
Different Features of Interleukin-37 and Interleukin-18 as Disease Activity Markers of Adult-Onset Still’s Disease


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and the Evaluation Period
2.2. Laboratory Studies
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Paired Comparison of Clinical Features and Laboratory Parameters between High and Low Disease Activity Status
3.3. Correlations between Disease Activity Parameters in High Disease Activity Status
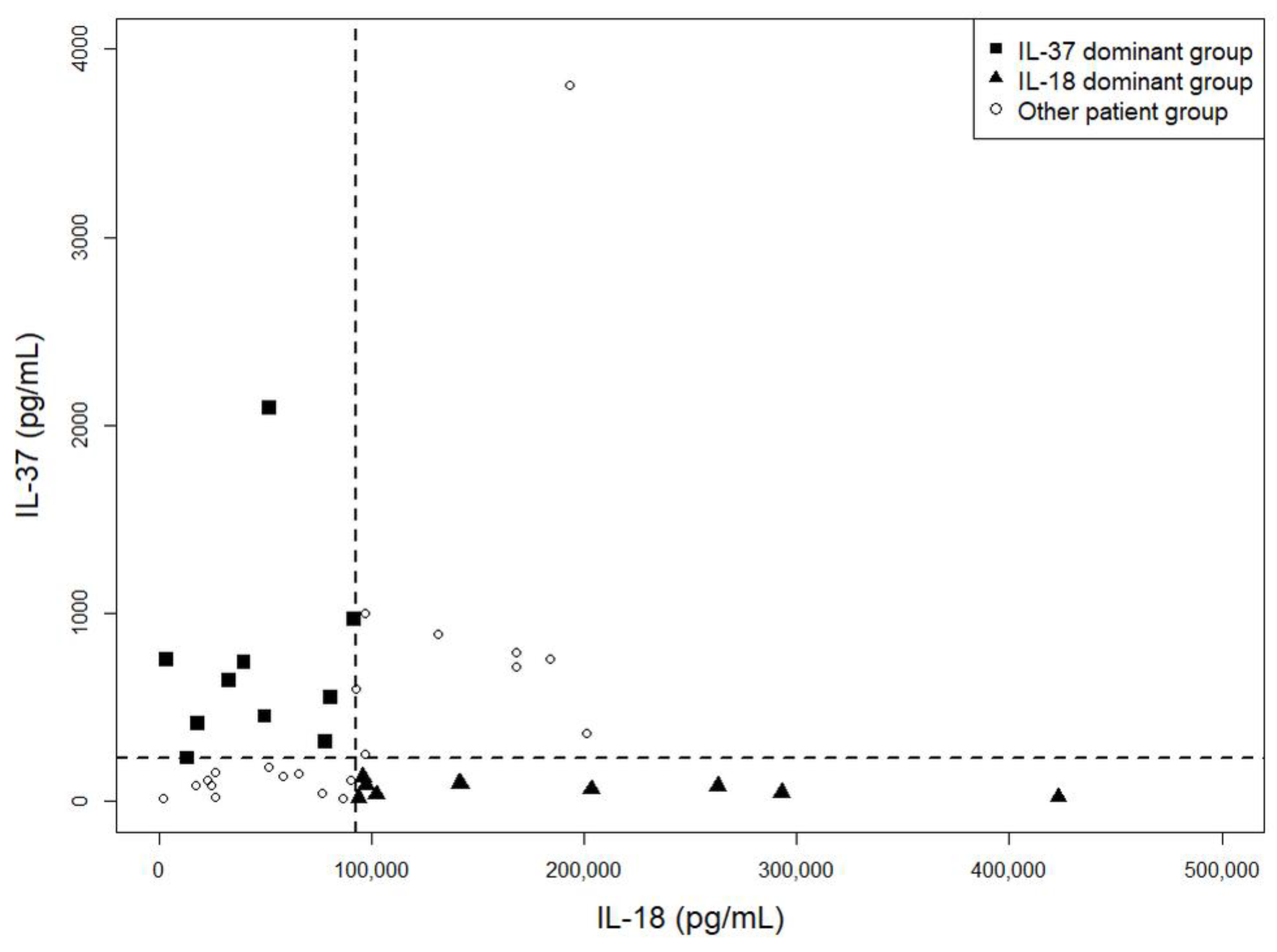
3.4. IL-37 and IL-18 in High Disease Activity Status of AOSD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mitrovic, S.; Fautrel, B. New markers for adult-onset still’s disease. Jt. Bone Spine 2018, 85, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.H.; Kim, J.J.; Lee, J.S.; Park, W.; Kim, T.H.; Jun, J.B.; Yoo, D.H. Interleukin-18 as an efficient marker for remission and follow-up in patients with inactive adult-onset still’s disease. Scand. J. Rheumatol. 2014, 43, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Pouchot, J.; Sampalis, J.S.; Beaudet, F.; Carette, S.; Decary, F.; Salusinsky-Sternbach, M.; Hill, R.O.; Gutkowski, A.; Harth, M.; Myhal, D.; et al. Adult still’s disease: Manifestations, disease course, and outcome in 62 patients. Medicine 1991, 70, 118–136. [Google Scholar] [CrossRef]
- Rau, M.; Schiller, M.; Krienke, S.; Heyder, P.; Lorenz, H.; Blank, N. Clinical manifestations but not cytokine profiles differentiate adult-onset still’s disease and sepsis. J. Rheumatol. 2010, 37, 2369–2376. [Google Scholar] [CrossRef]
- Kawaguchi, Y.; Terajima, H.; Harigai, M.; Hara, M.; Kamatani, N. Interleukin-18 as a novel diagnostic marker and indicator of disease severity in adult-onset still’s disease. Arthritis Rheum. 2001, 44, 1716–1717. [Google Scholar] [CrossRef]
- Feist, E.; Mitrovic, S.; Fautrel, B. Mechanisms, biomarkers and targets for adult-onset still’s disease. Nat. Rev. Rheumatol. 2018, 14, 603–618. [Google Scholar] [CrossRef]
- Kawashima, M.; Yamamura, M.; Taniai, M.; Yamauchi, H.; Tanimoto, T.; Kurimoto, M.; Miyawaki, S.; Amano, T.; Takeuchi, T.; Makino, H. Levels of interleukin-18 and its binding inhibitors in the blood circulation of patients with adult-onset still’s disease. Arthritis Rheum. 2001, 44, 550–560. [Google Scholar] [CrossRef]
- Priori, R.; Colafrancesco, S.; Alessandri, C.; Minniti, A.; Perricone, C.; Iaiani, G.; Palazzo, D.; Valesini, G. Interleukin 18: A biomarker for differential diagnosis between adult-onset still’s disease and sepsis. J. Rheumatol. 2014, 41, 1118–1123. [Google Scholar] [CrossRef]
