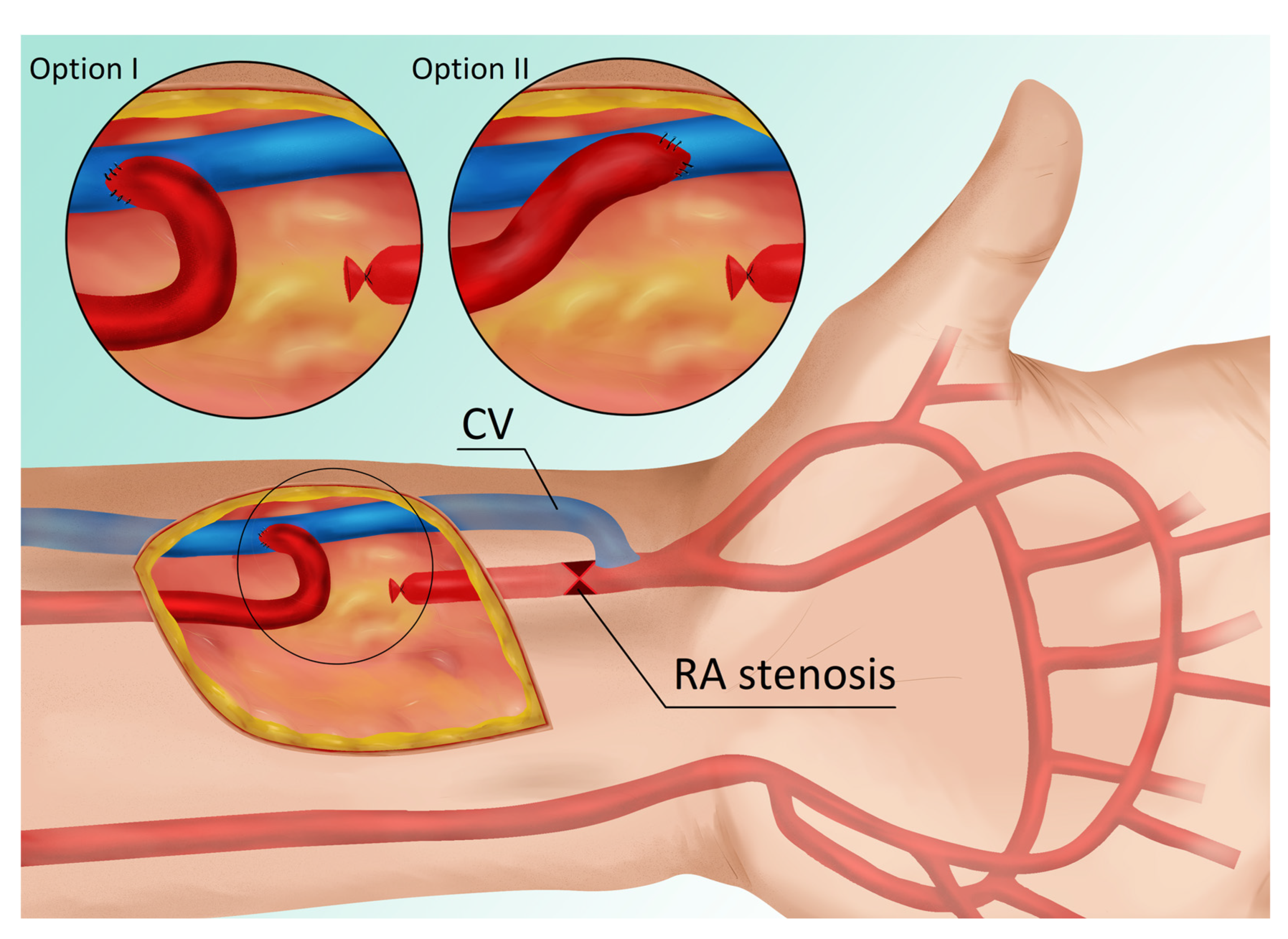
- The primary fistula is not ligated, and the blood flow from the ulnar artery is maintained.
- By connecting the end of the radial artery to the side of the vein, the blood supply to the cephalic vein is increased, thereby accelerating its maturation. In other words, the additional volume of flow from the RA enhances the total fistula blood flow as measured in the brachial artery.
- Increased radial blood flow protects against the development of degenerative changes; consequently, a third fistula can be created proximally between the RA and the CV in cases of AVF thrombosis.
- The risk of hand ischemia is theoretically reduced, as both the UA and the large portion of the RA are patent. The occluded distal part of the RA is bridged by the distal CV (Figure 1). The only limitation is the venous valves, which may impede retrograde flow through the CV. However, this risk is minimal when the venous bridge is not long.
- We have reported RA stenosis resulting from three possible causes of low fistula flow and maturation failure, but this approach can be used for any type of RA stenosis, including changes after the artery has been used as a vascular access in an intensive care unit or in cardiology procedures. In each of these circumstances, a RADAR procedure may be considered.
