
Association between Renal Function at Admission and COVID-19 in-Hospital Mortality in Southern Italy: Findings from the Prospective Multicenter Italian COVOCA Study
 , ,
, ,  , , , ,
, , , ,  ,
,  , , , , ,
, , , , ,  ,
,  ,
,  , ,
, ,  , and add
Show full author list
, and add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Variables (Outcome and Exposure)
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
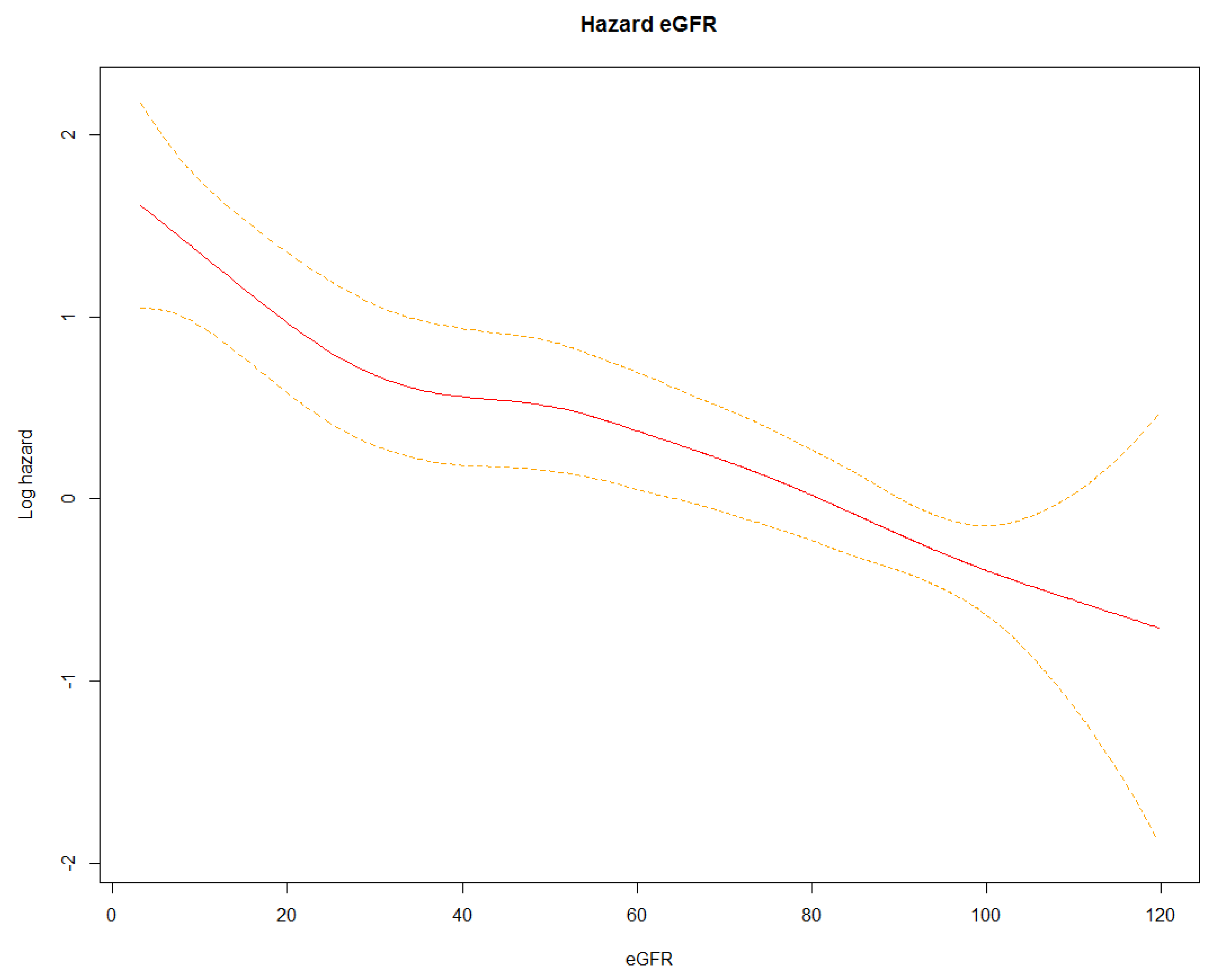
3.2. Mortality Risk and Clinical Prognostic Factors
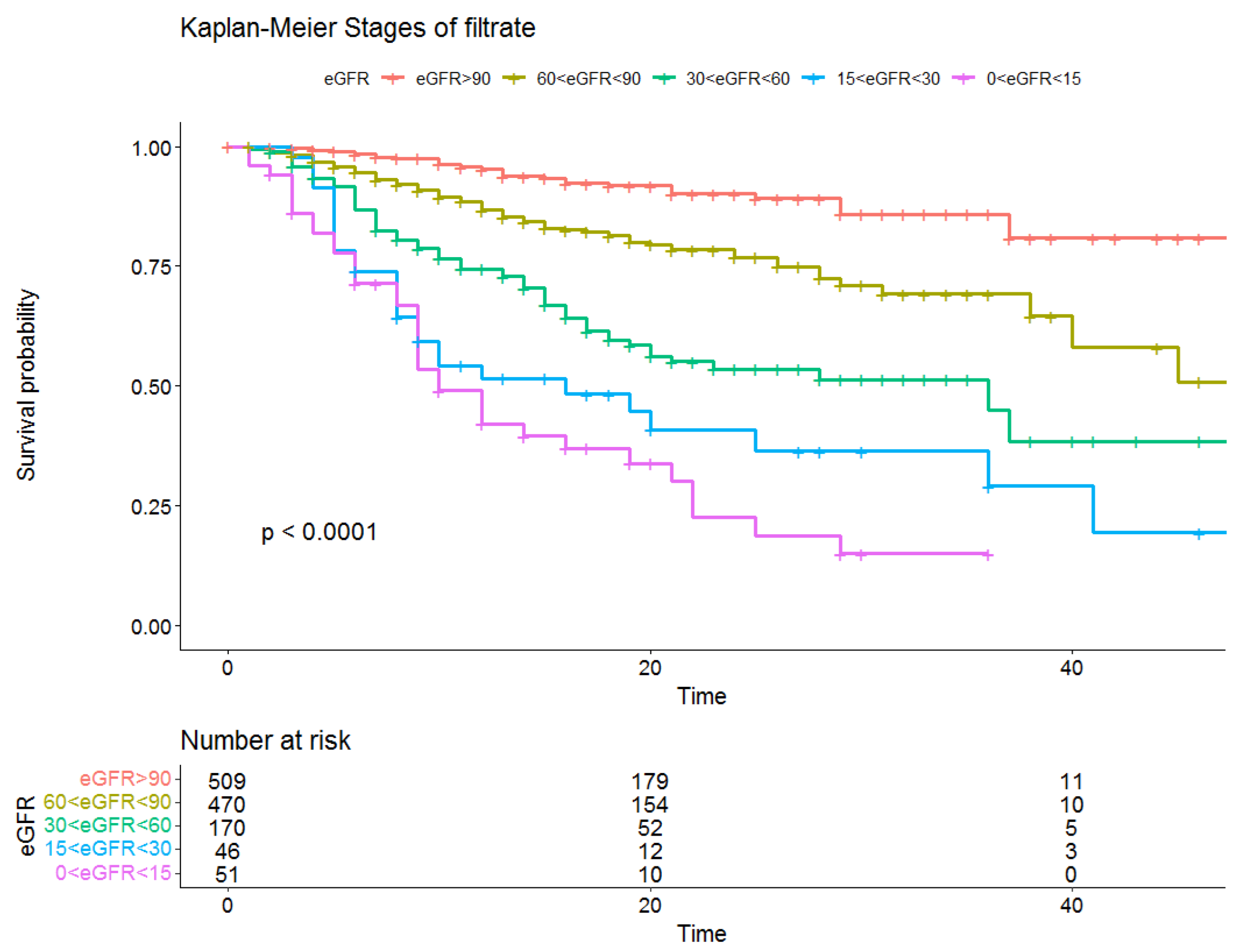
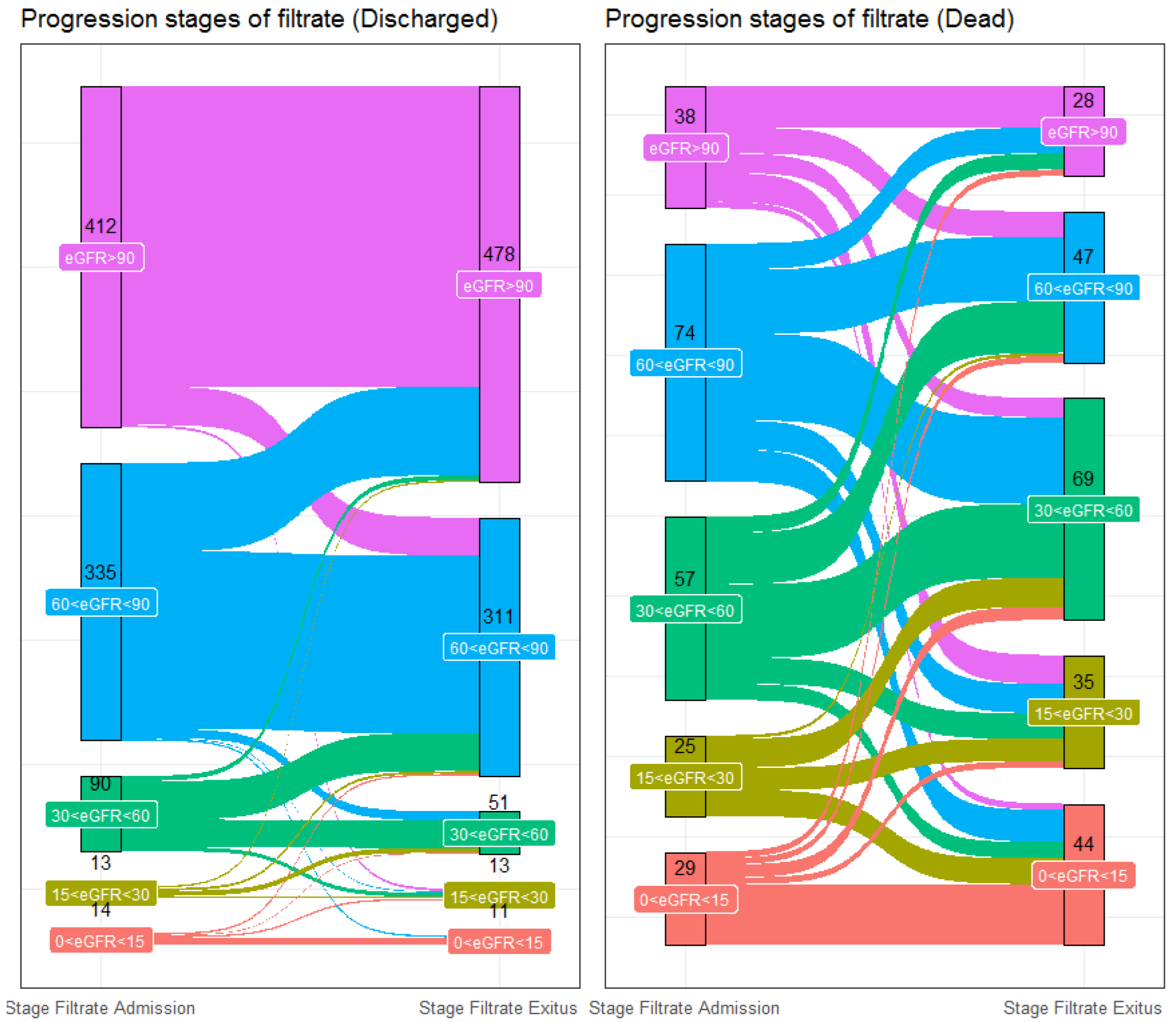
3.3. Evaluation of Admission/Discharged eGFR Stage
