Abstract
The aim of this analysis was to assess the quality of reporting of randomized controlled trials (RCTs) relating to pain management in rotator cuff (RC) tears. This review evaluated the quality of the studies in the literature regarding this topic through the use of some factors and trends. The online databases used to search all RCTs on the topic of RC surgery were Medline, Scopus, CINAHL, EMBASE, and CENTRAL. This research was completed in September 2020. To assess the quality of reports, the Consolidated Standards of Reporting Trials (CONSORT) and the modified Coleman methodology score (MCMS) were used. From the research, 262 articles emerged. Finally, 79 studies were included in this historical analysis. There were no statistically significant changes in MCMS across trials that included or did not include a CONSORT diagram (p = 0.10). A statistically significant difference in MCMS was discovered between papers produced prior to 2009 and publications produced after 2015 (p = 0.03). There was no association between the number of checklist items for each article and the Coleman score. During the years there has been a significant increase in both quantity and quality of RCTs relating to pain in RC tears.
1. Introduction
Rotator cuff tears are among the most prevalent cause of shoulder pain and disability for which patients need therapy [1,2]. With an incidence of approximately 6% and 30% in patients under and over 60 years [3]. Issues of the rotator cuff include alteration of collagen fiber structure, tenocytes, cellularity, and vascularity [4]. Surgical treatment is indicated in patients with persistent pain unresponsive to conservative treatment [1]. In the last ten years, the arthroscopic rotator cuff repairs (ARCR) overtook the open surgery in term of procedures performed [5,6]. ARCR is associated with shorter hospitalization time and complications, but it could be associated with postoperative pain [7,8].
So, during the postoperative period, the patient’s pain should be checked to reduce recovery times and to improve patient satisfaction [8]. It has also been verified that particular attention to pain enhances postoperative rehabilitation, helps early mobilization, and has better measures of functional recovery, including the range of motion and muscle power [9]. This type of pain is difficult to manage, so it is necessary to refer to studies that have performed well in terms of quality and reliability.
Randomized controlled trials (RCTs) are often considered the gold standard for a clinical trial. In this context, RCTs are useful to improve the health of patients affected by RC tears. In addition, randomization equipoises known and unknown prognostic elements among treatment groups [10].
These studies need to be carefully pursued, precisely because of the factors described above. Moreover, improving the allocation of randomization and performing an intent-to-treat analysis is useful to minimize the bias effects [11].
In recent years, CONSORT (Consolidated Standards of Reporting Trials) was introduced with the aim to improve the quality of RCTs reports, and to alleviate the problems arising from the inadequate reporting of these trials [12].
This paper aimed to evaluate the quality of reporting of all RCTs linked to pain treatments of RC tears.
2. Materials and Methods
A systematic review of the literature was performed following the preferred reported items for systematic review and meta-analysis statement (PRISMA). During the month of September 2020, the databases Medline, Scopus, CINAHL, EMBASE, and CENTRAL were searched. In order to find the RCTs in the literature on this topic, the “randomized controlled trials” filter and the following word combinations were used: “rotator cuff tear AND pain”; “rotator cuff repair AND pain”; “rotator cuff surgery AND pain”; “rotator cuff tear AND analgesia”; “rotator cuff repair AND analgesia”; and “rotator cuff surgery AND analgesia”. Initially, all articles were screened for relevance by title and abstract and obtaining the full-text article if the abstract did not allow the investigators to assess the defined inclusion and exclusion criteria. To obtain other relevant articles for the study we performed a cross-reference search of the selected articles. Inclusion criteria were: level of evidence I or II according to the Oxford Center of EBM; English language; studies on human patients; and focus on pain in patients affected by RC tears. Exclusion criteria were: pilot studies; commentary reports; preliminary studies; review articles; meta-analysis; animal and cadaveric studies; and conference papers. The title, abstracts, and full-text articles were screened independently by two researchers (G.S and C.D.N) that separately performed a careful reading of all trials. Furthermore, the CONSORT checklist was utilized individually by each investigator to evaluate each report. The CONSORT checklist consists of 25 items and 37 checklist items that focus on describing how the trial was conceived, analyzed, and interpreted. Each question receives a yes/no response based on the completeness of the information supplied in the survey. The flow diagram simply depicts the progression of all trial participants and is one of the elements on the CONSORT checklist [12].
2.1. Data Extraction
All extracted data were recorded using Microsoft Word and Excel. The characteristics of the study, such as the first author, year of publication, sample size, location of the study, level of evidence of the study, mean follow-up, the presence of CONSORT flow diagram, type of rehabilitation, and journal of publication were recorded. Other information of the studies, including the financial support or the number of centers involved in the treatment of patients, were abstracted.
2.2. Methodological Quality Assessment
The methodological quality of the included studies in this review was assessed independently using the modified Coleman methodology score (MCMS). Through this score and its eleven criteria, a score from 0 to 100 was calculated for each study. A score of 100 indicates an optimal study that avoids chance, various biases, and confounding factors [13]. The MCMS was used for the statistical analysis in order to evaluate correlation with other variables.
2.3. Assessment of Agreement
The information from the selected texts were extracted independently by two writers (G.S. and C.D.N.) and double-checked by a third author (G.F.). The two reviewers separately assessed the methodological quality and reliability of the findings using the MCMS.
