
Ulnar-Sided Sclerosis of the Lunate Does Not Affect Outcomes in Patients Undergoing Volar Locking Plate Fixation for Distal Radius Fracture


Abstract
:1. Introduction
2. Materials and Methods
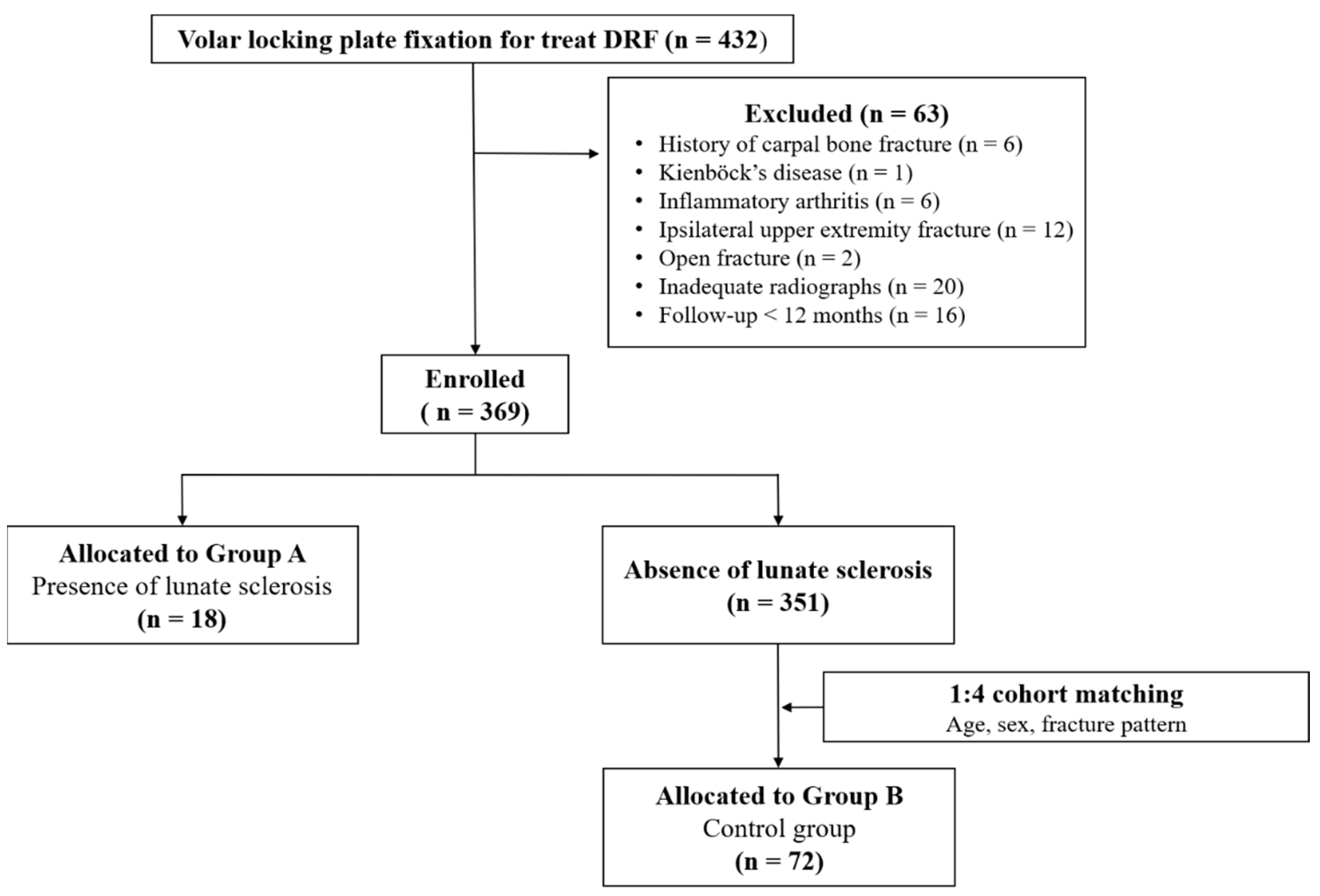
2.1. Study Design and Patient Selection
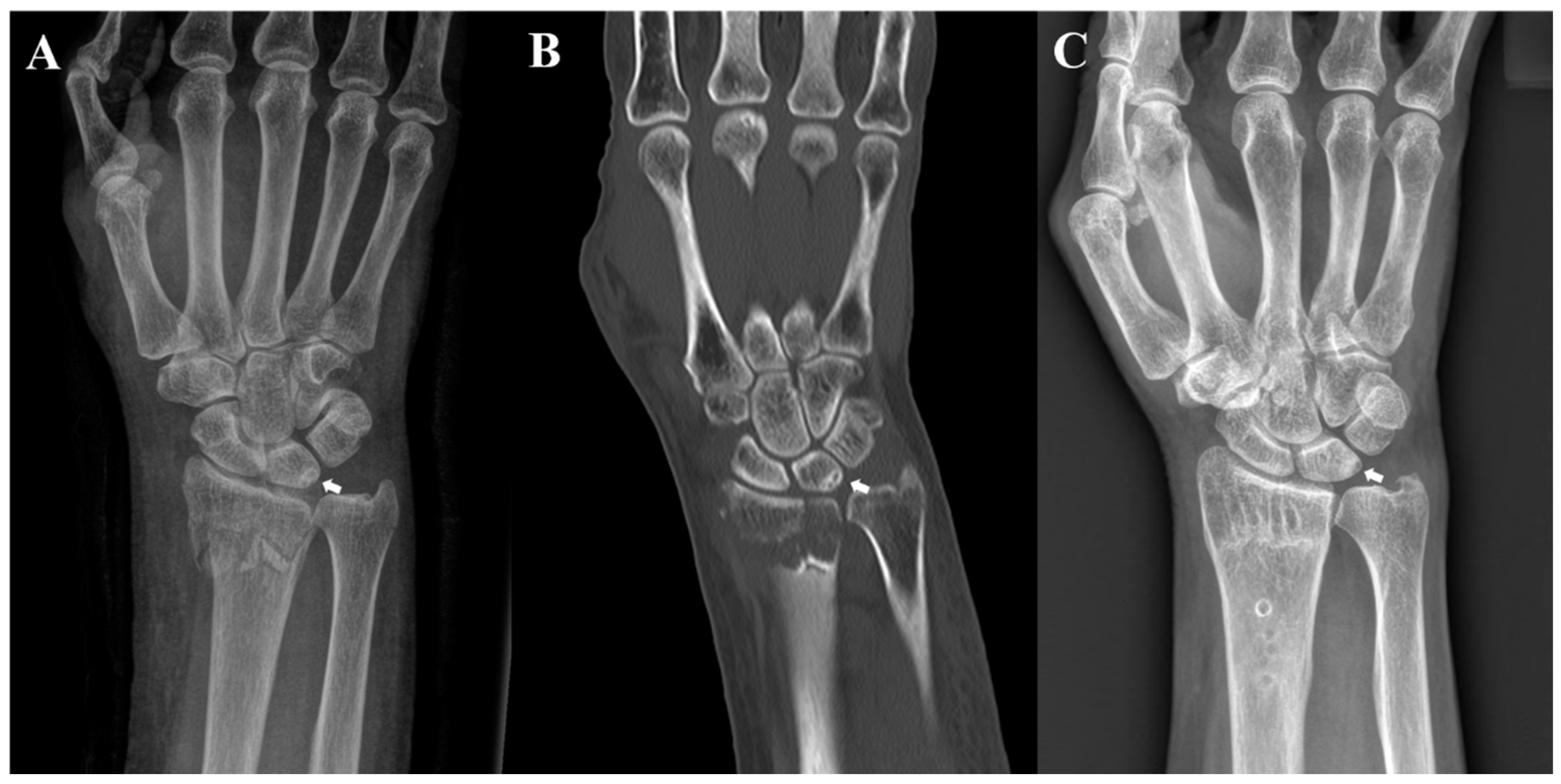
2.2. Cinical and Radiographic Evaluations
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chung, K.C.; Spilson, S.V. The frequency and epidemiology of hand and forearm fractures in the United States. J. Hand Surg. Am. 2001, 26, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Lee, J.K.; Park, J.S.; Kim, D.H.; Baek, J.H.; Kim, Y.J.; Yoon, K.T.; Song, S.H.; Gwak, H.G.; Ha, C.; et al. Complications associated with volar locking plate fixation for distal radius fractures in 1955 cases: A multicentre retrospective study. Int. Orthop. 2020, 44, 2057–2067. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.K.; Kim, D.J.; Yun, Y. Natural history and factors associated with ulnar-sided wrist pain in distal radial fractures treated by plate fixation. J. Hand Surg. Eur. Vol. 2016, 41, 727–731. [Google Scholar] [CrossRef] [PubMed]
- Sachar, K. Ulnar-sided wrist pain: Evaluation and treatment of triangular fibrocartilage complex tears, ulnocarpal impaction syndrome, and lunotriquetral ligament tears. J. Hand Surg. Am. 2012, 37, 1489–1500. [Google Scholar] [CrossRef] [PubMed]
- Stockton, D.J.; Pelletier, M.E.; Pike, J.M. Operative treatment of ulnar impaction syndrome: A systematic review. J. Hand Surg. Eur. Vol. 2015, 40, 470–476. [Google Scholar] [CrossRef]
- Sammer, D.M.; Rizzo, M. Ulnar impaction. Hand Clin. 2010, 26, 549–557. [Google Scholar] [CrossRef]
- Imaeda, T.; Nakamura, R.; Shionoya, K.; Makino, N. Ulnar impaction syndrome: MR imaging findings. Radiology 1996, 201, 495–500. [Google Scholar] [CrossRef]
- Terzis, A.; Koehler, S.; Sebald, J.; Sauerbier, M. Ulnar shortening osteotomy as a treatment of symptomatic ulnar impaction syndrome after malunited distal radius fractures. Arch. Orthop. Trauma Surg. 2020, 140, 681–695. [Google Scholar] [CrossRef]