- Shimizu, T.; Kikuchi-Taura, A.; Tsuji, S.; Matsushita, M.; Ohshima, S.; Saeki, Y. Up-regulation of cd64 expression on monocytes in patients with active adult-onset still disease: A possible biomarker of disease activity. J. Clin. Rheumatol. 2018. [Google Scholar] [CrossRef]
- Cavalli, G.; Dinarello, C.A. Suppression of inflammation and acquired immunity by il-37. Immunol. Rev. 2018, 281, 179–190. [Google Scholar] [CrossRef]
- Zhao, P.W.; Jiang, W.G.; Wang, L.; Jiang, Z.Y.; Shan, Y.X.; Jiang, Y.F. Plasma levels of il-37 and correlation with tnf-alpha, il-17a, and disease activity during dmard treatment of rheumatoid arthritis. PLoS ONE 2014, 9, e95346. [Google Scholar] [CrossRef]
- Ye, L.; Ji, L.; Wen, Z.; Zhou, Y.; Hu, D.; Li, Y.; Yu, T.; Chen, B.; Zhang, J.; Ding, L.; et al. Il-37 inhibits the production of inflammatory cytokines in peripheral blood mononuclear cells of patients with systemic lupus erythematosus: Its correlation with disease activity. J. Transl. Med. 2014, 12, 69. [Google Scholar] [CrossRef]
- Song, L.; Qiu, F.; Fan, Y.; Ding, F.; Liu, H.; Shu, Q.; Liu, W.; Li, X. Glucocorticoid regulates interleukin-37 in systemic lupus erythematosus. J. Clin. Immunol. 2013, 33, 111–117. [Google Scholar] [CrossRef]
- Chen, B.; Huang, K.; Ye, L.; Li, Y.; Zhang, J.; Zhang, J.; Fan, X.; Liu, X.; Li, L.; Sun, J.; et al. Interleukin-37 is increased in ankylosing spondylitis patients and associated with disease activity. J. Transl. Med. 2015, 13, 36. [Google Scholar] [CrossRef]
- Feng, M.; Kang, M.; He, F.; Xiao, Z.; Liu, Z.; Yao, H.; Wu, J. Plasma interleukin-37 is increased and inhibits the production of inflammatory cytokines in peripheral blood mononuclear cells in systemic juvenile idiopathic arthritis patients. J. Transl. Med. 2018, 16, 277. [Google Scholar] [CrossRef] [PubMed]
- Chi, H.; Liu, D.; Sun, Y.; Hu, Q.; Liu, H.; Cheng, X.; Ye, J.; Shi, H.; Yin, Y.; Liu, M.; et al. Interleukin-37 is increased in adult-onset still’s disease and associated with disease activity. Arthritis Res. Ther. 2018, 20, 54. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Ohta, A.; Tsunematsu, T.; Kasukawa, R.; Mizushima, Y.; Kashiwagi, H.; Kashiwazaki, S.; Tanimoto, K.; Matsumoto, Y.; Ota, T.; et al. Preliminary criteria for classification of adult still’s disease. J. Rheumatol. 1992, 19, 424–430. [Google Scholar] [PubMed]
- Kim, H.A.; An, J.M.; Nam, J.Y.; Jeon, J.Y.; Suh, C.H. Serum s100a8/a9, but not follistatin-like protein 1 and interleukin 18, may be a useful biomarker of disease activity in adult-onset still’s disease. J. Rheumatol. 2012, 39, 1399–1406. [Google Scholar] [CrossRef] [PubMed]
- Van de Veerdonk, F.L.; Netea, M.G. New insights in the immunobiology of il-1 family members. Front. Immunol. 2013, 4, 167. [Google Scholar] [CrossRef] [PubMed]
