
Evidence Mapping and Quality Analysis of Systematic Reviews on Various Aspects Related to Cleft Lip and Palate

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
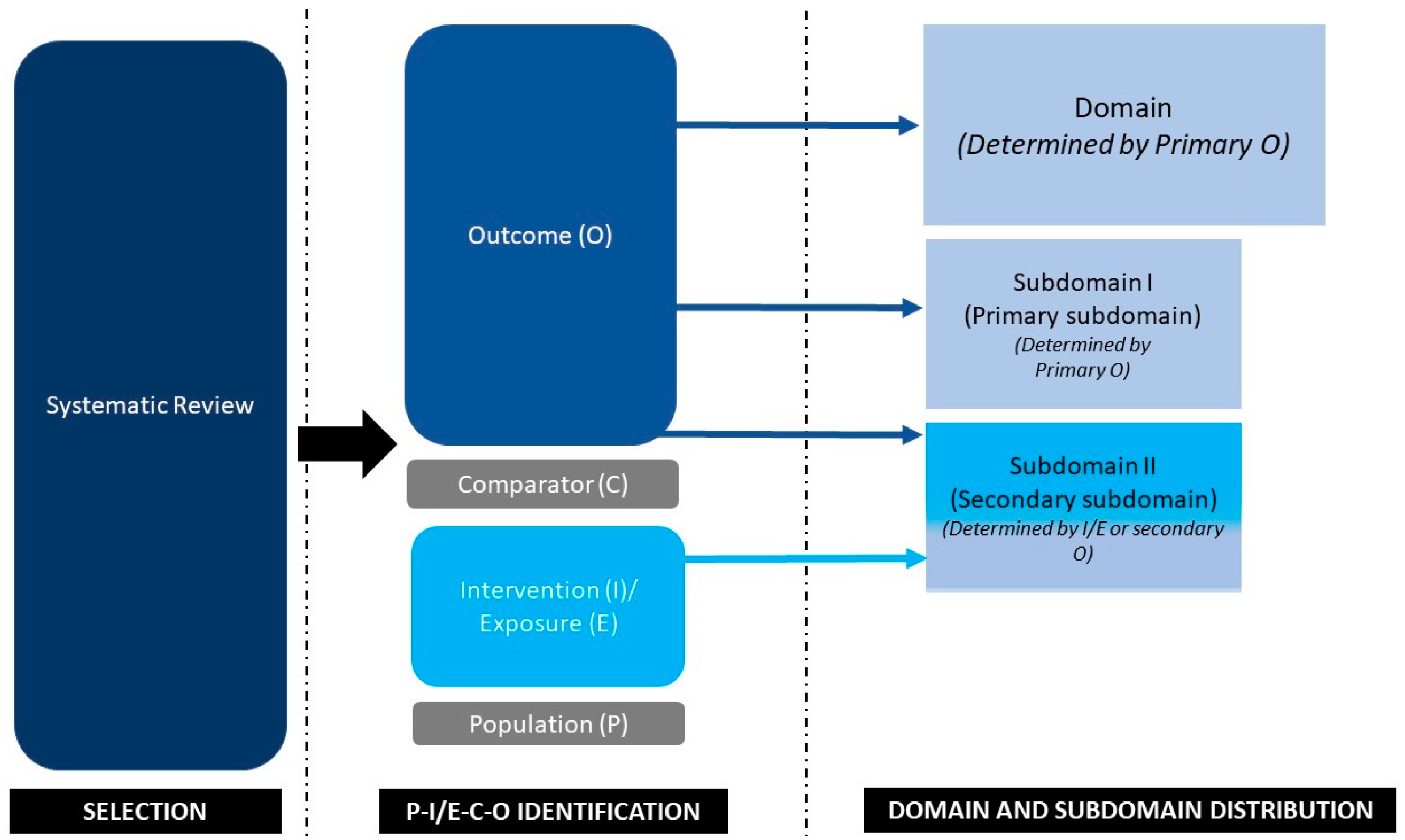
2.1. Establishment of Domains and Subdomains
2.2. Categorization of an Article into Domains and Subdomains
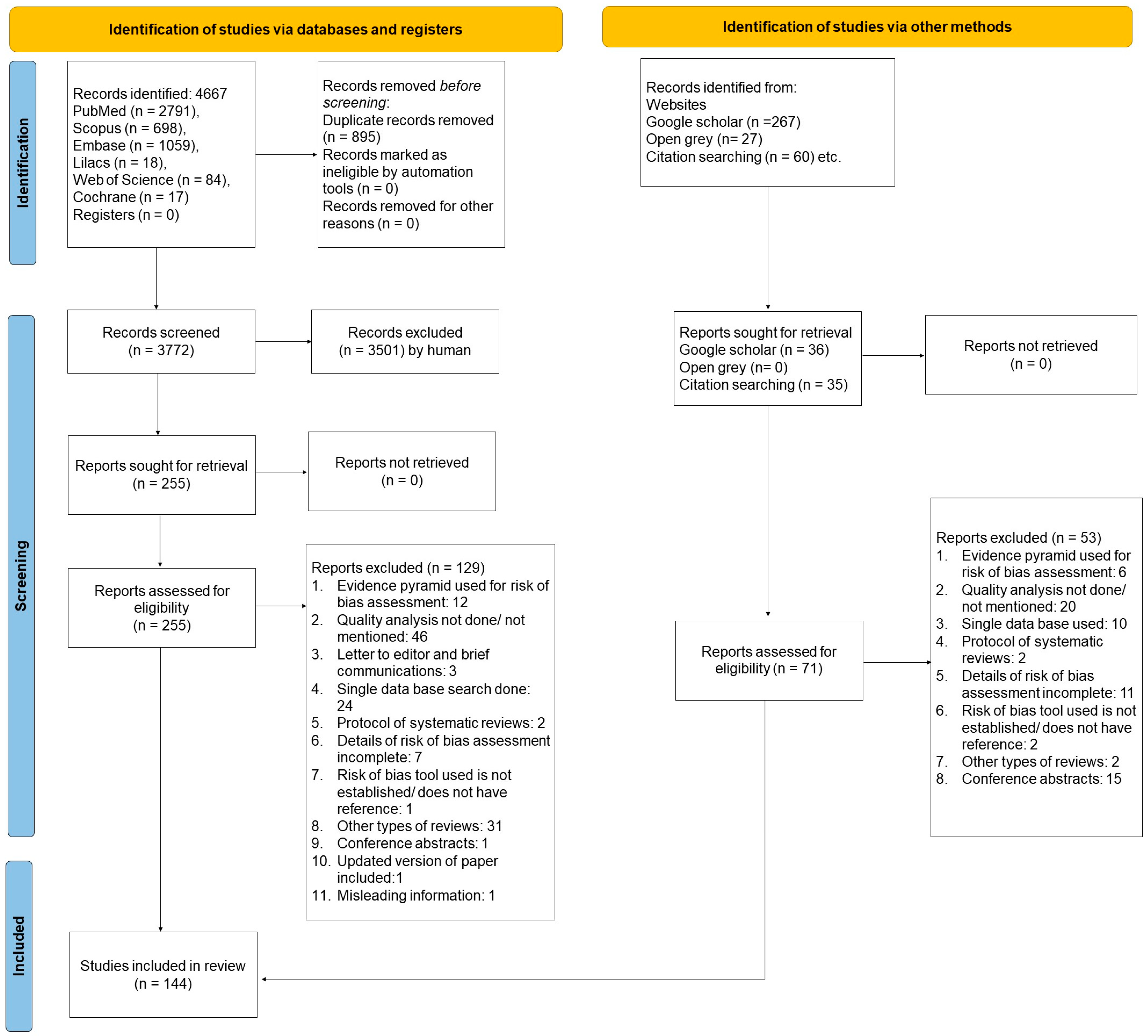
2.3. Search Strategy
2.4. Data Extraction
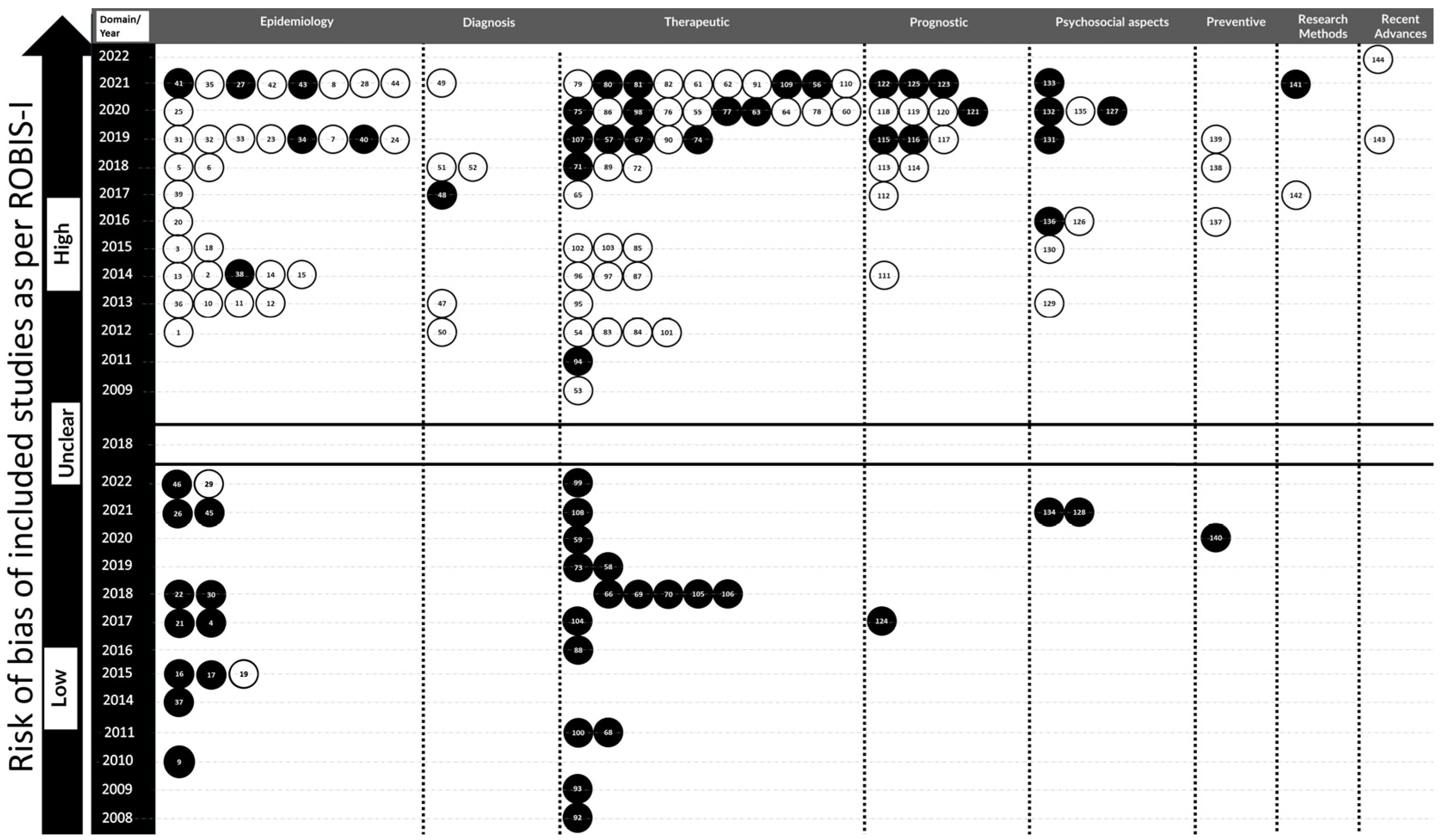
2.5. Quality Analysis and Risk of Bias
2.6. Data Presentation
3. Results
3.1. Characteristics of the Included Studies
3.2. Categorization under Domains and Subdomains
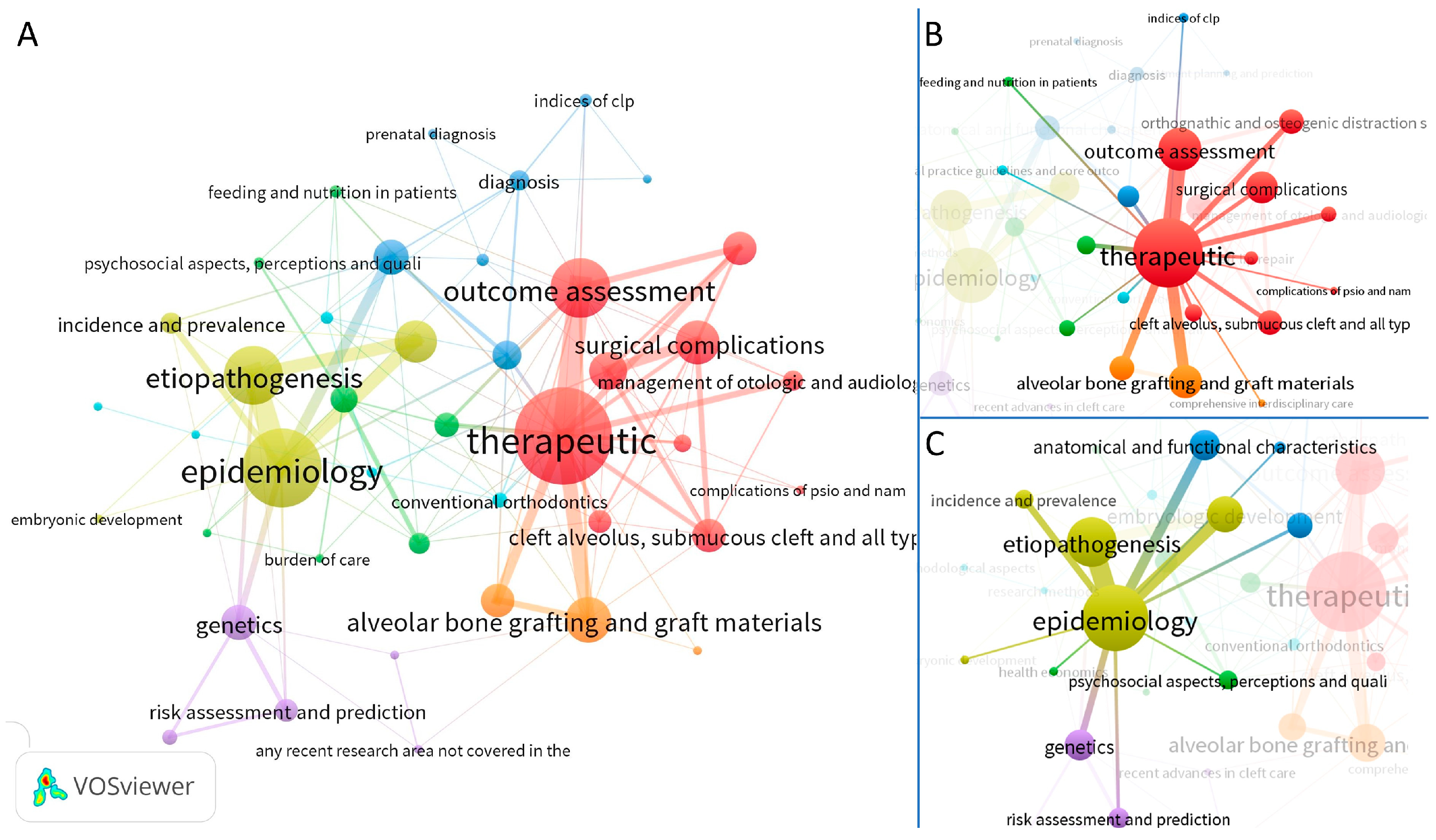
3.3. Co-Occurrence and Link Strength of Domains and Subdomains
3.4. Detailed Description of Studies under the Epidemiologic Domain
3.5. Detailed Description of Studies under the Diagnostic Domain
3.6. Detailed Description of Studies under the Therapeutic Domain
3.7. Detailed Description of Studies under the Prognostic Domain
3.8. Detailed Description of Studies under the Psychosocial Aspects, Perceptions and Quality of Life Domain
3.9. Detailed Description of Studies under the Preventive Domain
3.10. Detailed Description of Studies under the Research Methods Domain
3.11. Detailed Description of Studies under the Recent Advances in the Cleft Care Domain
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Borcbakan, C. An analysis of 1000 cases of cleft lip and palate in Turkey. Cleft Palate J. 1969, 6, 210–212. [Google Scholar]
- Cobourne, M.T. The complex genetics of cleft lip and palate. Eur. J. Orthod. 2004, 26, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A. Linee-guida ed “evidence-based medicine”: L’importanza di distinguerne i ruoli [Guidelines and “evidence-based medicine”: The importance of the role distinction]. Epidemiol. Prev. 1996, 20, 277–278. [Google Scholar] [PubMed]
- Cooper, N.J.; Jones, D.R.; Sutton, A.J. The use of systematic reviews when designing studies. Clin. Trials 2005, 2, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Hopewell, S.; Boutron, I.; Altman, D.G.; Ravaud, P. Deficiencies in the publication and reporting of the results of systematic reviews presented at scientific medical conferences. J. Clin. Epidemiol. 2015, 68, 1488–1495. [Google Scholar] [CrossRef]
- Bragge, P.; Clavisi, O.; Turner, T.; Tavender, E.; Collie, A.; Gruen, R.L. The Global Evidence Mapping Initiative: Scoping research in broad topic areas. BMC Med. Res. Methodol. 2011, 11, 92. [Google Scholar] [CrossRef]
- Madera Anaya, M.; Franco, J.; Ballesteros, M.; Solà, I.; Urrútia Cuchí, G.; Bonfill Cosp, X. Evidence mapping and quality assessment of systematic reviews on therapeutic interventions for oral cancer. Cancer Manag. Res. 2018, 11, 117–130. [Google Scholar] [CrossRef]
- Tewari, N.; Mathur, V.P.; Kaur, A.; Sardana, D.; Rahul, M.; Tamchos, R.; Ritwik, P.; Goel, S.; Schiavo, J. Evidence mapping and quality assessment of systematic reviews in dental traumatology. Dent. Traumatol. Off. Publ. Int. Assoc. Dent. Traumatol. 2021, 37, 17–36. [Google Scholar] [CrossRef]
- Mejàre, I.A.; Klingberg, G.; Mowafi, F.K.; Stecksén-Blicks, C.; Twetman, S.H.; Tranæus, S.H. A systematic map of systematic reviews in pediatric dentistry--what do we really know? PLoS ONE 2015, 10, e0117537. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ (Clin. Res. Ed.) 2009, 339, b2700. [Google Scholar] [CrossRef]
- Alonso, N.; Raposo-Amaral, C.E. (Eds.) Cleft Lip and Palate Treatment: A Comprehensive Guide; Springer: Cham, Switzerland, 2018. [Google Scholar]
- Berkowitz, S. (Ed.) Cleft Lip and Palate; Springer: Berlin/Heidelberg, Germany, 2006. [Google Scholar]
- Cobourne, M.T. (Ed.) Cleft Lip and Palate: Epidemiology, Aetiology, and Treatment; Karger Medical and Scientific Publishers: Basel, Switzerland, 2012; Volume 16. [Google Scholar]
- Katsaros, C. Cleft lip and palate—Epidemiology, aetiology and treatment (Frontiers of oral biology, Vol. 16) (2012). Eur. J. Orthodontics 2013, 35, 275. [Google Scholar] [CrossRef][Green Version]
- Brophy, T.W. Cleft lip and palate. Ann. Surg. 1924, 79, 154–157. [Google Scholar] [CrossRef]
- Losee, J.E.; Kirschner, R.E.; Smith, D.M.; Straub, A.E.; Lawrence, C. (Eds.) Comprehensive Cleft Care: Family Edition; CRC Press/Taylor & Francis Group: Boca Raton, FL, USA, 2015. [Google Scholar]
- Kharbanda, O.P. Cleft Orthodontics, A Holistic and Interdisciplinary Approach; Thieme Publishing Group: New York, NY, USA, 2022. [Google Scholar]
- Whiting, P.; Savović, J.; Higgins, J.P.; Caldwell, D.M.; Reeves, B.C.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J. Clin. Epidemiol. 2016, 69, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Eck, N.J.; Waltman, L. Citation-based clustering of publications using CitNetExplorer and VOSviewer. Scientometrics 2017, 111, 1053–1070. [Google Scholar] [PubMed]
- Tannure, P.N.; Oliveira, C.A.G.; Maia, L.C.; Vieira, A.R.; Granjeiro, J.M.; de Castro Costa, M. Prevalence of dental anomalies in nonsyndromic individuals with cleft lip and palate: A systematic review and meta-analysis. Cleft Palate-Craniofacial J. 2012, 49, 194–200. [Google Scholar] [CrossRef]
- Khalaf, K.; Miskelly, J.; Voge, E.; Macfarlane, T.V. Prevalence of hypodontia and associated factors: A systematic review and meta-analysis. J. Orthod. 2014, 41, 299–316. [Google Scholar] [CrossRef]
- Allagh, K.P.; Shamanna, B.R.; Murthy, G.V.; Ness, A.R.; Doyle, P.; Neogi, S.B.; Pant, H.B.; Wellcome Trust-PHFI Folic Acid Project Team. Birth prevalence of neural tube defects and orofacial clefts in India: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0118961. [Google Scholar] [CrossRef]
- Wang, M.; Yuan, Y.; Wang, Z.; Liu, D.; Wang, Z.; Sun, F.; Wang, P.; Zhu, H.; Li, J.; Wu, T.; et al. Prevalence of Orofacial Clefts among Live Births in China: A Systematic Review and Meta-Analysis. Birth Defects Res. 2017, 109, 1011–1019. [Google Scholar] [CrossRef]
