
Critically-Ill Patients with Biliary Obstruction and Cholangitis: Bedside Fluoroscopic-Free Endoscopic Drainage versus Percutaneous Drainage

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
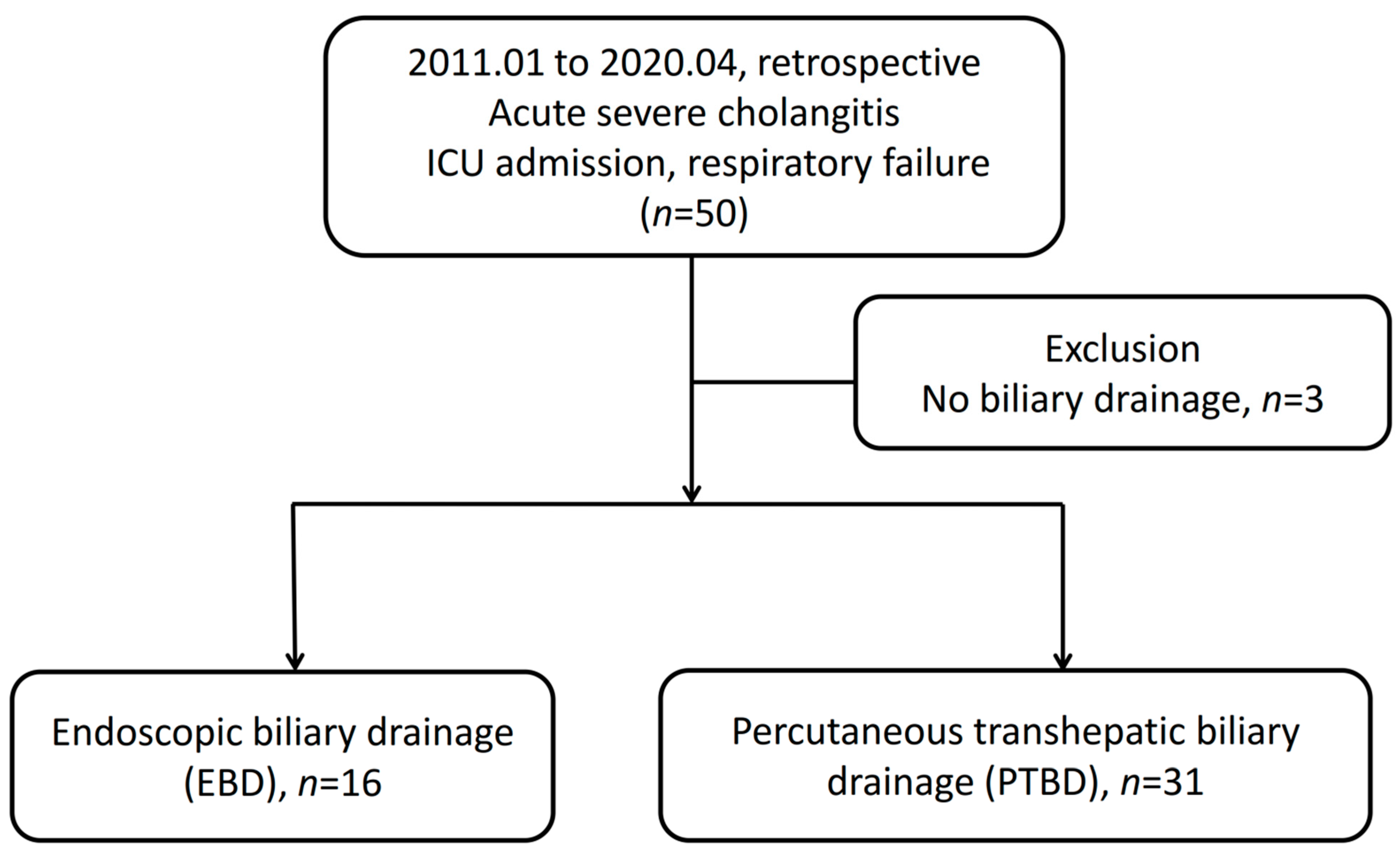
2.2. Study Subjects
2.3. Pre-Drainage Preparation
2.4. PTBD Procedures
2.5. EBD Procedures
2.6. Outcome Measurement
2.7. Statistical Analysis
3. Results
3.1. Study Subjects
3.2. Baseline Characteristics
3.3. Clinical Data
3.4. ERCP Procedures
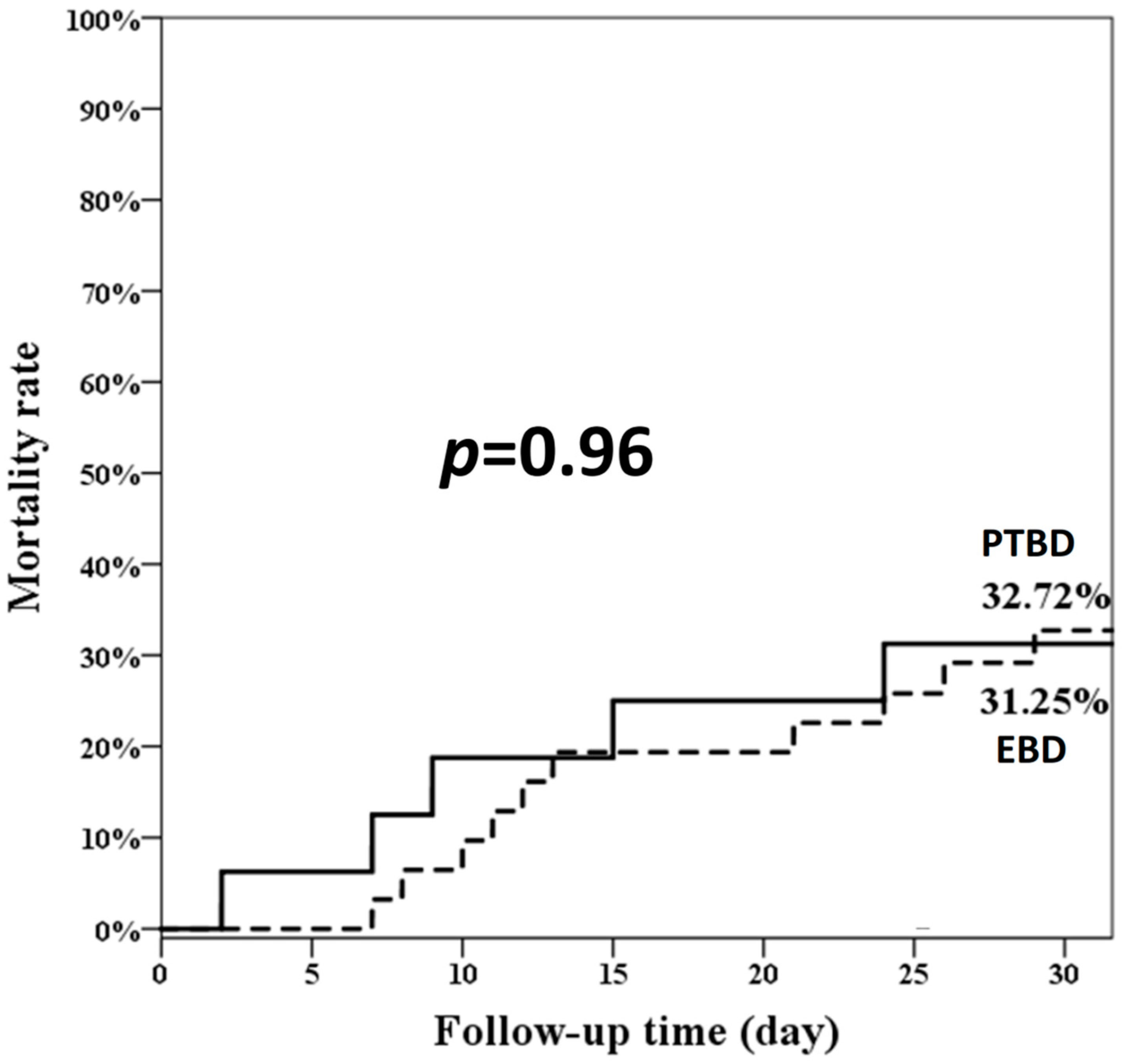
3.5. Risk Factors for 30-Day Mortality Rate
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leung, J.W.; Venezuela, R.R. Cholangiosepsis: Endoscopic drainage and antibiotic therapy. Endoscopy 1991, 23, 220–223. [Google Scholar] [CrossRef] [PubMed]
- Karvellas, C.J.; Abraldes, J.G.; Zepeda-Gomez, S.; Moffat, D.C.; Mirzanejad, Y.; Vazquez-Grande, G.; Esfahani, E.K.; Kumar, A.; Cooperative Antimicrobial Therapy of Septic Shock Database Research Group. The impact of delayed biliary decompression and anti-microbial therapy in 260 patients with cholangitis-associated septic shock. Aliment. Pharmacol. Ther. 2016, 44, 755–766. [Google Scholar] [CrossRef]
- Miura, F.; Okamoto, K.; Takada, T.; Strasberg, S.M.; Asbun, H.J.; Pitt, H.A.; Gomi, H.; Solomkin, J.S.; Schlossberg, D.; Han, H.S.; et al. Tokyo Guidelines 2018: Initial management of acute biliary infection and flowchart for acute cholangitis. J. Hepatobiliary Pancreat. Sci. 2018, 25, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Mukai, S.; Itoi, T.; Baron, T.H.; Takada, T.; Strasberg, S.M.; Pitt, H.A.; Ukai, T.; Shikata, S.; Teoh, A.Y.B.; Kim, M.H.; et al. Indications and techniques of biliary drainage for acute cholangitis in updated Tokyo Guidelines 2018. J. Hepatobiliary Pancreat. Sci. 2017, 24, 537–549. [Google Scholar] [CrossRef] [PubMed]
- Lai, E.C.; Mok, F.P.; Tan, E.S.; Lo, C.M.; Fan, S.T.; You, K.T.; Wong, J. Endoscopic biliary drainage for severe acute cholangitis. N. Engl. J. Med. 1992, 326, 1582–1586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, X.Z.; Chang, K.K.; Shin, J.S.; Chang, T.T.; Lin, C.Y. Endoscopic nasobiliary drainage for acute suppurative cholangitis: A sonographically guided method. Gastrointest. Endosc. 1993, 39, 174–176. [Google Scholar] [CrossRef]
