
The Gustave Roussy Immune (GRIm)-Score Variation Is an Early-on-Treatment Biomarker of Outcome in Advanced Non-Small Cell Lung Cancer (NSCLC) Patients Treated with First-Line Pembrolizumab

 , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Study Population and Data Collection
2.3. Study Objectives
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
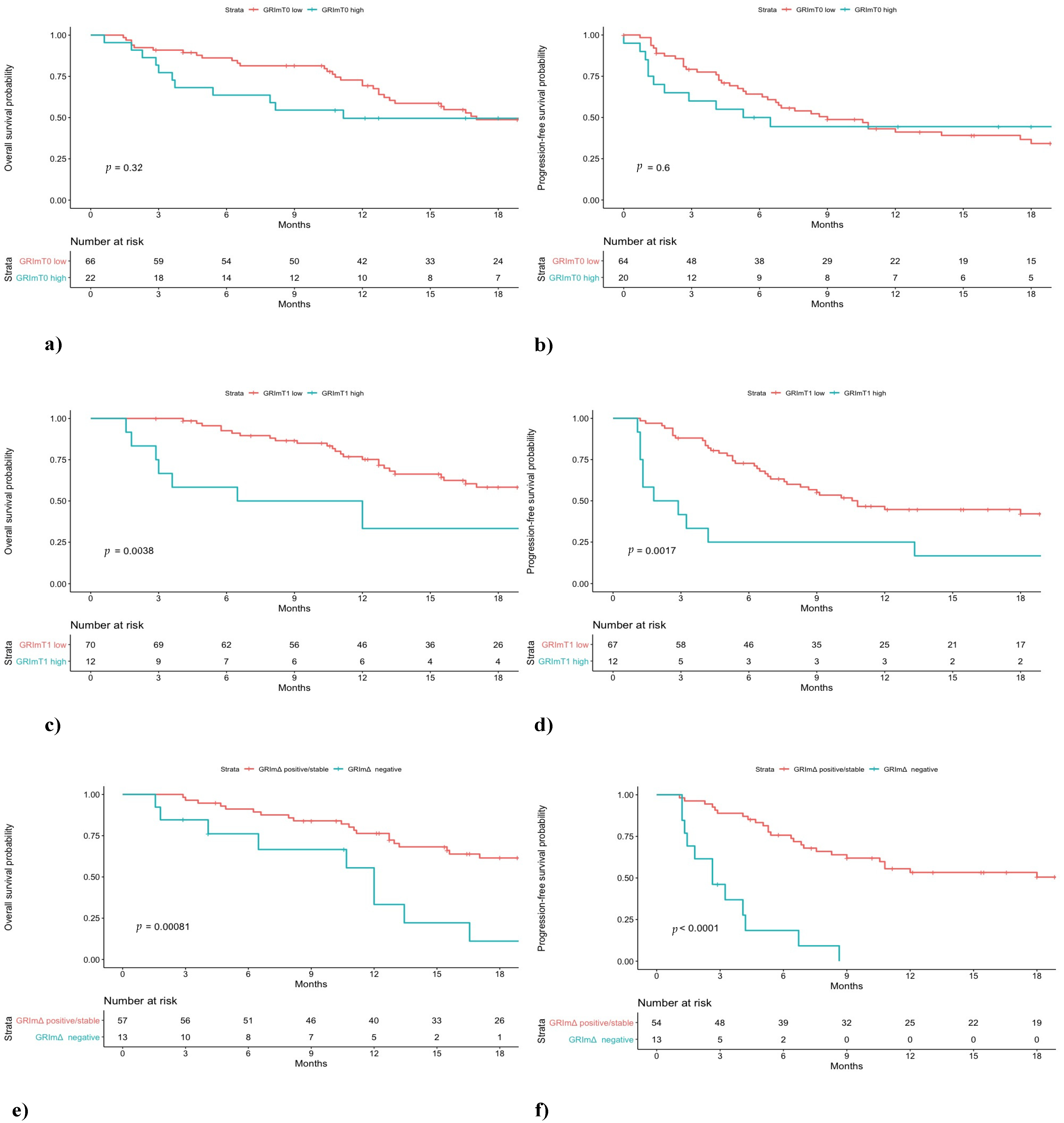
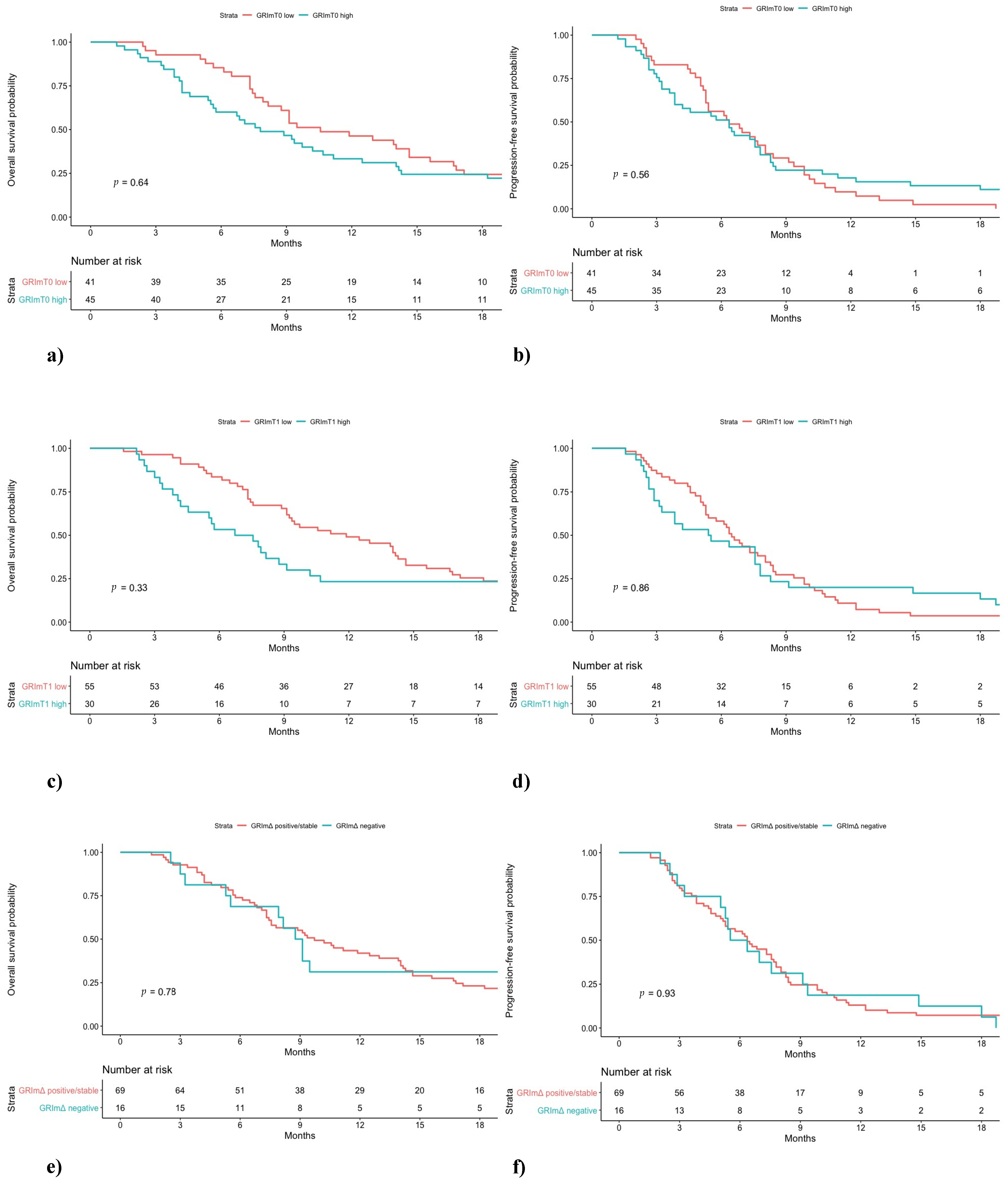
3.2. Clinical Outcome According to GRImT0
3.3. Clinical Outcome According to GRImT1
3.4. Clinical Outcome According to GRImΔ
3.5. Multivariate Analysis and Case-Control Random Matching
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Besse, B.; Adjei, A.; Baas, P.; Meldgaard, P.; Nicolson, M.; Paz-Ares, L.; Reck, M.; Smit, E.F.; Syrigos, K.; Stahel, R.; et al. 2nd ESMO Consensus Conference on Lung Cancer: Non-small-cell lung cancer first-line/second and further lines in advanced disease. Ann. Oncol. 2014. [Google Scholar] [CrossRef]
- Paz-Ares, L.G.; De Marinis, F.; Dediu, M.; Thomas, M.; Pujol, J.L.; Bidoli, P.; Molinier, O.; Sahoo, T.P.; Laack, E.; Reck, M.; et al. PARAMOUNT: Final overall survival results of the phase III study of maintenance pemetrexed versus placebo immediately after induction treatment with pemetrexed plus cisplatin for advanced nonsquamous non-small-cell lung cancer. J. Clin. Oncol. 2013. [Google Scholar] [CrossRef]
- Scagliotti, G.V.; Parikh, P.; Von Pawel, J.; Biesma, B.; Vansteenkiste, J.; Manegold, C.; Serwatowski, P.; Gatzemeier, U.; Digumarti, R.; Zukin, M.; et al. Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naive patients with advanced-stage non-small-cell lung cancer. J. Clin. Oncol. 2008. [Google Scholar] [CrossRef]
- Cortellini, A.; Tiseo, M.; Banna, G.L.; Cappuzzo, F.; Aerts, J.G.J.V.; Barbieri, F.; Giusti, R.; Bria, E.; Cortinovis, D.; Grossi, F.; et al. Clinicopathologic correlates of first-line pembrolizumab effectiveness in patients with advanced NSCLC and a PD-L1 expression of ≥ 50%. Cancer Immunol. Immunother. 2020. [Google Scholar] [CrossRef]
- Rolfo, C.; Caglevic, C.; Santarpia, M.; Araujo, A.; Giovannetti, E.; Gallardo, C.D.; Pauwels, P.; Mahave, M. Immunotherapy in NSCLC: A promising and revolutionary weapon. Adv. Exp. Med. Biol. 2017. [Google Scholar] [CrossRef]
