
Presentation and Prognosis of Primary Expansile and Infiltrative Mucinous Carcinomas of the Ovary
 , , ,
, , ,  , , , , ,
, , , , ,  on behalf of FRANCOGYN Research Group
on behalf of FRANCOGYN Research Group
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design and Study Population
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Variables and Measures
- -
- Intrinsic criteria for each patient: age, parity, and body mass index (BMI, which is weight divided by the square of height, expressed in kg/m2. We used the WHO classification of BMI. Thus, underweight was defined by a BMI <18.5 kg/m2, normal weight: 18.5 < BMI < 25 kg/m2, overweight: 25 < BMI < 30 kg/m2, and obesity by a BMI > 30 kg/m2).
- -
- Presence of type 1 or type 2 diabetes, presence of high blood pressure (HBP), menopausal status and use of menopausal hormone replacement therapy (HRT), smoking status.
- -
- Assessment of potential genetic predisposition: personal and family history of breast, endometrial, colon, or ovarian cancer. A cancer predisposition mutation was also recorded.
- (1)
- At diagnosis:
- -
- ASA anaesthetic score corresponding to (1) normal patient, (2) patient with moderate systemic abnormality, (3) patient with severe systemic abnormality, (4) patient with severe systemic abnormality representing a constant life threat, (5) moribund patient, and (6) patient declared brain dead; weight loss at diagnosis (in kg).
- -
- For biological tests: serum CA 125 level expressed as IU/mL (N < 35 IU/mL), serum CA 19.9 level expressed as IU/mL (N < 37 IU/mL).
- -
- Imaging data at diagnosis.
- (2)
- For initial stage assessment:
- -
- The type of surgery that resulted in a histological diagnosis: laparoscopy alone or combined with concomitant; delayed laparotomy or upfront laparotomy.
- -
- Initial stage of disease according to the 2014 International Federation of Gynecology and Obstetrics (FIGO) and TNM classification (7th edition).
- (a)
- In case of NACT
- -
- The presence of NACT, if applicable, the number of courses before surgery (if applicable) and the different chemotherapy regimens used.
- -
- For biological examinations: serum CA 125 level expressed in IU/mL (N < 35 IU/mL), serum CA 19.9 level expressed in IU/mL (N < 37 IU/mL), after three courses.
- -
- For imaging: a CT scan and/or PET-CT scan after three courses of NAC. with the observed involvement and associated RECIST criteria.
- (b)
- In case of primary cytoreductive surgery (CRS) or interval CRS
- -
- The type of surgery among primary CRS or interval CRS.
- -
- Surgical procedures among right and/or left adnexectomy, total hysterectomy, infundibulopelvic ligament removal, infra-gastric or infra-colic omentectomy.
- -
- Lymph node procedures among: lombo-aortic lymphadenectomy, bilateral pelvic lymphadenectomy, hepatic hilum lymphadenectomy.
- -
- Peritoneal procedures among biopsies or removal of the rectouterine pouch, of the pre-vesical peritoneum, of the right and/or left parieto-colic gutter, resection of the right and/or left diaphragmatic peritoneum, as well as their surface estimated in cm2.
- -
- Digestive procedures among appendectomy, cholecystectomy, recto-sigmoidectomy, right or left colectomy and/or transverse colectomy, bowel resection, splenectomy, hepatic nodule resection, Glisson’s capsule resection, falciform ligament resection, partial gastrectomy.
- -
- Urinary procedures including partial or total cystectomy.
- -
- Other procedures among diaphragmatic resection, fulguration procedures with electric energy, nodule resection (peritoneum, mesentery, mesocolon).
- -
- Bypass or protective procedures among digestive anastomoses, stomas.
- -
- The presence of drains among pleural drain, abdominal drain, nasogastric tube.
- (c)
- In case of adjuvant chemotherapy
- -
- The number of courses after surgery and the different lines of chemotherapy used.
- -
- On the histological reports:
- -
- The tumour size expressed in millimetres.
