
High Comorbidity Burden in Patients with SLE: Data from the Community-Based Lupus Registry of Crete

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Source Population and Setting
2.2. The Cretan Community-Based Lupus Registry
2.3. Variables and Comorbidities
2.4. Clinical Data Abstracted from the Medical Records
2.5. Statistical Analysis and Hierarchical Clustering
3. Results
3.1. High Prevalence of Comorbid Diseases in SLE Patients at the Community
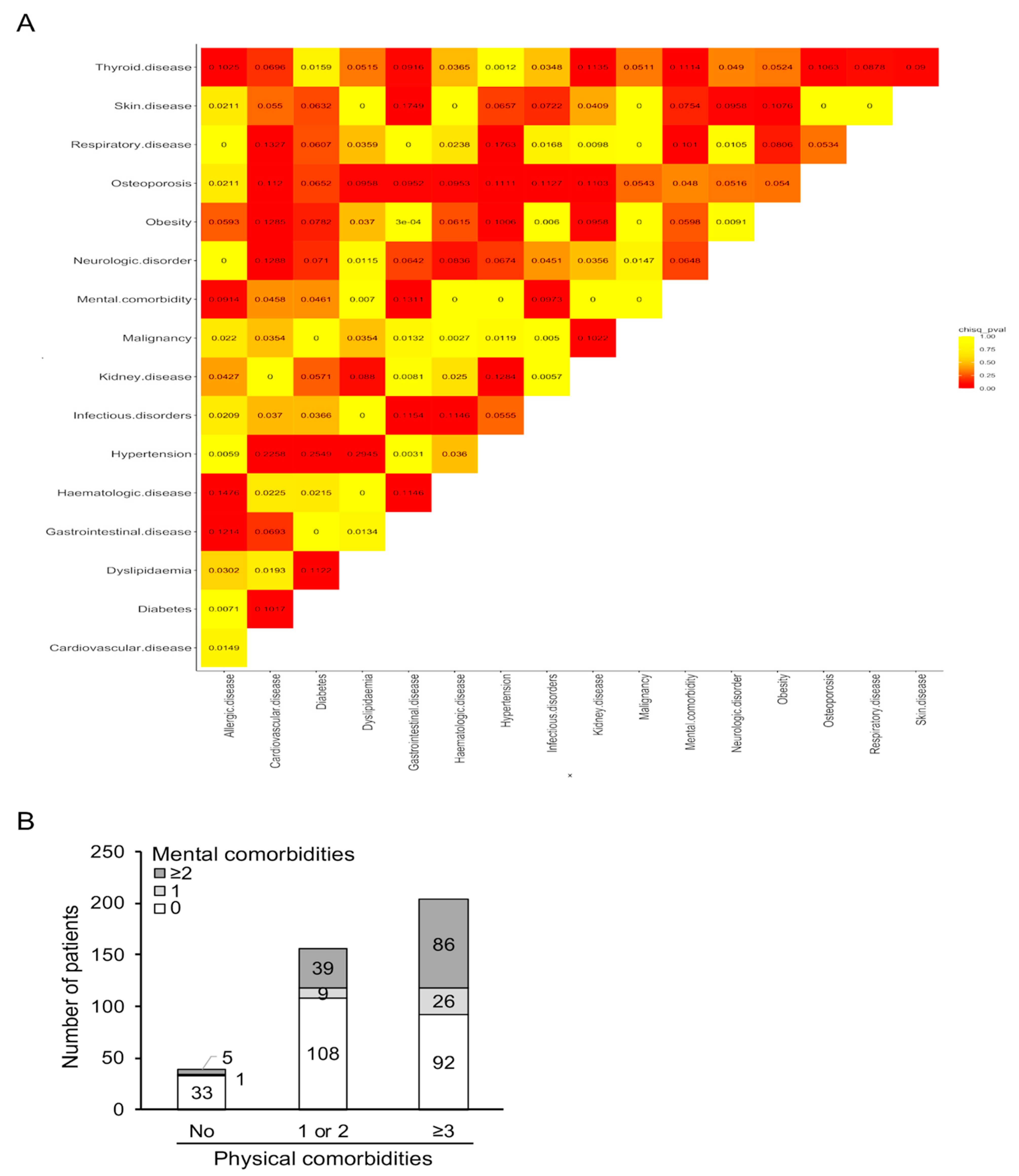
3.2. Co-Segregation of Physical and Mental Comorbidities in Patients with SLE
3.3. Predictors of Morbidity and Multimorbidity in Patients with SLE
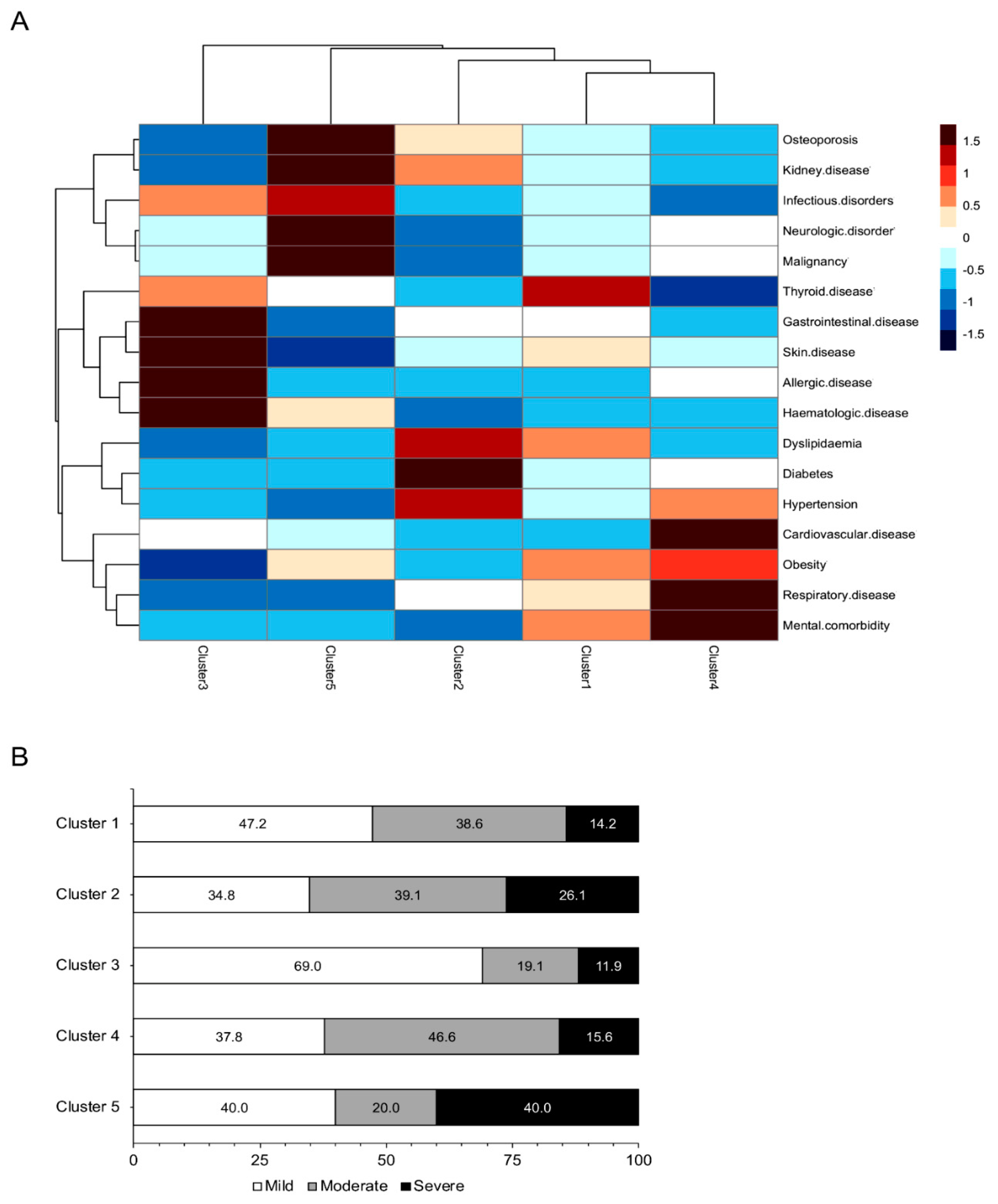
3.4. Distinct Comorbidities Phenotypes in Patients with SLE Revealed by Cluster Analysis
3.5. Association between Morbidities and Clinical Outcomes in Patients with SLE
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gonzalez, L.A.; Alarcon, G.S. The evolving concept of SLE comorbidities. Expert Rev. Clin. Immunol. 2017, 13, 1–16. [Google Scholar] [CrossRef]
- Urowitz, M.B.; Bookman, A.A.; Koehler, B.E.; Gordon, D.A.; Smythe, H.A.; Ogryzlo, M.A. The bimodal mortality pattern of systemic lupus erythematosus. Am. J. Med. 1976, 60, 221–225. [Google Scholar] [CrossRef]
- Rees, F.; Doherty, M.; Grainge, M.; Lanyon, P.; Davenport, G.; Zhang, W. Burden of comorbidity in systemic lupus erythematosus in the UK, 1999–2012. Arthritis Care Res. 2016, 68, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Kedves, M.; Kosa, F.; Kunovszki, P.; Takacs, P.; Szabo, M.Z.; Karyekar, C.; Lofland, J.H.; Nagy, G. Large-scale mortality gap between SLE and control population is associated with increased infection-related mortality in lupus. Rheumatology 2020, 59, 3443–3451. [Google Scholar] [CrossRef] [PubMed]
- Rua-Figueroa, I.; Lopez-Longo, J.; Galindo-Izquierdo, M.; Calvo-Alen, J.; Del Campo, V.; Olive-Marques, A.; Perez-Vicente, S.; Fernandez-Nebro, A.; Andres, M.; Erausquin, C.; et al. Incidence, associated factors and clinical impact of severe infections in a large, multicentric cohort of patients with systemic lupus erythematosus. Semin. Arthritis Rheum. 2017, 47, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Tektonidou, M.G.; Wang, Z.; Dasgupta, A.; Ward, M.M. Burden of serious infections in adults with systemic lupus erythematosus: A national population-based study, 1996–2011. Arthritis Care Res. 2015, 67, 1078–1085. [Google Scholar] [CrossRef] [PubMed]
- Parker, B.; Urowitz, M.B.; Gladman, D.D.; Lunt, M.; Bae, S.C.; Sanchez-Guerrero, J.; Romero-Diaz, J.; Gordon, C.; Wallace, D.J.; Clarke, A.E.; et al. Clinical associations of the metabolic syndrome in systemic lupus erythematosus: Data from an international inception cohort. Ann. Rheum. Dis. 2013, 72, 1308–1314. [Google Scholar] [CrossRef] [PubMed]
- Tselios, K.; Koumaras, C.; Gladman, D.D.; Urowitz, M.B. Dyslipidemia in systemic lupus erythematosus: Just another comorbidity? Semin. Arthritis Rheum. 2016, 45, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Katz, G.; Smilowitz, N.R.; Blazer, A.; Clancy, R.; Buyon, J.P.; Berger, J.S. Systemic lupus erythematosus and increased prevalence of atherosclerotic cardiovascular disease in hospitalized patients. Mayo Clin. Proc. 2019, 94, 1436–1443. [Google Scholar] [CrossRef]
- Urowitz, M.B.; Gladman, D.; Ibanez, D.; Bae, S.C.; Sanchez-Guerrero, J.; Gordon, C.; Clarke, A.; Bernatsky, S.; Fortin, P.R.; Hanly, J.G.; et al. Atherosclerotic vascular events in a multinational inception cohort of systemic lupus erythematosus. Arthritis Care Res. 2010, 62, 881–887. [Google Scholar] [CrossRef]
