
Cost-Effectiveness of Exercise Therapy in Patients with Intermittent Claudication—A Comparison of Supervised Exercise, Home-Based Structured Exercise, and Walk Advice from the SUNFIT Trial

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients and Interventions
2.3. Health Outcomes
2.4. Economic Costs
2.5. Cost-Effectiveness Analysis
2.6. Statistical Analysis
3. Results
3.1. Study Population and Baseline Data
3.2. Health Outcomes and Economic Costs
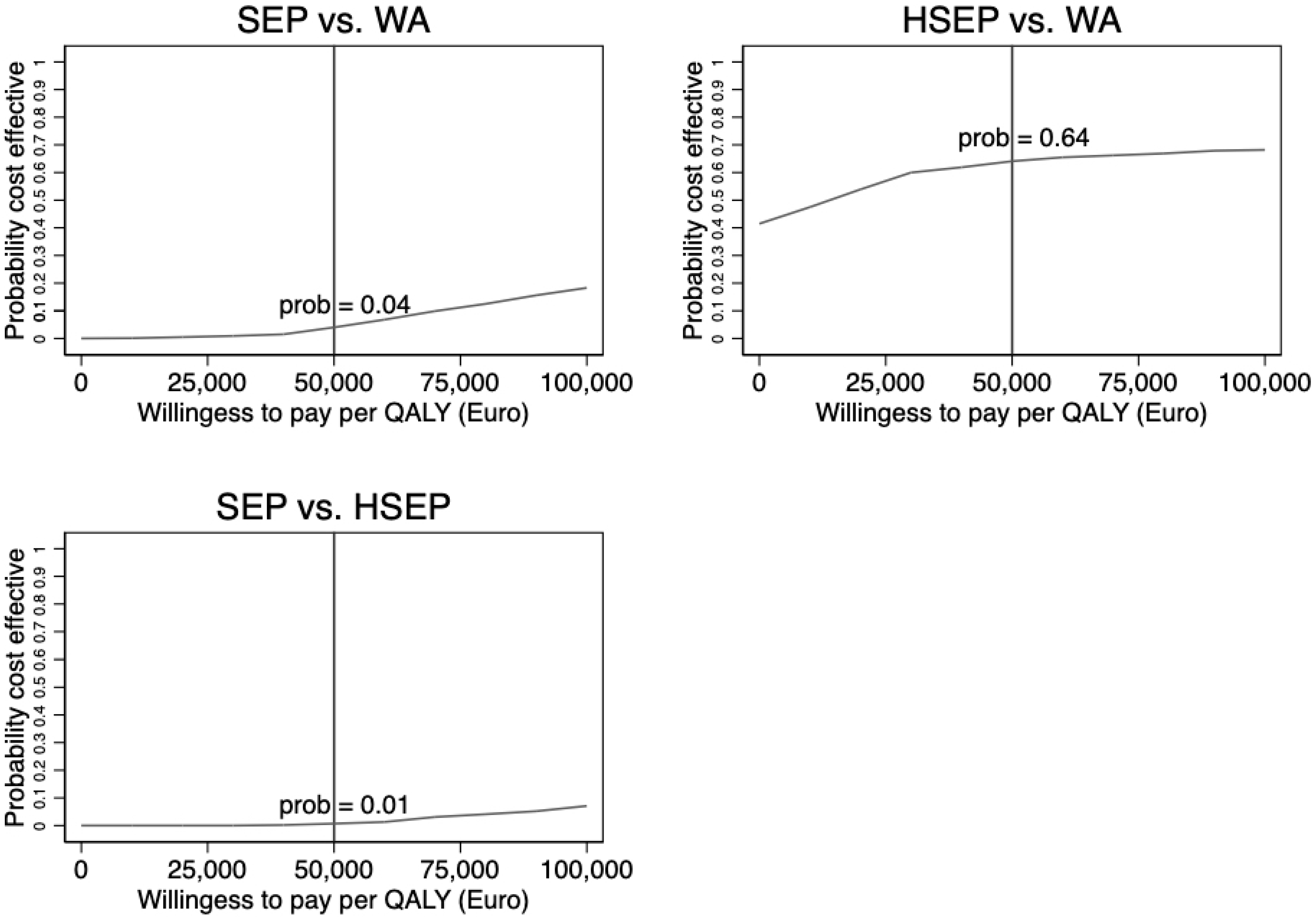
3.3. Cost-Effectiveness Analysis Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Song, P.; Rudan, D.; Zhu, Y.; Fowkes, F.J.I.; Rahimi, K.; Fowkes, F.G.R.; Rudan, I. Global, regional, and national prevalence and risk factors for peripheral artery disease in 2015: An updated systematic review and analysis. Lancet Glob. Health 2019, 7, e1020–e1030. [Google Scholar] [CrossRef]
- Peñín-Grandes, S.; Martín-Hernández, J.; Valenzuela, P.L.; López-Ortiz, S.; Pinto-Fraga, J.; Solá, L.D.R.; Emanuele, E.; Lista, S.; Lucia, A.; Santos-Lozano, A. Exercise and the hallmarks of peripheral arterial disease. Atherosclerosis 2022, 350, 41–50. [Google Scholar] [CrossRef]
- Fowkes, F.G.R.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.A.; Williams, L.J.; Mensah, G.A.; et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef]
- Sigvant, B.; Wiberg-Hedman, K.; Bergqvist, D.; Rolandsson, O.; Andersson, B.; Persson, E.; Wahlberg, E. A population-based study of peripheral arterial disease prevalence with special focus on critical limb ischemia and sex differences. J. Vasc. Surg. 2007, 45, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Sawlani, N.N.; Kinlay, S. Claudication: Pay for Structured Exercise or Go Take a Hike. JACC Cardiovasc. Interv. 2017, 10, 725–727. [Google Scholar] [CrossRef] [PubMed]
- Parmenter, B.J.; Dieberg, G.; Phipps, G.; Smart, N.A. Exercise training for health-related quality of life in peripheral artery disease: A systematic review and meta-analysis. Vasc. Med. 2015, 20, 30–40. [Google Scholar] [CrossRef]
- Milani, R.V.; Lavie, C.J. The role of exercise training in peripheral arterial disease. Vasc. Med. 2007, 12, 351–358. [Google Scholar] [CrossRef]
- Aboyans, V.; Ricco, J.-B.; Bartelink, M.-L.E.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.-P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: The European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2017, 39, 763–816. [Google Scholar] [CrossRef]