- -
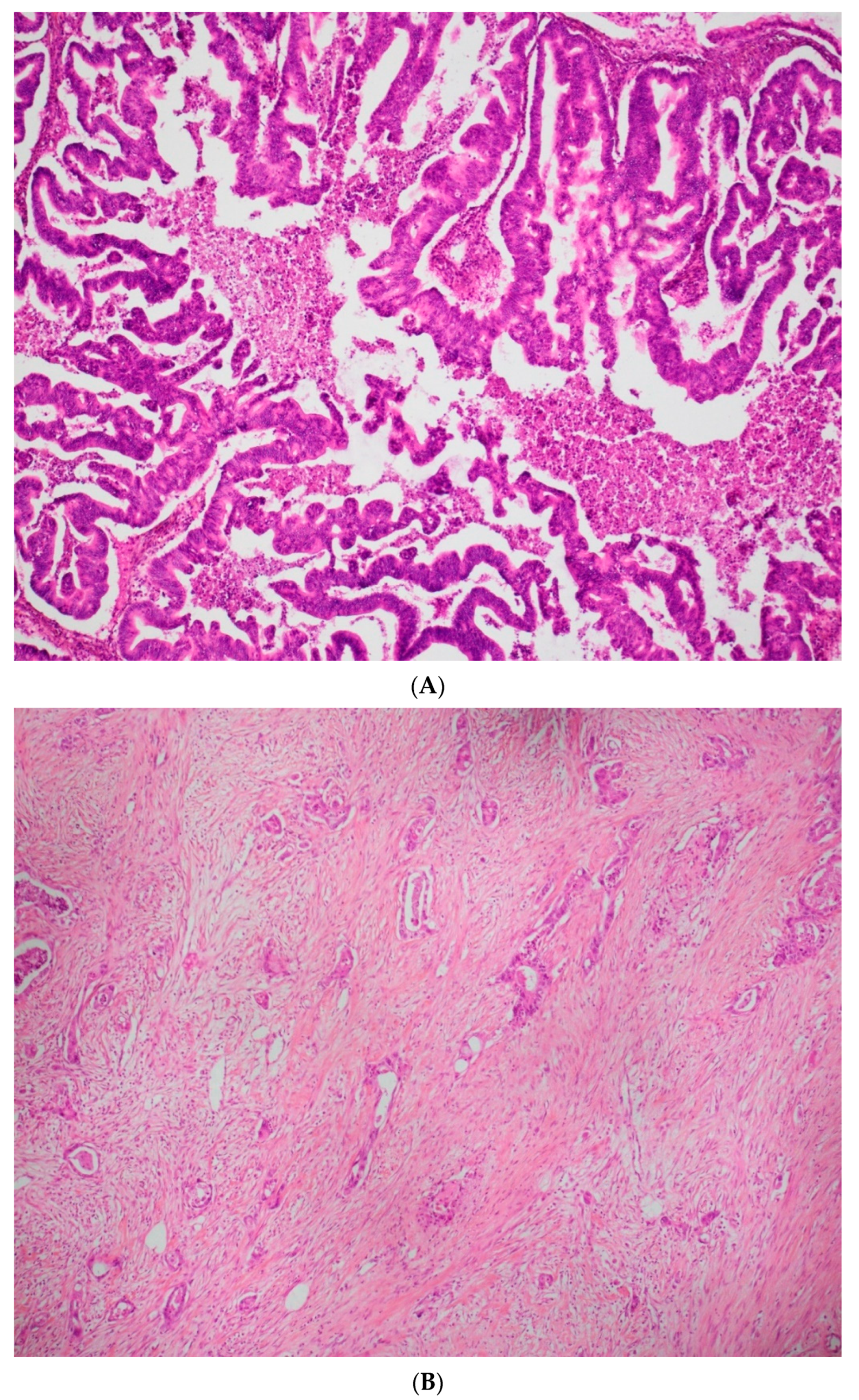
- The histological type of the lesion and its invasion type. Currently, there is no standardized grading system for primary mOC, according to the recommendations of the 2020 World Health Organization classification. The expansile invasive pattern displays marked glandular crowding, with little or absent intervening stroma, creating a labyrinth appearance. Papillary and cribriform areas may be present.
- -
- Tumour extension on the different surgical specimens (ovaries, uterus, tubes, omentum, peritoneal resections, digestive and urinary resections…).
- -
- Immunohistochemical markers identified.
- -
- Presence of lympho-vascular space involvement (LVSI—defined as the presence of tumour cells within the lymphatic or vascular capillaries draining the primary tumour).
- -
- The number of nodes removed, and the number of positive lymph nodes.
- -
- The presence of an associated other histological contingent.
- -
- The presence of an associated borderline contingent.