- Chuang, Y.W.; Yu, M.C.; Lin, C.L.; Yu, T.M.; Shu, K.H.; Kao, C.H. Risk of peripheral arterial occlusive disease in patients with systemic lupus erythematosus: A nationwide population-based cohort study. Medicine 2015, 94, e2121. [Google Scholar] [CrossRef]
- Holmqvist, M.; Simard, J.F.; Asplund, K.; Arkema, E.V. Stroke in systemic lupus erythematosus: A meta-analysis of population-based cohort studies. RMD Open 2015, 1, e000168. [Google Scholar] [CrossRef]
- Schoenfeld, S.R.; Kasturi, S.; Costenbader, K.H. The epidemiology of atherosclerotic cardiovascular disease among patients with SLE: A systematic review. Semin. Arthritis Rheum. 2013, 43, 77–95. [Google Scholar] [CrossRef]
- Cao, L.; Tong, H.; Xu, G.; Liu, P.; Meng, H.; Wang, J.; Zhao, X.; Tang, Y.; Jin, J. Systemic lupus erythematous and malignancy risk: A meta-analysis. PLoS ONE 2015, 10, e0122964. [Google Scholar] [CrossRef]
- Wadstrom, H.; Arkema, E.V.; Sjowall, C.; Askling, J.; Simard, J.F. Cervical neoplasia in systemic lupus erythematosus: A nationwide study. Rheumatology 2017, 56, 613–619. [Google Scholar] [CrossRef]
- Wu, Y.; Hou, Q. Systemic lupus erythematous increased lung cancer risk: Evidence from a meta-analysis. J. Cancer Res. Ther. 2016, 12, 721–724. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-Pinto, C.; Rojas-Villarraga, A.; Molano-Gonzalez, N.; Jimenez-Herrera, E.A.; Leon-Vazquez, M.L.; Montiel-Jarquin, A.; Garcia-Carrasco, M.; Cervera, R. Bone mineral density and vertebral fractures in patients with systemic lupus erythematosus: A systematic review and meta-regression. PLoS ONE 2018, 13, e0196113. [Google Scholar] [CrossRef] [PubMed]
- Tedeschi, S.K.; Kim, S.C.; Guan, H.; Grossman, J.M.; Costenbader, K.H. Comparative fracture risks among United States medicaid enrollees with and those without systemic lupus erythematosus. Arthritis Rheumatol. 2019, 71, 1141–1146. [Google Scholar] [CrossRef] [PubMed]
- Haliloglu, S.; Carlioglu, A.; Akdeniz, D.; Karaaslan, Y.; Kosar, A. Fibromyalgia in patients with other rheumatic diseases: Prevalence and relationship with disease activity. Rheumatol. Int. 2014, 34, 1275–1280. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Fu, T.; Yin, R.; Zhang, Q.; Shen, B. Prevalence of depression and anxiety in systemic lupus erythematosus: A systematic review and meta-analysis. BMC Psychiatry 2017, 17, 70. [Google Scholar] [CrossRef]
- Radner, H.; Yoshida, K.; Smolen, J.S.; Solomon, D.H. Multimorbidity and rheumatic conditions-enhancing the concept of comorbidity. Nat. Rev. Rheumatol. 2014, 10, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Balitsky, A.K.; Peeva, V.; Su, J.; Aghdassi, E.; Yeo, E.; Gladman, D.D.; Urowitz, M.B.; Fortin, P.R. Thrombovascular events affect quality of life in patients with systemic lupus erythematosus. J. Rheumatol. 2011, 38, 1017–1019. [Google Scholar] [CrossRef] [PubMed]
- Rizk, A.; Gheita, T.A.; Nassef, S.; Abdallah, A. The impact of obesity in systemic lupus erythematosus on disease parameters, quality of life, functional capacity and the risk of atherosclerosis. Int. J. Rheum. Dis. 2012, 15, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Baker, K.; Pope, J.; Fortin, P.; Silverman, E.; Peschken, C. Work disability in systemic lupus erythematosus is prevalent and associated with socio-demographic and disease related factors. Lupus 2009, 18, 1281–1288. [Google Scholar] [CrossRef]