- Pan, G.; Risser, P.; Mao, W.; Baldwin, D.T.; Zhong, A.W.; Filvaroff, E.; Yansura, D.; Lewis, L.; Eigenbrot, C.; Henzel, W.J.; et al. Il-1h, an interleukin 1-related protein that binds il-18 receptor/il-1rrp. Cytokine 2001, 13, 1–7. [Google Scholar] [CrossRef]
- Garlanda, C.; Dinarello, C.A.; Mantovani, A. The interleukin-1 family: Back to the future. Immunity 2013, 39, 1003–1018. [Google Scholar] [CrossRef]
- Jia, H.; Liu, J.; Han, B. Reviews of interleukin-37: Functions, receptors, and roles in diseases. BioMed Res. Int. 2018, 2018, 3058640. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; Jiang, B.; Deng, J.; Du, J.; Xiong, W.; Guan, Y.; Wen, Z.; Huang, K.; Huang, Z. Il-37 alleviates rheumatoid arthritis by suppressing il-17 and il-17-triggering cytokine production and limiting th17 cell proliferation. J. Immunol. 2015, 194, 5110–5119. [Google Scholar] [CrossRef]
- Bufler, P.; Gamboni-Robertson, F.; Azam, T.; Kim, S.H.; Dinarello, C.A. Interleukin-1 homologues il-1f7b and il-18 contain functional mrna instability elements within the coding region responsive to lipopolysaccharide. Biochem. J. 2004, 381, 503–510. [Google Scholar] [CrossRef]
- Nold, M.F.; Nold-Petry, C.A.; Zepp, J.A.; Palmer, B.E.; Bufler, P.; Dinarello, C.A. Il-37 is a fundamental inhibitor of innate immunity. Nat. Immunol. 2010, 11, 1014–1022. [Google Scholar] [CrossRef]
- Tsutsumi, N.; Kimura, T.; Arita, K.; Ariyoshi, M.; Ohnishi, H.; Yamamoto, T.; Zuo, X.; Maenaka, K.; Park, E.Y.; Kondo, N.; et al. The structural basis for receptor recognition of human interleukin-18. Nat. Commun. 2014, 5, 5340. [Google Scholar] [CrossRef]
- Nold-Petry, C.A.; Lo, C.Y.; Rudloff, I.; Elgass, K.D.; Li, S.; Gantier, M.P.; Lotz-Havla, A.S.; Gersting, S.W.; Cho, S.X.; Lao, J.C.; et al. Il-37 requires the receptors il-18ralpha and il-1r8 (sigirr) to carry out its multifaceted anti-inflammatory program upon innate signal transduction. Nat. Immunol. 2015, 16, 354–365. [Google Scholar] [CrossRef] [PubMed]
- Kadavath, S.; Efthimiou, P. Adult-onset still’s disease-pathogenesis, clinical manifestations, and new treatment options. Ann. Med. 2015, 47, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Giacomelli, R.; Ruscitti, P.; Shoenfeld, Y. A comprehensive review on adult onset still’s disease. J. Autoimmun. 2018, 93, 24–36. [Google Scholar] [CrossRef]
- Sabnis, G.R.; Gokhale, Y.A.; Kulkarni, U.P. Tocilizumab in refractory adult-onset still’s disease with aseptic meningitis--efficacy of interleukin-6 blockade and review of the literature. Semin. Arthritis Rheum. 2011, 40, 365–368. [Google Scholar] [CrossRef] [PubMed]