- Osmani, L.; Askin, F.; Gabrielson, E.; Li, Q.K. Current WHO guidelines and the critical role of immunohistochemical markers in the subclassification of non-small cell lung carcinoma (NSCLC): Moving from targeted therapy to immunotherapy. Semin. Cancer Biol. 2018. [Google Scholar] [CrossRef]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crinò, L.; Eberhardt, W.E.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2015. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Updated analysis of KEYNOTE-024: Pembrolizumab versus platinum-based chemotherapy for advanced non–small-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J. Clin. Oncol. 2019. [Google Scholar] [CrossRef]
- Cantini, L.; Merloni, F.; Rinaldi, S.; Lenci, E.; Marcantognini, G.; Meletani, T.; Fiordoliva, I.; Morgese, F.; Torniai, M.; Ricci, G.; et al. Electrolyte disorders in advanced non-small cell lung cancer patients treated with immune check-point inhibitors: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2020. [Google Scholar] [CrossRef]
- Frelaut, M.; Le Tourneau, C.; Borcoman, E. Hyperprogression under immunotherapy. Int. J. Mol. Sci. 2019, 20, 2674. [Google Scholar] [CrossRef]
- Cortellini, A.; Friedlaender, A.; Banna, G.L.; Porzio, G.; Bersanelli, M.; Cappuzzo, F.; Aerts, J.G.J.V.; Giusti, R.; Bria, E.; Cortinovis, D.; et al. Immune-related Adverse Events of Pembrolizumab in a Large Real-world Cohort of Patients With NSCLC With a PD-L1 Expression ≥ 50% and Their Relationship With Clinical Outcomes. Clin. Lung Cancer 2020. [Google Scholar] [CrossRef]
- Petrelli, F.; Cabiddu, M.; Coinu, A.; Borgonovo, K.; Ghilardi, M.; Lonati, V.; Barni, S. Prognostic role of lactate dehydrogenase in solid tumors: A systematic review and meta-analysis of 76 studies. Acta Oncol. 2015. [Google Scholar] [CrossRef]
- Zhang, Z.; Li, Y.; Yan, X.; Song, Q.; Wang, G.; Hu, Y.; Jiao, S.; Wang, J. Pretreatment lactate dehydrogenase may predict outcome of advanced non small-cell lung cancer patients treated with immune checkpoint inhibitors: A meta-analysis. Cancer Med. 2019. [Google Scholar] [CrossRef]
- Diem, S.; Schmid, S.; Krapf, M.; Flatz, L.; Born, D.; Jochum, W.; Templeton, A.J.; Früh, M. Neutrophil-to-Lymphocyte ratio (NLR) and Platelet-to-Lymphocyte ratio (PLR) as prognostic markers in patients with non-small cell lung cancer (NSCLC) treated with nivolumab. Lung Cancer 2017. [Google Scholar] [CrossRef]
- Mezquita, L.; Auclin, E.; Ferrara, R.; Charrier, M.; Remon, J.; Planchard, D.; Ponce, S.; Ares, L.P.; Leroy, L.; Audigier-Valette, C.; et al. Association of the lung immune prognostic index with immune checkpoint inhibitor outcomes in patients with advanced non-small cell lung cancer. JAMA Oncol. 2018. [Google Scholar] [CrossRef]