- Kim, S.K.; Choe, J.Y.; Lee, S.S. Charlson comorbidity index is related to organ damage in systemic lupus erythematosus: Data from KORean lupus network (KORNET) registry. J. Rheumatol. 2017, 44, 452–458. [Google Scholar] [CrossRef]
- Yang, Y.; Thumboo, J.; Earnest, A.; Yong, S.L.; Fong, K.Y. The effect of comorbidity on hospital mortality in patients with SLE from an Asian tertiary hospital. Lupus 2014, 23, 714–720. [Google Scholar] [CrossRef]
- Han, G.M.; Han, X.F. Comorbid conditions are associated with emergency department visits, hospitalizations, and medical charges of patients with systemic lupus erythematosus. J. Clin. Rheumatol. 2017, 23, 19–25. [Google Scholar] [CrossRef]
- Jonsen, A.; Clarke, A.E.; Joseph, L.; Belisle, P.; Bernatsky, S.; Nived, O.; Bengtsson, A.A.; Sturfelt, G.; Pineau, C.A. Association of the Charlson comorbidity index with mortality in systemic lupus erythematosus. Arthritis Care Res. 2011, 63, 1233–1237. [Google Scholar] [CrossRef]
- van Vollenhoven, R.F.; Mosca, M.; Bertsias, G.; Isenberg, D.; Kuhn, A.; Lerstrom, K.; Aringer, M.; Bootsma, H.; Boumpas, D.; Bruce, I.N.; et al. Treat-to-target in systemic lupus erythematosus: Recommendations from an international task force. Ann. Rheum. Dis. 2014, 73, 958–967. [Google Scholar] [CrossRef]
- Duru, N.; van der Goes, M.C.; Jacobs, J.W.; Andrews, T.; Boers, M.; Buttgereit, F.; Caeyers, N.; Cutolo, M.; Halliday, S.; Da Silva, J.A.; et al. EULAR evidence-based and consensus-based recommendations on the management of medium to high-dose glucocorticoid therapy in rheumatic diseases. Ann. Rheum. Dis. 2013, 72, 1905–1913. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Kostopoulou, M.; Alunno, A.; Aringer, M.; Bajema, I.; Boletis, J.N.; Cervera, R.; Doria, A.; Gordon, C.; Govoni, M.; et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 736–745. [Google Scholar] [CrossRef]
- Mosca, M.; Tani, C.; Aringer, M.; Bombardieri, S.; Boumpas, D.; Brey, R.; Cervera, R.; Doria, A.; Jayne, D.; Khamashta, M.A.; et al. European League against Rheumatism recommendations for monitoring patients with systemic lupus erythematosus in clinical practice and in observational studies. Ann. Rheum. Dis. 2010, 69, 1269–1274. [Google Scholar] [CrossRef] [PubMed]
- Leonard, D.; Svenungsson, E.; Dahlqvist, J.; Alexsson, A.; Arlestig, L.; Taylor, K.E.; Sandling, J.K.; Bengtsson, C.; Frodlund, M.; Jonsen, A.; et al. Novel gene variants associated with cardiovascular disease in systemic lupus erythematosus and rheumatoid arthritis. Ann. Rheum. Dis. 2018, 77, 1063–1069. [Google Scholar] [CrossRef] [PubMed]
- Greenstein, L.; Makan, K.; Tikly, M. Burden of comorbidities in South Africans with systemic lupus erythematosus. Clin. Rheumatol. 2019, 38, 2077–2082. [Google Scholar] [CrossRef]
- Falasinnu, T.; Chaichian, Y.; Li, J.; Chung, S.; Waitzfelder, B.E.; Fortmann, S.P.; Palaniappan, L.; Simard, J.F. Does SLE widen or narrow race/ethnic disparities in the risk of five co-morbid conditions? Evidence from a community-based outpatient care system. Lupus 2019, 28, 1619–1627. [Google Scholar] [CrossRef] [PubMed]
- Walsh, S.J.; Algert, C.; Rothfield, N.F. Racial aspects of comorbidity in systemic lupus erythematosus. Arthritis Care Res. 1996, 9, 509–516. [Google Scholar] [CrossRef]
- Akinyemiju, T.; Jha, M.; Moore, J.X.; Pisu, M. Disparities in the prevalence of comorbidities among US adults by state Medicaid expansion status. Prev. Med. 2016, 88, 196–202. [Google Scholar] [CrossRef]
- Schiotz, M.L.; Stockmarr, A.; Host, D.; Glumer, C.; Frolich, A. Social disparities in the prevalence of multimorbidity—A register-based population study. BMC Public Health 2017, 17, 422. [Google Scholar] [CrossRef]