- Aibinder, W.R.; Izadpanah, A.; Elhassan, B.T. Ulnar Shortening Versus Distal Radius Corrective Osteotomy in the Management of Ulnar Impaction After Distal Radius Malunion. Hand 2018, 13, 194–201. [Google Scholar] [CrossRef]
- Bu, J.; Patterson, R.M.; Morris, R.; Yang, J.; Viegas, S.F. The effect of radial shortening on wrist joint mechanics in cadaver specimens with inherent differences in ulnar variance. J. Hand Surg. Am. 2006, 31, 1594–1600. [Google Scholar] [CrossRef]
- Esenwein, P.; Sonderegger, J.; Gruenert, J.; Ellenrieder, B.; Tawfik, J.; Jakubietz, M. Complications following palmar plate fixation of distal radius fractures: A review of 665 cases. Arch. Orthop. Trauma Surg. 2013, 133, 1155–1162. [Google Scholar] [CrossRef]
- Ma, H.H.; Chen, Y.C.; Huang, H.K.; Huang, Y.C.; Chang, M.C.; Wang, J.P. Comparing radial lengthening osteotomy with ulnar shortening osteotomy to treat ulnar impaction syndrome after distal radius fracture malunion. Arch. Orthop. Trauma Surg. 2022, 142, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Stirling, P.H.C.; Oliver, W.M.; Ng, N.; Oliver, C.W.; McQueen, M.M.; Molyneux, S.G.; Duckworth, A.D. Distal radius malunion: Outcomes following an ulnar shortening osteotomy. Eur. J. Orthop. Surg. Traumatol. 2023, 33, 1635–1640. [Google Scholar] [CrossRef] [PubMed]
- Arora, R.; Lutz, M.; Hennerbichler, A.; Krappinger, D.; Espen, D.; Gabl, M. Complications following internal fixation of unstable distal radius fracture with a palmar locking-plate. J. Orthop. Trauma 2007, 21, 316–322. [Google Scholar] [CrossRef]
- Arora, R.; Lutz, M.; Fritz, D.; Zimmermann, R.; Oberladstatter, J.; Gabl, M. Palmar locking plate for treatment of unstable dorsal dislocated distal radius fractures. Arch. Orthop. Trauma Surg. 2005, 125, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.F.; Chiang, C.C.; Lin, C.C.; Chang, M.C.; Wang, C.S. Loss of radial height in extra-articular distal radial fracture following volar locking plate fixation. Orthop. Traumatol. Surg. Res. 2021, 107, 102842. [Google Scholar] [CrossRef]
