
Arrhythmias in COVID-19/SARS-CoV-2 Pneumonia Infection: Prevalence and Implication for Outcomes



 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dzieciatkowski, T.; Szarpak, L.; Filipiak, K.J.; Jaguszewski, M.; Ladny, J.R.; Smereka, J. COVID-19 challenge for modern medicine. Cardiol. J. 2020, 27, 175–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SARS-CoV2 Epidemiology. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---1-march-2022 (accessed on 25 December 2021).
- De Filippo, O.; D’Ascenzo, F.; Angelini, F.; Bocchino, P.P.; Conrotto, F.; Saglietto, A.; Secco, G.G.; Campo, G.; Gallone, G.; Verardi, R.; et al. Reduced Rate of Hospital Admissions for ACS during COVID-19 Outbreak in Northern Italy. N. Engl. J. Med. 2020, 383, 88–89. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Pellicori, P.; Doolub, G.; Wong, C.M.; Lee, K.S.; Mangion, K.; Ahmad, M.; Berry, C.; Squire, I.; Lambiase, P.D.; Lyon, A.; et al. COVID-19 and its cardiovascular effects: A systematic review of prevalence studies. Cochrane Database Syst. Rev. 2021, 3, CD013879. [Google Scholar] [PubMed]
- Bhatla, A.; Mayer, M.M.; Adusumalli, S.; Hyman, M.C.; Oh, E.; Tierney, A.; Moss, J.; Chahal, A.A.; Anesi, G.; Denduluri, S.; et al. COVID-19 and cardiac arrhythmias. Heart Rhythm 2020, 17, 1439–1444. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; Gong, W.; Liu, X.; Liang, J.; Zhao, Q.; et al. Association of Cardiac Injury with Mortality in Hospitalized Patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020, 5, 802–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chorin, E.; Dai, M.; Shulman, E.; Wadhwani, L.; Bar-Cohen, R.; Barbhaiya, C.; Aizer, A.; Holmes, D.; Bernstein, S.; Spinelli, M.; et al. The QT interval in patients with COVID-19 treated with hydroxychloroquine and azithromycin. Nat. Med. 2020, 26, 808–809. [Google Scholar] [CrossRef]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular Implications of Fatal Outcomes of Patients with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shao, F.; Xu, S.; Ma, X.; Xu, Z.; Lyu, J.; Ng, M.; Cui, H.; Yu, C.; Zhang, Q.; Sun, P.; et al. In-hospital cardiac arrest outcomes among patients with COVID-19 pneumonia in Wuhan, China. Resuscitation 2020, 151, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Inciardi, R.M.; Adamo, M.; Lupi, L.; Cani, D.S.; Di Pasquale, M.; Tomasoni, D.; Italia, L.; Zaccone, G.; Tedino, C.; Fabbricatore, D.; et al. Characteristics and outcomes of patients hospitalized for COVID-19 and cardiac disease in Northern Italy. Eur. Heart J. 2020, 41, 1821–1829. [Google Scholar] [CrossRef] [PubMed]