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard; World Health Organization: Geneva, Switzerland, 2021. Available online: https://covid19.who.int (accessed on 16 August 2022).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Rotshild, V.; Hirsh-Raccah, B.; Miskin, I.; Muszkat, M.; Matok, I. Comparing the clinical efficacy of COVID-19 vaccines: A systematic review and network meta-analysis. Sci. Rep. 2021, 11, 22777. [Google Scholar] [CrossRef]
- Mattiuzzi, C.; Lippi, G. Efficacy of COVID-19 vaccine booster doses in older people. Eur. Geriatr. Med. 2022, 13, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Meschiari, M.; Cozzi-Lepri, A.; Tonelli, R.; Bacca, E.; Menozzi, M.; Franceschini, E.; Cuomo, G.; Bedini, A.; Volpi, S.; Milic, J.; et al. First and second waves among hospitalised patients with COVID-19 with severe pneumonia: A comparison of 28-day mortality over the 1-year pandemic in a tertiary university hospital in Italy. BMJ Open 2022, 12, e054069. [Google Scholar] [CrossRef]
- Istituto Superiore di Sanità—Istituto Nazionale di Statistica. Report Esteso iss COVID-19: Sorveglianza, Impatto delle Infezioni ed Efficacia Vaccinale. May 2022. Available online: https://www.ISTAT.it/it/archivio/245415 (accessed on 1 August 2022).