- Gergianaki, I.; Fanouriakis, A.; Adamichou, C.; Spyrou, G.; Mihalopoulos, N.; Kazadzis, S.; Chatzi, L.; Sidiropoulos, P.; Boumpas, D.T.; Bertsias, G. Is systemic lupus erythematosus different in urban versus rural living environment? Data from the Cretan Lupus Epidemiology and Surveillance Registry. Lupus 2019, 28, 104–113. [Google Scholar] [CrossRef]
- Gergianaki, I.; Fanouriakis, A.; Repa, A.; Tzanakakis, M.; Adamichou, C.; Pompieri, A.; Spirou, G.; Bertsias, A.; Kabouraki, E.; Tzanakis, I.; et al. Epidemiology and burden of systemic lupus erythematosus in a Southern European population: Data from the community-based lupus registry of Crete, Greece. Ann. Rheum. Dis. 2017, 76, 1992–2000. [Google Scholar] [CrossRef]
- Chatziarsenis, M.; Lionis, C.; Faresjo, T.; Fioretos, M.; Trell, E. Community-based medical systems advancement in a hospital-primary health care centre in Crete, Greece: Concepts, methods, and the new role of the general practitioner. J. Med. Syst. 1998, 22, 173–188. [Google Scholar] [CrossRef]
- Hochberg, M.C. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997, 40, 1725. [Google Scholar] [CrossRef] [PubMed]
- Petri, M.; Orbai, A.M.; Alarcon, G.S.; Gordon, C.; Merrill, J.T.; Fortin, P.R.; Bruce, I.N.; Isenberg, D.; Wallace, D.J.; Nived, O.; et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012, 64, 2677–2686. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, S.; Jin, L.; Meltzer, D. Use of a self-report-generated Charlson Comorbidity Index for predicting mortality. Med. Care 2005, 43, 607–615. [Google Scholar] [CrossRef]
- Ho, P.J.; Tan, C.S.; Shawon, S.R.; Eriksson, M.; Lim, L.Y.; Miao, H.; Png, E.; Chia, K.S.; Hartman, M.; Ludvigsson, J.F.; et al. Comparison of self-reported and register-based hospital medical data on comorbidities in women. Sci. Rep. 2019, 9, 3527. [Google Scholar] [CrossRef] [PubMed]
- Ng, X.; Low, A.H.; Thumboo, J. Comparison of the Charlson Comorbidity Index derived from self-report and medical record review in Asian patients with rheumatic diseases. Rheumatol. Int. 2015, 35, 2005–2011. [Google Scholar] [CrossRef] [PubMed]
- Olomu, A.B.; Corser, W.D.; Stommel, M.; Xie, Y.; Holmes-Rovner, M. Do self-report and medical record comorbidity data predict longitudinal functional capacity and quality of life health outcomes similarly? BMC Health Serv. Res. 2012, 12, 398. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Pamfil, C.; Rednic, S.; Sidiropoulos, P.; Bertsias, G.; Boumpas, D.T. Is it primary neuropsychiatric systemic lupus erythematosus? Performance of existing attribution models using physician judgment as the gold standard. Clin. Exp. Rheumatol. 2016, 34, 910–917. [Google Scholar] [PubMed]
- Sutton, E.J.; Davidson, J.E.; Bruce, I.N. The systemic lupus international collaborating clinics (SLICC) damage index: A systematic literature review. Semin. Arthritis Rheum. 2013, 43, 352–361. [Google Scholar] [CrossRef] [PubMed]
- Isenberg, D.A.; Rahman, A.; Allen, E.; Farewell, V.; Akil, M.; Bruce, I.N.; D′Cruz, D.; Griffiths, B.; Khamashta, M.; Maddison, P.; et al. BILAG 2004. Development and initial validation of an updated version of the British Isles Lupus Assessment Group′s disease activity index for patients with systemic lupus erythematosus. Rheumatology 2005, 44, 902–906. [Google Scholar] [CrossRef]