- Quadlbauer, S.; Pezzei, C.; Jurkowitsch, J.; Rosenauer, R.; Pichler, A.; Schättin, S.; Hausner, T.; Leixnering, M. Functional and radiological outcome of distal radius fractures stabilized by volar-locking plate with a minimum follow-up of 1 year. Arch. Orthop. Trauma Surg. 2020, 140, 843–852. [Google Scholar] [CrossRef]
- Radius and Ulna. J. Orthop. Trauma 2018, 32, S21–S32. [CrossRef]
- Medoff, R.J. Essential radiographic evaluation for distal radius fractures. Hand Clin. 2005, 21, 279–288. [Google Scholar] [CrossRef]
- Sachar, K. Ulnar-sided wrist pain: Evaluation and treatment of triangular fibrocartilage complex tears, ulnocarpal impaction syndrome, and lunotriquetral ligament tears. J. Hand Surg. Am. 2008, 33, 1669–1679. [Google Scholar] [CrossRef]
- Shin, A.Y.; Deitch, M.A.; Sachar, K.; Boyer, M.I. Ulnar-sided wrist pain: Diagnosis and treatment. Instr. Course Lect. 2005, 54, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Baek, G.H.; Chung, M.S.; Lee, Y.H.; Gong, H.S.; Lee, S.; Kim, H.H. Ulnar shortening osteotomy in idiopathic ulnar impaction syndrome. Surgical technique. J. Bone Jt. Surg. Am. Vol. 2006, 88, 212–220. [Google Scholar] [CrossRef]
- Palmer, A.K.; Werner, F.W. Biomechanics of the distal radioulnar joint. Clin. Orthop. Relat. Res. 1984, 187, 26–35. [Google Scholar] [CrossRef]
- Werner, F.W.; Palmer, A.K.; Fortino, M.D.; Short, W.H. Force transmission through the distal ulna: Effect of ulnar variance, lunate fossa angulation, and radial and palmar tilt of the distal radius. J. Hand Surg. Am. 1992, 17, 423–428. [Google Scholar] [CrossRef]
- Tomaino, M.M. Ulnar impaction syndrome in the ulnar negative and neutral wrist. Diagnosis and pathoanatomy. J. Hand Surg. Br. 1998, 23, 754–757. [Google Scholar] [CrossRef]