- Ruiz-Bañobre, J.; Areses-Manrique, M.C.; Mosquera-Martínez, J.; Cortegoso, A.; Afonso-Afonso, F.J.; De Dios-Álvarez, N.; Fernández-Núñez, N.; Azpitarte-Raposeiras, C.; Amenedo, M.; Santomé, L.; et al. Evaluation of the lung immune prognostic index in advanced nonsmall cell lung cancer patients under nivolumab monotherapy. Transl. Lung Cancer Res. 2019. [Google Scholar] [CrossRef]
- Minami, S.; Ihara, S.; Ikuta, S.; Komuta, K. Gustave Roussy Immune Score and Royal Marsden Hospital Prognostic Score Are Biomarkers of Immune-Checkpoint Inhibitor for Non-Small Cell Lung Cancer. World J. Oncol. 2019. [Google Scholar] [CrossRef]
- Lalani, A.K.A.; Xie, W.; Martini, D.J.; Steinharter, J.A.; Norton, C.K.; Krajewski, K.M.; Duquette, A.; Bossé, D.; Bellmunt, J.; Van Allen, E.M.; et al. Change in Neutrophil-to-lymphocyte ratio (NLR) in response to immune checkpoint blockade for metastatic renal cell carcinoma. J. Immunother. Cancer 2018. [Google Scholar] [CrossRef]
- Simonaggio, A.; Elaidi, R.; Fournier, L.; Fabre, E.; Ferrari, V.; Borchiellini, D.; Thouvenin, J.; Barthelemy, P.; Thibault, C.; Tartour, E.; et al. Variation in neutrophil to lymphocyte ratio (NLR) as predictor of outcomes in metastatic renal cell carcinoma (mRCC) and non-small cell lung cancer (mNSCLC) patients treated with nivolumab. Cancer Immunol. Immunother. 2020. [Google Scholar] [CrossRef]
- Bigot, F.; Castanon, E.; Baldini, C.; Hollebecque, A.; Carmona, A.; Postel-Vinay, S.; Angevin, E.; Armand, J.P.; Ribrag, V.; Aspeslagh, S.; et al. Prospective validation of a prognostic score for patients in immunotherapy phase I trials: The Gustave Roussy Immune Score (GRIm-Score). Eur. J. Cancer 2017. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018. [Google Scholar] [CrossRef]
- Mok, T.S.K.; Wu, Y.L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019. [Google Scholar] [CrossRef]
- Cantini, L.; Pecci, F.; Hurkmans, D.P.; Belderbos, R.A.; Lanese, A.; Copparoni, C.; Aerts, S.; Cornelissen, R.; Dumoulin, D.W.; Fiordoliva, I.; et al. High-intensity statins are associated with improved clinical activity of PD-1 inhibitors in malignant pleural mesothelioma and advanced non-small cell lung cancer patients. Eur. J. Cancer 2021. [Google Scholar] [CrossRef]