- Marik, P.E.; Iglesias, J.; Varon, J.; Kory, P. A scoping review of the pathophysiology of COVID-19. Int. J. Immunopathol. Pharmacol. 2021, 35, 20587384211048026. [Google Scholar] [CrossRef]
- Magro, C.M.; Mulvey, J.; Kubiak, J.; Mikhail, S.; Suster, D.; Crowson, A.N.; Laurence, J.; Nuovo, G. Severe COVID-19: A multifaceted viral vasculopathy syndrome. Ann. Diagn. Pathol. 2021, 50, 151645. [Google Scholar] [CrossRef]
- Magro, C.; Mulvey, J.J.; Berlin, D.; Nuovo, G.; Salvatore, S.; Harp, J.; Baxter-Stoltzfus, A.; Laurence, J. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: A report of five cases. Transl. Res. 2020, 220, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Gralinski, L.E.; Sheahan, T.P.; Morrison, T.E.; Menachery, V.D.; Jensen, K.; Leist, S.R.; Whitmore, A.; Heise, M.T.; Baric, R.S. Complemenat activation contributes to severe acute respiratory syndrome coronavirus pathogenesis. mBio 2018, 9, e01753-18. [Google Scholar] [CrossRef]
- Galiero, R.; Pafundi, P.C.; Simeon, V.; Rinaldi, L.; Perrella, A.; Vetrano, E.; Caturano, A.; Alfano, M.; Beccia, D.; Nevola, R.; et al. Impact of chronic liver disease upon admission on COVID-19 in-hospital mortality: Findings from COVOCA study. PLoS ONE 2020, 15, e0243700. [Google Scholar] [CrossRef]
- Corbett, R.W.; Blakey, S.; Nitsch, D.; Loucaidou, M.; McLean, A.; Duncan, N.; Ashby, D.R.; West London Renal and Transplant Centre. Epidemiology of COVID-19 in an Urban Dialysis Center. J. Am. Soc. Nephrol. 2020, 31, 1815–1823. [Google Scholar] [CrossRef]
- Stevens, P.E.; Levin, A.; Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44 (Suppl. S1), S15–S33, Erratum in Diabetes Care 2021, 44, 2182. [Google Scholar] [CrossRef] [PubMed]
- Galiè, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; VonkNoordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2016, 37, 67–119. [Google Scholar] [CrossRef]
- Holman, N.; Knighton, P.; Kar, P.; O’Keefe, J.; Curley, M.; Weaver, A.; Barron, E.; Bakhai, C.; Khunti, K.; Wareham, N.J.; et al. Risk factors for COVID-19-related mortality in people with type 1 and type 2 diabetes in England: A population-based cohort study. Lancet Diabetes Endocrinol. 2020, 8, 823–833. [Google Scholar] [CrossRef]
- Akbari, A.; Fathabadi, A.; Razmi, M.; Zarifian, A.; Amiri, M.; Ghodsi, A.; Vafadar Moradi, E. Characteristics, risk factors, and outcomes associated with readmission in COVID-19 patients: A systematic review and meta-analysis. Am. J. Emerg. Med. 2022, 52, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Costa, R.; Castagna, A.; Ruotolo, G. COVID-19 and cardiovascular problems in elderly patients: Food for thought. Aging Med. 2021, 4, 146–152. [Google Scholar] [CrossRef]
- Semenzato, L.; Botton, J.; Drouin, J.; Cuenot, F.; Dray-Spira, R.; Weill, A.; Zureik, M. Chronic diseases, health conditions and risk of COVID-19-related hospitalization and in-hospital mortality during the first wave of the epidemic in France: A cohort study of 66 million people. Lancet Reg. Health Eur. 2021, 8, 100158. [Google Scholar] [CrossRef] [PubMed]