- Szarpak, L.; Filipiak, K.J.; Skwarek, A.; Pruc, M.; Rahnama, M.; Denegri, A.; Jachowicz, M.; Dawidowska, M.; Gasecka, A.; Jaguszewski, M.J.; et al. Outcomes and mortality associated with atrial arrhythmias among patients hospitalized with COVID-19: A systematic review and meta-analysis. Cardiol. J. 2021, 29, 33–43. [Google Scholar] [CrossRef]
- Kochav, S.M.; Coromilas, E.; Nalbandian, A.; Ranard, L.S.; Gupta, A.; Chung, M.K.; Gopinathannair, R.; Biviano, A.B.; Garan, H.; Wan, E.Y. Cardiac Arrhythmias in COVID-19 Infection. Circ. Arrhythm. Electrophysiol. 2020, 13, e008719. [Google Scholar] [CrossRef] [PubMed]
- Karamchandani, K.; Quintili, A.; Landis, T.; Bose, S. Cardiac Arrhythmias in Critically Ill Patients with COVID-19: A Brief Review. J. Cardiothorac. Vasc. Anesth. 2021, 35, 3789–3796. [Google Scholar] [CrossRef]
- Driggin, E.; Madhavan, M.V.; Bikdeli, B.; Chuich, T.; Laracy, J.; Biondi-Zoccai, G.; Brown, T.S.; Der Nigoghossian, C.; Zidar, D.A.; Haythe, J.; et al. Cardiovascular considerations for patients, health care workers, and health systems during the COVID-19 pandemic. J. Am. Coll. Cardiol. 2020, 75, 2352–2371. [Google Scholar] [CrossRef]
- Goyal, P.; Choi, J.J.; Pinheiro, L.C.; Schenck, E.J.; Chen, R.; Jabri, A.; Satlin, M.J.; Campion, T.R., Jr.; Nahid, M.; Ringel, J.B.; et al. Clinical characteristics of COVID-19 in New York City. N. Engl. J. Med. 2020, 382, 2372–2374. [Google Scholar] [CrossRef]
- Tasdemir, G.; Kelebek Girgin, N.; Aydin Kaderli, A.; Cizmeci, E.; Iscimen, R.; Kahveci, F.; Aydinlar, A. Arrhythmia incidence and risk factors in critically ill patients. Crit. Care 2015, 19, P156. [Google Scholar] [CrossRef] [Green Version]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [PubMed]
- Giudicessi, J.R.; Roden, D.M.; Wilde, A.A.M.; Ackerman, M.J. Classification and reporting of potentially proarrhythmic common genetic variation in long QT syndrome genetic testing. Circulation 2018, 137, 619–630. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Wang, T.J.; Parise, H.; Levy, D.; D’Agostino, R.B., Sr.; Wolf, P.A.; Vasan, R.S.; Benjamin, E.J. Obesity and the risk of new-onset atrial fibrillation. JAMA 2004, 292, 2471–2477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaghee, F.; Nafakhi, H.; Alareedh, M.; Nafakhi, A.; Al-Buthabhak, K. ECG markers of malignant arrhythmias and in-hospital outcome of COVID-19 pneumonia. J. Arrhythm. 