- Stavropoulos, S.; Larghi, A.; Verna, E.; Stevens, P. Therapeutic endoscopic retrograde cholangiopancreatography without fluoroscopy in four critically ill patients using wire-guided intraductal ultrasound. Endoscopy 2005, 37, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Trindade, A.J.; Brun, A.; Vamadevan, A.S.; Sideridis, K.; Sejpal, D.V.; Mayo, P.H.; Khanijo, S.; Koenig, S.J. Use of bedside transabdominal US in facilitating emergent intensive care unit ERCP without fluoroscopy. Gastrointest. Endosc. 2015, 81, 1268–1269. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.P.; Huang, S.P.; Sun, M.S.; Chen, J.H.; Wang, H.H.; Lin, C.C.; Chang, Y.S.; Yang, C.S.; Wu, M.S.; Lin, J.T. Urgent endoscopic nasobiliary drainage without fluoroscopic guidance: A useful treatment for critically ill patients with biliary obstruction. Gastrointest. Endosc. 2000, 52, 741–744. [Google Scholar] [CrossRef] [PubMed]
- Saleem, A.; Gostout, C.J.; Petersen, B.T.; Topazian, M.D.; Gajic, O.; Baron, T.H. Outcome of emergency ERCP in the intensive care unit. Endoscopy 2011, 43, 549–551. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Zuo, W.; Zhou, X.; Zhou, X.; Li, G.; Liu, Z.; Wang, A.; Zhu, Y.; Lu, N.; Chen, Y. Bedside Biliary Drainage without Fluoroscopy for Critically Ill Patients. Biomed. Res. Int. 2020, 2020, 2850540. [Google Scholar] [CrossRef] [PubMed]
- Schorn, T.F.; Jahns, U.; Vollmer, C.; Gugler, R. Ultrasound-guided emergency endoscopic retrograde biliary drainage without radiography. Endoscopy 1997, 29, 232–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokoe, M.; Hata, J.; Takada, T.; Strasberg, S.M.; Asbun, H.J.; Wakabayashi, G.; Kozaka, K.; Endo, I.; Deziel, D.J.; Miura, F.; et al. Tokyo Guidelines 2018: Diagnostic criteria and severity grading of acute cholecystitis (with videos). J. Hepatobiliary Pancreat. Sci. 2018, 25, 41–54. [Google Scholar] [CrossRef]
- Knaus, W.A.; Zimmerman, J.E.; Wagner, D.P.; Draper, E.A.; Lawrence, D.E. APACHE-acute physiology and chronic health evaluation: A physiologically based classification system. Crit. Care Med. 1981, 9, 591–597. [Google Scholar] [CrossRef]