- Canonico, M.E.; Piccolo, R.; Avvedimento, M.; Leone, A.; Esposito, S.; Franzone, A.; Giugliano, G.; Gargiulo, G.; Hess, C.N.; Berkowitz, S.D.; et al. Antithrombotic Therapy in Peripheral Artery Disease: Current Evidence and Future Directions. J. Cardiovasc. Dev. Dis. 2023, 10, 164. [Google Scholar] [CrossRef]
- Lane, R.; Harwood, A.; Watson, L.; Leng, G.C. Exercise for intermittent claudication. Cochrane Database Syst. Rev. 2017, 12, CD000990. [Google Scholar] [CrossRef]
- Van den Houten, M.M.; Lauret, G.J.; Fakhry, F.; Fokkenrood, H.J.; van Asselt, A.D.; Hunink, M.G.; Teijink, J.A. Cost-effectiveness of supervised exercise therapy compared with endovascular revascularization for intermittent claudication. Br. J. Surg. 2016, 103, 1616–1625. [Google Scholar] [CrossRef] [PubMed]
- Fakhry, F.; Fokkenrood, H.J.; Spronk, S.; Teijink, J.A.; Rouwet, E.V.; Hunink, M.G.M. Endovascular revascularisation versus conservative management for intermittent claudication. Cochrane Database Syst. Rev. 2018, 3, CD010512. [Google Scholar] [CrossRef] [PubMed]
- Bäck, M.; Jivegård, L.; Johansson, A.; Nordanstig, J.; Svanberg, T.; Adania, U.W.; Sjögren, P. Home-based supervised exercise versus hospital-based supervised exercise or unsupervised walk advice as treatment for intermittent claudication: A systematic review. J. Rehabil. Med. 2015, 47, 801–808. [Google Scholar] [CrossRef]
- Gerhard-Herman, M.D.; Gornik, H.L.; Barrett, C.; Barshes, N.R.; Corriere, M.A.; Drachman, D.E.; Fleisher, L.A.; Fowkes, F.G.R.; Hamburg, N.M.; Kinlay, S.; et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: A report of the American college of cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e726–e779. [Google Scholar] [CrossRef] [PubMed]
- Murphy, T.P.; Cutlip, D.E.; Regensteiner, J.G.; Mohler, E.R., 3rd; Cohen, D.J.; Reynolds, M.R.; Massaro, J.M.; Lewis, B.A.; Cerezo, J.; Oldenburg, N.C.; et al. Supervised exercise, stent revascularization, or medical therapy for claudication due to aortoiliac peripheral artery disease: The CLEVER study. J. Am. Coll. Cardiol. 2015, 65, 999–1009. [Google Scholar] [CrossRef]
- Layden, J.; Michaels, J.; Bermingham, S.; Higgins, B. Diagnosis and management of lower limb peripheral arterial disease: Summary of NICE guidance. BMJ 2012, 345, e4947. [Google Scholar] [CrossRef]
- Makris, G.C.; Lattimer, C.R.; Lavida, A.; Geroulakos, G. Availability of Supervised Exercise Programs and the Role of Structured Home-based Exercise in Peripheral Arterial Disease. Eur. J. Vasc. Endovasc. Surg. 2012, 44, 569–575. [Google Scholar] [CrossRef]