- Chen, L.; Yang, T.; Zheng, Z.; Yu, H.; Wang, H.; Qin, J. Birth prevalence of congenital malformations in singleton pregnancies resulting from in vitro fertilization/intracytoplasmic sperm injection worldwide: A systematic review and meta-analysis. Arch. Gynecol. Obstet. 2018, 297, 1115–1130. [Google Scholar] [CrossRef]
- Haseli, A.; Hajimirzaie, S.; Bagheri, L.; Sadeghian, A.; Ahmadnia, E. Prevalence of cleft lip and cleft palate in Iran: A systematic review and meta-analysis. J. Maz. Univ. Med. Sci. 2019, 28, 185–197. [Google Scholar]
- Pereira, F.D.S.C.F.; Guimarães, R.M.; Lucidi, A.R.; Brum, D.G.; Paiva, C.L.A.; Alvarenga, R.M.P. A systematic literature review on the European, African and Amerindian genetic ancestry components on Brazilian health outcomes. Sci. Rep. 2019, 9, 8874. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Darvishi, N.; Heydari, M.; Bokaee, S.; Darvishi, F.; Mohammadi, M. Global prevalence of cleft palate, cleft lip and cleft palate and lip: A comprehensive systematic review and meta-analysis. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Chi, C.C.; Wang, S.H.; Kirtschig, G.; Wojnarowska, F. Systematic review of the safety of topical corticosteroids in pregnancy. J. Am. Acad. Dermatol. 2010, 62, 694–705. [Google Scholar] [CrossRef]
- Dreier, J.W.; Andersen, A.M.N.; Berg-Beckhoff, G. Systematic review and meta-analyses: Fever in pregnancy and health impacts in the offspring. Pediatrics 2014, 133, e674–e688. [Google Scholar] [CrossRef]
- Molina-Solana, R.; Yáñez-Vico, R.M.; Iglesias-Linares, A.; Mendoza-Mendoza, A.; Solano-Reina, E. Current concepts on the effect of environmental factors on cleft lip and palate. Int. J. Oral Maxillofac. Surg. 2013, 42, 177–184. [Google Scholar] [CrossRef]
- Popoff, D.A.V.; Coelho, M.P.; Martelli, D.R.B.; Saini, R.; Della Coletta, R.; Martelli-Júnior, H. Non-syndromic oral clefts and risk of cancer: A systematic review. Dentistry 3000 2013, 1, 12–18. [Google Scholar] [CrossRef]
- Bell, J.C.; Raynes-Greenow, C.; Turner, R.M.; Bower, C.; Nassar, N.; O’Leary, C.M. Maternal alcohol consumption during pregnancy and the risk of orofacial clefts in infants: A systematic review and meta-analysis. Paediatr. Perinat. Epidemiol. 2014, 28, 322–332. [Google Scholar] [CrossRef]
- Luteijn, J.M.; Brown, M.J.; Dolk, H. Influenza and congenital anomalies: A systematic review and meta-analysis. Hum. Reprod. 2014, 29, 809–823. [Google Scholar] [CrossRef]
- Sabbagh, H.J.; Ahmed Hassan, M.H.; Innes, N.P.; Baik, A.A.; Mossey, P.A. Parental consanguinity and nonsyndromic orofacial clefts in children: A systematic review and meta-analyses. Cleft Palate-Craniofacial J. 2014, 51, 501–513. [Google Scholar] [CrossRef]
- De-Regil, L.M.; Peña-Rosas, J.P.; Fernández-Gaxiola, A.C.; Rayco-Solon, P. Effects and safety of periconceptional oral folate supplementation for preventing birth defects. Cochrane Database Syst. Rev. 2015, 12, CD007950. [Google Scholar] [CrossRef] [PubMed]
- Izedonmwen, O.M.; Cunningham, C.; Macfarlane, T.V. What is the risk of having offspring with cleft lip/palate in pre-maternal obese/overweight women when compared to pre-maternal normal weight women? A systematic review and meta-analysis. J. Oral Maxillofac. Res. 2015, 6, e1. [Google Scholar] [CrossRef] [PubMed]
- Sabbagh, H.J.; Hassan, M.H.A.; Innes, N.P.; Elkodary, H.M.; Little, J.; Mossey, P.A. Passive smoking in the etiology of non-syndromic orofacial clefts: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0116963. [Google Scholar] [CrossRef] [PubMed]
- Tanoshima, M.; Kobayashi, T.; Tanoshima, R.; Beyene, J.; Koren, G.; Ito, S. Risks of congenital malformations in offspring exposed to valproic acid in utero: A systematic review and cumulative meta-analysis. Clin. Pharmacol. Ther. 2015, 98, 417–441. [Google Scholar] [CrossRef]
- Rao, A.; Ahmed, M.K.; Taub, P.J.; Mamoun, J.S. The correlation between maternal exposure to air pollution and the risk of orofacial clefts in infants: A systematic review and meta-analysis. J. Oral Maxillofac. Res. 2016, 7, e2. [Google Scholar] [CrossRef]
- Veroniki, A.A.; Cogo, E.; Rios, P.; Straus, S.E.; Finkelstein, Y.; Kealey, R.; Reynen, E.; Soobiah, C.; Thavorn, K.; Hutton, B.; et al. Comparative safety of anti-epileptic drugs during pregnancy: A systematic review and network meta-analysis of congenital malformations and prenatal outcomes. BMC Med. 2017, 15, 1–20. [Google Scholar] [CrossRef]
- Liang, Y.; Chen, L.; Yu, H.; Wang, H.; Li, Q.; Yu, R.; Qin, J. Which type of congenital malformations is significantly increased in singleton pregnancies following after in vitro fertilization/intracytoplasmic sperm injection: A systematic review and meta-analysis. Oncotarget 2018, 9, 4267. [Google Scholar] [CrossRef]
- Jayarajan, R.; Natarajan, A.; Nagamuttu, R. Efficacy of periconceptional high-dose folic acid in isolated orofacial cleft prevention: A systematic review. Indian J. Plast. Surg. 2019, 52, 153–159. [Google Scholar] [CrossRef]
- Yin, X.; Li, J.; Li, Y.; Zou, S. Maternal alcohol consumption and oral clefts: A meta-analysis. Br. J. Oral Maxillofac. Surg. 2019, 57, 839–846. [Google Scholar] [CrossRef]
- Picot, C.; Berard, A.; Grenet, G.; Ripoche, E.; Cucherat, M.; Cottin, J. Risk of malformation after ondansetron in pregnancy: An updated systematic review and meta-analysis. Birth Defects Res. 2020, 112, 996–1013. [Google Scholar] [CrossRef]
- Fell, M.; Dack, K.; Chummun, S.; Sandy, J.; Wren, Y.; Lewis, S. Maternal cigarette smoking and cleft lip and palate: A systematic review and meta-analysis. Cleft Palate-Craniofacial J. 2022, 59, 1185–1200. [Google Scholar] [CrossRef] [PubMed]
- Kruppa, K.; Krüger, E.; Vorster, C.; der Linde, J.V. Cleft Lip and/or Palate and Associated Risks in Lower-Middle-Income Countries: A Systematic Review. Cleft Palate-Craniofacial J. Off. Publ. Am. Cleft Palate-Craniofacial Assoc. 2022, 59, 568–576. [Google Scholar] [CrossRef] [PubMed]