- Barbhaiya, M.; Feldman, C.H.; Guan, H.; Chen, S.K.; Fischer, M.A.; Solomon, D.H.; Everett, B.M.; Costenbader, K.H. Racial/ethnic variation in stroke rates and risks among patients with systemic lupus erythematosus. Semin. Arthritis Rheum. 2019, 48, 840–846. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.A.; Gebregziabher, M.; Kamen, D.L.; White, B.M.; Williams, E.M. Examining racial differences in access to primary care for people living with lupus: Use of ambulatory care sensitive conditions to measure access. Ethn. Dis. 2020, 30, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Avina-Zubieta, J.A.; To, F.; Vostretsova, K.; De Vera, M.; Sayre, E.C.; Esdaile, J.M. Risk of myocardial infarction and stroke in newly diagnosed systemic lupus erythematosus: A general population-based study. Arthritis Care Res. 2017, 69, 849–856. [Google Scholar] [CrossRef]
- Katz, P.; Gregorich, S.; Yazdany, J.; Trupin, L.; Julian, L.; Yelin, E.; Criswell, L.A. Obesity and its measurement in a community-based sample of women with systemic lupus erythematosus. Arthritis Care Res. 2011, 63, 261–268. [Google Scholar] [CrossRef]
- Nived, O.; Ingvarsson, R.F.; Joud, A.; Linge, P.; Tyden, H.; Jonsen, A.; Bengtsson, A.A. Disease duration, age at diagnosis and organ damage are important factors for cardiovascular disease in SLE. Lupus Sci. Med. 2020, 7, e000398. [Google Scholar] [CrossRef] [PubMed]
- Sabio, J.M.; Vargas-Hitos, J.A.; Navarrete-Navarrete, N.; Mediavilla, J.D.; Jimenez-Jaimez, J.; Diaz-Chamorro, A.; Jimenez-Alonso, J.; Grupo Lupus Virgen de las, N. Prevalence of and factors associated with hypertension in young and old women with systemic lupus erythematosus. J. Rheumatol. 2011, 38, 1026–1032. [Google Scholar] [CrossRef] [PubMed]
- Tselios, K.; Gladman, D.D.; Su, J.; Ace, O.; Urowitz, M.B. Evolution of risk factors for atherosclerotic cardiovascular events in systemic lupus erythematosus: A longterm prospective study. J. Rheumatol. 2017, 44, 1841–1849. [Google Scholar] [CrossRef]
- Magder, L.S.; Petri, M. Incidence of and risk factors for adverse cardiovascular events among patients with systemic lupus erythematosus. Am. J. Epidemiol. 2012, 176, 708–719. [Google Scholar] [CrossRef]
- Kostopoulou, M.; Nikolopoulos, D.; Parodis, I.; Bertsias, G. Cardiovascular disease in systemic lupus erythematosus: Recent data on epidemiology, risk factors and prevention. Curr. Vasc. Pharm. 2020, 18, 549–565. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Yoshida, K.; Feldman, C.H.; Speyer, C.; Barbhaiya, M.; Guan, H.; Solomon, D.H.; Everett, B.M.; Costenbader, K.H. Initial disease severity, cardiovascular events and all-cause mortality among patients with systemic lupus erythematosus. Rheumatology 2020, 59, 495–504. [Google Scholar] [CrossRef]
- Romero-Diaz, J.; Vargas-Vorackova, F.; Kimura-Hayama, E.; Cortazar-Benitez, L.F.; Gijon-Mitre, R.; Criales, S.; Cabiedes-Contreras, J.; Iniguez-Rodriguez Mdel, R.; Lara-Garcia, E.A.; Nunez-Alvarez, C.; et al. Systemic lupus erythematosus risk factors for coronary artery calcifications. Rheumatology 2012, 51, 110–119. [Google Scholar] [CrossRef]
- Robles-Vera, I.; Visitacion, N.; Toral, M.; Sanchez, M.; Gomez-Guzman, M.; O′Valle, F.; Jimenez, R.; Duarte, J.; Romero, M. Toll-like receptor 7-driven lupus autoimmunity induces hypertension and vascular alterations in mice. J. Hypertens 2020, 38, 1322–1335. [Google Scholar] [CrossRef]
- Petri, M.; Magder, L.S. Comparison of remission and lupus low disease activity state in damage prevention in a United States systemic lupus erythematosus cohort. Arthritis Rheumatol. 2018, 70, 1790–1795. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, S.M.; Elia, G.; Virili, C.; Centanni, M.; Antonelli, A.; Fallahi, P. Systemic lupus erythematosus and thyroid autoimmunity. Front. Endocrinol. (Lausanne) 2017, 8, 138. [Google Scholar] [CrossRef]