- Cortellini, A.; De Giglio, A.; Cannita, K.; Cortinovis, D.L.; Cornelissen, R.; Baldesarri, C.; Giusti, R.; D’Argento, E.; Grossi, F.; Santoni, M.; et al. Smoking status during first-line immunotherapy and chemotherapy in NSCLC patients: A case–control matched analysis from a large multicenter study. Thorac. Cancer 2021. [Google Scholar] [CrossRef]
- Cortellini, A.; Ricciuti, B.; Tiseo, M.; Bria, E.; Banna, G.L.; Aerts, J.G.J.V.; Barbieri, F.; Giusti, R.; Cortinovis, D.L.; Migliorino, M.R.; et al. Baseline BMI and BMI variation during first line pembrolizumab in NSCLC patients with a PD-L1 expression ≥ 50%: A multicenter study with external validation. J. Immunother. Cancer 2020. [Google Scholar] [CrossRef]
- Marabelle, A.; Fakih, M.G.; Lopez, J.; Shah, M.; Shapira-Frommer, R.; Nakagawa, K.; Chung, H.C.; Kindler, H.L.; Lopez-Martin, J.A.; Miller, W.; et al. Association of tumour mutational burden with outcomes in patients with select advanced solid tumours treated with pembrolizumab in KEYNOTE-158. Ann. Oncol. 2019. [Google Scholar] [CrossRef]
- Kümpers, C.; Jokic, M.; Haase, O.; Offermann, A.; Vogel, W.; Grätz, V.; Langan, E.A.; Perner, S.; Terheyden, P. Immune Cell Infiltration of the Primary Tumor, Not PD-L1 Status, Is Associated With Improved Response to Checkpoint Inhibition in Metastatic Melanoma. Front. Med. 2019. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, Z.; Hu, Y.; Yan, X.; Song, Q.; Wang, G.; Chen, R.; Jiao, S.; Wang, J. Pretreatment Neutrophil-to-Lymphocyte Ratio (NLR) May Predict the Outcomes of Advanced Non-small-cell Lung Cancer (NSCLC) Patients Treated With Immune Checkpoint Inhibitors (ICIs). Front. Oncol. 2020. [Google Scholar] [CrossRef]
- Soyano, A.E.; Dholaria, B.; Marin-Acevedo, J.A.; Diehl, N.; Hodge, D.; Luo, Y.; Manochakian, R.; Chumsri, S.; Adjei, A.; Knutson, K.L.; et al. Peripheral blood biomarkers correlate with outcomes in advanced non-small cell lung Cancer patients treated with anti-PD-1 antibodies. J. Immunother. Cancer 2018. [Google Scholar] [CrossRef]
- Khunger, M.; Patil, P.D.; Khunger, A.; Li, M.; Hu, B.; Rakshit, S.; Basu, A.; Pennell, N.; Stevenson, J.P.; Elson, P.; et al. Post-treatment changes in hematological parameters predict response to nivolumab monotherapy in non-small cell lung cancer patients. PLoS ONE 2018. [Google Scholar] [CrossRef]
- Dusselier, M.; Deluche, E.; Delacourt, N.; Ballouhey, J.; Egenod, T.; Melloni, B.; Vergnenègre, C.; Veillon, R.; Vergnenègre, A. Neutrophil-to-lymphocyte ratio evolution is an independent predictor of early progression of second-line nivolumab-treated patients with advanced non-small-cell lung cancers. PLoS ONE 2019. [Google Scholar] [CrossRef]
