
Efficacy and Safety of Rituximab in Autoimmune Disease—Associated Interstitial Lung Disease: A Prospective Cohort Study

 ,
, 
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Study Population
2.3. Protocol
2.4. Working Definitions and Variables
2.5. Statistical Analysis
3. Results
3.1. Baseline Clinical Characteristics
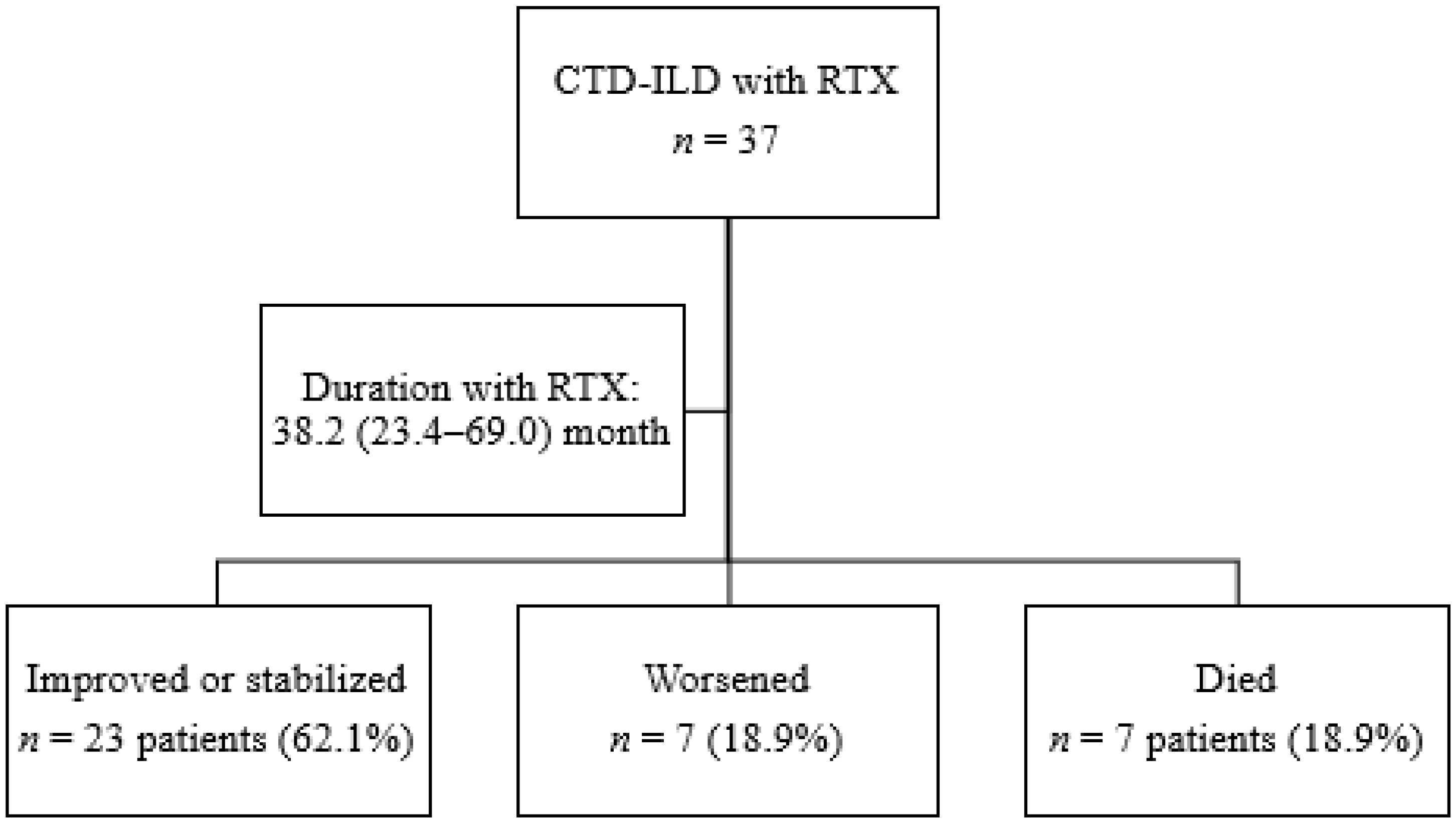
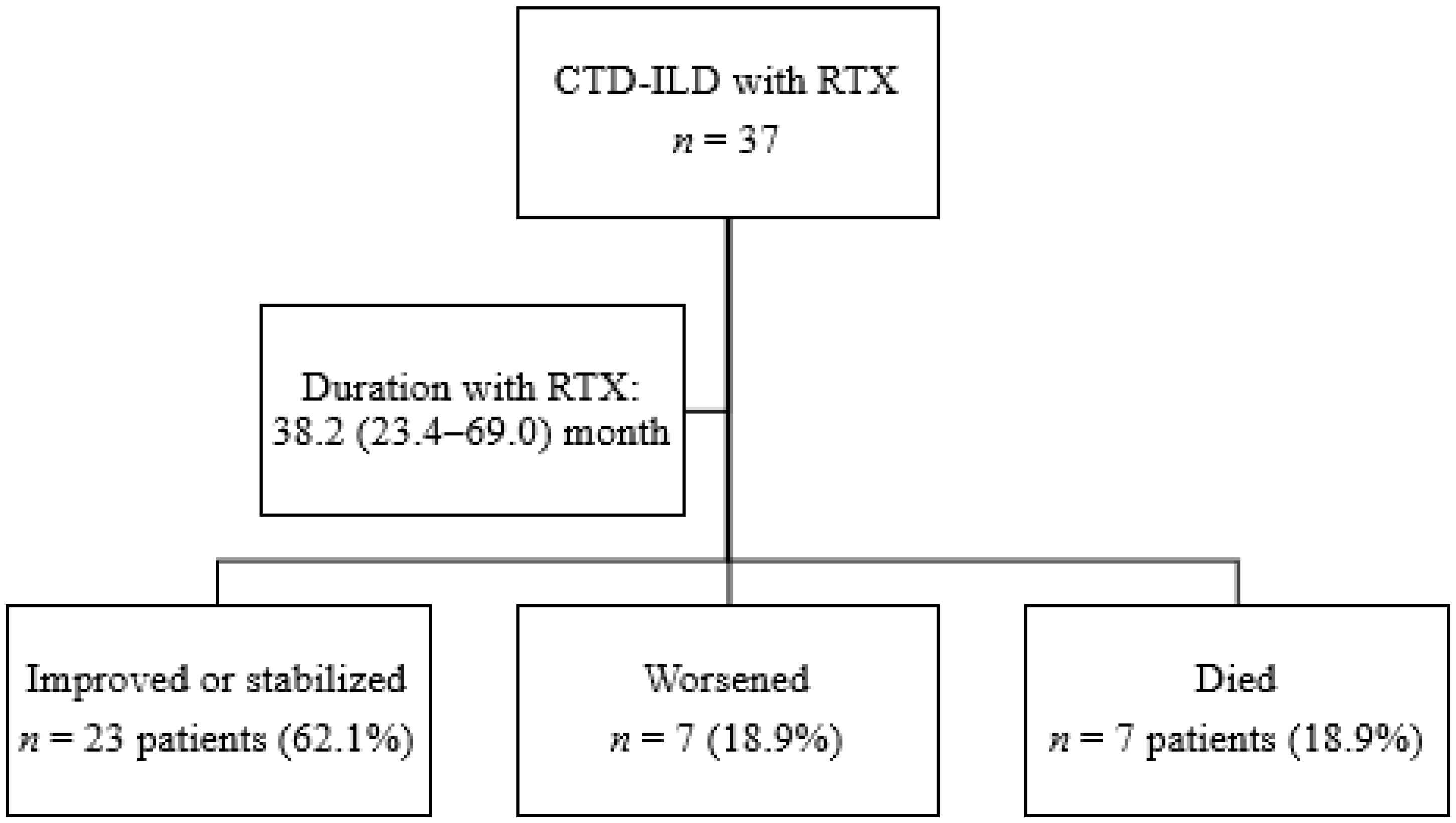
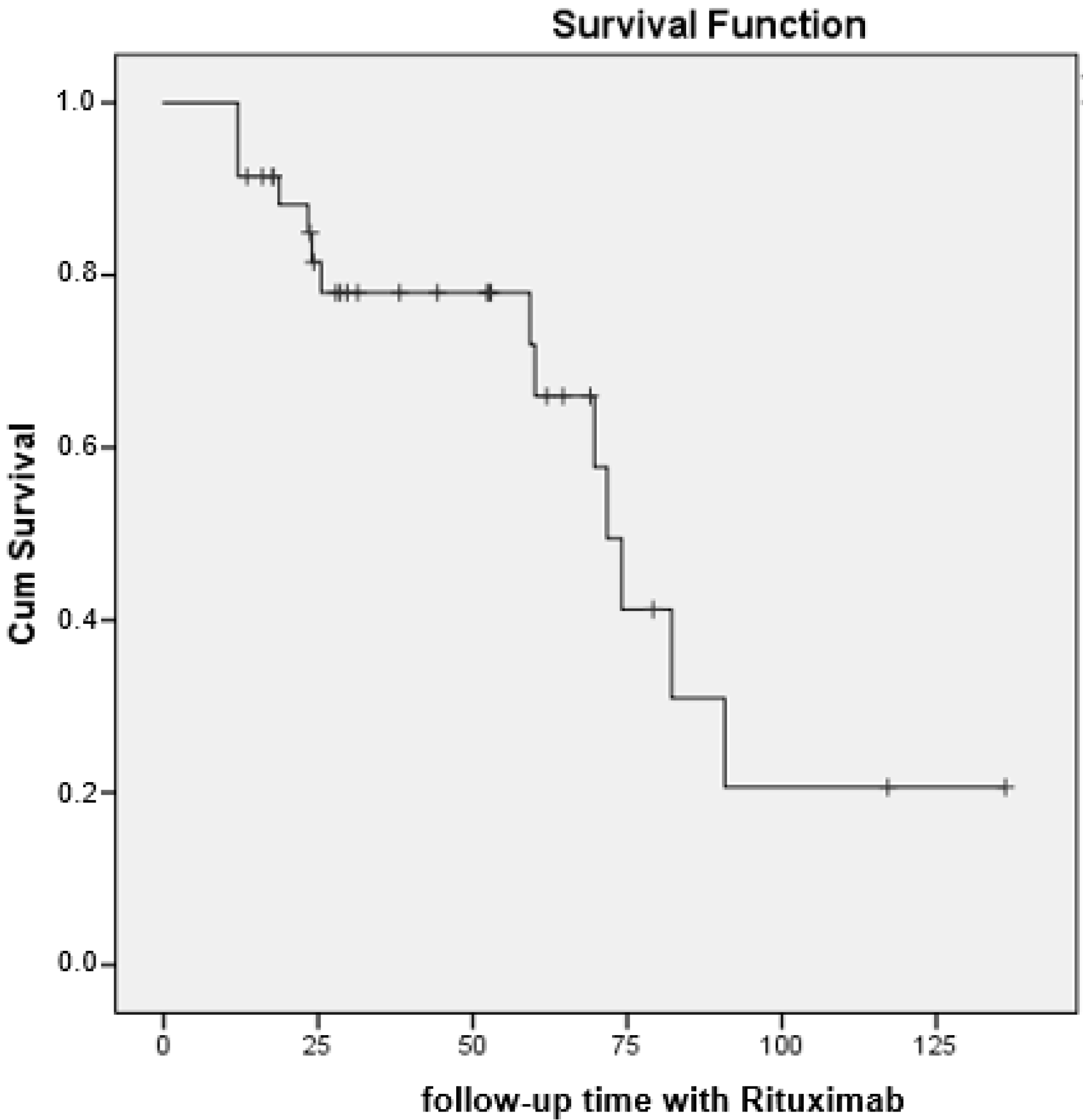
3.2. Clinical Course
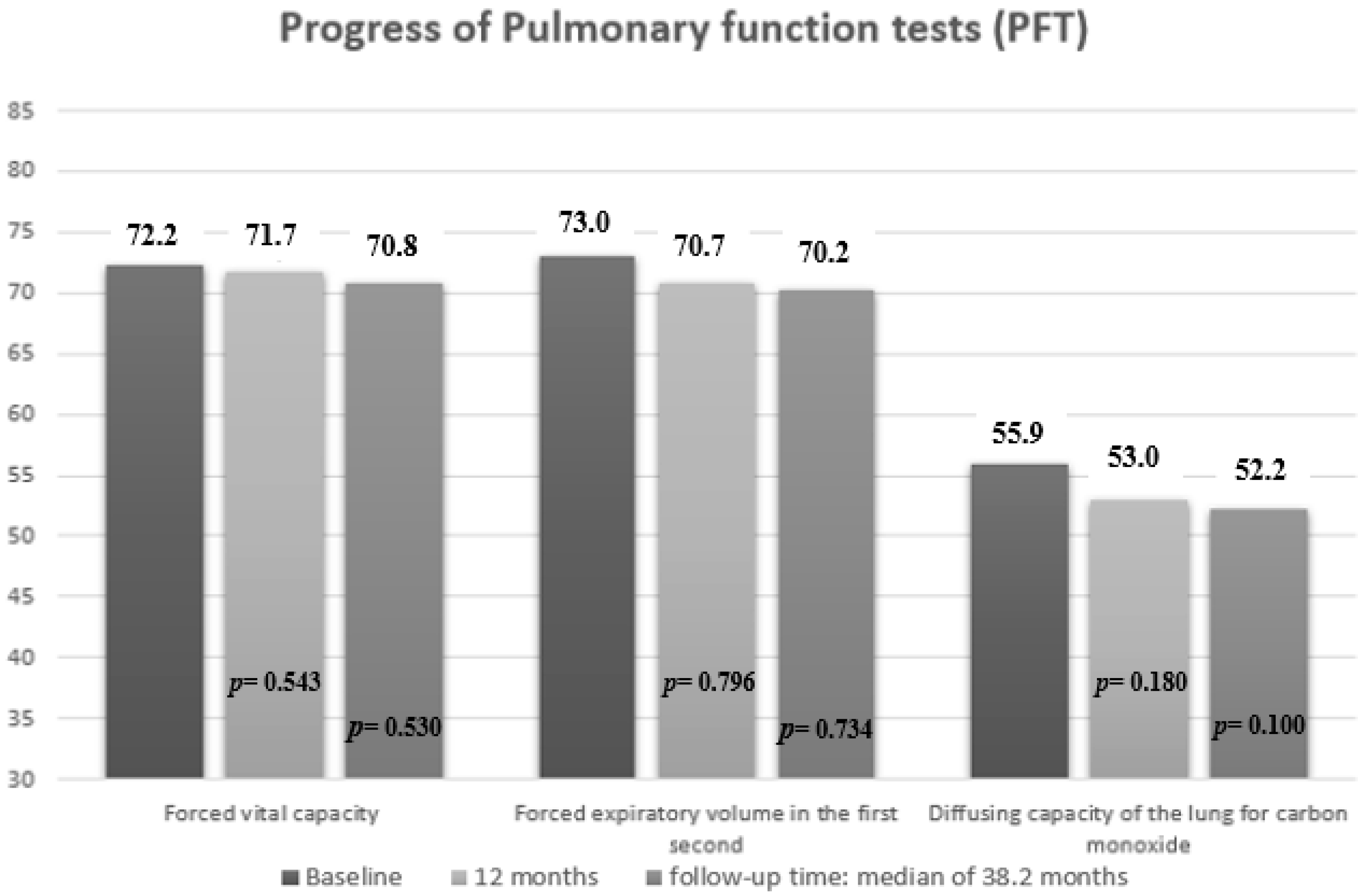
3.3. Pulmonary Outcomes
3.4. Factors Associated with Progression of ILD in Patients with CTD-ILD Treated with Rituximab
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Robles-Pérez, A.; Luburich, P.; Bolivar, S.; Dorca, J.; Nolla, J.M.; Molina-Molina, M.; Narváez, J.A. A prospective study of lung disease in a cohort of early rheumatoid arthritis patients. Sci. Rep. 2020, 10, 15640. [Google Scholar] [CrossRef] [PubMed]
- Demoruelle, M.K.; Mittoo, S.; Solomon, J.J. Connective tissue disease-related interstitial lung disease. Best Pract. Res. Clin. Rheumatol. 2016, 30, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Steen, V.D.; Medsger, T.A. Changes in causes of death in systemic sclerosis, 1972–2002. Ann. Rheum. Dis. 2007, 66, 940–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cottin, V.; Thivolet-Béjui, F.; Reynaud-Gaubert, M.; Cadranel, J.; Delaval, P.; Ternamian, P.J.; Cordier, J.F. Interstitial lung disease in amyopathic dermatomyositis, dermatomyositis and polymyositis. Eur. Respir. J. 2003, 22, 245–250. [Google Scholar] [CrossRef] [Green Version]
- Chan, C.; Ryerson, C.J.; Dunne, J.V.; Wilcox, P.G. Demographic and clinical predictors of progression and mortality in connective tissue disease-associated interstitial lung disease: A retrospective cohort study. BMC Pulm. Med. 2019, 19, 192. [Google Scholar] [CrossRef]
- Md Yusof, M.Y.; Kabia, A.; Darby, M.; Lettieri, G.; Beirne, P.; Vital, E.M.; Dass, S.; Emery, P. Effect of rituximab on the progression of rheumatoid arthritis-related interstitial lung disease: 10 years’ experience at a single centre. Rheumatology (Oxford) 2017, 56, 1348–1357. [Google Scholar] [CrossRef] [Green Version]
- Saketkoo, L.A.; Espinoza, L.R. Rheumatoid arthritis interstitial lung disease: Mycophenolate mofetil as an antifibrotic and disease-modifying antirheumatic drug. Arch. Intern. Med. 2008, 168, 1718–1719. [Google Scholar]
- Oldham, J.M.; Lee, C.; Valenzi, E.; Witt, L.J.; Adegunsoye, A.; Hsu, S.; Chen, L.; Montner, S.; Chung, J.H.; Noth, I.; et al. Azathioprine response in patients with fibrotic connective tissue disease-associated interstitial lung disease. Respir. Med. 2016, 121, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Barnes, H.; Holland, A.E.; Westall, G.P.; Goh, N.S.; Glaspole, I.N. Cyclophosphamide for connective tissue disease-associated interstitial lung disease. Cochrane Database Syst. Rev. 2018, 1, Cd010908. [Google Scholar] [CrossRef]