2021, 37, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, J.Y.C.; Kan, J.Y.L.; Mattar, S.A.M.; Qin, Y. The clinical implications of sinus tachycardia in mild COVID-19 infection: A retrospective cohort study. SAGE Open Med. 2021, 9, 20503121211054973. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.H.; Namazi, A.; Shelton, R.; Ramireddy, A.; Ehdaie, A.; Shehata, M.; Wang, X.; Marbán, E.; Chugh, S.S.; Cingolani, E. Cardiac arrhythmias in hospitalized patients with COVID-19: A prospective observational study in the western United States. PLoS ONE 2020, 15, e0244533. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Yu, Z.; Yuan, Y.; Han, J.; Wang, Z.; Chen, H.; Wang, S.; Wang, Z.; Hu, H.; Zhou, L.; et al. Alteration of Autonomic Nervous System Is Associated with Severity and Outcomes in Patients with COVID-19. Front. Physiol. 2021, 12, 630038. [Google Scholar] [CrossRef] [PubMed]
- Mol, M.B.A.; Strous, M.T.A.; van Osch, F.H.M.; Vogelaar, F.J.; Barten, D.G.; Farchi, M.; Foudraine, N.A.; Gidron, Y. Heart-rate-variability (HRV), predicts outcomes in COVID-19. PLoS ONE 2021, 16, e0258841. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Liang, X.; Xu, J.; Hou, H.; Wang, Y. Meta-analysis of atrial fibrillation in patients with COVID-19. Am. J. Cardiol. 2021, 144, 152–156. [Google Scholar] [CrossRef]
- Uribarri, A.; Núñez-Gil, I.J.; Aparisi, Á.; Arroyo-Espliguero, R.; Maroun Eid, C.; Romero, R.; Becerra-Muñoz, V.M.; Feltes, G.; Molina, M.; García-Aguado, M.; et al. Atrial fibrillation in patients with COVID-19. Usefulness of the CHA2DS2-VASc score: An analysis of the international HOPE COVID-19 registry. Rev. Esp. Cardiol. Engl. Ed. 2021, 74, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Sanchis-Gomar, F.; Perez-Quilis, C.; Lavie, C.J. Should atrial fibrillation be considered a cardiovascular risk factor for a worse prognosis in COVID-19 patients? Eur. Heart J. 2020, 41, 3092–3093. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Chen, S.; Fu, Y.; Gao, Z.; Long, H.; Ren, H.W.; Zuo, Y.; Wang, J.; Li, H.; Xu, Q.B.; et al. Risk factors associated with clinical outcomes in 323 COVID-19 patients in Wuhan, China. Clin. Infect. Dis. 2020, 71, 2089–2098. [Google Scholar] [CrossRef] [PubMed]