- Gardner, A.W.; Parker, D.E.; Montgomery, P.S.; Scott, K.J.; Blevins, S.M. Efficacy of Quantified Home-Based Exercise and Supervised Exercise in Patients With Intermittent Claudication. Circulation 2011, 123, 491–498. [Google Scholar] [CrossRef]
- Al-Jundi, W.; Madbak, K.; Beard, J.D.; Nawaz, S.; Tew, G.A. Systematic review of home-based exercise programmes for individuals with intermittent claudication. Eur. J. Vasc. Endovasc. Surg. 2013, 46, 690–706. [Google Scholar] [CrossRef]
- King, R.W.; Canonico, M.E.; Bonaca, M.P.; Hess, C.N. Management of Peripheral Arterial Disease: Lifestyle Modifications and Medical Therapies. J. Soc. Cardiovasc. Angiogr. Interv. 2022, 1, 100513. [Google Scholar] [CrossRef]
- Harwood, A.E.; Hitchman, L.H.; Ingle, L.; Doherty, P.; Chetter, I.C. Preferred exercise modalities in patients with intermittent claudication. J. Vasc. Nurs. 2018, 36, 81–84. [Google Scholar] [CrossRef]
- Nicolaï, S.P.A.; Teijink, J.A.W.; Prins, M.H. Multicenter randomized clinical trial of supervised exercise therapy with or without feedback versus walking advice for intermittent claudication. J. Vasc. Surg. 2010, 52, 348–355. [Google Scholar] [CrossRef]
- Bartelink, M.L.; Stoffers, H.E.; Biesheuvel, C.J.; Hoes, A.W. Walking exercise in patients with intermittent claudication. Experience in routine clinical practice. Br. J. Gen. Pr. 2004, 54, 196–200. [Google Scholar]
- Bermingham, S.L.; Sparrow, K.; Mullis, R.; Fox, M.; Shearman, C.; Bradbury, A.; Michaels, J. The Cost-effectiveness of Supervised Exercise for the Treatment of Intermittent Claudication. Eur. J. Vasc. Endovasc. Surg. 2013, 46, 707–714. [Google Scholar] [CrossRef]
- Van Asselt, A.D.I.; Nicolaï, S.P.A.; Joore, M.A.; Prins, M.H.; Teijink, J.A.W. Cost-effectiveness of Exercise Therapy in Patients with Intermittent Claudication: Supervised Exercise Therapy versus a ‘Go Home and Walk’ Advice. Eur. J. Vasc. Endovasc. Surg. 2011, 41, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Sandberg, A.; Back, M.; Cider, A.; Jivegard, L.; Sigvant, B.; Wittboldt, S.; Nordanstig, J. Effectiveness of supervised exercise, home-based exercise or walk advice strategies on walking performance and muscle endurance in patients with intermittent claudication (SUNFIT trial)—A randomized clinical trial. Eur. J. Cardiovasc. Nurs. 2022, 22, 400–411. [Google Scholar] [CrossRef]
- Djerf, H.; Falkenberg, M.; Jivegård, L.; Lindgren, H.; Svensson, M.; Nordanstig, J. Cost-effectiveness of revascularization in patients with intermittent claudication. Br. J. Surg. 2018, 105, 1742–1748. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Snow, K.K.; Kolinski, M.; Gandeck, B. SF-36 Health Survey Manual and Interpretation Guide; New England Medical Center—The Health Institute: Boston, MA, USA, 1993. [Google Scholar]