- Distler, O.; Brown, K.K.; Distler, J.H.W.; Assassi, S.; Maher, T.M.; Cottin, V.; Varga, J.; Coeck, C.; Gahlemann, M.; Sauter, W.; et al. Design of a randomised, placebo-controlled clinical trial of nintedanib in patients with systemic sclerosis-associated interstitial lung disease (SENSCIS™). Clin. Exp. Rheumatol. 2017, 35 (Suppl. S106), 75–81. [Google Scholar]
- Flaherty, K.R.; Wells, A.U.; Cottin, V.; Devaraj, A.; Walsh, S.L.F.; Inoue, Y.; Richeldi, L.; Kolb, M.; Tetzlaff, K.; Stowasser, S.; et al. Nintedanib in Progressive Fibrosing Interstitial Lung Diseases. N. Engl. J. Med. 2019, 381, 1718–1727. [Google Scholar] [CrossRef] [Green Version]
- Ibfelt, E.H.; Jacobsen, R.K.; Kopp, T.I.; Cordtz, R.L.; Jakobsen, A.S.; Seersholm, N.; Shaker, S.B.; Dreyer, L. Methotrexate and risk of interstitial lung disease and respiratory failure in rheumatoid arthritis: A nationwide population-based study. Rheumatology (Oxford) 2020, 60, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Kiely, P.; Busby, A.D.; Nikiphorou, E.; Sullivan, K.; Walsh, D.A.; Creamer, P.; Dixey, J.; Young, A. Is incident rheumatoid arthritis interstitial lung disease associated with methotrexate treatment? Results from a multivariate analysis in the ERAS and ERAN inception cohorts. BMJ Open 2019, 9, e028466. [Google Scholar] [CrossRef] [Green Version]
- Cubero, C.C.; Carmona, E.C.; Casasempere, P.V. Systematic review of the impact of drugs on diffuse interstitial lung disease associated with rheumatoid arthritis. Reumatol. Clín. 2020, 17, 504–513. [Google Scholar]
- Narváez, J.; Robles-Pérez, A.; Molina-Molina, M.; Vicens-Zygmunt, V.; Luburich, P.; Yañez, M.A.; Alegre, J.J.; Nolla, J.M. Real-world clinical effectiveness of rituximab rescue therapy in patients with progressive rheumatoid arthritis-related interstitial lung disease. Semin. Arthritis Rheum. 2020, 50, 902–910. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Díaz, C.; Loricera, J.; Castañeda, S.; López-Mejías, R.; Ojeda-García, C.; Olivé, A.; Rodríguez-Muguruza, S.; Carreira, P.E.; Pérez-Sandoval, T.; Retuerto, M.; et al. Abatacept in patients with rheumatoid arthritis and interstitial lung disease: A national multicenter study of 63 patients. Semin. Arthritis Rheum. 2018, 48, 22–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Díaz, C.; Castañeda, S.; Melero-González, R.B.; Ortiz-Sanjuán, F.; Juan-Mas, A.; Carrasco-Cubero, C.; Casafont-Solé, I.; Olivé, A.; Rodríguez-Muguruza, S.; Almodóvar-González, R.; et al. Abatacept in interstitial lung disease associated with rheumatoid arthritis: National multicenter study of 263 patients. Rheumatology (Oxford) 2020, 59, 3906–3916. [Google Scholar] [CrossRef]
- Manfredi, A.; Cassone, G.; Furini, F.; Gremese, E.; Venerito, V.; Atzeni, F.; Arrigoni, E.; Della Casa, G.; Cerri, S.; Govoni, M.; et al. Tocilizumab therapy in rheumatoid arthritis with interstitial lung disease: A multicenter retrospective study. Intern. Med. J. 2020, 50, 1085–1090. [Google Scholar] [CrossRef]