- Shah, R.; Qayed, E. Bedside Endoscopic Retrograde Cholangiopancreatography Using Portable X-ray in Acute Severe Cholangitis. Case Rep. Gastrointest. Med. 2018, 2018, 8763671. [Google Scholar] [CrossRef] [Green Version]
- Takada, T.; Hanyu, F.; Kobayashi, S.; Uchida, Y. Percutaneous transhepatic cholangial drainage: Direct approach under fluoroscopic control. J. Surg. Oncol. 1976, 8, 83–97. [Google Scholar] [CrossRef] [PubMed]
- Saad, W.E.; Wallace, M.J.; Wojak, J.C.; Kundu, S.; Cardella, J.F. Quality improvement guidelines for percutaneous transhepatic cholangiography, biliary drainage, and percutaneous cholecystostomy. J. Vasc. Interv. Radiol. 2010, 21, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Dumonceau, J.M.; Kapral, C.; Aabakken, L.; Papanikolaou, I.S.; Tringali, A.; Vanbiervliet, G.; Beyna, T.; Dinis-Ribeiro, M.; Hritz, I.; Mariani, A.; et al. ERCP-related adverse events: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2020, 52, 127–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.Y.; Park, C.H.; Cho, S.B.; Yoon, K.W.; Lee, W.S.; Kim, H.S.; Choi, S.K.; Rew, J.S. The safety and effectiveness of endoscopic biliary decompression by plastic stent placement in acute suppurative cholangitis compared with nasobiliary drainage. Gastrointest. Endosc. 2008, 68, 1076–1080. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Chan, A.C.; Lam, Y.H.; Ng, E.K.; Lau, J.Y.; Law, B.K.; Lai, C.W.; Sung, J.J.; Chung, S.C. Biliary decompression by nasobiliary catheter or biliary stent in acute suppurative cholangitis: A prospective randomized trial. Gastrointest. Endosc. 2002, 56, 361–365. [Google Scholar] [CrossRef]
- Sharma, B.C.; Kumar, R.; Agarwal, N.; Sarin, S.K. Endoscopic biliary drainage by nasobiliary drain or by stent placement in patients with acute cholangitis. Endoscopy 2005, 37, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Sekine, A.; Nakahara, K.; Sato, J.; Michikawa, Y.; Suetani, K.; Morita, R.; Igarashi, Y.; Itoh, F. Clinical Outcomes of Early Endoscopic Transpapillary Biliary Drainage for Acute Cholangitis Associated with Disseminated Intravascular Coagulation. J. Clin. Med. 2021, 10, 3606. [Google Scholar] [CrossRef] [PubMed]