- Shi, F.P.; Huang, Y.Y.; Dai, Q.Q.; Chen, Y.L.; Jiang, H.Y.; Liang, S.Y. Maternal Common Cold or Fever during Pregnancy and the Risk of Orofacial Clefts in the Offspring: A Systematic Review and Meta-analysis. Cleft Palate-Craniofacial J. Off. Publ. Am. Cleft Palate-Craniofacial Assoc. 2023, 60, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Tran, C.; Crawford, A.A.; Hamilton, A.; French, C.E.; Wren, Y.; Sandy, J.; Sharp, G. Maternal Stressful Life Events During the Periconceptional Period and Orofacial Clefts: A Systematic Review and Meta-Analysis. Cleft Palate-Craniofacial J. Off. Publ. Am. Cleft Palate-Craniofacial Assoc. 2022, 59, 1253–1263. [Google Scholar] [CrossRef]
- Assis Machado, R.; de Toledo, I.P.; Martelli-Júnior, H.; Reis, S.R.; Neves Silva Guerra, E.; Coletta, R.D. Potential genetic markers for nonsyndromic oral clefts in the Brazilian population: A systematic review and meta-analysis. Birth Defects Res. 2018, 110, 827–839. [Google Scholar] [CrossRef]
- Imani, M.M.; Lopez-Jornet, P.; López, E.P.; Ghanbari, F.; Sadeghi, M. Association of Betaine-Homocysteine S-Methyl Transferase (rs3797546 and rs3733890) polymorphisms with non-syndromic cleft lip/palate: A meta-analysis. Int. Orthod. 2019, 17, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Imani, M.M.; Lopez-Jornet, P.; Pons-Fuster López, E.; Sadeghi, M. Polymorphic Variants of V-Maf Musculoaponeurotic Fibrosarcoma Oncogene Homolog B (rs13041247 and rs11696257) and Risk of Non-Syndromic Cleft Lip/Palate: Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 2792. [Google Scholar] [CrossRef] [PubMed]
- Imani, M.M.; Safaei, M.; Lopez-Jornet, P.; Sadeghi, M. A systematic review and meta-analysis on protective role of forkhead box E1 (FOXE1) polymorphisms in susceptibility to non-syndromic cleft lip/palate. Int. Orthod. 2019, 17, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Mendes, S.; Espinosa, D.; Moreira, P.; Marques, D.; Fagundes, N.; Ribeiro-Dos-Santos, Â. miRNAs as biomarkers of orofacial clefts: A systematic review. J. Oral Pathol. Med. Off. Publ. Int. Assoc. Oral Pathol. Am. Acad. Oral Pathol. 2020, 49, 201–209. [Google Scholar] [CrossRef]
- Imani, M.M.; Sadeghi, M.; Tadakamadla, S.K.; Brühl, A.; Sadeghi Bahmani, D.; Taheri, M.; Brand, S. Polymorphisms of ATP-Binding Cassette, Sub-Family A, Member 4 (rs560426 and rs481931) and Non-Syndromic Cleft Lip/Palate: A Meta-Analysis. Life 2021, 11, 58. [Google Scholar] [CrossRef]
- Antonarakis, G.S.; Tsiouli, K.; Christou, P. Mesiodistal tooth size in non-syndromic unilateral cleft lip and palate patients: A meta-analysis. Clin. Oral Investig. 2013, 17, 365–377. [Google Scholar] [CrossRef] [PubMed]
- Berrocal, C.; Terrero-Pérez, Á.; Peralta-Mamani, M.; Fischer Rubira-Bullen, I.R.; Honório, H.M.; de Carvalho, I.; Alvares Capelozza, A.L. Cervical vertebrae anomalies and cleft lip and palate: A systematic review and meta-analysis. Dento Maxillo Facial Radiol. 2019, 48, 20190085. [Google Scholar] [CrossRef] [PubMed]
- Kuijpers, M.A.; Chiu, Y.T.; Nada, R.M.; Carels, C.E.; Fudalej, P.S. Three-dimensional imaging methods for quantitative analysis of facial soft tissues and skeletal morphology in patients with orofacial clefts: A systematic review. PLoS ONE 2014, 9, e93442. [Google Scholar] [CrossRef] [PubMed]
- Boyce, J.O.; Kilpatrick, N.; Morgan, A.T. Speech and language characteristics in individuals with nonsyndromic submucous cleft palate-A systematic review. Child Care Health Dev. 2018, 44, 818–831. [Google Scholar] [CrossRef]
- Van Dyck, J.; Cadenas de Llano-Pérula, M.; Willems, G.; Verdonck, A. Dental development in cleft lip and palate patients: A systematic review. Forensic Sci. Int. 2019, 300, 63–74. [Google Scholar] [CrossRef]
- Gallego Sobrino, R.; Iglesia-Altaba, I.; Moreno-Aznar, L.A.; Rodríguez, G. Long-term growth patterns in children born with cleft lip and/or palate. A systematic review. Patrones de crecimiento a largo plazo en niños nacidos con fisura labial y/o palatina. Una revisión sistemática. Nutr. Hosp. 2021, 38, 410–417. [Google Scholar] [CrossRef]
- Marzouk, T.; Alves, I.L.; Wong, C.L.; DeLucia, L.; McKinney, C.M.; Pendleton, C.; Howe, B.J.; Marazita, M.L.; Peter, T.K.; Kopycka-Kedzierawski, D.T.; et al. Association between Dental Anomalies and Orofacial Clefts: A Meta-analysis. JDR Clin. Transl. Res. 2021, 6, 368–381. [Google Scholar] [CrossRef]
- Murugan, C.; Kailasam, V. Cranial Base Angle in Patients with Cleft Lip and Palate-A Systematic Review and Meta-Analysis. Cleft Palate-Craniofacial J. Off. Publ. Am. Cleft Palate-Craniofacial Assoc. 2023, 60, 39–54. [Google Scholar] [CrossRef]
- Southby, L.; Harding, S.; Phillips, V.; Wren, Y.; Joinson, C. Speech input processing in children born with cleft palate: A systematic literature review with narrative synthesis. Int. J. Lang. Commun. Disord. 2021, 56, 668–693. [Google Scholar] [CrossRef]
- Wu, X.; Kuang, W.; Zheng, J.; Yang, Z.; Ren, M.; Yang, R.; Yuan, W. Skeletal Maturation in Patients with Cleft Lip and/or Palate: A Systematic Review. Cleft Palate-Craniofacial J. Off. Publ. Am. Cleft Palate-Craniofacial Assoc. 2022, 59, 307–319. [Google Scholar] [CrossRef]
- Srivastav, S.; Tewari, N.; Duggal, R.; Goel, S.; Rahul, M.; Mathur, V.P.; Yadav, R.; Upadhyaya, A.D. Cone-Beam Computed Tomographic Assessment of Maxillary Sinus Characteristics in Patients with Cleft Lip and Palate: A Systematic Review and Meta-Analysis. Cleft Palate-Craniofacial J. Off. Publ. Am. Cleft Palate-Craniofacial Assoc. 2023, 60, 742–751. [Google Scholar] [CrossRef] [PubMed]
- Altalibi, M.; Saltaji, H.; Edwards, R.; Major, P.W.; Flores-Mir, C. Indices to assess malocclusions in patients with cleft lip and palate. Eur. J. Orthod. 2013, 35, 772–782. [Google Scholar] [CrossRef] [PubMed]
- Buj-Acosta, C.; Paredes-Gallardo, V.; Montiel-Company, J.M.; Albaladejo, A.; Bellot-Arcís, C. Predictive validity of the GOSLON Yardstick index in patients with unilateral cleft lip and palate: A systematic review. PLoS ONE 2017, 12, e0178497. [Google Scholar] [CrossRef] [PubMed]
- Lai, G.P.; Weng, X.J.; Wang, M.; Tao, Z.F.; Liao, F.H. Diagnostic Accuracy of Prenatal Fetal Ultrasound to Detect Cleft Palate in High-Risk Fetuses: A Systematic Review and Meta-Analysis. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2022, 41, 605–614. [Google Scholar] [CrossRef]