- Bosello, S.L.; De Luca, G.; Rucco, M.; Berardi, G.; Falcione, M.; Danza, F.M.; Pirronti, T.; Ferraccioli, G. Long-term efficacy of B cell depletion therapy on lung and skin involvement in diffuse systemic sclerosis. Semin. Arthritis Rheum. 2015, 44, 428–436. [Google Scholar] [CrossRef]
- Marie, I.; Dominique, S.; Janvresse, A.; Levesque, H.; Menard, J.F. Rituximab therapy for refractory interstitial lung disease related to antisynthetase syndrome. Respir. Med. 2012, 106, 581–587. [Google Scholar] [CrossRef] [Green Version]
- Mena-Vázquez, N.; Godoy-Navarrete, F.J.; Manrique-Arija, S.; Aguilar-Hurtado, M.C.; Romero-Barco, C.M.; Ureña-Garnica, I.; Espildora, F.; Añón-Oñate, I.; Pérez-Albaladejo, L.; Gomez-Cano, C.; et al. Non-anti-TNF biologic agents are associated with slower worsening of interstitial lung disease secondary to rheumatoid arthritis. Clin. Rheumatol. 2021, 40, 133–142. [Google Scholar] [CrossRef]
- Mena-Vázquez, N.; Rojas-Gimenez, M.; Romero-Barco, C.M.; Manrique-Arija, S.; Francisco, E.; Aguilar-Hurtado, M.C.; Añón-Oñate, I.; Pérez-Albaladejo, L.; Ortega-Castro, R.; Godoy-Navarrete, F.J.; et al. Predictors of Progression and Mortality in Patients with Prevalent Rheumatoid Arthritis and Interstitial Lung Disease: A Prospective Cohort Study. J. Clin. Med. 2021, 10, 874. [Google Scholar] [CrossRef] [PubMed]
- Khanna, D.; Lin, C.J.F.; Furst, D.E.; Wagner, B.; Zucchetto, M.; Raghu, G.; Martinez, F.J.; Goldin, J.; Siegel, J.; Denton, C.P. Long-Term Safety and Efficacy of Tocilizumab in Early Systemic Sclerosis-Interstitial Lung Disease: Open Label Extension of a Phase 3 Randomized Controlled Trial. Am. J. Respir. Crit. Care Med. 2021. Am. J. Respir. Crit. Care Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Smolen, J.S.; Landewé, R.; Bijlsma, J.; Burmester, G.; Chatzidionysiou, K.; Dougados, M.; Nam, J.; Ramiro, S.; Voshaar, M.; van Vollenhoven, R.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2016 update. Ann. Rheum. Dis. 2017, 76, 960–977. [Google Scholar] [CrossRef] [PubMed]
- Yates, M.; Watts, R.A.; Bajema, I.M.; Cid, M.C.; Crestani, B.; Hauser, T.; Hellmich, B.; Holle, J.U.; Laudien, M.; Little, M.A.; et al. EULAR/ERA-EDTA recommendations for the management of ANCA-associated vasculitis. Ann. Rheum. Dis. 2016, 75, 1583–1594. [Google Scholar] [CrossRef] [Green Version]
- Matteson, E.L.; Bongartz, T.; Ryu, J.H.; Crowson, C.S.; Hartman, T.E.; Dellaripa, P.F. Open-Label, Pilot Study of the Safety and Clinical Effects of Rituximab in Patients with Rheumatoid Arthritis-Associated Interstitial Pneumonia. Open J. Rheumatol. Autoimmune Dis. 2012, 2, 53. [Google Scholar] [CrossRef] [Green Version]
- Fui, A.; Bergantini, L.; Selvi, E.; Mazzei, M.A.; Bennett, D.; Pieroni, M.G.; Rottoli, P.; Bargagli, E. Rituximab therapy in interstitial lung disease associated with rheumatoid arthritis. Intern. Med. J. 2020, 50, 330–336. [Google Scholar] [CrossRef]