- Lim, Z.J.; Subramaniam, A.; Ponnapa Reddy, M.; Blecher, G.; Kadam, U.; Afroz, A.; Billah, B.; Ashwin, S.; Kubicki, M.; Bilotta, F.; et al. Case Fatality Rates for Patients with COVID-19 Requiring Invasive Mechanical Ventilation. A Meta-analysis. Am. J. Respir. Crit. Care Med. 2021, 203, 54–66. [Google Scholar] [CrossRef]
- Pafundi, P.C.; Galiero, R.; Simeon, V.; Rinaldi, L.; Perrella, A.; Vetrano, E.; Caturano, A.; Alfano, M.; Beccia, D.; Nevola, R.; et al. Lack of effect on in-hospital mortality of drugs used during COVID-19 pandemic: Findings of the retrospective multicenter COVOCA study. PLoS ONE 2021, 16, e0256903. [Google Scholar] [CrossRef]
- Ravaglia, F.; Francesconi, P.; Profili, F.; Rosati, A. FP354 Prevalence of chronic kidney disease in Italy: The role of demographic shift towards older age groups. Nephrol. Dial. Transplant. 2018, 33 (Suppl. S1), i150–i151. [Google Scholar] [CrossRef]
- Mancia, G.; Rea, F.; Ludergnani, M.; Apolone, G.; Corrao, G. Renin-Angiotensin-Aldosterone System Blockers and the Risk of Covid-19. N. Engl. J. Med. 2020, 382, 2431–2440. [Google Scholar] [CrossRef] [PubMed]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- ERA-EDTA Council; ERACODA Working Group. Chronic kidney disease is a key risk factor for severe COVID-19: A call to action by the ERA-EDTA. Nephrol. Dial. Transplant. 2021, 36, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, B.O.; Ingebretsen, O.C. The progression of chronic kidney disease: A 10-year population-based study of the effects of gender and age. Kidney Int. 2006, 69, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Imai, E.; Horio, M.; Yamagata, K.; Iseki, K.; Hara, S.; Ura, N.; Kiyohara, Y.; Makino, H.; Hishida, A.; Matsuo, S. Slower decline of glomerular filtration rate in the Japanese general population: A longitudinal 10-year follow-up study. Hypertens. Res. 2008, 31, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, J.P.; Barone, S.; Zahedi, K.; Soleimani, M. Kidney Injury in COVID-19: Epidemiology, Molecular Mechanisms and Potential Therapeutic Targets. Int. J. Mol. Sci. 2022, 23, 2242. [Google Scholar] [CrossRef]
- Lin, W.; Fan, J.; Hu, L.F.; Zhang, Y.; Ooi, J.D.; Meng, T.; Jin, P.; Ding, X.; Peng, L.K.; Song, L.; et al. Single-cell analysis of angiotensin-converting enzyme II expression in human kidneys and bladders reveals a potential route of 2019 novel coronavirus infection. Chin. Med. J. 2021, 134, 935–943. [Google Scholar] [CrossRef]
- Zou, X.; Chen, K.; Zou, J.; Han, P.; Hao, J.; Han, Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front. Med. 2020, 14, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.M.; Zhang, H. Genetic Roadmap for Kidney Involvement of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection. Clin. J. Am. Soc. Nephrol. 2020, 15, 1044–1046. [Google Scholar] [CrossRef]