- Criscitiello, C.; Marra, A.; Morganti, S.; Zagami, P.; Viale, G.; Esposito, A.; Curigliano, G. Pretreatment Blood Parameters Predict Efficacy from Immunotherapy Agents in Early Phase Clinical Trials. Oncologist 2020. [Google Scholar] [CrossRef]
- Cantini, L.; Belderbos, R.A.; Gooijer, C.J.; Dumoulin, D.W.; Cornelissen, R.; Baart, S.; Burgers, J.A.; Baas, P.; Aerts, J.G.J.V. Nivolumab in pre-treated malignant pleural mesothelioma: Real-world data from the Dutch expanded access program. Transl. Lung Cancer Res. 2020. [Google Scholar] [CrossRef]
- Minami, S.; Ihara, S.; Komuta, K. Gustave Roussy Immune Score Is a Prognostic Factor for Chemotherapy-Naive Pulmonary Adenocarcinoma With Wild-Type Epidermal Growth Factor Receptor. World J. Oncol. 2019. [Google Scholar] [CrossRef]
- Russo, G.L.; Facchinetti, F.; Tiseo, M.; Garassino, M.C.; Ferrara, R. Hyperprogressive Disease upon Immune Checkpoint Blockade: Focus on Non–small Cell Lung Cancer. Curr. Oncol. Rep. 2020. [Google Scholar] [CrossRef]
- Banna, G.L.; Signorelli, D.; Metro, G.; Galetta, D.; De Toma, A.; Cantale, O.; Banini, M.; Friedlaender, A.; Pizzutillo, P.; Garassino, M.C.; et al. Neutrophil-to-lymphocyte ratio in combination with PD-L1 or lactate dehydrogenase as biomarkers for high PD-L1 non-small cell lung cancer treated with first-line pembrolizumab. Transl. Lung Cancer Res. 2020. [Google Scholar] [CrossRef]
- Sakurada, T.; Kakiuchi, S.; Tajima, S.; Horinouchi, Y.; Konaka, K.; Okada, N.; Nishisako, H.; Nakamura, T.; Teraoka, K.; Kawazoe, K.; et al. Pemetrexed-induced rash may be prevented by supplementary corticosteroids. Biol. Pharm. Bull. 2015. [Google Scholar] [CrossRef][Green Version]



{kind=link}
{kind=link}
| Characteristic | Pembrolizumab No. (%) | Chemotherapy No. (%) | p-Value a |
|---|---|---|---|
| Total | 135 (61) | 87 (39) | |
| Median age (range) | 71 (44–91) | 73 (36–88) | 0.12 |
| Sex | |||
| Male | 84 (62) | 59 (68) | |
| Female | 51 (38) | 28 (32) | 0.48 |
| ECOG PS | |||
| 0–1 | 103 (76) | 81 (93) | |
| ≥2 | 26 (19) | 6 (7) | 0.01 |
| Unknown | 6 (5) | 0 (0) | |
| Smoking status | |||
| Never smoker | 16 (12) | 5 (6) | |
| Current/former smoker | 116 (86) | 77 (88) | 0.22 |
| Unknown | 3 (2) | 5 (6) | |
| Tumor histotype | |||
| Adenocarcinoma | 113 (84) | 68 (78) | |