- van Vlijmen, O.J.; Kuijpers, M.A.; Bergé, S.J.; Schols, J.G.; Maal, T.J.; Breuning, H.; Kuijpers-Jagtman, A.M. Evidence supporting the use of cone-beam computed tomography in orthodontics. J. Am. Dent. Assoc. 2012, 143, 241–252. [Google Scholar] [CrossRef]
- Thierens, L.; De Roo, N.; De Pauw, G.; Brusselaers, N. Quantifying Soft Tissue Changes in Cleft Lip and Palate Using Nonionizing Three-Dimensional Imaging: A Systematic Review. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2018, 76, 2210.e1–2210.e13. [Google Scholar] [CrossRef]
- Thierens, L.; De Roo, N.; De Pauw, G.; Brusselaers, N. Assessment modalities of non-ionizing three-dimensional images for the quantification of facial morphology, symmetry, and appearance in cleft lip and palate: A systematic review. Int. J. Oral Maxillofac. Surg. 2018, 47, 1095–1105. [Google Scholar] [CrossRef]
- Mei, C.; Morgan, A.T.; Reilly, S. Benchmarking clinical practice against best evidence: An example from breastfeeding infants with cleft lip and/or palate. Evid. -Based Commun. Assess. Interv. 2009, 3, 48–66. [Google Scholar] [CrossRef]
- van der Heijden, P.; Dijkstra, P.U.; Stellingsma, C.; van der Laan, B.F.; Korsten-Meijer, A.G.; Goorhuis-Brouwer, S.M. Limited evidence for the effect of presurgical nasoalveolar molding in unilateral cleft on nasal symmetry: A call for unified research. Plast. Reconstr. Surg. 2013, 131, 62e–71e. [Google Scholar] [CrossRef]
- Namdar, P.; Lal Alizadeh, F.; Etezadi, T.; Sadri, L.; Shiva, A. Effect of nasoalveolar molding on nasal symmetry in patients with cleft lip and palate: A systematic review. J. Pediatr. Rev. 2020, 8, 79–92. [Google Scholar] [CrossRef]
- Padovano, W.M.; Skolnick, G.B.; Naidoo, S.D.; Snyder-Warwick, A.K.; Patel, K.B. Long-term effects of nasoalveolar molding in patients with unilateral cleft lip and palate: A systematic review and meta-analysis. Cleft Palate-Craniofacial J. 2022, 59, 462–474. [Google Scholar] [CrossRef] [PubMed]
- De Mulder, D.; Cadenas de Llano-Pérula, M.; Jacobs, R.; Verdonck, A.; Willems, G. Three-dimensional radiological evaluation of secondary alveolar bone grafting in cleft lip and palate patients: A systematic review. Dentomaxillofacial Radiol. 2019, 48, 20180047. [Google Scholar] [CrossRef] [PubMed]
- Scalzone, A.; Flores-Mir, C.; Carozza, D.; d’Apuzzo, F.; Grassia, V.; Perillo, L. Secondary alveolar bone grafting using autologous versus alloplastic material in the treatment of cleft lip and palate patients: Systematic review and meta-analysis. Prog. Orthod. 2019, 20, 6. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, F.H.D.S.L.; Drummond, R.J.; Frota, C.M.; Bartzela, T.N.; Dos Santos, P.B. Comparison of early and conventional autogenous secondary alveolar bone graft in children with cleft lip and palate: A systematic review. Orthod. Craniofacial Res. 2020, 23, 385–397. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Guo, R.; Li, W. Comparison of 2-and 3-dimensional radiologic evaluation of secondary alveolar bone grafting of clefts: A systematic review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 130, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Jahanbin, A.; Kamyabnezhad, E.; Raisolsadat, M.A.; Farzanegan, F.; Bardideh, E. Long-Term Stability of Alveolar Bone Graft in Cleft Lip and Palate Patients: Systematic Review and Meta-Analysis. J. Craniofacial Surg. 2022, 33, e194–e200. [Google Scholar] [CrossRef]
- Lacerda-Santos, R.; Batista, R.G.; Neves, S.S.; dos Santos Araújo, J.L.; Vieira, R.A.; de Carvalho, F.G.; Pithon, M.M.; de Castro Martins, C. Effectiveness of secondary alveolar bone graft on canine eruption: Systematic review. Eur. J. Dent. 2021, 15, 579–587. [Google Scholar] [CrossRef]
- Palikaraki, G.; Makrygiannakis, M.A.; Zafeiriadis, A.A.; Benetou, V.; Sanoudos, M.; Bitsanis, I.; Tsolakis, A.I. The effect of facemask in patients with unilateral cleft lip and palate: A systematic review and meta-analysis. Eur. J. Orthod. 2021, 43, 69–79. [Google Scholar] [CrossRef]
- Shafaee, H.; Mazloumhoseini, B.; Bardideh, E.; Dadgarmoghaddam, M. Changes in airway dimensions after face-mask therapy in cleft lip and palate and non-cleft patients: Systematic review and meta-analysis. Iran. J. Orthod. 2020, 15, e113740. [Google Scholar] [CrossRef]
- Thierens, L.A.M.; Brusselaers, N.; De Roo, N.M.C.; De Pauw, G.A.M. Effects of labial adhesion on maxillary arch dimensions and nasolabial esthetics in cleft lip and palate: A systematic review. Oral Dis. 2017, 23, 889–896. [Google Scholar] [CrossRef]
- Jayarajan, R.; Natarajan, A.; Nagamuttu, R. Outcomes of closed versus open technique of rhinoplasty during primary repair of unilateral cleft lip: A systematic review. Cleft Palate-Craniofacial J. 2019, 56, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Salgado, K.R.; Wendt, A.R.; Fagundes, N.C.F.; Maia, L.C.; Normando, D.; Leao, P.B. Early or delayed palatoplasty in complete unilateral cleft lip and palate patients? A systematic review of the effects on maxillary growth. J. Cranio-Maxillofac. Surg. 2019, 47, 1690–1698. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Li, C.; Zhang, Q.; Wu, G.; Deacon, S.A.; Chen, J.; Hu, H.; Zou, S.; Ye, Q. Secondary bone grafting for alveolar cleft in children with cleft lip or cleft lip and palate. Cochrane Database Syst. Rev. 2011, 6, CD008050. [Google Scholar] [CrossRef] [PubMed]
- Canellas, J.V.D.S.; Medeiros, P.J.D.; Figueredo, C.M.D.S.; Fischer, R.G.; Ritto, F.G. Platelet-rich fibrin in oral surgical procedures: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2019, 48, 395–414. [Google Scholar] [CrossRef]
- da Rosa, W.L.D.O.; da Silva, T.M.; Galarça, A.D.; Piva, E.; da Silva, A.F. Efficacy of rhBMP-2 in cleft lip and palate defects: Systematic review and meta-analysis. Calcif. Tissue Int. 2019, 104, 115–129. [Google Scholar] [CrossRef] [PubMed]
- Kamal, M.; Ziyab, A.H.; Bartella, A.; Mitchell, D.; Al-Asfour, A.; Hölzle, F.; Kessler, P.; Lethaus, B. Volumetric comparison of autogenous bone and tissue-engineered bone replacement materials in alveolar cleft repair: A systematic review and meta-analysis. Br. J. Oral Maxillofac. Surg. 2018, 56, 453–462. [Google Scholar] [CrossRef]