- Robles-Perez, A.; Dorca, J.; Castellví, I.; Nolla, J.M.; Molina-Molina, M.; Narváez, J. Rituximab effect in severe progressive connective tissue disease-related lung disease: Preliminary data. Rheumatol. Int. 2020, 40, 719–726. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Bohan, A.; Peter, J.B. Polymyositis and dermatomyositis (first of two parts). N. Engl. J. Med. 1975, 292, 344–347. [Google Scholar] [CrossRef]
- Bohan, A.; Peter, J.B. Polymyositis and dermatomyositis (second of two parts). N. Engl. J. Med. 1975, 292, 403–407. [Google Scholar] [CrossRef] [Green Version]
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E., Jr.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef] [PubMed]
- Moazedi-Fuerst, F.C.; Kielhauser, S.M.; Brickmann, K.; Hermann, J.; Lutfi, A.; Meilinger, M.; Brezinschek, H.P.; Graninger, W.B. Rituximab for systemic sclerosis: Arrest of pulmonary disease progression in five cases. Results of a lower dosage and shorter interval regimen. Scand. J. Rheumatol. 2014, 43, 257–258. [Google Scholar] [CrossRef] [Green Version]
- Wallace, B.; Vummidi, D.; Khanna, D. Management of connective tissue diseases associated interstitial lung disease: A review of the published literature. Curr. Opin. Rheumatol. 2016, 28, 236–245. [Google Scholar] [CrossRef]
- Nurmi, H.M.; Purokivi, M.K.; Kärkkäinen, M.S.; Kettunen, H.P.; Selander, T.A.; Kaarteenaho, R.L. Are risk predicting models useful for estimating survival of patients with rheumatoid arthritis-associated interstitial lung disease? BMC Pulm. Med. 2017, 17, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xing, N.S.; Fan, G.Z.; Yan, F.; Liu, Y.P.; Zhang, R. Safety and efficacy of rituximab in connective tissue disease-associated interstitial lung disease: A systematic review and meta-analysis. Int. Immunopharmacol. 2021, 95, 107524. [Google Scholar] [CrossRef] [PubMed]
- Hartung, W.; Maier, J.; Pfeifer, M.; Fleck, M. Effective treatment of rheumatoid arthritis-associated interstitial lung disease by B-cell targeted therapy with rituximab. Case Rep. Immunol. 2012, 2012, 272303. [Google Scholar] [CrossRef]
- Tashkin, D.P.; Roth, M.D.; Clements, P.J.; Furst, D.E.; Khanna, D.; Kleerup, E.C.; Goldin, J.; Arriola, E.; Volkmann, E.R.; Kafaja, S.; et al. Mycophenolate mofetil versus oral cyclophosphamide in scleroderma-related interstitial lung disease (SLS II): A randomised controlled, double-blind, parallel group trial. Lancet Respir. Med. 2016, 4, 708–719. [Google Scholar] [CrossRef] [Green Version]
- Liossis, S.N.; Bounas, A.; Andonopoulos, A.P. Mycophenolate mofetil as first-line treatment improves clinically evident early scleroderma lung disease. Rheumatology (Oxford) 2006, 45, 1005–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simeón-Aznar, C.P.; Fonollosa-Plá, V.; Tolosa-Vilella, C.; Selva-O’Callaghan, A.; Solans-Laqué, R.; Vilardell-Tarrés, M. Effect of mycophenolate sodium in scleroderma-related interstitial lung disease. Clin. Rheumatol. 2011, 30, 1393–1398. [Google Scholar] [CrossRef]