- Tatebe, M.; Nakamura, R.; Horii, E.; Nakao, E. Results of ulnar shortening osteotomy for ulnocarpal impaction syndrome in wrists with neutral or negative ulnar variance. J. Hand Surg. Br. 2005, 30, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Rhee, S.M.; Lee, J.Y.; Song, K.S.; Lee, G.Y.; Lee, J.S. Lunate subchondral cysts: Are there specific radiologic findings for patients with symptomatic ulnocarpal impaction? J. Orthop. Sci. 2019, 24, 636–642. [Google Scholar] [CrossRef]
- Cha, S.M.; Shin, H.D.; Kim, K.C. Positive or negative ulnar variance after ulnar shortening for ulnar impaction syndrome: A retrospective study. Clin. Orthop. Surg. 2012, 4, 216–220. [Google Scholar] [CrossRef]
- Ikeda, M.; Oka, Y. Cystic lesion in carpal bone. Hand Surg. 2000, 5, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Yin, J.; Gao, J.; Cheng, T.S.; Pavlos, N.J.; Zhang, C.; Zheng, M.H. Subchondral bone in osteoarthritis: Insight into risk factors and microstructural changes. Arthritis Res. Ther. 2013, 15, 223. [Google Scholar] [CrossRef]
- Ding, M.; Odgaard, A.; Linde, F.; Hvid, I. Age-related variations in the microstructure of human tibial cancellous bone. J. Orthop. Res. 2002, 20, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, H.L.; Selin, G. Tumors of bones and joints. Bull. N. Y Acad. Med. 1951, 27, 165–174. [Google Scholar] [PubMed]
- Eiken, O.; Jonsson, K. Carpal bone cysts: A clinical and radiographic study. Scand. J. Plast. Reconstr. Surg. 1980, 14, 285–290. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Group A † (n = 18) | Group B ‡ (n = 72) | p-Value | |
|---|---|---|---|
| Sex (female, %) | 13 (72.2%) | 48 (66.7%) | 0.652 |
| Age (year) | 67.06 ± 9.01 | 62.10 ± 12.88 | 0.128 |
| Fracture type | 0.894 | ||
| Type A | 1 (5.6%) | 4 (5.6%) | |
| Type B | 4 (22.2%) | 14 (19.4%) | |
| Type C | 13 (72.2%) | 54 (75.0%) | |
| Follow-up period (months) | 17.51 ± 6.62 | 16.32 ± 5.29 | 0.424 |
| Group A † (n = 18) | Group B ‡ (n = 72) | p-Value | Cohen’s d | |
|---|---|---|---|---|
| Ulnar-sided wrist pain (n) | 2 (11.1%) | 3 (4.1%) | ||
| VAS | ||||
| PO 6 months | 0.7 (0–4) | 0.6 (0–3) | 0.672 | 0.102 |