- Simpson, A.; Samargandi, O.A.; Wong, A.; Graham, M.E.; Bezuhly, M. Repair of primary cleft palate and oronasal fistula with acellular dermal matrix: A systematic review and surgeon survey. Cleft Palate-Craniofacial J. 2019, 56, 187–195. [Google Scholar] [CrossRef]
- Sales, P.H.H.; Oliveira-Neto, O.B.; Torres, T.S.; de Lima, F.J.C. Effectiveness of dental implants placed in bone graft area of cleft Patients. Int. J. Oral Maxillofac. Surg. 2019, 48, 1109–1114. [Google Scholar] [CrossRef]
- Uribe, F.; Alister, J.P.; Zaror, C.; Olate, S.; Fariña, R. Alveolar cleft reconstruction using morphogenetic protein (rhBMP-2): A systematic review and meta-analysis. Cleft Palate-Craniofacial J. 2020, 57, 589–598. [Google Scholar] [CrossRef]
- Francisco, I.; Fernandes, M.H.; Vale, F. Platelet-rich fibrin in bone regenerative strategies in Orthodontics: A systematic review. Materials 2020, 13, 1866. [Google Scholar] [CrossRef]
- Ma, L.; Hou, Y.; Liu, G.; Zhang, T. Effectiveness of presurgical orthodontics in cleft lip and palate patients with alveolar bone grafting: A systematic review. J. Stomatol. Oral Maxillofac. Surg. 2021, 122, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Osorio, C.C.; Escobar, L.M.; González, M.C.; Gamboa, L.F.; Chambrone, L. Evaluation of density, volume, height and rate of bone resorption of substitutes of autologous bone grafts for the repair of alveolar clefts in humans: A systematic review. Heliyon 2020, 6, e04646. [Google Scholar] [CrossRef] [PubMed]
- Xiao, W.L.; Jia, K.N.; Yu, G.; Zhao, N. Outcomes of bone morphogenetic protein-2 and iliac cancellous bone transplantation on alveolar cleft bone grafting: A meta-analysis. J. Plast. Reconstr. Aesthetic Surg. 2020, 73, 1135–1142. [Google Scholar] [CrossRef] [PubMed]
- Alkaabi, S.A.; Alsabri, G.A.; NatsirKalla, D.S.; Alavi, S.A.; Mueller, W.E.G.; Forouzanfar, T.; Helder, M.N. A systematic review on regenerative alveolar graft materials in clinical trials: Risk of bias and meta-analysis. J. Plast. Reconstr. Aesthetic Surg. 2022, 75, 356–365. [Google Scholar] [CrossRef]
- Carbullido, M.K.; Dean, R.A.; Kamel, G.N.; Davis, G.L.; Hornacek, M.; Segal, R.M.; Gosman, A.A. Long-term treatment outcomes of primary alveolar bone grafts for alveolar clefts: A qualitative systematic review. Cleft Palate-Craniofacial J. 2022, 59, 86–97. [Google Scholar] [CrossRef]
- Chetpakdeechit, W.; Pisek, P.; Pitiphat, W.; Rattanakanokchai, S. Cleft Size and Success of Secondary Alveolar Bone Grafting—A Systematic Review. Cleft Palate-Craniofacial J. 2023, 60, 285–298. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, A.; Hemavathy, O.R.; Krishnan, S. Comparison of Autogenous Iliac Bone Grafting with PRP And Conventional Iliac Bone Grafting in Alveolar Bone Grafting—A Systematic Review. Int. J. Dent. Oral Sci. 2021, 8, 3323–3329. [Google Scholar] [CrossRef]
- Saltaji, H.; Major, M.P.; Alfakir, H.; Al-Saleh, M.A.; Flores-Mir, C. Maxillary advancement with conventional orthognathic surgery in patients with cleft lip and palate: Is it a stable technique? J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2012, 70, 2859–2866. [Google Scholar] [CrossRef]
- Saltaji, H.; Major, M.P.; Altalibi, M.; Youssef, M.; Flores-Mir, C. Long-term skeletal stability after maxillary advancement with distraction osteogenesis in cleft lip and palate patients: A systematic review. Angle Orthod. 2012, 82, 1115–1122. [Google Scholar] [CrossRef]
- Viwattanatipa, N.; Puntien, T.; Nanthavanich, N. Systematic review and meta-analysis: Mandibular plane change after orthognathic surgery and distraction osteogenesis in cleft lip and palate patients. Orthod. Waves 2015, 74, 27–36. [Google Scholar] [CrossRef]
- Jiang, L.; Zheng, Y.; Li, N.; Chen, X.; Lu, Z.; Tong, H.; Tong, H.; Yin, N.; Song, T. Relapse rate after surgical treatment of maxillary hypoplasia in non-growing cleft patients: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2020, 49, 421–431. [Google Scholar] [CrossRef]
- Suresh, S.; Schaldenbrand, K.; Wallis, B.; De Oliveira, G.S., Jr. Regional anaesthesia to improve pain outcomes in paediatric surgical patients: A qualitative systematic review of randomized controlled trials. Br. J. Anaesth. 2014, 113, 375–390. [Google Scholar] [CrossRef] [PubMed]
- Feriani, G.; Hatanaka, E.; Torloni, M.R.; da Silva, E.M. Infraorbital nerve block for postoperative pain following cleft lip repair in children. Cochrane Database Syst. Rev. 2016, 4, CD011131. [Google Scholar] [CrossRef] [PubMed]
- Kendall, M.C.; Alves, L.; Suh, E.I.; McCormick, Z.L.; De Oliveira, G.S. Regional anesthesia to ameliorate postoperative analgesia outcomes in pediatric surgical patients: An updated systematic review of randomized controlled trials. Local Reg. Anesth. 2018, 11, 91–109. [Google Scholar] [CrossRef]
- Tache, A.; Mommaerts, M.Y. Pain management at iliac donor sites after grafting of alveolar clefts. Int. J. Oral Maxillofac. Surg. 2022, 51, 62–69. [Google Scholar] [CrossRef]
- Liu, D.; Pan, L.; Gao, Y.; Liu, J.; Li, F.; Li, X.; Quan, J.; Huang, C.; Lian, C. Efficaciousness of dexmedetomidine in children undergoing cleft lip and palate repair: A systematic review and meta-analysis. BMJ Open 2021, 11, e046798. [Google Scholar] [CrossRef]
- Nasser, M.; Fedorowicz, Z.; Newton, J.T.; Nouri, M. Interventions for the management of submucous cleft palate. Cochrane Database Syst. Rev. 2008, 1, CD006703. [Google Scholar] [CrossRef]
- Lee, A.S.; Law, J.; Gibbon, F.E. Electropalatography for articulation disorders associated with cleft palate. Cochrane Database Syst. Rev. 2009, 3, CD006854. [Google Scholar] [CrossRef] [PubMed]
- Meinusch, M.; Romonath, R. Early language intervention for children with cleft lip and/or palate: A systematic review. Evid.-Based Commun. Assess. Interv. 2011, 5, 197–215. [Google Scholar] [CrossRef]