- We believe this technique allows clinicians to avoid upper fistulas involving the brachial artery and graft-based fistulas.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United States Renal Data System. 2022 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2022. [Google Scholar]
- Gołębiowski, T.; Weyde, W.; Kusztal, M.; Porażko, T.; Augustyniak-Bartosik, H.; Madziarska, K.; Krajewska, M.; Koniński, P.; Sydor, A.; Letachowicz, K.; et al. Vascular access in diabetic patients. Are these patients “difficult”? Postepy Hig. Med. Dosw. 2015, 69, 913–917. [Google Scholar] [CrossRef] [PubMed]
- Rothuizen, T.C.; Wong, C.; Quax, P.H.; van Zonneveld, A.J.; Rabelink, T.J.; Rotmans, J.I. Arteriovenous access failure: More than just intimal hyperplasia? Nephrol. Dial. Transplant. 2013, 28, 1085–1092. [Google Scholar] [CrossRef] [PubMed]
- Röhl, L.; Franz, H.E.; Möhring, K.; Ritz, E.; Schüler, H.W.; Uhse, H.G.; Ziegler, M. Direct arteriovenous fistula for hemodialysis. Scand. J. Urol. Nephrol. 1968, 2, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Tordoir, J.H.M.; Zonnebeld, N.; van Loon, M.M.; Gallieni, M.; Hollenbeck, M. Surgical and Endovascular Intervention for Dialysis Access Maturation Failure During and After Arteriovenous Fistula Surgery: Review of the Evidence. Eur. J. Vasc. Endovasc. Surg. 2018, 55, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Sadaghianloo, N.; Declemy, S.; Jean-Baptiste, E.; Haudebourg, P.; Robino, C.; Islam, M.S.; Hassen-Khodja, R.; Dardik, A. Radial artery deviation and reimplantation inhibits venous juxta-anastomotic stenosis and increases primary patency of radial-cephalic fistulas for hemodialysis. J. Vasc. Surg. 2016, 64, 698–706.e691. [Google Scholar] [CrossRef] [PubMed]
- Jennings, W.C.; Glazer, S.M. Regarding “Radial artery deviation and reimplantation inhibits venous juxta-anastomotic stenosis and increases primary patency of radial-cephalic fistulas for hemodialysis”. J. Vasc. Surg. 2017, 65, 933–934. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RA Before Surgery (mm) | RA Post-Surgery (mm) | UA Before Surgery (mm) | UA Post-Surgery (mm) | BA Before Surgery (mm) | BA Post-Surgery (mm) | CV * Before Surgery (mm) | CV * Post-Surgery (mm) | Fistula Flow Before Surgery (mL/min) | Fistula Flow Post-Surgery (mL/min) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Case 1 | 1.3 | 2 | 4 | 3.8 | 5 | 5.2 | 5.8 | 6 | 264 | 482 |
| Case 2 | 1.9 | 2.1 ** | 2.4 | 2.4 ** | 3.6 | 3.8 ** | 5 | 6.9 ** | 170 | 376 ** |
| Case 3 | 1.6 | 4 | 2.1 | 2 | 3.7 | 4.5 | 6 | 7.8 | 211 | 541 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gołębiowski, T.; Kusztal, M.; Konieczny, A.; Gołębiowski, M.; Letachowicz, K.; Janczak, D.; Krajewska, M. Radial Artery Deviation and Reimplantation (RADAR) to Accelerate the Maturation of Radial-Cephalic Fistulas for Hemodialysis in Patients with End-Stage Renal Disease. J. Clin. Med. 2023, 12, 6481. https://doi.org/10.3390/jcm12206481
Gołębiowski T, Kusztal M, Konieczny A, Gołębiowski M, Letachowicz K, Janczak D, Krajewska M. Radial Artery Deviation and Reimplantation (RADAR) to Accelerate the Maturation of Radial-Cephalic Fistulas for Hemodialysis in Patients with End-Stage Renal Disease. Journal of Clinical Medicine. 2023; 12(20):6481. https://doi.org/10.3390/jcm12206481
Chicago/Turabian StyleGołębiowski, Tomasz, Mariusz Kusztal, Andrzej Konieczny, Maciej Gołębiowski, Krzysztof Letachowicz, Dariusz Janczak, and Magdalena Krajewska. 2023. "Radial Artery Deviation and Reimplantation (RADAR) to Accelerate the Maturation of Radial-Cephalic Fistulas for Hemodialysis in Patients with End-Stage Renal Disease" Journal of Clinical Medicine 12, no. 20: 6481. https://doi.org/10.3390/jcm12206481
APA StyleGołębiowski, T., Kusztal, M., Konieczny, A., Gołębiowski, M., Letachowicz, K., Janczak, D., & Krajewska, M. (2023). Radial Artery Deviation and Reimplantation (RADAR) to Accelerate the Maturation of Radial-Cephalic Fistulas for Hemodialysis in Patients with End-Stage Renal Disease. Journal of Clinical Medicine, 12(20), 6481. https://doi.org/10.3390/jcm12206481