- Cavalli, G.; Justice, J.N.; Boyle, K.E.; D’Alessandro, A.; Eisenmesser, E.Z.; Herrera, J.J.; Hansen, K.C.; Nemkov, T.; Stienstra, R.; Garlanda, C.; et al. Interleukin 37 reverses the metabolic cost of inflammation, increases oxidative respiration, and improves exercise tolerance. Proc. Natl. Acad. Sci. USA 2017, 114, 2313–2318. [Google Scholar] [CrossRef] [PubMed]
- Cavalli, G.; Koenders, M.; Kalabokis, V.; Kim, J.; Tan, A.C.; Garlanda, C.; Mantovani, A.; Dagna, L.; Joosten, L.A.; Dinarello, C.A. Treating experimental arthritis with the innate immune inhibitor interleukin-37 reduces joint and systemic inflammation. Rheumatology 2016, 55, 2220–2229. [Google Scholar] [CrossRef] [PubMed]
- Ballak, D.B.; Li, S.; Cavalli, G.; Stahl, J.L.; Tengesdal, I.W.; van Diepen, J.A.; Kluck, V.; Swartzwelter, B.; Azam, T.; Tack, C.J.; et al. Interleukin-37 treatment of mice with metabolic syndrome improves insulin sensitivity and reduces pro-inflammatory cytokine production in adipose tissue. J. Biol. Chem. 2018, 293, 14224–14236. [Google Scholar] [CrossRef] [PubMed]
- Kluck, V.; van Deuren, R.C.; Cavalli, G.; Shaukat, A.; Arts, P.; Cleophas, M.C.; Crisan, T.O.; Tausche, A.K.; Riches, P.; Dalbeth, N.; et al. Rare genetic variants in interleukin-37 link this anti-inflammatory cytokine to the pathogenesis and treatment of gout. Ann. Rheum. Dis. 2020, 79, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Suh, C.H.; Lee, Y.M.; Suh, Y.J.; Lee, S.K.; Kim, S.S.; Nahm, D.H.; Park, H.S. Serum cytokine profiles in patients with adult onset still’s disease. J. Rheumatol. 2003, 30, 2422–2427. [Google Scholar]
- Kudela, H.; Drynda, S.; Lux, A.; Horneff, G.; Kekow, J. Comparative study of interleukin-18 (il-18) serum levels in adult onset still’s disease (aosd) and systemic onset juvenile idiopathic arthritis (sjia) and its use as a biomarker for diagnosis and evaluation of disease activity. BMC Rheumatol. 2019, 3, 4. [Google Scholar] [CrossRef]
- Inoue, N.; Shimizu, M.; Tsunoda, S.; Kawano, M.; Matsumura, M.; Yachie, A. Cytokine profile in adult-onset still’s disease: Comparison with systemic juvenile idiopathic arthritis. Clin. Immunol. 2016, 169, 8–13. [Google Scholar] [CrossRef]
- Priori, R.; Barone, F.; Alessandri, C.; Colafrancesco, S.; McInnes, I.B.; Pitzalis, C.; Valesini, G.; Bombardieri, M. Markedly increased il-18 liver expression in adult-onset still’s disease-related hepatitis. Rheumatology 2011, 50, 776–780. [Google Scholar] [CrossRef] [PubMed]
- Finotto, S.; Siebler, J.; Hausding, M.; Schipp, M.; Wirtz, S.; Klein, S.; Protschka, M.; Doganci, A.; Lehr, H.A.; Trautwein, C.; et al. Severe hepatic injury in interleukin 18 (il-18) transgenic mice: A key role for il-18 in regulating hepatocyte apoptosis in vivo. Gut 2004, 53, 392–400. [Google Scholar] [CrossRef]