- Bessell, A.; Sell, D.; Whiting, P.; Roulstone, S.; Albery, L.; Persson, M.; Varhoeven, A.; Burke, M.; Ness, A.R. Speech and language therapy interventions for children with cleft palate: A systematic review. Cleft Palate-Craniofacial J. 2013, 50, 1–17. [Google Scholar] [CrossRef]
- Gilleard, O.; Sell, D.; Ghanem, A.M.; Tavsanoglu, Y.; Birch, M.; Sommerlad, B. Submucous cleft palate: A systematic review of surgical management based on perceptual and instrumental analysis. Cleft Palate-Craniofacial J. 2014, 51, 686–695. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.L.; Tsao, Y.H.; Cheng, H.M.; Lien, C.F.; Hsu, C.H.; Huang, C.Y.; Shiao, A.S. Grommets for otitis media with effusion in children with cleft palate: A systematic review. Pediatrics 2014, 134, 983–994. [Google Scholar] [CrossRef] [PubMed]
- Lane, H.; Harding, S.; Wren, Y. A systematic review of early speech interventions for children with cleft palate. Int. J. Lang. Commun. Disord. 2022, 57, 226–245. [Google Scholar] [CrossRef]
- Sand, A.; Hagberg, E.; Lohmander, A. On the Benefits of Speech-Language Therapy for Individuals Born with Cleft Palate: A Systematic Review and Meta-Analysis of Individual Participant Data. J. Speech Lang. Hear. Res. JSLHR 2022, 65, 555–573. [Google Scholar] [CrossRef] [PubMed]
- Bessell, A.; Hooper, L.; Shaw, W.C.; Reilly, S.; Reid, J.; Glenny, A.M. Feeding interventions for growth and development in infants with cleft lip, cleft palate or cleft lip and palate. Cochrane Database Syst. Rev. 2011, 2011, CD003315. [Google Scholar] [CrossRef] [PubMed]
- Sharshar, H.H.; El-Bialy, T.H. Cephalometric evaluation of airways after maxillary anterior advancement by distraction osteogenesis in cleft lip and palate patients: A systematic review. Cleft Palate-Craniofacial J. Off. Publ. Am. Cleft Palate-Craniofacial Assoc. 2012, 49, 255–261. [Google Scholar] [CrossRef]
- Austin, S.L.; Mattick, C.R.; Waterhouse, P.J. Distraction osteogenesis versus orthognathic surgery for the treatment of maxillary hypoplasia in cleft lip and palate patients: A systematic review. Orthod. Craniofacial Res. 2015, 18, 96–108. [Google Scholar] [CrossRef]
- Norman, A.; Persson, M.; Stock, N.; Rumsey, N.; Sandy, J.; Waylen, A.; Edwards, Z.; Hammond, V.; Partridge, L.; Ness, A. The Effectiveness of Psychosocial Intervention for Individuals with Cleft Lip and/or Palate. Cleft Palate-Craniofacial J. Off. Publ. Am. Cleft Palate-Craniofacial Assoc. 2015, 52, 301–310. [Google Scholar] [CrossRef]
- Hosseini, H.R.; Kaklamanos, E.G.; Athanasiou, A.E. Treatment outcomes of pre-surgical infant orthopedics in patients with non-syndromic cleft lip and/or palate: A systematic review and meta-analysis of randomized controlled trials. PLoS ONE 2017, 12, e0181768. [Google Scholar] [CrossRef]
- El-Ashmawi, N.A.; ElKordy, S.A.; Salah Fayed, M.M.; El-Beialy, A.; Attia, K.H. Effectiveness of Gingivoperiosteoplasty on Alveolar Bone Reconstruction and Facial Growth in Patients with Cleft Lip and Palate: A Systematic Review and Meta-Analysis. Cleft Palate-Craniofacial J. Off. Publ. Am. Cleft Palate-Craniofacial Assoc. 2019, 56, 438–453. [Google Scholar] [CrossRef]
- Kloukos, D.; Fudalej, P.; Sequeira-Byron, P.; Katsaros, C. Maxillary distraction osteogenesis versus orthognathic surgery for cleft lip and palate patients. Cochrane Database Syst. Rev. 2018, 8, CD010403. [Google Scholar] [CrossRef] [PubMed]
- Awarun, B.; Blok, J.; Pauwels, R.; Politis, C.; Jacobs, R. Three-dimensional imaging methods to quantify soft and hard tissues change after cleft-related treatment during growth in patients with cleft lip and/or cleft palate: A systematic review. Dento Maxillo Facial Radiol. 2019, 48, 20180084. [Google Scholar] [CrossRef] [PubMed]
- Kuang, W.; Aarts, M.; Kuijpers-Jagtman, A.M.; He, H.; Ongkosuwito, E.M. Treatment Outcome in Bilateral Cleft lip and Palate Patients Evaluated with the Huddart-Bodenham Scoring System and the Bilateral Cleft lip and Palate Yardstick: A Systematic Review. Cleft Palate-Craniofacial J. Off. Publ. Am. Cleft Palate-Craniofacial Assoc. 2022, 59, 1377–1390. [Google Scholar] [CrossRef] [PubMed]
- Nimbalkar, K.A.; Datana, S.; Agarwal, S.S.; Chopra, S.S.; Bhandari, S.K. Comparison of long-term skeletal stability following maxillary advancement using rigid external distraction in growing and non-growing patients with cleft lip and palate: A systematic review and meta-analysis. Eur. J. Orthod. 2022, 44, 22–29. [Google Scholar] [CrossRef]
- Sazo, J.S.; Molina, R.T.; Fierro-Monti, C.; Pérez-Flores, A. Presurgical orthopedics in patients with cleft lip and palate: Nutrition, aesthetics and gap between maxillary segments. A systematic review. Odontoestomatología 2021, 23, e303. [Google Scholar]
- Hardwicke, J.T.; Landini, G.; Richard, B.M. Fistula incidence after primary cleft palate repair: A systematic review of the literature. Plast. Reconstr. Surg. 2014, 134, 618e–627e. [Google Scholar] [CrossRef]
- Felton, M.; Lee, J.W.; Balumuka, D.D.; Arneja, J.S.; Chadha, N.K. Early placement of ventilation tubes in infants with cleft lip and palate: A systematic review. Otolaryngol.—Head Neck Surg. 2018, 158, 459–464. [Google Scholar] [CrossRef]
- Kappen, I.F.; Yoder, W.R.; van der Molen, A.B.M.; Breugem, C.C. Long-term craniofacial morphology in young adults treated for a non-syndromal UCLP: A systematic review. J. Plast. Reconstr. Aesthetic Surg. 2018, 71, 504–517. [Google Scholar] [CrossRef]
- Liu, K.; Zhou, N. Long-term skeletal changes after maxillary distraction osteogenesis in growing children with cleft lip/palate. J. Craniofacial Surg. 2018, 29, e349–e352. [Google Scholar] [CrossRef]
- dos Santos Alves, J.M.; de Freitas Alves, B.W.; de Figueiredo Costa, A.C.; Carneiro, B.G.D.S.; de Sousa, L.M.; Gondim, D.V. Cranial nerve injuries in Le Fort I osteotomy: A systematic review. Int. J. Oral Maxillofac. Surg. 2019, 48, 601–611. [Google Scholar] [CrossRef]
- Minatel, L.; de Luna Gomes, J.M.; Lemos, C.A.A.; de Oliveira Limírio, J.P.J.; Pellizzer, E.P. Influence of vomer flap on craniofacial growth in patients with cleft lip and palate: A systematic review. J. Cranio-Maxillofac. Surg. 2019, 47, 902–908. [Google Scholar] [CrossRef]