- Su, H.; Yang, M.; Wan, C.; Yi, L.X.; Tang, F.; Zhu, H.Y.; Yi, F.; Yang, H.C.; Fogo, A.B.; Nie, X.; et al. Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China. Kidney Int. 2020, 98, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Diao, B.; Wang, C.; Wang, R.; Feng, Z.; Zhang, J.; Yang, H.; Tan, Y.; Wang, H.; Wang, C.; Liu, L.; et al. Human kidney is a target for novel severe acute respiratory syndrome coronavirus 2 infection. Nat. Commun. 2021, 12, 2506. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.M.; Phadke, M.; Dai, F.; Simonov, M.; Dahl, N.K.; Kodali, R. Association of AKI-D with Urinary Findings and Baseline eGFR in Hospitalized COVID-19 Patients. Kidney360 2021, 2, 1215–1224. [Google Scholar] [CrossRef] [PubMed]
- Portolés, J.; Marques, M.; López-Sánchez, P.; de Valdenebro, M.; Muñez, E.; Serrano, M.L.; Malo, R.; García, E.; Cuervas, V. Chronic kidney disease and acute kidney injury in the COVID-19 Spanish outbreak. Nephrol. Dial. Transplant. 2020, 35, 1353–1361. [Google Scholar] [CrossRef] [PubMed]
- Gibertoni, D.; Reno, C.; Rucci, P.; Fantini, M.P.; Buscaroli, A.; Mosconi, G.; Rigotti, A.; Giudicissi, A.; Mambelli, E.; Righini, M.; et al. COVID-19 incidence and mortality in non-dialysischronickidneydiseasepatients. PLoS ONE 2021, 16, e0254525. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Kruger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Overall | 1 | 2 | 3 | 4 | 5 | p-Overall | p-Trend |
|---|---|---|---|---|---|---|---|---|
| (n = 1246) | (n = 509) | (n = 470) | (n = 170) | (n = 46) | (n = 51) | |||
| Age, mean (SD) | 63.5 (14.6) | 53.6 (12.2) | 68.5 (11.7) | 74.4 (10.7) | 73.5 (14.9) | 70.2 (12.8) | ||
| Sex, n (%) | <0.001 | <0.001 | ||||||
| M | 814 (65.3) | 392 (77.0) | 267 (56.8) | 98 (57.6) | 25 (54.3) | 32 (62.7) | ||
| F | 432 (34.7) | 117 (23.0) | 203 (43.1) | 72 (42.4) | 21 (45.7) | 19 (37.3) | ||
| Duration of hospitalization, median (IQR) | 15 [9–22] | 15 [10–23] | 15 [10–22] | 14 [8–21] | 9.5 [6.0–19.8] | 9 [5–17] | <0.001 | <0.001 |
| Any positive in the family, n (%) | 226 (31.7) | 102 (32.5) | 96 (36.2) | 23 (26.1) | 2 (10.0) | 3 (11.1) | 0.009 | 0.017 |
| First positive in the family, n (%) | 352 (68.3) | 145 (66.2) | 128 (64.3) | 51 (78.5) | 12 (80.0) | 16 (76.2) | 0.159 | 0.071 |
| Days before hospitalization, median (IQR) | 6 [3–9] | 7 [4–10] | 5 [2–8] | 5 [2–10] | 7 [2.8–11.5] | 4.5 [1.3–10.3] | 0.112 | 0.023 |
| Body temp (°C), mean (SD) | 36.7 (0.9) | 36.8 (0.9) | 36.7 (0.8) | 36.7 (0.8) | 36.7 (0.9) | 36.6 (0.8) | 0.016 | 0.001 |
| Respiratory rate (apm), median (IQR) | 20 [16–24] | 20 [16–23] | 20 [16–24] | 20 [16–25] | 21 [18–25] | 20 [16–25] | 0.054 | 0.011 |
| Heart rate (bpm), mean (SD) | 85.9 (15.2) | 86.9 (13.9) | 84.3 (14.4) | 85.6 (17.6) | 89.5 (19.1) | 89.5 (20.0) | 0.012 | 0.052 |
| Blood pressure (mmHg), mean (SD) | ||||||||
| Systolic | 132.9 (18.5) | 131.5 (16.4) | 134.9 (18.1) | 132.3 (19.7) | 128.9 (24.2) | 135.9 (28.5) | 0.020 | 0.135 |