- Mendoza, F.A.; Nagle, S.J.; Lee, J.B.; Jimenez, S.A. A prospective observational study of mycophenolate mofetil treatment in progressive diffuse cutaneous systemic sclerosis of recent onset. J. Rheumatol. 2012, 39, 1241–1247. [Google Scholar] [CrossRef] [Green Version]
- Volkmann, E.R.; Tashkin, D.P.; Li, N.; Roth, M.D.; Khanna, D.; Hoffmann-Vold, A.M.; Kim, G.; Goldin, J.; Clements, P.J.; Furst, D.E.; et al. Mycophenolate Mofetil Versus Placebo for Systemic Sclerosis-Related Interstitial Lung Disease: An Analysis of Scleroderma Lung Studies I and II. Arthritis Rheumatol. 2017, 69, 1451–1460. [Google Scholar] [CrossRef] [Green Version]
- Naidu, G.S.R.S.N.K.; Sharma, S.K.; Adarsh, M.B.; Dhir, V.; Sinha, A.; Dhooria, S.; Jain, S. Effect of mycophenolate mofetil (MMF) on systemic sclerosis-related interstitial lung disease with mildly impaired lung function: A double-blind, placebo-controlled, randomized trial. Rheumatol. Int. 2020, 40, 207–216. [Google Scholar] [CrossRef]
- Fischer, A.; Brown, K.K.; Du Bois, R.M.; Frankel, S.K.; Cosgrove, G.P.; Fernandez-Perez, E.R.; Huie, T.J.; Krishnamoorthy, M.; Meehan, R.T.; Olson, A.L.; et al. Mycophenolate mofetil improves lung function in connective tissue disease-associated interstitial lung disease. J. Rheumatol. 2013, 40, 640–646. [Google Scholar] [CrossRef]
- Swigris, J.J.; Olson, A.L.; Fischer, A.; Lynch, D.A.; Cosgrove, G.P.; Frankel, S.K.; Meehan, R.T.; Brown, K.K. Mycophenolate mofetil is safe, well tolerated, and preserves lung function in patients with connective tissue disease-related interstitial lung disease. Chest 2006, 130, 30–36. [Google Scholar] [CrossRef]
- Fraticelli, P.; Fischetti, C.; Salaffi, F.; Carotti, M.; Mattioli, M.; Pomponio, G.; Gabrielli, A. Combination therapy with rituximab and mycophenolate mofetil in systemic sclerosis. A single-centre case series study. Clin. Exp. Rheumatol. 2018, 36 (Suppl. S113), 142–145. [Google Scholar]
- Narváez, J.; LLuch, J.; Molina-Molina, M.; Vicens-Zygmunt, V.; Luburich, P.; Yañez, M.A.; Nolla, J.M. Rituximab as a rescue treatment added on mycophenolate mofetil background therapy in progressive systemic sclerosis associated interstitial lung disease unresponsive to conventional immunosuppression. Semin. Arthritis Rheum. 2020, 50, 977–987. [Google Scholar] [CrossRef]
- Bejan-Angoulvant, T.; Naccache, J.M.; Caille, A.; Borie, R.; Nunes, H.; Ferreira, M.; Cadranel, J.; Crestani, B.; Cottin, V.; Marchand-Adam, S.; et al. Evaluation of efficacy and safety of rituximab in combination with mycophenolate mofetil in patients with nonspecific interstitial pneumonia non-responding to a first-line immunosuppressive treatment (EVER-ILD): A double-blind placebo-controlled randomized trial. Respir. Med. Res. 2020, 78, 100770. [Google Scholar]
- Andersson, H.; Sem, M.; Lund, M.B.; Aaløkken, T.M.; Günther, A.; Walle-Hansen, R.; Garen, T.; Molberg, Ø. Long-term experience with rituximab in anti-synthetase syndrome-related interstitial lung disease. Rheumatology (Oxford) 2015, 54, 1420–1428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duarte, A.C.; Cordeiro, A.; Fernandes, B.M.; Bernardes, M.; Martins, P.; Cordeiro, I.; Santiago, T.; Seixas, M.I.; Ribeiro, A.R.; Santos, M.J. Rituximab in connective tissue disease-associated interstitial lung disease. Clin. Rheumatol. 2019, 38, 2001–2009. [Google Scholar] [CrossRef]