- Tache, A.; Mommaerts, M.Y. On the frequency of oronasal fistulation after primary cleft palate repair. Cleft Palate-Craniofacial J. 2019, 56, 1302–1313. [Google Scholar] [CrossRef] [PubMed]
- Corthouts, P.; Boels, F.; Van de Casteele, E.; Nadjmi, N. Effects of various surgical protocols on maxillofacial growth in patients with unilateral cleft lip and palate: A systematic review. Plast. Aesthetic Res. 2020, 7, 46. [Google Scholar] [CrossRef]
- Miranda, B.L.; de Araújo Júnior, J.L.; de Paiva, M.A.F.; Lacerda, R.H.W.; Vieira, A.R. Management of oronasal fistulas in patients with cleft lip and palate. J. Craniofacial Surg. 2020, 31, 1526–1528. [Google Scholar] [CrossRef]
- Vandenberg, K.; Castle, M.; Qeadan, F.; Kraai, T. Oronasal fistula incidence associated with vomer flap repair of cleft palate: A systematic review and meta-analysis. Cleft Palate-Craniofacial J. 2021, 58, 957–965. [Google Scholar] [CrossRef] [PubMed]
- Velasques, B.D.; Moura, L.B.; Martins, J.R.; Damian, M.F.; Xavier, C.B. What is the relapse after Le Fort I maxillary advancement in cleft lip and palate patients? A systematic review. Oral Maxillofac. Surg. 2021, 25, 139–148. [Google Scholar] [CrossRef]
- Egbunah, U.P.; Adamson, O.; Fashina, A.; Adekunle, A.A.; James, O.; Adeyemo, W.L. Comparing the Treatment Outcomes of Absorbable Sutures, Nonabsorbable Sutures, and Tissue Adhesives in Cleft Lip Repair: A Systematic Review. Cleft Palate-Craniofacial J. 2022, 59, 110–120. [Google Scholar] [CrossRef]
- Valls-Ontañón, A.; Fernandes-Ciaccia, L.; Haas-Junior, O.L.; Hernández-Alfaro, F. Relapse-related factors of Le Fort I osteotomy in cleft lip and palate patients: A systematic review and meta-analysis. J. Cranio-Maxillofac. Surg. 2021, 49, 879–890. [Google Scholar] [CrossRef]
- Worth, V.; Perry, R.; Ireland, T.; Wills, A.K.; Sandy, J.; Ness, A. Are people with an orofacial cleft at a higher risk of dental caries? A systematic review and meta-analysis. Br. Dent. J. 2017, 223, 37–47. [Google Scholar] [CrossRef]
- Vale, F.; Correia, L.; Guimarães, A.; Caramelo, F.; Francisco, I. Salivary counts of Streptococcus mutans and Lactobacillus in patients with and without cleft lip and/or palate undergoing orthodontic treatment: A meta-analysis. Int. J. Dent. Hyg. 2022, 20, 112–119. [Google Scholar] [CrossRef]
- Zhu, S.; Jayaraman, J.; Khambay, B. Evaluation of facial appearance in patients with cleft lip and palate by laypeople and professionals: A systematic literature review. Cleft Palate-Craniofacial J. 2016, 53, 187–196. [Google Scholar] [CrossRef]
- Abd El-Ghafour, M.; Elkordy, S.A.; Fayed, M.M.S.; El-Beialy, A.R.; Eid, F.H.K. Parents’ Acceptance to Alveolar and Nasoalveolar Molding Appliances during Early Cleft Lip and Palate Care: A Call for High-Quality Research. Open Access Maced. J. Med. Sci. 2020, 8, 58–64. [Google Scholar] [CrossRef]
- Srivastav, S.; Duggal, I.; Duggal, R.; Tewari, N.; Chaudhari, P.K.; Pandey, R.M. Parental response to the feeding behavior problems in children with cleft lip and palate: A systematic review. Spec. Care Dent. 2021, 41, 559–571. [Google Scholar] [CrossRef] [PubMed]
- Antonarakis, G.S.; Patel, R.N.; Tompson, B. Oral health-related quality of life in non-syndromic cleft lip and/or palate patients: A systematic review. Community Dent. Health 2013, 30, 189–195. [Google Scholar] [PubMed]
- De Queiroz Herkrath, A.P.C.; Herkrath, F.J.; Rebelo, M.A.B.; Vettore, M.V. Measurement of health-related and oral health–related quality of life among individuals with nonsyndromic orofacial clefts: A systematic review and meta-analysis. Cleft Palate-Craniofacial J. 2015, 52, 157–172. [Google Scholar] [CrossRef]
- Chung, K.Y.; Sorouri, K.; Wang, L.; Suryavanshi, T.; Fisher, D. The impact of social stigma for children with cleft lip and/or palate in low-resource areas: A systematic review. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2487. [Google Scholar] [CrossRef]
- Acum, M.; Mastroyannopoulou, K.; O’Curry, S.; Young, J. The psychosocial patient-reported outcomes of end of pathway cleft surgery: A systematic review. Cleft Palate-Craniofacial J. 2020, 57, 990–1007. [Google Scholar] [CrossRef]
- Glinianaia, S.V.; McLean, A.; Moffat, M.; Shenfine, R.; Armaroli, A.; Rankin, J. Academic achievement and needs of school-aged children born with selected congenital anomalies: A systematic review and meta-analysis. Birth Defects Res. 2021, 113, 1431–1462. [Google Scholar] [CrossRef]
- Nascimento, V.D.C.; Martins, M.M.E.; Vilella, B.D.S.; Mattos, C.T.; Vilella, O.D.V. Influence of clinical and demographic factors on the oral health-related quality of life of patients with cleft lip and palate undergoing orthodontic treatment: A systematic review and meta-analysis. Eur. J. Orthod. 2022, 44, 268–278. [Google Scholar] [CrossRef]
- Alfonso, A.R.; Ramly, E.P.; Kantar, R.S.; Wang, M.M.; Eisemann, B.S.; Staffenberg, D.A.; Shetye, P.R.; Flores, R.L. What is the burden of care of nasoalveolar molding? Cleft Palate-Craniofacial J. 2020, 57, 1078–1092. [Google Scholar] [CrossRef]
- Saxton, A.T.; Poenaru, D.; Ozgediz, D.; Ameh, E.A.; Farmer, D.; Smith, E.R.; Rice, H.E. Economic analysis of children’s surgical care in low-and middle-income countries: A systematic review and analysis. PLoS ONE 2016, 11, e0165480. [Google Scholar] [CrossRef]
- Zhao, H.; Zhang, J.; Zhang, M.; Deng, F.; Zheng, L.; Zheng, H.; Chen, F.; Lin, J. Is MTHFD1 polymorphism rs 2236225 (c. 1958G> A) associated with the susceptibility of NSCL/P? A systematic review and meta-analysis. F1000Research 2015, 4, 142. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.Q.; Gao, S.T.; Chen, K.; Xu, Z.Q.; Sun, J.M.; Xia, Y.; Lv, Z.T. Association of the WNT3 polymorphisms and non-syndromic cleft lip with or without cleft palate: Evidence from a meta-analysis. Biosci. Rep. 2018, 38, BSR20181676. [Google Scholar] [CrossRef] [PubMed]