| Diastolic | 77.7 (11.1) | 78.7 (9.9) | 78.3 (10.9) | 74.4 (11.2) | 74.3 (15.2) | 76.3 (15.6) | <0.001 | <0.001 |
| Oxygen saturation %, median (IQR) | 94 [91–96] | 95 [92–97] | 94 [90–96] | 93 [89–96] | 92 [86.3–95.0] | 95 [91.3–97.0] | <0.001 | <0.001 |
| ARDS Scale, n (%) | ||||||||
| Absent | 349 (28.0) | 160 (31.4) | 132 (28.1) | 41 (24.1) | 7 (15.2) | 9 (17.7) | <0.001 | <0.001 |
| Mild | 284 (22.8) | 118 (23.2) | 110 (23.4) | 42 (24.7) | 3 (6.5) | 11 (21.6) | ||
| Moderate | 239 (19.2) | 106 (20.8) | 94 (20.0) | 27 (15.9) | 7 (15.2) | 5 (9.8) | ||
| Severe | 207 (16.6) | 65 (12.8) | 74 (15.7) | 36 (21.2) | 16 (34.8) | 16 (31.4) | ||
| Missing | 167 (13.4) | 60 (11.8) | 60 (12.8) | 24 (14.1) | 13 (28.2) | 10 (19.6) | ||
| GCS/15, n (%) | . | . | . | . | . | 0.016 | 0.002 | |
| Mild impaired consciousness | 1076 (86.4) | 452 (88.8) | 404 (86.0) | 145 (85.3) | 35 (76.1) | 40 (78.4) | ||
| Moderate/severe impaired | 29 (2.3) | 7 (1.4) | 11 (2.3) | 4 (2.3) | 4 (8.7) | 3 (5.9) | ||
| consciousness | ||||||||
| Missing | 141 (11.3) | 50 (9.8) | 55 (11.7) | 21 (12.4) | 7 (15.2) | 8 (15.7) | ||
| Respiratory Severity Scale, n (%) | ||||||||
| None | 241 (19.3) | 132 (25.9) | 71 (15.1) | 28 (16.5) | 4 (8.7) | 6 (11.8) | <0.001 | <0.001 |
| Mask/Glasses/Cannula | 596 (47.8) | 230 (45.2) | 229 (48.7) | 87 (51.2) | 22 (47.8) | 28 (54.8) | ||
| NIV | 385 (31.0) | 142 (27.9) | 62 (34.5) | 47 (27.6) | 18 (39.1) | 16 (31.4) | ||
| OTI | 24 (1.9) | 5 (1.0) | 8 (1.7) | 8 (4.7) | 2 (4.4) | 1 (2.0) | ||
| Chronic Cardiac Disease, n (%) | 303 (25.2) | 62 (12.5) | 114 (24.8) | 78 (48.8) | 29 (70.7) | 20 (41.7) | <0.001 | <0.001 |
| CKD, n (%) | 118 (10.0) | 4 (0.8) | 15 (3.3) | 35 (22.6) | 17 (44.7) | 47 (92.2) | <0.001 | <0.001 |
| Hypertension, n (%) | 698 (57.3) | 202 (40.6) | 299 (64.4) | 126 (77.3) | 31 (72.1) | 40 (78.4) | <0.001 | <0.001 |
| Diabetes, n (%) | 274 (22.7) | 57 (11.5) | 114 (24.8) | 67 (41.9) | 14 (35.0) | 22 (44.0) | <0.001 | <0.001 |
| Smoking, n (%) | 129 (14.2) | 56 (14.3) | 41 (12.0) | 18 (15.7) | 8 (28.6) | 6 (18.2) | 0.155 | 0.199 |
| CLD, n (%) | 66 (5.6) | 18 (3.7) | 31 (6.8) | 11 (7.0) | 3 (8.1) | 3 (6.5) | 0.182 | 0.062 |
| Chronic Respiratory Disease, n (%) | 189 (15.8) | 47 (9.5) | 86 (18.9) | 37 (23.1) | 9 (23.7) | 10 (20.8) | <0.001 | <0.001 |
| Chronic Neurological Disorder, n (%) | 110 (9.1) | 27 (5.8) | 49 (10.9) | 27 (16.6) | 3 (7.3) | 4 (10.2) | <0.001 | 0.006 |
| Malign, n (%) | 111 (9.3) | 36 (7.3) | 42 (9.3) | 25 (15.7) | 5 (12.5) | 3 (6.4) | 0.026 | 0.071 |
| Laboratory | ||||||||
| Creatinine, median (IQR) | 0.9 [0.7–1.1] | 0.7 [0.7–0.8] | 0.9 [0.7–1.0] | 1.3 [1.1–1.5] | 2.4 [2.0–2.7] | 6.3 [4.6–8.1] | ||
| eGFR, median (IQR) | 85.1 [64.5–97.7] | 99.9 [95.7–106.4] | 78.2 [70.9–84.9] | 48.1 [38.2–55.0] | 23.8 [20.7–27.3] | 7.3 [5.9–10.7] | ||
| Drugs | ||||||||
| Cortison, n (%) | 1141 (92.8) | 468 (92.5) | 436 (93.6) | 152 (92.1) | 39 (90.7) | 46 (92.0) | 0.931 | 0.780 |