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Perren, T.J. Mucinous epithelial ovarian carcinoma. Ann. Oncol. 2016, 27, i53–i57. [Google Scholar] [CrossRef] [PubMed]
- Babaier, A.; Ghatage, P. Mucinous Cancer of the Ovary: Overview and Current Status. Diagnostics 2020, 10, 52. [Google Scholar] [CrossRef] [PubMed]
- Marko, J.; Marko, K.I.; Pachigolla, S.L.; Crothers, B.A.; Mattu, R.; Wolfman, D.J. Mucinous Neoplasms of the Ovary: Radiologic-Pathologic Correlation. RadioGraphics 2019, 39, 982–997. [Google Scholar] [CrossRef] [PubMed]
- Ledermann, J.A.; Luvero, D.; Shafer, A.; O’Connor, D.; Mangili, G.; Friedlander, M.; Pfisterer, J.; Mirza, M.R.; Kim, J.-W.; Alexandre, J.; et al. Gynecologic Cancer InterGroup (GCIG) Consensus Review for Mucinous Ovarian Carcinoma. Int. J. Gynecol. Cancer 2014, 24, S14–S19. [Google Scholar] [CrossRef] [PubMed]
- Simons, M.; Bolhuis, T.; De Haan, A.F.; Bruggink, A.H.; Bulten, J.; Massuger, L.F.; Nagtegaal, I.D. A novel algorithm for better distinction of primary mucinous ovarian carcinomas and mucinous carcinomas metastatic to the ovary. Virchows Arch. 2019, 474, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Nasioudis, D.; Chapman-Davis, E.; Witkin, S.S.; Holcomb, K. Prognostic significance of lymphadenectomy and prevalence of lymph node metastasis in clinically-apparent stage I endometrioid and mucinous ovarian carcinoma. Gynecol. Oncol. 2016, 144, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Simons, M.; Ezendam, N.; Bulten, J.; Nagtegaal, I.; Massuger, L. Survival of Patients With Mucinous Ovarian Carcinoma and Ovarian Metastases: A Population-Based Cancer Registry Study. Int. J. Gynecol. Cancer 2015, 25, 1208–1215. [Google Scholar] [CrossRef]
- Lokuhetty, D.; White, V.A.; Cree, I.A. WHO Classification of Tumours of Female Reproductive Organs; International Agency for Research on Cancer (IARC): Lyon, France, 2020. [Google Scholar]
- Muyldermans, K.; Moerman, P.; Amant, F.; Leunen, K.; Neven, P.; Vergote, I. Primary invasive mucinous ovarian carcinoma of the intestinal type: Importance of the expansile versus infiltrative type in predicting recurrence and lymph node metastases. Eur. J. Cancer 2013, 49, 1600–1608. [Google Scholar] [CrossRef]
- Schiavone, M.B.; Herzog, T.J.; Lewin, S.N.; Deutsch, I.; Sun, X.; Burke, W.M.; Wright, J.D. Natural history and outcome of mucinous carcinoma of the ovary. Am. J. Obstet. Gynecol. 2011, 205, 480.e1–480.e8. [Google Scholar] [CrossRef]
- Rosendahl, M.; Haueberg Oester, L.A.; Høgdall, C.K. The Importance of Appendectomy in Surgery for Mucinous Adenocarcinoma of the Ovary. Int. J. Gynecol. Cancer 2017, 27, 430–436. [Google Scholar] [CrossRef]
- Massad, L.S.; Gao, F.; Hagemann, I.; Powell, M. Clinical Outcomes among Women with Mucinous Adenocarcinoma of the Ovary. Gynecol. Obstet. Investig. 2015, 81, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Schmeler, K.M.; Tao, X.; Frumovitz, M.; Deavers, M.T.; Sun, C.C.; Sood, A.K.; Brown, J.; Gershenson, D.M.; Ramirez, P.T. Prevalence of Lymph Node Metastasis in Primary Mucinous Carcinoma of the Ovary. Obstet. Gynecol. 