- Motoo, Y.; Ohta, H.; Okai, T.; Sawabu, N. Adult-onset still’s disease: Hepatic involvement and various serum markers relating to the disease activity. Jpn. J. Med. 1991, 30, 247–250. [Google Scholar] [CrossRef][Green Version]
- Khan, A.A.; Allemailem, K.S.; Alhumaydhi, F.A.; Gowder, S.J.T.; Rahmani, A.H. The biochemical and clinical perspectives of lactate dehydrogenase: An enzyme of active metabolism. Endocr. Metab. Immune Disord. Drug Targets 2020, 20, 855–868. [Google Scholar] [CrossRef] [PubMed]
- Tsutsui, H.; Matsui, K.; Okamura, H.; Nakanishi, K. Pathophysiological roles of interleukin-18 in inflammatory liver diseases. Immunol. Rev. 2000, 174, 192–209. [Google Scholar] [CrossRef] [PubMed]
- Tsutsui, H.; Kayagaki, N.; Kuida, K.; Nakano, H.; Hayashi, N.; Takeda, K.; Matsui, K.; Kashiwamura, S.; Hada, T.; Akira, S.; et al. Caspase-1-independent, fas/fas ligand-mediated il-18 secretion from macrophages causes acute liver injury in mice. Immunity 1999, 11, 359–367. [Google Scholar] [CrossRef]
- Pepys, M.B.; Hirschfield, G.M. C-reactive protein: A critical update. J. Clin. Investig. 2003, 111, 1805–1812. [Google Scholar] [CrossRef] [PubMed]
- Pieri, G.; Agarwal, B.; Burroughs, A.K. C-reactive protein and bacterial infection in cirrhosis. Ann. Gastroenterol. 2014, 27, 113–120. [Google Scholar]
- Lim, K.B.; Schiano, T.D. Still disease and the liver-an underappreciated association. Gastroenterol. Hepatol. 2011, 7, 844–846. [Google Scholar]
- Slaats, J.; Ten Oever, J.; van de Veerdonk, F.L.; Netea, M.G. Il-1beta/il-6/crp and il-18/ferritin: Distinct inflammatory programs in infections. PLoS Pathog. 2016, 12, e1005973. [Google Scholar] [CrossRef]
- Kowdley, K.V.; Belt, P.; Wilson, L.A.; Yeh, M.M.; Neuschwander-Tetri, B.A.; Chalasani, N.; Sanyal, A.J.; Nelson, J.E.; Nash Clinical Research Network. Serum ferritin is an independent predictor of histologic severity and advanced fibrosis in patients with nonalcoholic fatty liver disease. Hepatology 2012, 55, 77–85. [Google Scholar] [CrossRef]
- Hirata, S.; Tanaka, Y. Assessment of disease activity in rheumatoid arthritis by multi-biomarker disease activity (mbda) score. Nihon Rinsho Meneki Gakkai Kaishi 2016, 39, 37–41. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chen, D.Y.; Lan, J.L.; Lin, F.J.; Hsieh, T.Y. Proinflammatory cytokine profiles in sera and pathological tissues of patients with active untreated adult onset still’s disease. J. Rheumatol. 2004, 31, 2189–2198. [Google Scholar]
- Whitley, E.; Ball, J. Statistics review 6: Nonparametric methods. Crit Care 2002, 6, 509–513. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total Patients (n = 45) | |
|---|---|
| Age | 47.1 ± 14.0 |
| Female, n (%) | 39 (86.7) |