- Brazier, J.; Roberts, J.; Deverill, M. The estimation of a preference-based measure of health from the SF-36. J. Health Econ. 2002, 21, 271–292. [Google Scholar] [CrossRef]
- Swedish National Board of Health and Welfare (Socialstyrelsen). Nationella Riktlinjer för Hjärtsjukvård: Hälsoekonomiskt Underlag Bilaga. Available online: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/nationella-riktlinjer/2018-6-28-halsoekonomiskt-underlag.pdf (accessed on 1 June 2020).
- Manca, A.; Hawkins, N.; Sculpher, M.J. Estimating mean QALYs in trial-based cost-effectiveness analysis: The importance of controlling for baseline utility. Health Econ. 2005, 14, 487–496. [Google Scholar] [CrossRef]
- Efron, B.; Tibshirani, R. Statistical data analysis in the computer age. Science 1991, 253, 390–395. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ 2009, 338, b2393. [Google Scholar] [CrossRef] [PubMed]
- StataCorp. Stata Statistical Software: Release 16; StataCorp LLC: College Station, TX, USA, 2019. [Google Scholar]
- Vanness, D.J.; Lomas, J.; Ahn, H. A Health Opportunity Cost Threshold for Cost-Effectiveness Analysis in the United States. Ann. Intern. Med. 2021, 174, 25–32. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Number of Patients (%) | WA (n = 51) | HSEP (n = 48) | SEP (n = 50) |
|---|---|---|---|
| Mean age (SD) | 72.5 (8.4) | 71.6 (6.8) | 72.3 (7.5) |
| Men:Women | 31:20 (61:39) | 28:20 (58:42) | 29:21 (58:42) |
| Smoking habits | |||
| Smoker | 15 (29) | 11 (23) | 15 (30) |
| Before | 30 (59) | 34 (71) | 31 (62) |
| Never | 6 (12) | 3 (6) | 4 (8) |
| Comorbidity | |||
| Diabetes Mellitus | 15 (30) | 16 (33) | 14 (28) |
| Heart disease a | 16 (31) | 12 (25) | 16 (32) |
| COPD | 5 (10) | 7 (15) | 7 (14) |
| Disease severity status (Rutherford classification) | |||
| Mild | 9 (18) | 7 (15) | 8 (16) |
| Moderate | 34 (67) | 28 (58) | 32 (64) |
| Severe | 8 (15) | 13 (27) | 10 (20) |
| Physically active before trial (30 min 3×/week) | 17 (33) | 14 (30) | 14 (28) |
| WA (n = 51) | HSEP (n = 48) | SEP (n = 50) | p-Value | |
|---|---|---|---|---|
| HRQoL scores, Mean (SD) | ||||
| Baseline (n = 131) | 0.70 (0.13) | 0.70 (0.12) | 0.68 (0.11) | 0.84 |
| At 3 months (n = 122) | 0.73 (0.13) | 0.74 (0.11) | 0.69 (0.13) | 0.17 |
| At 6 months (n = 117) | 0.71 (0.12) | 0.72 (0.12) | 0.72 (0.14) | 0.88 |
| At 12 months (n = 122) | 0.73 (0.12) | 0.73 (0.13) | 0.74 (0.12) | 0.94 |