2010, 116, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Gouy, S.; Saidani, M.; Maulard, A.; Faron, M.; Bach-Hamba, S.; Bentivegna, E.; Leary, A.; Pautier, P.; Devouassoux-Shisheboran, M.; Genestie, C.; et al. Staging surgery in early-stage ovarian mucinous tumors according to expansile and infiltrative types. Gynecol. Oncol. Rep. 2017, 22, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Yoshihara, M.; Kajiyama, H.; Tamauchi, S.; Iyoshi, S.; Yokoi, A.; Suzuki, S.; Kawai, M.; Nagasaka, T.; Takahashi, K.; Matsui, S.; et al. Prognostic impact of pelvic and para-aortic lymphadenectomy on clinically-apparent stage I primary mucinous epithelial ovarian carcinoma: A multi-institutional study with propensity score-weighted analysis. Jpn. J. Clin. Oncol. 2020, 50, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Lavoue, V.; Huchon, C.; Akladios, C.; Alfonsi, P.; Bakrin, N.; Ballester, M.; Bendifallah, S.; Bolze, P.; Bonnet, F.; Bourgin, C.; et al. Management of epithelial cancer of the ovary, fallopian tube, and primary peritoneum. Short text of the French Clinical Practice Guidelines issued by FRANCOGYN, CNGOF, SFOG, and GINECO-ARCAGY, and endorsed by INCa. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 236, 214–223. [Google Scholar] [CrossRef]
- Morice, P.; Gouy, S.; Leary, A. Mucinous Ovarian Carcinoma. N. Engl. J. Med. 2019, 380, 1256–1266. [Google Scholar] [CrossRef]
- Jain, A.; Seiden, M.V. Rare epithelial tumors arising in or near the ovary: A review of the risk factors, presentation, and future treatment direction for ovarian clear cell and mucinous carcinoma. Am. Soc. Clin. Oncol. Educ. Book 2013, 33, e200–e204. [Google Scholar] [CrossRef]
- Nasioudis, D.; Albright, B.B.; Ko, E.M.; Haggerty, A.F.; Giuntoli, R.L.; Burger, R.A.; Morgan, M.A.; Latif, N.A. Advanced stage primary mucinous ovarian carcinoma. Where do we stand? Arch. Gynecol. Obstet. 2020, 301, 1047–1054. [Google Scholar] [CrossRef]
- Genestie, C.; Auguste, A.; Al Battal, M.; Scoazec, J.-Y.; Gouy, S.; Lacroix, L.; Morice, P.; Pautier, P.; Leary, A.; Devouassoux-Shisheboran, M. Histological classification of mucinous ovarian tumors: Inter-observer reproducibility, clinical relevance, and role of genetic biomarkers. Virchows Arch. 2020, 478, 885–891. [Google Scholar] [CrossRef]
- Hada, T.; Miyamoto, M.; Ishibashi, H.; Matsuura, H.; Sakamoto, T.; Kakimoto, S.; Iwahashi, H.; Tsuda, H.; Takano, M. Survival and biomarker analysis for ovarian mucinous carcinoma according to invasive patterns: Retrospective analysis and review literature. J. Ovarian Res. 2021, 14, 1–12. [Google Scholar] [CrossRef]
- Zaino, R.J.; Brady, M.F.; Lele, S.M.; Michael, H.; Greer, B.; Bookman, M.A. Advanced stage mucinous adenocarcinoma of the ovary is both rare and highly lethal: A Gynecologic Oncology Group study. Cancer 2011, 117, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Hess, V.; A’Hern, R.; Nasiri, N.; King, D.M.; Blake, P.R.; Barton, D.P.; Shepherd, J.H.; Ind, T.; Bridges, J.; Harrington, K.; et al. Mucinous Epithelial Ovarian Cancer: A Separate Entity Requiring Specific Treatment. J. Clin. Oncol. 2004, 22, 1040–1044. [Google Scholar] [CrossRef] [PubMed]
- Winter, W.E., 3rd; Maxwell, G.L.; Tian, C.; Carlson, J.W.; Ozols, R.F.; Rose, P.G.; Markman, M.; Armstrong, D.K.; Muggia, F.; McGuire, W.P.; et al. Prognostic Factors for Stage III Epithelial Ovarian Cancer: A Gynecologic Oncology Group Study. J. Clin. Oncol. 2007, 25, 3621–3627. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Population (n = 94) | NA |