| Disease duration (months) | 59.5 ± 48.2 |
| Number of Yamaguchi criteria met at diagnosis | 6.3 ± 1.0 |
| AOSD onset symptom, n (%) | |
| Systemic | 11 (24.4) |
| Articular | 3 (6.7) |
| Combined | 31 (68.9) |
| Number of disease flares (per year) | 0.6 ± 0.4 |
| Disease duration until high disease activity status (months) | 28.9 ± 43.3 |
| Interval between high and low disease activity status (months) | 6.0 ± 2.7 |
| Medications used during the evaluation period, n (%) | |
| Corticosteroids | 45 (100) |
| Cumulative corticosteroid dose (mg) b | 2769.7 ± 1511.0 |
| Mean corticosteroid dose (mg/day) b | 17.1 ± 9.5 |
| Corticosteroid pulse therapy c | 8 (17.8) |
| Methotrexate | 35 (77.8) |
| Leflunomide | 10 (22.2) |
| Cyclosporin A | 18 (40.0) |
| Azathioprine | 2 (4.4) |
| Hydroxychloroquine | 5 (11.1) |
| IV immunoglobulin | 1 (2.2) |
| Tocilizumab | 3 (6.7) |
| Patients with re-flare after low disease activity status | |
| Re-flare within 1 year (missing = 3), n (%) | 14 (33.3) |
| Duration until re-flare (months) | 4.3 ± 4.8 |
| Re-flare within 2 years (missing = 10), n (%) | 19 (54.3) |
| Duration until re-flare (months) | 8.3 ± 7.5 |
| Death, n (%) | 1 (2.2) |
| High Disease Activity (mPouchot Score ≥ 4) | Low Disease Activity (mPouchot Score ≤ 2) | p | |
|---|---|---|---|
| Modified Pouchot score b | 6.0 (4.5–7.0) | 0 (0–0) | <0.01 |
| Fever | 39 (86.7) | 0 (0) | <0.01 |
| Evanescent rash | 37 (82.2) | 2 (4.4) | <0.01 |
| Sore throat | 30 (66.7) | 0 (0) | <0.01 |
| Arthritis | 33 (73.3) | 5 (11.1) | <0.01 |
| Myalgia | 31 (68.9) | 0 (0) | <0.01 |
| Pleuritis | 6 (13.3) | 0 (0) | 0.03 |
| Pericarditis | 2 (4.4) | 1 (2.2) | 0.32 |
| Pneumonitis | 12 (26.7) | 0 (0) | <0.01 |
| Lymphadenopathy | 14 (31.1) | 0 (0) | <0.01 |
| Hepatomegaly or abnormal LFT c | |||
| Hepatomegaly | 4 (8.9) | 0 (0) | 0.13 |
| Abnormal LFT c | 29 (64.4) | 3 (6.7) | <0.01 |
| WBC > 15,000 (109/L) | 19 (42.2) | 2 (4.4) | <0.01 |
| Ferritin > 3000 (ng/mL) | 22 (48.9) | 0 (0) | <0.01 |
| Laboratory findings b | |||
| WBC (109/L) | 12.8 (7.4–20.0) | 8.0 (6.9–10.1) | <0.01 |
| ESR (mm/hr) | 79.5 (34.0–101.0) | 13.0 (8.0–32.0) | <0.01 |
| CRP (mg/dL) | 7.5 (3.2–12.7) | 0.4 (0.2–0.4) | <0.01 |
| AST (U/L) | 38.0 (26.0–56.0) | 20.0 (16.0–23.0) | <0.01 |
| ALT (U/L) | 32.0 (17.0–56.0) | 16.0 (12.0–19.5) | <0.01 |
| LDH (U/L) | 368.0 (285.0–489.0) | 198.0 (161.0–240.0) | <0.01 |
| Ferritin (ng/mL) | 2628.0 (538.4–8791.0) | 59.3 (35.4–108.1) | <0.01 |
| IL-18 (pg/mL) | 92,874.2 (49,764.2–141,944.5) | 1316.0 (666.8–6069.9) | <0.01 |
| IL-37 (pg/mL) | 231.6 (86.5–754.0) | 29.2 (7.5–64.0) | <0.01 |
| mPouchot Score | ESR | CRP | Ferritin | AST | ALT | LDH | IL-18 | IL-37 | |
|---|---|---|---|---|---|---|---|---|---|