- Shu, X.; Shu, S.; Yang, L. Association between methylenetetrahydrofolate reductase polymorphisms and non-syndromic cleft lip with or without palate susceptibility: An updated systematic review and meta-analysis. Br. J. Oral Maxillofac. Surg. 2019, 57, 819–830. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Sinnathamby, V.; Yu, Y.; Sikora, L.; Johnson, C.Y.; Mossey, P.; Little, J. Folate intake, markers of folate status and oral clefts: An updated set of systematic reviews and meta-analyses. Birth Defects Res. 2020, 112, 1699–1719. [Google Scholar] [CrossRef] [PubMed]
- Saikia, A.; Muthu, M.S.; Orenuga, O.O.; Mossey, P.; Ousehal, L.; Yan, S.; Compodonico, M.; England, R.; Taylor, S.; Sheeran, P. Systematic review of clinical practice guidelines for oral health in children with cleft lip and palate. Cleft Palate-Craniofacial J. 2022, 59, 800–814. [Google Scholar] [CrossRef]
- Hardwicke, J.; Nassimizadeh, M.; Richard, B. Reporting of randomized controlled trials in cleft lip and palate: A 10-year review. Cleft Palate-Craniofacial J. 2017, 54, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Shanbhag, S.; Suliman, S.; Pandis, N.; Stavropoulos, A.; Sanz, M.; Mustafa, K. Cell therapy for orofacial bone regeneration: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46, 162–182. [Google Scholar] [CrossRef]
- Wei, Y.; Tian, Y.; Yu, X.; Miao, Z.; Xu, Y.; Pan, Y. Advances in research regarding the roles of non-coding RNAs in non-syndromic cleft lip with or without cleft palate: A systematic review. Arch. Oral Biol. 2022, 134, 105319. [Google Scholar] [CrossRef]
- Wormald, R.; Evans, J. What makes systematic reviews systematic and why are they the highest level of evidence? Ophthalmic Epidemiol. 2018, 25, 27–30. [Google Scholar] [CrossRef]
- Dixon, M.J.; Marazita, M.L.; Beaty, T.H.; Murray, J.C. Cleft lip and palate: Understanding genetic and environmental influences. Nature reviews. Genetics 2011, 12, 167–178. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Domains and Subdomains Related to Cleft Lip and Palate | |||
|---|---|---|---|
| Code | Domain | Code | Subdomain |
| A | Epidemiologic | A1 | Incidence and prevalence |
| A2 | Etiopathogenesis | ||
| A3 | Embryologic development | ||
| A4 | Genetics | ||
| A5 | Syndromes and anomalies of head and neck in relation to CLP | ||
| A6 | Anatomical and functional characteristics | ||
| B | Diagnostic | B1 | Classifications |
| B2 | Indices of CLP | ||
| B3 | Prenatal diagnosis | ||
| B4 | Clinical diagnostic methods | ||
| B5 | Conventional radiography and 2D imaging | ||
| B6 | Advanced radiography including 3D imaging and 3D printing | ||
| B7 | Photography and records | ||
| C | Therapeutic | C1 | Treatment planning and prediction |
| C2 | Feeding and nutrition in patients | ||
| C3 | Presurgical infant orthopedics (PSIO) and naso-alveolar molding (PNAM) | ||
| C4 | Early orthodontics | ||
| C5 | Orthodontic and surgical perspectives of secondary alveolar bone grafting | ||
| C6 | Conventional orthodontics | ||
| C7 | Late and retreatment adult orthodontics | ||
| C8 | Cleft lip repair | ||
| C9 | Cleft alveolus, submucous cleft, and all types of cleft palate closure/repair | ||
| C10 | Alveolar bone grafting and graft materials | ||
| C11 | Orthognathic and osteogenic distraction surgical orthodontics | ||
| C12 | Other surgical aspects of cleft lip and palate including revisions, scar management, post-operative pain, and anesthesia | ||
| C13 | Comprehensive interdisciplinary care | ||
| C14 | Management of speech and hearing problems | ||
| C15 | Outcome assessment | ||
| D | Prognostic | D1 | Effects/complications of untreated CLP |
| D2 | Effects/complications of PSIO and PNAM | ||
| D3 | Effects/complications of orthodontic treatment | ||
| D4 | Effects/complications of surgical treatment and/or alveolar bone grafting | ||
| D5 | Obstructive sleep apnea | ||
| D6 | Oral health aspects including dental caries and other dental problems | ||
| D7 | Systemic problems | ||
| E | Psychosocial aspects, perceptions and quality of life | E1 | Psychosocial aspects, perceptions and quality of life of family members of the patients with CLP, lay people, and healthcare professionals |
| E2 | Psychosocial aspects, perceptions and quality of life of patients with CLP | ||
| E3 | Burden of care | ||
| E4 | Health economics | ||
| E5 | Support groups and charity associations | ||
| F | Preventive | F1 | Genetic counselling |
| F2 | Risk assessment and prediction | ||
| F3 | Public awareness | ||
| F4 | Patient awareness | ||
| F5 | Awareness of medical and dental specialists | ||
| G | Research methods | G1 | Clinical practice guidelines and core outcome sets |
| G2 | Ethical aspects of research | ||
| G3 | Methodological aspects | ||
| H | Recent advances in cleft care | H1 | Any recent research area not covered in the above categorization |
| I | Others | I1 | Any area not covered in above categorization |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Srivastav, S.; Tewari, N.; Antonarakis, G.S.; Duggal, R.; Saji, S.; Lokade, A.K.; Yadav, R. Evidence Mapping and Quality Analysis of Systematic Reviews on Various Aspects Related to Cleft Lip and Palate. J. Clin. Med. 2023, 12, 6002. https://doi.org/10.3390/jcm12186002
Srivastav S, Tewari N, Antonarakis GS, Duggal R, Saji S, Lokade AK, Yadav R. Evidence Mapping and Quality Analysis of Systematic Reviews on Various Aspects Related to Cleft Lip and Palate. Journal of Clinical Medicine. 2023; 12(18):6002. https://doi.org/10.3390/jcm12186002
Chicago/Turabian StyleSrivastav, Sukeshana, Nitesh Tewari, Gregory S. Antonarakis, Ritu Duggal, Seba Saji, Amol Kumar Lokade, and Rahul Yadav. 2023. "Evidence Mapping and Quality Analysis of Systematic Reviews on Various Aspects Related to Cleft Lip and Palate" Journal of Clinical Medicine 12, no. 18: 6002. https://doi.org/10.3390/jcm12186002
APA StyleSrivastav, S., Tewari, N., Antonarakis, G. S., Duggal, R., Saji, S., Lokade, A. K., & Yadav, R. (2023). Evidence Mapping and Quality Analysis of Systematic Reviews on Various Aspects Related to Cleft Lip and Palate. Journal of Clinical Medicine, 12(18), 6002. https://doi.org/10.3390/jcm12186002