- Lavillegrand, J.R.; Mercier-Des-Rochettes, E.; Baron, E.; Pene, F.; Contou, D.; Favory, R.; Preau, S.; Galbois, A.; Molliere, C.; Miailhe, A.F.; et al. Acute cholangitis in intensive care units: Clinical, biological, microbiological spectrum and risk factors for mortality: A multicenter study. Crit. Care 2021, 25, 49. [Google Scholar] [CrossRef]
- Zhu, Y.; Tu, J.; Zhao, Y.; Jing, J.; Dong, Z.; Pan, W. Association of Timing of Biliary Drainage with Clinical Outcomes in Severe Acute Cholangitis: A Retrospective Cohort Study. Int. J. Gen. Med. 2021, 14, 2953–2963. [Google Scholar] [CrossRef] [PubMed]
- Aboelsoud, M.; Siddique, O.; Morales, A.; Seol, Y.; Al-Qadi, M. Early biliary drainage is associated with favourable outcomes in critically-ill patients with acute cholangitis. Prz. Gastroenterol. 2018, 13, 16–21. [Google Scholar] [CrossRef]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; McIntyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristics | EBD (n = 16) | PTBD (n = 31) | p Value |
|---|---|---|---|
| Age, median (range), years | 81.60 (68.93–86.12) | 78.22 (68.76–84.76) | 0.74 |
| Gender, Male (%) | 9 (50.00) | 15 (48.39) | 1.00 |
| APACHE II score, median (range) | 28 (24.5–34.25) | 27 (21–33) | 0.47 |
| Underling comorbidities, n (%) | |||
| Hypertension | 6 (37.50) | 19 (61.29) | 0.22 |
| Type 2 diabetes mellitus | 5 (31.25) | 12 (38.71) | 0.85 |
| Chronic kidney disease | 7 (43.75) | 11 (35.48) | 0.81 |
| Congestive heart failure | 6 (37.50) | 5 (16.13) | 0.15 |
| Liver cirrhosis | 2 (12.50) | 4 (12.90) | 1.00 |
| Cerebral vascular accident | 3 (18.75) | 3 (9.68) | 0.40 |
| COPD | 4 (25.00) | 4 (12.90) | 0.42 |
| Pancreaticobiliary malignancy | 1 (6.25) | 4 (12.90) | 0.65 |
| Other malignancy | 5 (31.25) | 3 (9.68) | 0.10 |
| APACHE II score, median (range) | 26.5 (23.5–33.75) | 27 (21–33) | 0.71 |
| Septic shock, n (%) | 12 (75.00) | 24 (77.42) | 1.00 |
| Bacteremia, n (%) | 5 (31.25) | 16 (51.61) | 0.31 |
| Acute renal failure, n (%) | 8 (50.00) | 20 (64.52) | 0.52 |
| Emergent hemodialysis, n (%) | 5 (31.25) | 12 (38.71) | 0.85 |
| PTINR > 1.5, n (%) | 5 (31.25) | 5 (16.13) | 0.41 |
| Platelet < 100,000/mm3, n (%) | 9 (56.25) | 14 (45.16) | 0.68 |
| Time to biliary drainage (day) | 3.5 (2–6.75) | 1 (1–3) | 0.01 * |
| EBD (n = 16) | PTBD (n = 31) | p Value | |