| mPouchot score | 1 | 0.515 ** | 0.481 ** | 0.616 ** | 0.247 | 0.228 | 0.236 | 0.399 ** | 0.355 * |
| ESR | 0.515 ** | 1 | 0.418 ** | 0.218 | −0.140 | −0.04 | −0.340 * | −0.126 | 0.270 |
| CRP | 0.481 ** | 0.418 ** | 1 | 0.424 ** | 0.09 | −0.09 | 0.079 | 0.287 | 0.573 ** |
| ferritin | 0.616 ** | 0.218 | 0.424 ** | 1 | 0.543 ** | 0.343 * | 0.564 ** | 0.656 ** | 0.336 * |
| AST | 0.247 | −0.140 | 0.090 | 0.543 * | 1 | 0.559 ** | 0.640 ** | 0.468 * | 0.026 |
| ALT | 0.228 | −0.040 | −0.087 | 0.343 * | 0.559 ** | 1 | 0.263 | 0.238 | −0.088 |
| LDH | 0.236 | −0.340* | 0.079 | 0.564 ** | 0.640 ** | 0.263 | 1 | 0.741 ** | 0.153 |
| IL-18 | 0.399 ** | −0.126 | 0.287 | 0.656 ** | 0.468 ** | 0.238 | 0.741 ** | 1 | 0.159 |
| IL-37 | 0.355 * | 0.270 | 0.573 ** | 0.336 * | 0.03 | −0.088 | 0.153 | 0.159 | 1 |
| IL-37 Dominant Group (n = 10) | IL-18 Dominant Group (n = 10) | p | |
|---|---|---|---|
| Disease activity parameters at high disease activity status | |||
| Modified Pouchot score | 7 (6–7) | 6 (6–7) | 0.97 |
| Laboratory findings | |||
| WBC (109/L) | 16.4 (8.4–24.0) | 10.8 (6.3–17.0) | 0.25 |
| ESR (mm/hr) | 102.5 (62.0–115.0) | 73.0 (36.0–83.0) | 0.09 |
| CRP (mg/dL) | 8.8 (5.3–15.0) | 4.1 (2.8–7.6) | 0.11 |
| AST (U/L) | 30.5 (22.0–40.0) | 42.0 (29.0–69.0) | 0.17 |
| ALT (U/L) | 23.5 (12.0–49.0) | 45.0 (17.0–90.0) | 0.12 |
| LDH (U/L) | 302.0 (246.0–354.0) | 492.0 (355.0–522.0) | 0.01 |
| Ferritin (ng/mL) | 2069.5 (727.0–2628.0) | 5246.5 (2268.0–11254.0) | 0.11 |
| Medications used during the evaluation period | |||
| Corticosteroids, n (%) | 10 (100) | 10 (100) | 1.00 |
| Cumulative corticosteroid dose (mg) b | 2590.0 (1675.0–3155.0) | 2672.5 (2000.0–3307.5) | 0.80 |
| Mean corticosteroid dose (mg/day) b | 12.9 (10.7–23.7) | 24.6 (17.3–26.4) | 0.02 |
| Corticosteroid pulse therapyc, n (%) | 4 (40.0) | 0 (0.0) | 0.09 |
| Methotrexate, n (%) | 8 (80.0) | 7 (70.0) | 1.00 |
| Leflunomide, n (%) | 1 (10.0) | 5 (50.0) | 0.14 |
| Cyclosporin A, n (%) | 3 (30.0) | 5 (50.0) | 0.65 |
| Disease Manifestation | n | Serum IL-37 (pg/mL) a | p | Serum IL-18 (pg/mL) b | p |
|---|---|---|---|---|---|
| Fever | (+), n = 39 | 320.6 (87.1–794.9) | 0.09 | 95,879.0 (51,460.0–168,103.9) | 0.14 |
| (−), n = 6 | 88.3 (24.4–150.0) | 46,295.9 (22,779.3–86,407.4) | |||
| Skin rash | (+), n = 37 | 231.6 (94.5–740.1) | 0.58 | 90,140.0 (39,970.0–131,420.0) | 0.14 |
| (−), n = 8 | 339.3 (30.2–857.2) | 143,178.8 (72,357.1–342,925.0) | |||
| Sore throat | (+), n = 30 | 434.4 (97.1–794.9) | 0.10 | 88,979.8 (32,665.4–131,420.0) | 0.14 |
| (−), n = 15 | 114.4 (47.7–365.2) | 95,879.0 (76,861.7–203,430.2) | |||
| Arthritis | (+), n = 33 | 185.0 (86.5–740.1) | 0.34 | 90,140.0 (39,970.0–131,420.0) | 0.15 |