- Luo, W.; Mao, P.; Zhang, L.; Yang, Z. Association between systemic lupus erythematosus and thyroid dysfunction: A meta-analysis. Lupus 2018, 27, 2120–2128. [Google Scholar] [CrossRef]
- Yun, J.S.; Bae, J.M.; Kim, K.J.; Jung, Y.S.; Kim, G.M.; Kim, H.R.; Lee, J.S.; Ko, S.H.; Cha, S.A.; Ahn, Y.B. Increased risk of thyroid diseases in patients with systemic lupus erythematosus: A nationwide population-based study in Korea. PLoS ONE 2017, 12, e0179088. [Google Scholar] [CrossRef]
- Cramarossa, G.; Urowitz, M.B.; Su, J.; Gladman, D.; Touma, Z. Prevalence and associated factors of low bone mass in adults with systemic lupus erythematosus. Lupus 2017, 26, 365–372. [Google Scholar] [CrossRef]
- Bultink, I.E.; Lems, W.F. Systemic lupus erythematosus and fractures. RMD Open 2015, 1, e000069. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, Y.P.; Tsai, J.D.; Muo, C.H.; Tsai, C.H.; Sung, F.C.; Liao, Y.T.; Chang, Y.J.; Yang, J.H. Atopic diseases and systemic lupus erythematosus: An epidemiological study of the risks and correlations. Int. J. Environ. Res. Public Health 2014, 11, 8112–8122. [Google Scholar] [CrossRef] [PubMed]
- Wongtrakul, W.; Charoenngam, N.; Ponvilawan, B.; Ungprasert, P. Allergic rhinitis and risk of systemic lupus erythematosus: A systematic review and meta-analysis. Int. J. Rheum. Dis. 2020, 23, 1460–1467. [Google Scholar] [CrossRef]
- Sin, E.; Anand, P.; Frieri, M. A link: Allergic rhinitis, asthma & systemic lupus erythematosus. Autoimmun. Rev. 2016, 15, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, H.; Cevallos, A.; Jimbo Sotomayor, R.; Naranjo-Saltos, F.; Mera Orces, D.; Basantes, E. Mental disorders in systemic lupus erythematosus: A cohort study. Rheumatol. Int. 2019, 39, 1689–1695. [Google Scholar] [CrossRef] [PubMed]
- Hesselvig, J.H.; Egeberg, A.; Kofoed, K.; Gislason, G.; Dreyer, L. Increased risk of depression in patients with cutaneous lupus erythematosus and systemic lupus erythematosus: A Danish nationwide cohort study. Br. J. Derm. 2018, 179, 1095–1101. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, A.T.; Moazzami, M.; Engel, L.; Bangert, E.; Hassanein, M.; Marzouk, S.; Kravtsenyuk, M.; Fung, W.; Eder, L.; Su, J.; et al. Prevalence and metric of depression and anxiety in systemic lupus erythematosus: A systematic review and meta-analysis. Semin. Arthritis Rheum. 2020, 50, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Abd-Alrasool, Z.A.; Gorial, F.I.; Hashim, M.T. Prevalence and severity of depression among Iraqi patients with systemic lupus rythematosus: A descriptive study. Mediterr. J. Rheumatol. 2017, 28, 142–146. [Google Scholar] [CrossRef]
- Tiosano, S.; Nir, Z.; Gendelman, O.; Comaneshter, D.; Amital, H.; Cohen, A.D.; Amital, D. The association between systemic lupus erythematosus and bipolar disorder—A big data analysis. Eur. Psychiatry J. Assoc. Eur. Psychiatr. 2017, 43, 116–119. [Google Scholar] [CrossRef]
- Mok, C.C.; Chan, K.L.; Cheung, E.F.; Yip, P.S. Suicidal ideation in patients with systemic lupus erythematosus: Incidence and risk factors. Rheumatology 2014, 53, 714–721. [Google Scholar] [CrossRef]