- Lee, Y.H.; Cha, S.I.; Lim, J.K.; Yoo, S.S.; Lee, S.Y.; Lee, J.; Kim, C.H.; Park, J.Y. Clinical and radiological features of pulmonary tuberculosis in patients with idiopathic pulmonary fibrosis. Respir. Investig. 2019, 57, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Langlois, V.; Gillibert, A.; Uzunhan, Y.; Chabi, M.L.; Hachulla, E.; Landon-Cardinal, O.; Mariampillai, K.; Champtiaux, N.; Nunes, H.; Benveniste, O.; et al. Rituximab and Cyclophosphamide in Antisynthetase Syndrome-related Interstitial Lung Disease: An Observational Retrospective Study. J. Rheumatol. 2020, 47, 1678–1686. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Variable | Total n = 37 | RA n = 19 | SS n = 14 | IM n = 4 | p Value |
|---|---|---|---|---|---|
| Epidemiological characteristics | |||||
| Female sex, n (%) | 27 (73.0) | 13 (68.4) | 11 (78.6) | 3 (75.0) | 0.806 |
| Age in years, mean (SD) | 62.8 (9.9) | 67.7 (9.7) | 57.9 (7.9) | 56.6 (5.5) | 0.001 |
| Caucasian race, n (%) | 36 (97.3) | 19 (100.0) | 13 (92.9) | 4 (100.0) | 0.430 |
| Clinical–analytical characteristics | |||||
| Smoking | 0.147 | ||||
| Never smoked, n (%) | 20 (54.1) | 9 (47.4) | 7 (50.0) | 4 (100.0) | |
| Smoked at some stage, n (%) | 17 (45.9) | 10 (52.6) | 7 (50.0) | 0 (0.0) | |
| Duration of CTD, months, median (IQR) | 107.8 (49.5–188.8) | 151.0 (8.0–240.5) | 89.6 (51.3–184.4) | 35.1 (25.1–49.0) | 0.017 |
| Duration of ILD, months, median (IQR) | 65.4 (31.1–110.3) | 82.2 (37.4–120.1) | 64.5 (35.5–107.1) | 25.9 (25.0–36.0) | 0.136 |
| RF-positive (>10) n (%) | 19 (51.4) | 19 (100.0) | 0 (0.0) | 0 (0.0) | <0.001 |
| ACPA (<20), n (%) | 18 (48.6) | 18 (94.7) | 0 (0.0) | 0 (0.0) | <0.001 |
| ANA-positive, n (%) | 24 (64.9) | 6 (31.6) | 14 (100.0) | 4 (100.0) | <0.001 |
| Anti-scl70, n (%) | 7 (18.9) | 0 (0.0) | 7 (50.0) | 0 (0.0) | <0.001 |
| Anticentromere, n (%) | 3 (9.0) | 0 (0,0) | 3 (21,4) | 0 (0,0) | 0.156 |
| Anti-RNA polymerase 3, n (%) | 1 (2.7) | 0 (0.0) | 1 (7.1) | 0 (0.0) | 0.430 |
| Anti Ku, n (%) | 1 (2.7) | 0 (0.0) | 1 (7.1) | 0 (0.0) | 0.430 |
| Anti-PL7, n (%) | 2 (5.4) | 0 (0.0) | 0 (0.0) | 2 (50.0) | <0.001 |
| Anti-EJ, n (%) | 1 (2.7) | 0 (0.0) | 0 (0.0) | 1 (25.0) | 0.014 |
| Anti-TIF, n (%) | 1 (2.7) | 0 (0.0) | 0 (0.0) | 1 (25.0) | 0.014 |
| Treatment | |||||
| Time to initiation of rituximab *, median (IRQ) | 12.0 (6.5–48.2) | 25.1 (7.0–57.6) | 11.4 (3.9–43.6) | 7.4 (7.0–10.4) | 0.455 |
| Duration of treatment with rituximab, median (IQR) ** | 38.2 (23.4–69.9) | 45.3 (22.2–79.9) | 52.5 (24.7–63.3) | 22.8 (17.7–36.2) | 0.291 |
| Combined with csDMARDs, n (%) | 15 (40.5) | 9 (47.4) | 5 (35.7) | 1 (25.0) | 0.637 |
| Methotrexate, n (%) | 5 (13.5) | 2 (10.5) | 3 (21.4) | 0 (0.0) | 0.468 |
| Leflunomide, n (%) | 2 (5.4) | 2 (10.5) | 0 (0.0) | 0 (0.0) | 0.367 |