| QALYs, Mean (95% CI) | ||||
| QALYs Complete case (n = 93) | 0.72 (0.69–0.75) | 0.74 (0.71–0.77) | 0.73 (0.70–0.76) | 0.77 |
| QALYs Multiple imputation (n = 149) | 0.72 (0.69–0.75) | 0.72 (0.69–0.75) | 0.71 (0.68–0.74) | 0.86 |
| Costs, Mean (95% CI) | ||||
| Outpatient costs |
EUR 1291 (EUR 1111–EUR 1471) | EUR 1327 (EUR 1162–EUR 1491) | EUR 3410 (EUR 2946–EUR 3872) | <0.01 |
| Inpatient costs |
EUR 490 (EUR 0–EUR 1473) |
EUR 493 (EUR 0–EUR 1012) | EUR 1209 (EUR 0–EUR 2423) | 0.47 |
| Total costs | 1781 (EUR 717–EUR 2845) | EUR 1820 (EUR 1203–EUR 2438) | EUR 4619 (EUR 3227–EUR 6010) | <0.01 |
| Comparison | Incremental Cost (95% CI) | Incremental QALYs (95% CI) * | Cost-Effectiveness Ratio |
|---|---|---|---|
| HSEP vs. WA | EUR 39.57 (−1194.83–1273.97) | 0.01 (−0.04–0.08) | EUR 3749 per QALY |
| SEP vs. WA | EUR 2837.94 (1112.64–4563.25) | 0.01 (−0.03–0.05) | EUR 278,981 per QALY |
| SEP vs. HSEP | EUR 2798.37 (1273.69–4323.05) | −0.0001 (−0.03–0.03) | HSEP dominates ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ulfsdottir, H.; Bäck, M.; Cider, Å.; Jivegård, L.; Sandberg, A.; Nordanstig, J.; Svensson, M. Cost-Effectiveness of Exercise Therapy in Patients with Intermittent Claudication—A Comparison of Supervised Exercise, Home-Based Structured Exercise, and Walk Advice from the SUNFIT Trial. J. Clin. Med. 2023, 12, 5277. https://doi.org/10.3390/jcm12165277
Ulfsdottir H, Bäck M, Cider Å, Jivegård L, Sandberg A, Nordanstig J, Svensson M. Cost-Effectiveness of Exercise Therapy in Patients with Intermittent Claudication—A Comparison of Supervised Exercise, Home-Based Structured Exercise, and Walk Advice from the SUNFIT Trial. Journal of Clinical Medicine. 2023; 12(16):5277. https://doi.org/10.3390/jcm12165277
Chicago/Turabian StyleUlfsdottir, Hildigunnur, Maria Bäck, Åsa Cider, Lennart Jivegård, Anna Sandberg, Joakim Nordanstig, and Mikael Svensson. 2023. "Cost-Effectiveness of Exercise Therapy in Patients with Intermittent Claudication—A Comparison of Supervised Exercise, Home-Based Structured Exercise, and Walk Advice from the SUNFIT Trial" Journal of Clinical Medicine 12, no. 16: 5277. https://doi.org/10.3390/jcm12165277
APA StyleUlfsdottir, H., Bäck, M., Cider, Å., Jivegård, L., Sandberg, A., Nordanstig, J., & Svensson, M. (2023). Cost-Effectiveness of Exercise Therapy in Patients with Intermittent Claudication—A Comparison of Supervised Exercise, Home-Based Structured Exercise, and Walk Advice from the SUNFIT Trial. Journal of Clinical Medicine, 12(16), 5277. https://doi.org/10.3390/jcm12165277