- Gao, P.; Wu, W.; Tian, R.; Yan, X.; Qian, H.; Guo, F.; Li, T.; Liu, Z.; Wang, J.; Zhou, X.; et al. Association between tachyarrhythmia and mortality in a cohort of critically ill patients with coronavirus disease 2019 (COVID-19). Ann. Transl. Med. 2021, 9, 883. [Google Scholar] [CrossRef] [PubMed]
- D’Ascenzo, F.; De Filippo, O.; Borin, A.; Barbieri, L.; Adamo, M.; Morici, N.; Truffa Giachet, A.; Iannaccone, M.; Crimi, G.; Gaido, L.; et al. Impact of COVID-19 pandemic and infection on in hospital survival for patients presenting with acute coronary syndromes: A multicenter registry. Int. J. Cardiol. 2021, 332, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Turagam, M.K.; Musikantow, D.; Goldman, M.E.; Bassily-Marcus, A.; Chu, E.; Shivamurthy, P.; Lampert, J.; Kawamura, I.; Bokhari, M.; Whang, W.; et al. Malignant Arrhythmias in Patients with COVID-19: Incidence, Mechanisms, and Outcomes. Circ. Arrhythm. Electrophysiol. 2020, 13, e008920. [Google Scholar] [CrossRef] [PubMed]
- Weng, H.; Yang, F.; Zhang, L.; Jin, H.; Liu, S.; Fan, F.; Liu, Z.; Zheng, X.; Yang, H.; Li, Y.; et al. Joint Predictive Value of cTnI and NT-proBNP on Mortality in Patients with Coronavirus Disease 2019: A Retrospective Research in Wuhan, China. J. Transl. Int. Med. 2021, 9, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Lazzerini, P.E.; Boutjdir, M.; Capecchi, P.L. COVID-19, arrhythmic risk, and inflammation: Mind the gap! Circulation 2020, 142, 7–9. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Total (n = 902) | ARs (n = 122) | No-ARs (n = 515) | p | |
|---|---|---|---|---|
| Comorbidities | ||||
| Age, years [IQR] | 72.0 (24) | 75.5 (22) | 72.0 (29) | <0.001 |
| Female sex, % | 36.5 | 39.3 | 36.7 | 0.329 |
| Hypertension, % | 55.7 | 68.0 | 52.8 | 0.001 |
| Diabetes, % | 22.4 | 19.7 | 23.1 | 0.245 |
| Obesity, % | 12.7 | 11.5 | 13.0 | 0.388 |
| COPD, % | 9.4 | 10.7 | 9.1 | 0.355 |
| Cancer, % | 12.7 | 14.8 | 12.2 | 0.269 |
| Previous AF, % | 11.6 | 34.4 | 6.2 | <0.001 |
| CAD, % | 13.7 | 23.8 | 13.6 | 0.005 |
| PAD, % | 8.0 | 11.5 | 9.9 | 0.354 |
| CKD, % | 10.6 | 18.0 | 9.5 | 0.008 |
| Previous TE, % | 3.2 | 6.6 | 3.1 | 0.069 |
| Previous CVE, % | 7.4 | 9.0 | 8.0 | 0.409 |
| Symptoms | ||||
| Fever, % | 81.6 | 79.5 | 82.1 | 0.289 |
| Cough, % | 44.9 | 38.5 | 46.6 | 0.065 |
| Dyspnea, % | 64.9 | 69.7 | 64.7 | 0.173 |
| Vital parameters | ||||
| HR (bpm) | 90 | 83 (29) | 90 (23) | 0.542 |
| SO2 (%) | 93 | 90 (9) | 94 (5) | 0.918 |