| Sulfasalazine, n (%) | 1 (2.7) | 1 (5.3) | 0 (0.0) | 0 (0.0) | 0.615 |
| Hydroxychloroquine, n (%) | 7 (18.9) | 4 (21.1) | 2 (14.3) | 1 (25.0) | 0.840 |
| Combination with immunosuppressants, n (%) | 20 (54.1) | 7 (36.8) | 9 (64.3) | 4 (100.0) | 0.044 |
| Mycophenolate, n (%) | 19 (51.4) | 6 (31.6) | 9 (64.3) | 4 (100.0) | 0.021 |
| Azathioprine, n (%) | 1 (2.7) | 1 (5.3) | 0 (0.0) | 0 (0.0) | 0.615 |
| Corticosteroids, n (%) | 25 (67.6) | 14 (73.7) | 7 (50.0) | 4 (100.0) | 0.121 |
| Doses of corticosteroids, median (IQR) | 5.0 (0.0–10.0) | 5.0 (0.0–10.0) | 2.5 (0.0–7.5) | 10.0 (8.1–10.5) | 0.519 |
| Variable | Total n = 37 | RA n = 19 | SS n = 14 | IM n = 4 | p Value |
|---|---|---|---|---|---|
| Infections, n (%) | 29 (78.4) | 15 (78.9) | 11 (78.6) | 3 (75.0) | 0.985 |
| Respiratory infection, n (%) | 26 (70.3) | 13 (68.4) | 10 (71.4) | 3 (75.0) | 0.959 |
| Other infections, n (%) | 10 (27.0) | 5 (26.3) | 4 (28.6) | 1(25.0) | 0.980 |
| Herpes simplex labialis, n (%) | 2 (5.4) | 1 (5.2) | 0 (0.0) | 1 (25.0) | 0.333 |
| Cutaneous involvement, n (%) | 5 (13.5) | 2 (10.5) | 3 (21.4) | 0 (0.0) | 0.401 |
| Urinary tract infection, n (%) | 5 (13.5) | 3 (15.7) | 1 (7.1) | 1 (25.0) | 0.560 |
| Hospitalization, n (%) | 16 (43.2) | 10 (52.6) | 5 (35.7) | 1 (25.0) | 0.461 |
| Reasons for hospitalization | 0.360 | ||||
| Progression of ILD, n (%) | 10 (27.0) | 7 (36.8) | 3 (21.4) | 0 (0.0) | |
| Respiratory infection, n (%) | 14 (37.8) | 7 (36.8) | 6 (42.8) | 1 (25.0) | |
| Mortality, n (%) | 7 (18.9) | 6 (31.6) | 1 (7.1) | 0 (0.0) | 0.123 |
| Variable | Total n = 37 | RA n = 19 | SS n = 14 | IM n = 4 | p Value | |
|---|---|---|---|---|---|---|
| Outcome * | 0.179 | |||||
| Improvement, n (%) | Final | 6 (16.2) | 1 (5.3) | 4 (28.6) | 1 (25.0) | |
| Stabilization, n (%) | Final | 17 (45.9) | 9 (47.4) | 5 (35.7) | 3 (75.0) | |
| Worsening, n (%) | Final | 7 (18.9) | 3 (15.8) | 4 (28.6) | 0 (0.0) | |
| Death, n (%) | Final | 7 (18.9) | 6 (31.6) | 1 (7.1) | 0 (0.0) | |
| Pulmonary function tests | ||||||
| FVC, mean (SD) | Baseline | 72.2 (21.3) | 69.1 (15.0) | 71.6(21.7) | 79.0 (15.0) | 0.644 |
| Final | 70.8 (18.6) | 67.4 (20.2) | 70.7(25.2) | 81.5 (10.0) | 0.312 | |
| FVC < 80%, n (%) | Baseline | 24 (64.9) | 12 (63.2) | 11 (78.6) | 1 (25.0) | 0.138 |
| Final | 25(67.6) | 15 (78.9) | 9 (64.3) | 1 (25.0) | 0.105 | |
| FEV1, mean (SD) | Baseline | 73.0 (18.8) | 69.8 (16.0) | 76.9 (24.9) | 76.2 (7.5) | 0.570 |
| Final | 70.2 (18.7) | 67.1 (19.9) | 72.7 (19.7) | 78.0 (8.0) | 0.516 | |
| DLCO-SB, mean (SD) | Baseline | 55.9 (15.7) | 56.2 (17.7) | 52.8 (15.6) | 58.0 (5.0) | 0.935 |
| Final | 52.2 (17.0) | 53.8 (19.4) | 48.3 (15.2) | 57.1 (4.0) | 0.577 | |
| HRCT pattern | ||||||
| Radiologic type | 0.011 | |||||
| UIP, n (%) | Baseline | 18 (48.6) | 14 (73.7) | 4 (28.6) | 0 (0.0) | |
| Final | 18 (48.6) | 14 (73.7) | 4 (28.6) | 0 (0.0) | ||
| NSIP, n (%) | Baseline | 18 (48.6) | 4 (21.1) | 10 (71.4) | 4 (100.0) | |
| Final | 18 (48.6) | 4 (21.1) | 10 (71.4) | 4 (100.0) | ||