|---|---|---|
| Age (years) | 56.5 ± 15.4 (18–88) | - |
| BMI (in kg/m2) | 25.1 ± 5.9 (14.5–44) | 9 |
| Weight loss | 14 (15%) | 24 |
| Parity | 3 | |
| 0 | 23 | |
| 1 | 18 | |
| 2 | 28 | |
| 3 | 16 | |
| 4 | 3 | |
| >4 | 3 | |
| ASA | 38 | |
| 0 | 0 | |
| 1 | 27 (29%) | |
| 2 | 22 (23.5%) | |
| 3 | 7 (7.5%) | |
| CT at initial diagnosis | 56 (60%) | 9 |
| Infiltrative (n = 59) | Expansile (n = 35) | NA | p | |
|---|---|---|---|---|
| Age (median in years) | 58 | 57 | 0 | 0.62 |
| Parity (median) | 1 | 2 | 0.07 | |
| Predisposing mutation | 5 | 2 | 1 | |
| FIGO clinical stage at diagnosis | 6 | <0.0001 | ||
| Stage I | 19 | 28 | ||
| Stage II | 0 | 1 | ||
| Stage III | 27 | 3 | ||
| Stage IV | 9 | 0 | ||
| First surgery | 31 (52%) | 34 (97%) | <0.0001 | |
| Type of surgery | 0 | <0.0001 | ||
| Primary cytoreductive surgery | 30 (51%) | 34 (97%) | ||
| Interval cytoreductive surgery | 14 (24%) | 1 (3%) | ||
| Closure cytoreductive surgery | 5(8%) | 0 | ||
| Surgery exploration | 10(17%) | 0 | ||
| Residual disease at end of surgery | 2 | 0.14 | ||
| R0 (complete surgery) | 40 (83%) | 31 (91%) | ||
| R1 (optimal surgery) | 3 (6.5%) | 3 (9%) | ||
| R2 (sub-optimal surgery) | 5 (10.5%) | 0 | ||
| Overall recurrence | 15 (25%) | 2 (6%) | 0.03 |
| Infiltrative (n = 59) | Expansile (n = 35) | NA | p | |
|---|---|---|---|---|
| Capsule rupture | 12 (20%) | 2 (6%) | 0.01 | |
| Lymph node involvement | - | |||
| Pelvic | 7 (12%) | 0 | 0.23 | |
| Para-aortic | 9 (15%) | 0 | 0.10 | |
| Immunohistochemical markers | ||||
| CK7 | 22 | 1 | 0.86 | |
| CK20 | 9 | 11 | 0.03 | |
| WT1 | 6 | 2 | 0.87 | |
| Estrogen receptors | 8 | 1 | 0.26 | |
| Progesterone receptors | 4 | 0 | 0.45 | |
| P53 | 5 | 3 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huin, M.; Lorenzini, J.; Arbion, F.; Carcopino, X.; Touboul, C.; Dabi, Y.; Kerbage, Y.; Costaz, H.; Lecointre, L.; Lavoué, V.; et al. Presentation and Prognosis of Primary Expansile and Infiltrative Mucinous Carcinomas of the Ovary. J. Clin. Med. 2022, 11, 6120. https://doi.org/10.3390/jcm11206120
Huin M, Lorenzini J, Arbion F, Carcopino X, Touboul C, Dabi Y, Kerbage Y, Costaz H, Lecointre L, Lavoué V, et al. Presentation and Prognosis of Primary Expansile and Infiltrative Mucinous Carcinomas of the Ovary. Journal of Clinical Medicine. 2022; 11(20):6120. https://doi.org/10.3390/jcm11206120
Chicago/Turabian StyleHuin, Marine, Jerome Lorenzini, Flavie Arbion, Xavier Carcopino, Cyril Touboul, Yohann Dabi, Yohan Kerbage, Hélène Costaz, Lise Lecointre, Vincent Lavoué, and et al. 2022. "Presentation and Prognosis of Primary Expansile and Infiltrative Mucinous Carcinomas of the Ovary" Journal of Clinical Medicine 11, no. 20: 6120. https://doi.org/10.3390/jcm11206120
APA StyleHuin, M., Lorenzini, J., Arbion, F., Carcopino, X., Touboul, C., Dabi, Y., Kerbage, Y., Costaz, H., Lecointre, L., Lavoué, V., Bolze, P.-A., Huchon, C., Bricou, A., Canlorbe, G., Mimoun, C., Bendifallah, S., Gauthier, T., Body, G., & Ouldamer, L., on behalf of FRANCOGYN Research Group. (2022). Presentation and Prognosis of Primary Expansile and Infiltrative Mucinous Carcinomas of the Ovary. Journal of Clinical Medicine, 11(20), 6120. https://doi.org/10.3390/jcm11206120