|---|---|---|---|
| Pre-drainage | |||
| WBC (×1000/μL) | 11.73 (7.51–17.53) | 16.85 (9.34–21) | 0.08 |
| Hemoglobin (g/dL) | 9.05 (8.05–11.03) | 10.5 (9.4–12.1) | 0.03 |
| Platelet (×1000/μL) | 90 (43.25–154.50) | 117 (67–196) | 0.21 |
| Total bilirubin (mg/dL) | 5.45 (3.00–11.25) | 4.8 (2.4–8.3) | 0.45 |
| Alk-P (U/L) | 234 (121.75–416.50) | 317 (166–506) | 0.24 |
| AST (U/L) | 94 (57–188.5) | 113 (65–239) | 0.44 |
| ALT(U/L) | 36 (18.5–97.5) | 88 (41–153) | 0.03 * |
| PTINR | 1.25 (1.15–1.65) | 1.26 (1.17–1.36) | 0.77 |
| Creatinine (mg/dL) | 2.02 (0.81–3.59) | 1.69 (1.12–3.04) | 0.74 |
| Post-drainage | |||
| WBC (×1000/μL) | 10.05 (9.28–12.7) | 15.73 (11.2–21.29) | 0.05 |
| Hemoglobin(g/dL) | 9.35 (7.95–10.23) | 9.8 (8.9–10.9) | 0.20 |
| Platelet (×1000/μL) | 79.5 (47–143.25) | 74 (49–124) | 0.88 |
| Total bilirubin (mg/dL) | 5 (2.3–14.2) | 4.1 (1.2–6.6) | 0.31 |
| ΔTotal bilirubin | 0.2 (−1–2.73) | 0.7 (−2–2.2) | 0.75 |
| Alk-P (U/L) | 209 (143–540.75) | 207 (131–382) | 0.73 |
| AST (U/L) | 66 (41–184) | 98.5 (40.75–194) | 0.71 |
| ALT (U/L) | 20 (15–63) | 74 (33–148.75) | 0.02 * |
| PTINR | 1.57 (1.16–1.81) | 1.15 (1.05–1.38) | 0.02 * |
| Creatinine (mg/dL) | 1.42 (90.85–2.93) | 2.06 (0.86–2.70) | 0.65 |
| EBD (n = 16) | |
|---|---|
| Indications, n (%) | |
| CBD dilatation, cholangitis | 5 (31.25) |
| Choledocholithiasis | 8 (50.00) |
| Biliary pancreatitis | 1 (6.25) |
| Post-operation biliary leakage | 1 (6.25) |
| Ampulla vater tumor | 1 (6.25) |
| Procedure time (min), median (IQR) | 20 (20.35) |
| Interventions, n (%) | |
| EPT | 1 (6.25) |
| ERBD | 15 (93.75) |
| Technical success, n (%) | 15 (93.75) |
| Adverse events, n (%) | 1 (6.25) |
| Overall 30-day mortality rate | 5 (31.25) |
| Variable | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Group (PTBD vs. EBD) | 0.97 | (0.33–2.84) | 0.956 | |||
| Age | 1.05 | (0.99–1.12) | 0.082 | |||
| Male gender | 0.99 | (0.36–2.73) | 0.982 | |||
| APACHE II score | 1.05 | (0.97–1.14) | 0.195 | |||
| Underlying comorbidities | ||||||
| Chronic kidney disease | 1.44 | (0.52–3.98) | 0.480 | |||
| Congestive heart failure | 1.84 | (0.63–5.40) | 0.264 | |||
| Liver cirrhosis | 2.28 | (0.64–8.13) | 0.202 | |||
| COPD | 0.78 | (0.18–3.47) | 0.747 | |||