| Fibrotic NSIP, n (%) | Baseline | 1 (2.7) | 1 (5.3) | 0 (0.0) | 0 (0.0) | |
| Final | 1 (2.7) | 1 (5.3) | 0 (0.0) | 0 (0.0) | ||
| Progress on HRCT | 0.142 | |||||
| Progression, n (%) | Final | 14 (37.8) | 9 (47.4) | 5 (35.7) | 0 (0.0) | |
| Stabilization, n (%) | Final | 16 (43.2) | 9 (47.4) | 5 (35.7) | 2 (50.0) | |
| Improvement, n (%) | Final | 7 (18.9) | 1 (5.3) | 4 (28.6) | 2 (50.0) | |
| Variable | Univariate HR (95% CI) | Multivariate HR (95% CI) | p Value |
|---|---|---|---|
| Age in years | 1.007 (0.94–1.06) | ||
| Sex, male | 0.756 (0.21–2.72) | ||
| Current or previous history of smoking | 2.074 (0.77–6.04) | ||
| Radiological pattern, UIP | 1.200 (0.38–3.73) | ||
| Progression of ILD, months | 1.001 (0.99–1.01) | ||
| Baseline FVC | 0.956 (0.92–0.99) | ||
| Baseline DLCO-SB | 0.949 (0.91–0.98) | 0.904 (0.83–0.98) | 0.015 |
| Time to initiation of rituximab, months | 1.010 (1.00–1.01) | 1.011 (1.00–1.02) | 0.029 |
| csDMARDs | 0.877 (0.29–2.57) | ||
| Combination with mycophenolate | 0.252 (0.06–0.92) | 0.202 (0.04–0.88) | 0.034 |
| Corticosteroids | 0.667 (0.21–2.12) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mena-Vázquez, N.; Redondo-Rodríguez, R.; Rojas-Gimenez, M.; Romero-Barco, C.M.; Manrique-Arija, S.; Ortega-Castro, R.; Hidalgo Conde, A.; Arnedo Díez de los Ríos, R.; Cabrera César, E.; Espildora, F.; et al. Efficacy and Safety of Rituximab in Autoimmune Disease—Associated Interstitial Lung Disease: A Prospective Cohort Study. J. Clin. Med. 2022, 11, 927. https://doi.org/10.3390/jcm11040927
Mena-Vázquez N, Redondo-Rodríguez R, Rojas-Gimenez M, Romero-Barco CM, Manrique-Arija S, Ortega-Castro R, Hidalgo Conde A, Arnedo Díez de los Ríos R, Cabrera César E, Espildora F, et al. Efficacy and Safety of Rituximab in Autoimmune Disease—Associated Interstitial Lung Disease: A Prospective Cohort Study. Journal of Clinical Medicine. 2022; 11(4):927. https://doi.org/10.3390/jcm11040927
Chicago/Turabian StyleMena-Vázquez, Natalia, Rocío Redondo-Rodríguez, Marta Rojas-Gimenez, Carmen María Romero-Barco, Sara Manrique-Arija, Rafaela Ortega-Castro, Ana Hidalgo Conde, Rocío Arnedo Díez de los Ríos, Eva Cabrera César, Francisco Espildora, and et al. 2022. "Efficacy and Safety of Rituximab in Autoimmune Disease—Associated Interstitial Lung Disease: A Prospective Cohort Study" Journal of Clinical Medicine 11, no. 4: 927. https://doi.org/10.3390/jcm11040927
APA StyleMena-Vázquez, N., Redondo-Rodríguez, R., Rojas-Gimenez, M., Romero-Barco, C. M., Manrique-Arija, S., Ortega-Castro, R., Hidalgo Conde, A., Arnedo Díez de los Ríos, R., Cabrera César, E., Espildora, F., Aguilar-Hurtado, M. C., Añón-Oñate, I., Pérez-Albaladejo, L., Abarca-Costalago, M., Ureña-Garnica, I., Velloso-Feijoo, M. L., Irigoyen-Oyarzábal, M. V., & Fernández-Nebro, A. (2022). Efficacy and Safety of Rituximab in Autoimmune Disease—Associated Interstitial Lung Disease: A Prospective Cohort Study. Journal of Clinical Medicine, 11(4), 927. https://doi.org/10.3390/jcm11040927