| Monoclonal Abs, n (%) | 46 (4.1) | 17 (3.6) | 16 (3.8) | 9 (5.9) | 4 (11.1) | - | 0.076 | 0.478 |
| Antivirals, n (%) | 325 (28.4) | 169 (35.4) | 131 (30.5) | 24 (15.4) | 1 (2.8) | - | <0.001 | <0.001 |
| Parameter | Multivariable Analysis | |||
|---|---|---|---|---|
| HR | 95% CI | p | ||
| Age | 1.03 | 1.01 | 1.04 | <0.001 |
| Sex | ||||
| M (ref) | 1 | |||
| F | 0.76 | 0.55 | 1.03 | 0.079 |
| Respiratory rate | 1.08 | 1.06 | 1.11 | <0.001 |
| Respiratory severity scale | ||||
| None (ref) | 1 | |||
| Mask/glasses/cannula | 1.97 | 0.98 | 3.95 | 0.058 |
| NIV | 2.01 | 0.98 | 4.10 | 0.056 |
| OTI | 13.33 | 5.82 | 30.53 | <0.001 |
| GCS/15, n (%) | ||||
| Mild impaired consciousness (ref) | 1 | |||
| Moderate/severe impaired | 4.03 | 2.24 | 7.24 | <0.001 |
| consciousness | ||||
| Missing | 0.81 | 0.43 | 1.53 | 0.524 |
| Chronic cardiac disease | 1.39 | 1.00 | 1.92 | 0.047 |
| Antivirals | 0.43 | 0.27 | 0.68 | <0.001 |
| Stages of eGFR | ||||
| 1 (ref) | 1 | |||
| 2 | 1.71 | 1.08 | 2.70 | 0.022 |
| 3 | 2.94 | 1.76 | 4.91 | <0.001 |
| 4 | 3.68 | 1.90 | 7.12 | <0.001 |
| 5 | 7.25 | 4.04 | 13.01 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galiero, R.; Simeon, V.; Loffredo, G.; Caturano, A.; Rinaldi, L.; Vetrano, E.; Medicamento, G.; Alfano, M.; Beccia, D.; Brin, C.; et al. Association between Renal Function at Admission and COVID-19 in-Hospital Mortality in Southern Italy: Findings from the Prospective Multicenter Italian COVOCA Study. J. Clin. Med. 2022, 11, 6121. https://doi.org/10.3390/jcm11206121
Galiero R, Simeon V, Loffredo G, Caturano A, Rinaldi L, Vetrano E, Medicamento G, Alfano M, Beccia D, Brin C, et al. Association between Renal Function at Admission and COVID-19 in-Hospital Mortality in Southern Italy: Findings from the Prospective Multicenter Italian COVOCA Study. Journal of Clinical Medicine. 2022; 11(20):6121. https://doi.org/10.3390/jcm11206121
Chicago/Turabian StyleGaliero, Raffaele, Vittorio Simeon, Giuseppe Loffredo, Alfredo Caturano, Luca Rinaldi, Erica Vetrano, Giulia Medicamento, Maria Alfano, Domenico Beccia, Chiara Brin, and et al. 2022. "Association between Renal Function at Admission and COVID-19 in-Hospital Mortality in Southern Italy: Findings from the Prospective Multicenter Italian COVOCA Study" Journal of Clinical Medicine 11, no. 20: 6121. https://doi.org/10.3390/jcm11206121
APA StyleGaliero, R., Simeon, V., Loffredo, G., Caturano, A., Rinaldi, L., Vetrano, E., Medicamento, G., Alfano, M., Beccia, D., Brin, C., Colantuoni, S., Di Salvo, J., Epifani, R., Nevola, R., Marfella, R., Sardu, C., Coppola, C., Scarano, F., Maggi, P., ... on behalf of COVOCA Study Group. (2022). Association between Renal Function at Admission and COVID-19 in-Hospital Mortality in Southern Italy: Findings from the Prospective Multicenter Italian COVOCA Study. Journal of Clinical Medicine, 11(20), 6121. https://doi.org/10.3390/jcm11206121