| Pancreaticobiliary malignancy | 0.56 | (0.07–4.28) | 0.578 | |||
| Other malignancy | 3.73 | (1.27–11.01) | 0.017 * | 5.27 | (1.01–27.57) | 0.049 * |
| Septic shock | 0.54 | (0.18–1.58) | 0.262 | |||
| Time to drainage >2 days | 2.68 | (0.95–7.57) | 0.062 | |||
| Emergent dialysis | 4.86 | (1.65–14.29) | 0.004 * | 7.30 | (2.20–24.24) | 0.001 ** |
| Pre-drainage data | ||||||
| WBC (×1000/μL) | 1.00 | (1.00–1.00) | 0.339 | |||
| Hemoglobin (g/dL) | 0.92 | (0.74–1.15) | 0.451 | |||
| Platelet (×1000/μL) | 1.00 | (0.99–1.01) | 0.716 | |||
| Total bilirubin (mg/dL) | 0.27 | (0.97–1.13) | 0.273 | |||
| AlK-P (U/L) | 1.00 | (1.00–1.00) | 0.752 | |||
| AST (U/L) | 1.00 | (1.00–1.00) | 0.173 | |||
| ALT (U/L) | 1.00 | (1.00–1.00) | 0.902 | |||
| PTINR | 4.14 | (1.18–14.57) | 0.027 * | 3.42 | (0.68–17.32) | 0.137 |
| ΔTotal bilirubin | 0.82 | (0.73–0.93) | 0.001 ** | 0.90 | (0.76–1.06) | 0.197 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, Y.-J.; Lin, W.-T.; Tsai, H.-J.; Chen, C.-C.; Tung, C.-F.; Yang, S.-S.; Peng, Y.-C. Critically-Ill Patients with Biliary Obstruction and Cholangitis: Bedside Fluoroscopic-Free Endoscopic Drainage versus Percutaneous Drainage. J. Clin. Med. 2022, 11, 1869. https://doi.org/10.3390/jcm11071869
Liao Y-J, Lin W-T, Tsai H-J, Chen C-C, Tung C-F, Yang S-S, Peng Y-C. Critically-Ill Patients with Biliary Obstruction and Cholangitis: Bedside Fluoroscopic-Free Endoscopic Drainage versus Percutaneous Drainage. Journal of Clinical Medicine. 2022; 11(7):1869. https://doi.org/10.3390/jcm11071869
Chicago/Turabian StyleLiao, Yi-Jun, Wan-Tzu Lin, Hsin-Ju Tsai, Chia-Chang Chen, Chun-Fang Tung, Sheng-Shun Yang, and Yen-Chun Peng. 2022. "Critically-Ill Patients with Biliary Obstruction and Cholangitis: Bedside Fluoroscopic-Free Endoscopic Drainage versus Percutaneous Drainage" Journal of Clinical Medicine 11, no. 7: 1869. https://doi.org/10.3390/jcm11071869
APA StyleLiao, Y.-J., Lin, W.-T., Tsai, H.-J., Chen, C.-C., Tung, C.-F., Yang, S.-S., & Peng, Y.-C. (2022). Critically-Ill Patients with Biliary Obstruction and Cholangitis: Bedside Fluoroscopic-Free Endoscopic Drainage versus Percutaneous Drainage. Journal of Clinical Medicine, 11(7), 1869. https://doi.org/10.3390/jcm11071869