| PO 12 months | 0.5 (0–3) | 0.4 (0–2) | 0.593 | 0.124 |
| DASH | ||||
| PO 6 months | 7.2 (0–25.8) | 7.1 (0–18.5) | 0.795 | 0.03 |
| PO 12 months | 5.6 (0–16.8) | 4.2 (0–11.5) | 0.882 | 0.48 |
| Grip strength(% compared to contra.) | ||||
| PO 6 months | 85.5% (80.5–98.2) | 90.9% (82.3–98.5) | 0.349 | 1.46 |
| PO 12 months | 88.5% (80.2–100) | 92.2% (82.6–100) | 0.687 | 0.9 |
| Group A † (n = 18) | Group B ‡ (n = 72) | p-Value | Cohen’s d | |
|---|---|---|---|---|
| UV at 2 weeks after surgery | 2.0 ± 2.4 | 0.4 ± 2.3 | 0.010 * | 0.690 |
| UV at last follow-up | 2.6 ± 3.0 | 0.6 ± 2.2 | 0.007 * | 0.842 |
| ΔUV (mm) | 0.6 ± 1.2 | 0.5 ± 1.0 | 0.225 | 0.096 |
| RI (°) at last follow-up | 21.7 ± 3.1 | 24.4 ± 3.7 | 0.055 | 0.752 |
| RL (mm) at last follow-up | 10.3 ± 1.6 | 11.4 ± 1.7 | 0.113 | 0.654 |
| VT (°) at last follow-up | 6.6 ± 7.6 | 8.9 ± 6.5 | 0.195 | 0.341 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baek, J.-H.; Lee, J.-H.; Ku, K.-H. Ulnar-Sided Sclerosis of the Lunate Does Not Affect Outcomes in Patients Undergoing Volar Locking Plate Fixation for Distal Radius Fracture. J. Clin. Med. 2023, 12, 6003. https://doi.org/10.3390/jcm12186003
Baek J-H, Lee J-H, Ku K-H. Ulnar-Sided Sclerosis of the Lunate Does Not Affect Outcomes in Patients Undergoing Volar Locking Plate Fixation for Distal Radius Fracture. Journal of Clinical Medicine. 2023; 12(18):6003. https://doi.org/10.3390/jcm12186003
Chicago/Turabian StyleBaek, Jong-Hun, Jae-Hoon Lee, and Ki-Hyeok Ku. 2023. "Ulnar-Sided Sclerosis of the Lunate Does Not Affect Outcomes in Patients Undergoing Volar Locking Plate Fixation for Distal Radius Fracture" Journal of Clinical Medicine 12, no. 18: 6003. https://doi.org/10.3390/jcm12186003
APA StyleBaek, J.-H., Lee, J.-H., & Ku, K.-H. (2023). Ulnar-Sided Sclerosis of the Lunate Does Not Affect Outcomes in Patients Undergoing Volar Locking Plate Fixation for Distal Radius Fracture. Journal of Clinical Medicine, 12(18), 6003. https://doi.org/10.3390/jcm12186003