| SBP (mmHg) | 135 | 138 (64) | 130 (40) | 0.696 |
| DBP (mmHg) | 80 | 75 (33) | 80 (20) | 0.185 |
| ECG parameters | ||||
| HR (bpm) | 90 (22) | 75 (46) | 82 (22) | 0.462 |
| QTc (msec) | 441 (39) | 483 (99) | 440 (30) | <0.001 |
| aConduction | 20.4 | 27.0 | 19.2 | 0.039 |
| aRepolarization | 5.6 | 7.4 | 5.2 | 0.236 |
| Biomarkers | ||||
| cTnI (ng/L) | 12 (30) | 41 (56) | 13 (57) | 0.298 |
| BNP (pg/mL) | 89 (180.5) | 287.5 (369) | 92 (168) | 0.160 |
| WBC (103/mm3) | 6.6 (3.9) | 7.2 (5.2) | 7.9 (4.2) | 0.042 |
| CRP (mg/L) | 5.7 (12.4) | 14.1 (24.8) | 13.1 (15.8) | 0.986 |
| LDH (U/L) | 533 (227.3) | 479 (473) | 584 (183) | 0.719 |
| Uraemia (mg/dL) | 42 (30) | 48.5 (24) | 42 (19) | <0.001 |
| HR | 95% CI | p Value | |
|---|---|---|---|
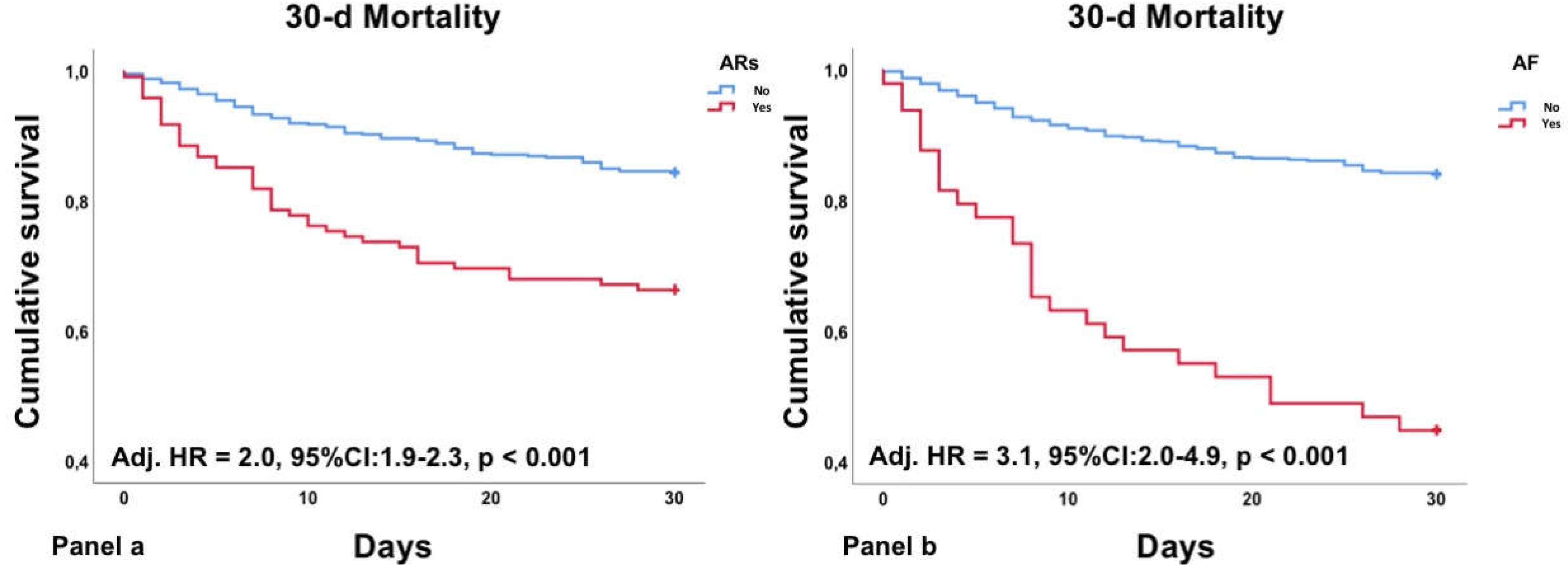
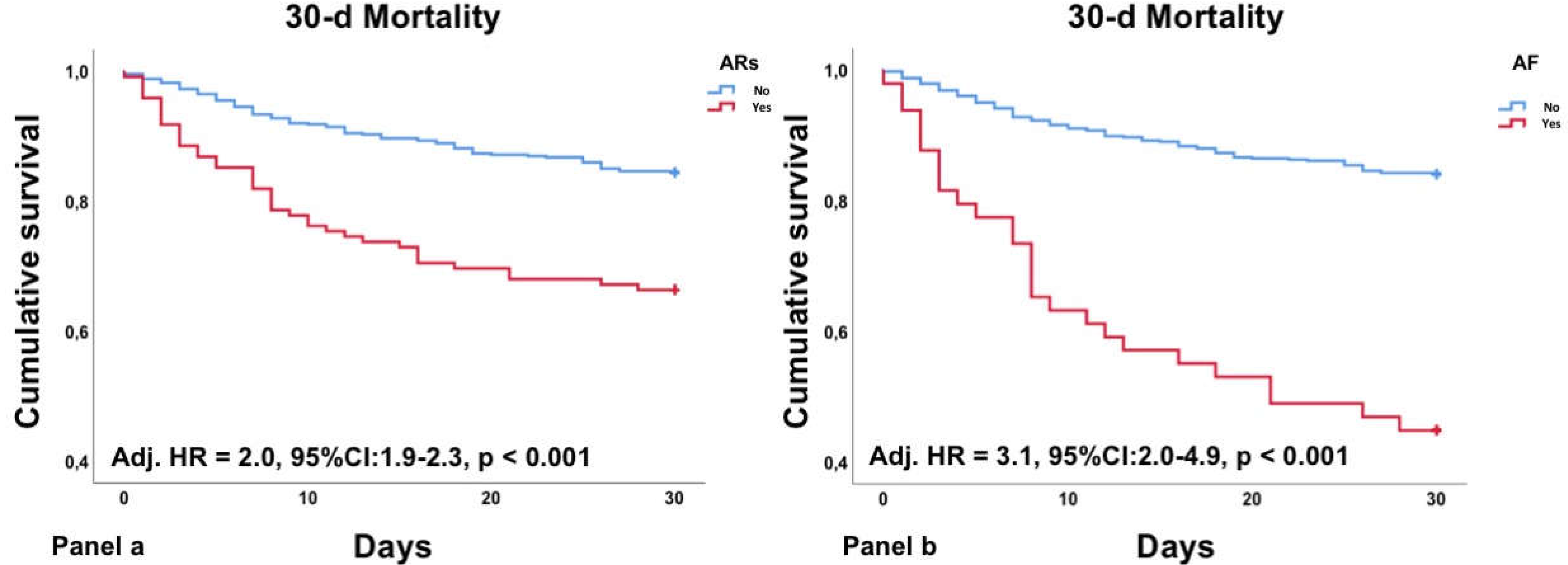
| ARs | 2.0 | 1.9–2.3 | <0.001 |
| Age > 65 | 6.1 | 3.1–11.9 | <0.001 |
| Hypertension | 1.6 | 1.1–2.4 | 0.023 |
| CAD | 1.0 | 0.6–1.6 | 0.893 |
| Comorbidities > 2 | 1.9 | 1.2–2.8 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Denegri, A.; Sola, M.; Morelli, M.; Farioli, F.; Tosetti, A.; D’Arienzo, M.; Savorani, F.; Pezzuto, G.S.; Boriani, G.; Szarpak, L.; et al. Arrhythmias in COVID-19/SARS-CoV-2 Pneumonia Infection: Prevalence and Implication for Outcomes. J. Clin. Med. 2022, 11, 1463. https://doi.org/10.3390/jcm11051463
Denegri A, Sola M, Morelli M, Farioli F, Tosetti A, D’Arienzo M, Savorani F, Pezzuto GS, Boriani G, Szarpak L, et al. Arrhythmias in COVID-19/SARS-CoV-2 Pneumonia Infection: Prevalence and Implication for Outcomes. Journal of Clinical Medicine. 2022; 11(5):1463. https://doi.org/10.3390/jcm11051463
Chicago/Turabian StyleDenegri, Andrea, Matteo Sola, Marianna Morelli, Francesco Farioli, Alberto Tosetti, Matteo D’Arienzo, Fulvio Savorani, Giuseppe Stefano Pezzuto, Giuseppe Boriani, Lukasz Szarpak, and et al. 2022. "Arrhythmias in COVID-19/SARS-CoV-2 Pneumonia Infection: Prevalence and Implication for Outcomes" Journal of Clinical Medicine 11, no. 5: 1463. https://doi.org/10.3390/jcm11051463
APA StyleDenegri, A., Sola, M., Morelli, M., Farioli, F., Tosetti, A., D’Arienzo, M., Savorani, F., Pezzuto, G. S., Boriani, G., Szarpak, L., & Magnani, G. (2022). Arrhythmias in COVID-19/SARS-CoV-2 Pneumonia Infection: Prevalence and Implication for Outcomes. Journal of Clinical Medicine, 11(5), 1463. https://doi.org/10.3390/jcm11051463