- Tiosano, S.; Farhi, A.; Watad, A.; Grysman, N.; Stryjer, R.; Amital, H.; Comaneshter, D.; Cohen, A.D.; Amital, D. Schizophrenia among patients with systemic lupus erythematosus: Population-based cross-sectional study. Epidemiol. Psychiatr. Sci. 2017, 26, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Lillis, T.A.; Tirone, V.; Gandhi, N.; Weinberg, S.; Nika, A.; Sequeira, W.; Hobfoll, S.E.; Block, J.A.; Jolly, M. Sleep disturbance and depression symptoms mediate relationship between pain and cognitive dysfunction in lupus. Arthritis Care Res. 2019, 71, 406–412. [Google Scholar] [CrossRef]
- Figueiredo-Braga, M.; Cornaby, C.; Cortez, A.; Bernardes, M.; Terroso, G.; Figueiredo, M.; Mesquita, C.D.S.; Costa, L.; Poole, B.D. Depression and anxiety in systemic lupus erythematosus: The crosstalk between immunological, clinical, and psychosocial factors. Medicine 2018, 97, e11376. [Google Scholar] [CrossRef]
- Tisseverasinghe, A.; Peschken, C.; Hitchon, C. Anxiety and mood disorders in systemic lupus erythematosus: Current insights and future directions. Curr. Rheumatol. Rep. 2018, 20, 85. [Google Scholar] [CrossRef] [PubMed]
- McQueenie, R.; Nicholl, B.I.; Jani, B.D.; Canning, J.; Macdonald, S.; McCowan, C.; Neary, J.; Browne, S.; Mair, F.S.; Siebert, S. Patterns of multimorbidity and their effects on adverse outcomes in rheumatoid arthritis: A study of 5658 UK Biobank participants. BMJ Open 2020, 10, e038829. [Google Scholar] [CrossRef] [PubMed]
- Radner, H.; Yoshida, K.; Mjaavatten, M.D.; Aletaha, D.; Frits, M.; Lu, B.; Iannaccone, C.; Shadick, N.; Weinblatt, M.; Hmamouchi, I.; et al. Development of a multimorbidity index: Impact on quality of life using a rheumatoid arthritis cohort. Semin. Arthritis Rheum. 2015, 45, 167–173. [Google Scholar] [CrossRef]
- Ziade, N.; El Khoury, B.; Zoghbi, M.; Merheb, G.; Abi Karam, G.; Mroue, K.; Messaykeh, J. Prevalence and pattern of comorbidities in chronic rheumatic and musculoskeletal diseases: The COMORD study. Sci Rep. 2020, 10, 7683. [Google Scholar] [CrossRef]
- Kariniemi, S.; Rantalaiho, V.; Virta, L.J.; Puolakka, K.; Sokka-Isler, T.; Elfving, P. Multimorbidity among incident Finnish systemic lupus erythematosus patients during 2000–2017. Lupus 2021, 30, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Medhat, B.M.; Behiry, M.E.; Sobhy, N.; Farag, Y.; Marzouk, H.; Mostafa, N.; Khalifa, I.; Elkhalifa, M.; Eissa, B.M.; Hassan, E.H.E. Late-onset systemic lupus erythematosus: Characteristics and outcome in comparison to juvenile- and adult-onset patients-a multicenter retrospective cohort. Clin. Rheumatol. 2020, 39, 435–442. [Google Scholar] [CrossRef]
- Petri, M.A.; Barr, E.; Magder, L.S. Development of a systemic lupus erythematosus cardiovascular risk equation. Lupus Sci. Med. 2019, 6, e000346. [Google Scholar] [CrossRef]
- Kubota, Y.; Heiss, G.; MacLehose, R.F.; Roetker, N.S.; Folsom, A.R. Association of educational attainment with lifetime risk of cardiovascular disease: The atherosclerosis risk in communities study. JAMA Intern. Med. 2017, 177, 1165–1172. [Google Scholar] [CrossRef]
- Nagel, G.; Peter, R.; Braig, S.; Hermann, S.; Rohrmann, S.; Linseisen, J. The impact of education on risk factors and the occurrence of multimorbidity in the EPIC-Heidelberg cohort. BMC Public Health 2008, 8, 384. [Google Scholar] [CrossRef]
- Richette, P.; Clerson, P.; Perissin, L.; Flipo, R.M.; Bardin, T. Revisiting comorbidities in gout: A cluster analysis. Ann. Rheum. Dis. 2015, 74, 142–147. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | No. (%) or Mean ± Standard Deviation |
|---|---|
| Gender (female) | 364 (91.2%) |
| Age at diagnosis (years) | 42.8 ± 14.6 |
| Disease duration (years) | 9.9 ± 6.6 |
| No. ACR criteria | 4.7 ± 1.2 |
| Lupus nephritis (biopsy-proven) | 45 (11.3%) |
| Neuropsychiatric lupus | 43 (10.8%) |