| (−), n = 12 | 409.4 (99.0–2383.6) | 116,849.2 (57,839.5–232,115.6) | |||
| Myalgia | (+), n = 31 | 157.4 (82.5–740.1) | 0.53 | 80,626.0 (32,665.4–141,081.1) | 0.40 |
| (−), n = 14 | 409.4 (86.5–794.9) | 94,815.6 (86,407.3–184,044.8) | |||
| Pleuritis | (+), n = 6 | 444.7 (64.3–5160.0) | 0.73 | 154,595.5 (131,385.5–203,430.2) | 0.02 |
| (−), n = 39 | 231.6 (86.5–740.1) | 86,407.3 (32,665.4–131,420.0) | |||
| Pericarditis | (+), n = 2 | 532.1 (64.3–1000.0) | 0.89 | 150,216.7 (97,003.2–203,430.2) | 0.26 |
| (−), n = 43 | 231.6 (86.5–754.0) | 91,552.2 (39,970.0–141,944.5) | |||
| Pneumonitis | (+), n = 12 | 504.2 (172.6–978.6) | 0.17 | 116,849.2 (88,691.5–184,742.5) | 0.05 |
| (−), n = 33 | 150.0 (85.5–716.0) | 86,407.3 (26,677.0–131,420.0) | |||
| Lymphadenopathy | (+), n = 14 | 409.4 (157.4–794.9) | 0.14 | 131,402.8 (78,019.7–168,103.9) | 0.12 |
| (−), n = 31 | 137.7 (64.3–740.1) | 86,407.3 (32,665.4–102,312.8) | |||
| Hepatomegaly | (+), n = 4 | 458.4 (170.8–776.6) | 0.89 | 93,422.0 (85,447.0–874,084.9) | 0.49 |
| (−), n = 41 | 185.0 (86.5–754.0) | 91,552.2 (39,970.0–141,944.5) | |||
| Abnormal LFT | (+), n = 29 | 231.6 (85.5–740.1) | 0.86 | 97,003.2 (65,914.8–168,103.9) | 0.03 |
| (−), n = 16 | 239.0 (90.5–755.6) | 67,616.7 (22,186.5–97,900.1) | |||
| WBC > 15,000 (109/L) c | (+), n = 19 | 716.0 (231.6–972.9) | <0.01 | 97,003.2 (51,840.0–168,103.9) | 0.36 |
| (−), n = 26 | 123.5 (64.3–320.6) | 82,213.5 (26,677.0–141,081.1) | |||
| Ferritin > 3000 (ng/mL) d | (+), n = 22 | 656.1 (82.5–957.1) | 0.18 | 154,592.5 (96,757.0–203,430.2) | <0.01 |
| (−), n = 23 | 150.0 (87.1–453.5) | 58,371.8 (22,779.3–90,140.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nam, S.W.; Kang, S.; Lee, J.H.; Yoo, D.H. Different Features of Interleukin-37 and Interleukin-18 as Disease Activity Markers of Adult-Onset Still’s Disease. J. Clin. Med. 2021, 10, 910. https://doi.org/10.3390/jcm10050910
Nam SW, Kang S, Lee JH, Yoo DH. Different Features of Interleukin-37 and Interleukin-18 as Disease Activity Markers of Adult-Onset Still’s Disease. Journal of Clinical Medicine. 2021; 10(5):910. https://doi.org/10.3390/jcm10050910
Chicago/Turabian StyleNam, Seoung Wan, SuMan Kang, Jun Hyeok Lee, and Dae Hyun Yoo. 2021. "Different Features of Interleukin-37 and Interleukin-18 as Disease Activity Markers of Adult-Onset Still’s Disease" Journal of Clinical Medicine 10, no. 5: 910. https://doi.org/10.3390/jcm10050910
APA StyleNam, S. W., Kang, S., Lee, J. H., & Yoo, D. H. (2021). Different Features of Interleukin-37 and Interleukin-18 as Disease Activity Markers of Adult-Onset Still’s Disease. Journal of Clinical Medicine, 10(5), 910. https://doi.org/10.3390/jcm10050910