| Non Adenocarcinoma | 18 (13) | 09 (10) | 0.83 |
| Unknown | 4 (3) | 10 (12) | |
| PD-L1 | |||
| 50–77% | 56 (42) | NA | |
| 78–100% | 55 (40) | NA | NA |
| >50 % (not otherwise specified) | 24 (18) | NA | |
| Number of metastatic sites | |||
| ≤2 metastatic sites | 73 (54) | 62 (71) | |
| >2 metastatic sites | 62 (46) | 25 (29) | 0.01 |
| Metastatic sites | |||
| Brain metastases | |||
| No | 112 (83) | 71 (82) | |
| Yes | 23 (17) | 16 (18) | 0.93 |
| Liver metastases | |||
| No | 113 (84) | 75 (86) | |
| Yes | 22 (16) | 12 (14) | 0.75 |
| Bone metastases | |||
| No | 93 (69) | 57 (65) | |
| Yes | 42 (31) | 30 (35) | 0.70 |
| GRImT0 | |||
| Low (0–1) | 66 (49) | 41 (47) | |
| High (2–3) | 22 (16) | 45 (53) | <0.01 |
| Unknown | 47 (35) | 0 (0) | |
| GRImT1 | |||
| Low (0–1) | 70 (52) | 55 (63) | |
| High (2–3) | 12 (8) | 30 (35) | <0.01 |
| Unknown | 53 (40) | 2 (2) | |
| GRImΔ | |||
| Positive/stable Negative Unknown | 57 (42) 13 (10) 65 (48) | 69 (79) 16 (18) 2 (2) | 1 |
| ORR | |||
| CR/PR | 75 (55) | 34 (40) | |
| SD/PD | 45 (33) | 38 (44) | <0.01 |
| Unknown | 15 (12) | 15 (16) | |
| Median PFS (months) | 7.0 (95% CI 5.3–12.0) | 6.4 (95% CI 5.3–7.6) | <0.01 |
| Median OS (months) | 15.6 (95% CI 12.0–NR) | 9.2 (95% CI 7.6–13.0) | <0.01 |
| Test Variables | ORR OR (95% CI) | p-Value | PFS HR (95% CI) | p-Value | OS HR (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| GRImT1 low (ref.)/high | 0.79 (0.52–1.20) | 0.29 | 3.05 (1.42–6.54) | <0.01 a | 2.63 (1.18–5.86) | 0.01 a |
| Never smokers (ref.)/ Current-former smokers | 1.19 (0.71–1.96) | 0.50 | 0.97 (0.29–3.26) | 0.96 | 0.41 (0.12–1.44) | 0.16 |
| ECOG PS 0–1 (ref.)/≥2 | 0.83 (0.57–1.20) | 0.34 | 1.29 (0.61–2.72) | 0.49 | 1.14 (0.46–2.81) | 0.76 |
| Non adenocarcinoma (ref.)/ Adenocarcinoma | 0.71 (0.49–1.02) | 0.07 | – | – | – | – |
| Metastatic sites ≤2/>2 | – | – | 2.18 (1.14–4.17) | 0.02 a | 1.75 (0.88–3.49) | 0.10 |
| PD-L1 percentage <78/≥78 | 1.32 (1.02–1.71) | 0.04 a | – | – | – | – |
| Liver metastases No. (ref.)/Yes | – | – | 1.24 (0.52–2.96) | 0.61 | – | – |
| Bone metastases No. (ref.)/Yes | 0.79 (0.59–1.06) | 0.12 | – | – | – | – |
| Test Variables | ORR OR (95% CI) | p-Value | PFS HR (95% CI) | p-Value | OS HR (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| GRImΔ positive-stable (ref.)/negative | 0.74 (0.50–1.08) | 0.12 | 6.98 (2.94–16.61) | <0.01 a | 3.28 (1.39–7.74) | <0.01 a |