| Disease severity 1 | |
| Mild | 190 (47.7%) |
| Moderate | 144 (36.1%) |
| Severe | 65 (16.2%) |
| Organ damage | 144 (36.2%) |
| Residence | |
| Rural | 172 (43.1%) |
| Urban and semi-urban | 227 (56.9%) |
| Education level | |
| <12 years | 284 (71.2%) |
| ≥12 years | 115 (28.8%) |
| Marital status | |
| Single | 55 (13.7%) |
| Married | 299 (74.9%) |
| Divorced or separated | 21 (5.3%) |
| Widowed | 24 (6.1%) |
| Tobacco use | |
| Never | 208 (55.3%) 2 |
| Past | 55 (14.6%) |
| Active | 113 (30.1%) |
| Comorbidiy | Prevalence |
|---|---|
| Thyroid disease 1 | 45.6% |
| Mental disorder 2 | 42.1% |
| Depression | 26.7% |
| Anxiety disorder | 10.7% |
| Obesity 3 | 35.3% |
| Dyslipidemia | 33.3% |
| Hypertension | 24.6% |
| Osteoporosis and osteoporotic fracture | 22.3% |
| Cardiovascular disease 4 | 20.8% |
| Allergic disorders 5 | 20.6% |
| Gastrointestinal disease 6 | 19.0% |
| Infectious disease 7 | 12.8% |
| Neurologic disease 8 | 10.3% |
| Cerebrovascular disease | 2.5% |
| Kidney disease | 9.5% |
| Respiratory disease | 9.3% |
| Diabetes mellitus | 8.8% |
| Malignant disease | 4.8% |
| Skin disease | 3.3% |
| Hematologic disease | 2.3% |
| Comorbidities | Mean ± Standard Deviation or Prevalence (%) |
|---|---|
| Physical comorbidities | 2.8 ± 2.0 |
| None | 9.8% |
| 1 or 2 | 39.2% |
| ≥3 | 51.0% |
| Mental comorbidities | 0.94 ± 1.25 |
| None | 57.9% |
| 1 | 9.0% |
| ≥2 | 33.1% |
| Charlson Comorbidity Index (CCI) | 0.91 ± 1.16 |
| >0 | 50.3% |
| Dependent Variable 1 | Predictor (s) | OR (95% CI) 2 | p Value |
|---|---|---|---|
| ≥3 physical comorbidities | Education level | ||
| ≥12 years vs. <12 years | 0.46 (0.28–0.75) | 0.002 | |
| SLE severity | |||
| Moderate vs. mild | 2.30 (1.43–3.71) | 0.001 | |
| Severe vs. mild | 1.30 (0.71–2.41) | 0.398 | |
| ≥2 mental comorbidities | Marital status | ||
| Divorced or widowed vs. single or married | 2.76 (1.43–5.35) | 0.003 | |
| ACR-1997 neurologic item | |||
| Present vs. absent | 6.02 (1.86–19.53) | 0.003 | |
| Charlson comorbidity index ≥ 1 | Education level | ||
| ≥12 years vs. <12 years | 0.52 (0.31–0.86) | 0.011 | |
| No. ACR-1997 criteria (per 1-item) | 1.30 (1.06–1.59) | 0.013 | |
| Marital status | |||
| Divorced or widowed vs. single or married | 2.18 (1.02–4.68) | 0.045 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gergianaki, I.; Garantziotis, P.; Adamichou, C.; Saridakis, I.; Spyrou, G.; Sidiropoulos, P.; Bertsias, G. High Comorbidity Burden in Patients with SLE: Data from the Community-Based Lupus Registry of Crete. J. Clin. Med. 2021, 10, 998. https://doi.org/10.3390/jcm10050998
Gergianaki I, Garantziotis P, Adamichou C, Saridakis I, Spyrou G, Sidiropoulos P, Bertsias G. High Comorbidity Burden in Patients with SLE: Data from the Community-Based Lupus Registry of Crete. Journal of Clinical Medicine. 2021; 10(5):998. https://doi.org/10.3390/jcm10050998
Chicago/Turabian StyleGergianaki, Irini, Panagiotis Garantziotis, Christina Adamichou, Ioannis Saridakis, Georgios Spyrou, Prodromos Sidiropoulos, and George Bertsias. 2021. "High Comorbidity Burden in Patients with SLE: Data from the Community-Based Lupus Registry of Crete" Journal of Clinical Medicine 10, no. 5: 998. https://doi.org/10.3390/jcm10050998
APA StyleGergianaki, I., Garantziotis, P., Adamichou, C., Saridakis, I., Spyrou, G., Sidiropoulos, P., & Bertsias, G. (2021). High Comorbidity Burden in Patients with SLE: Data from the Community-Based Lupus Registry of Crete. Journal of Clinical Medicine, 10(5), 998. https://doi.org/10.3390/jcm10050998