| Never smokers (ref.)/ Current-former smokers | 1.13 (0.67–1.89) | 0.64 | 0.83 (0.24–2.90) | 0.78 | 0.34 (0.09–1.21) | 0.10 |
| ECOG PS 0–1 (ref.)/≥2 | 0.87 (0.58–1.29) | 0.50 | 0.95 (0.38–2.38) | 0.92 | 0.81 (0.27–2.43) | 0.71 |
| Non adenocarcinoma (ref.)/ Adenocarcinoma | 0.79 (0.54–1.15) | 0.22 | – | – | – | – |
| Metastatic sites ≤2/>2 | – | – | 1.28 (0.59–2.77) | 0.52 | 1.15 (0.54–2.47) | 0.70 |
| PD-L1 percentage <78/≥78 | 1.21 (0.91–1.60) | 0.17 | – | – | – | – |
| Liver metastases No. (ref.)/Yes | – | – | 2.14 (0.85–5.40) | 0.10 | – | – |
| Bone metastases No. (ref.)/Yes | 0.85 (0.62–1.15) | 0.30 | – | – | – | – |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lenci, E.; Cantini, L.; Pecci, F.; Cognigni, V.; Agostinelli, V.; Mentrasti, G.; Lupi, A.; Ranallo, N.; Paoloni, F.; Rinaldi, S.; et al. The Gustave Roussy Immune (GRIm)-Score Variation Is an Early-on-Treatment Biomarker of Outcome in Advanced Non-Small Cell Lung Cancer (NSCLC) Patients Treated with First-Line Pembrolizumab. J. Clin. Med. 2021, 10, 1005. https://doi.org/10.3390/jcm10051005
Lenci E, Cantini L, Pecci F, Cognigni V, Agostinelli V, Mentrasti G, Lupi A, Ranallo N, Paoloni F, Rinaldi S, et al. The Gustave Roussy Immune (GRIm)-Score Variation Is an Early-on-Treatment Biomarker of Outcome in Advanced Non-Small Cell Lung Cancer (NSCLC) Patients Treated with First-Line Pembrolizumab. Journal of Clinical Medicine. 2021; 10(5):1005. https://doi.org/10.3390/jcm10051005
Chicago/Turabian StyleLenci, Edoardo, Luca Cantini, Federica Pecci, Valeria Cognigni, Veronica Agostinelli, Giulia Mentrasti, Alessio Lupi, Nicoletta Ranallo, Francesco Paoloni, Silvia Rinaldi, and et al. 2021. "The Gustave Roussy Immune (GRIm)-Score Variation Is an Early-on-Treatment Biomarker of Outcome in Advanced Non-Small Cell Lung Cancer (NSCLC) Patients Treated with First-Line Pembrolizumab" Journal of Clinical Medicine 10, no. 5: 1005. https://doi.org/10.3390/jcm10051005
APA StyleLenci, E., Cantini, L., Pecci, F., Cognigni, V., Agostinelli, V., Mentrasti, G., Lupi, A., Ranallo, N., Paoloni, F., Rinaldi, S., Nicolardi, L., Caglio, A., Aerts, S., Cortellini, A., Ficorella, C., Chiari, R., Di Maio, M., Dingemans, A.-M. C., Aerts, J. G. J. V., & Berardi, R. (2021). The Gustave Roussy Immune (GRIm)-Score Variation Is an Early-on-Treatment Biomarker of Outcome in Advanced Non-Small Cell Lung Cancer (NSCLC) Patients Treated with First-Line Pembrolizumab. Journal of Clinical Medicine, 10(5), 1005. https://doi.org/10.3390/jcm10051005