2.4. Statistical Analysis
Descriptive statistics were used to present the results. The Shapiro–Wilk test for normal distribution of the data was used to assess variable normal distribution. To assess statistically significant differences of MCMS between the studies either containing the CONSORT diagram or not, the independent t-test was used. To evaluate the MCMS and the number of checklist items of the articles over the different years (2000–2009, 2010–2014, ≥2015) ANOVA and independent t-test were used. To statistically calculate significant differences of MCMS between dissimilar blinded studies (blinded patients, blinded observers, double-blinded and no-blinded), ANOVA and independent t-test were used. The inter-rater reliability in grading the Coleman score, as well as the Pearson’s correlation between the number of checklist items and the Coleman score for each article, were assessed. The inter-rater reliability of grading the CONSORT checklist was assessed using % agreement amongst raters.
3. Results
3.1. Study Characteristics
Figure 1 depicts the selecting procedure. A total of 251 articles were found throughout the literature search. Finally, the study comprised 79 trials.
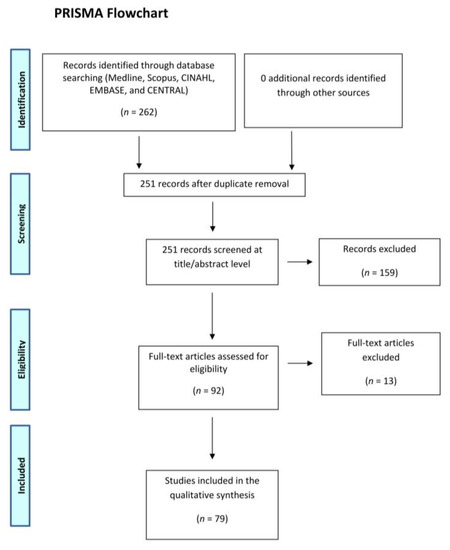
Figure 1.
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2009 flow diagram.
A total of 5403 patients were initially analyzed in the involved studies. By the final follow-up, 212 patients were lost. A total of 74 of the 79 studies were single-centered [1,2,5,6,7,8,9,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80] and only 1 report [81] was multi-centered. In the remaining 4 articles [82,83,84,85] it is unclear.
According to the Oxford Center of EBM, a total of 52 (66%) of 79 studies had a level of evidence I and 27 (34%) of 79 studies had a level of evidence II.
The analyzed studies were published in a total of 37 journals. Most of the included studies were published in the following four major journals: J Shoulder Elbow Surg (10 studies; 12.6%), Arthroscopy (9 studies; 11.3%), The American Journal of Sports Medicine (3 studies; 3.8% of the total), and J Anesthesia and Analgesia (5 studies; 6.3% of the total).
3.2. Topic
Despite the common general topic, 6 studies were focused on post-operative rehabilitation (3 on the immobilization with an abduction brace), 29 on the use of nerve block (in particular, 18 on the brachial plexus block, 9 on suprascapular nerve block, and 2 on supraclavicular block), 8 studies were focused on the intravenous patient-controlled analgesia, 4 on the intra-articular injection, and 11 on the subacromial injections. Finally, 7 studies were focused on the use and effect of specific drugs (gabapentin, zolpidem) and 1 study was focused on surgery. The remaining trials (13) were focused on other items linked to pain in patients undergoing rotator cuff surgery (miscellaneous).
3.3. Modified Coleman Methodology Score (MCMS)
The inter-rater reliability of the grading of Coleman score was 0.998. As for the quality indexes (the MCMS, the blinding of patients and observers, and the intent-to-treat) we considered in this review, there are considerations to be made. Of the 79 studies, only 11 included the intent-to-treat. Furthermore, 33 trials were double-blind, 23 were single-blind (11 blind patients and 12 blind observers), and the remaining 23 studies never performed the blinding of patients and observers.
The average MCMS in trials with blind patients was 65.09 (±7.39), the average MCMS in trials with blind observers was 67.67 (±7.33), the average MCMS in trials double-blinded was 69.06 (±7.50), and the average MCMS in trials without blinding was 63.17 (±6.84).
A statistically significant difference in MCMS between groups was found (p = 0.03). Multiple comparisons showed a statistically significant difference between trials double-blind and trials without blind (p = 0.02) (Table 1).

Table 1.
Mean MCMS between different blinded articles.
Figure 2 shows an increase in single blinded studies and a decrease in no-blinded and double-blinded studies after 2015.
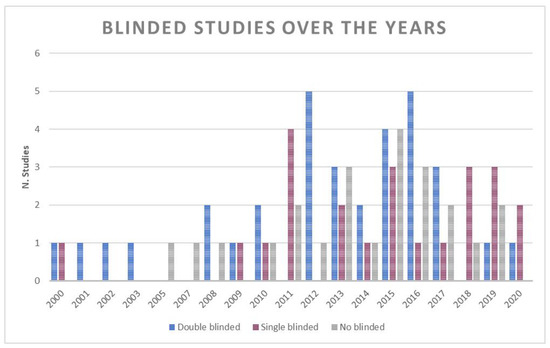
Figure 2.
Number of double blinded, single blinded and no blinded studies over the years.
Coleman score was greatest in articles featuring a CONSORT diagram. However, no statistically significant changes in MCMS were detected for trials that included or did not include a CONSORT diagram (p = 0.10) (Table 2).
Table 2.
Mean MCMS in articles with and without CONSORT flow-diagram.
3.4. Trends
The earliest identified RCT was published in 2000. In the last 10 years (since 2010) 67 RCTs were published and 12 were published between 2000 and 2013. From about 2011, the number of RCTs published has increased compared to previous years. Above all, in 2015 more articles were published (Figure 3).
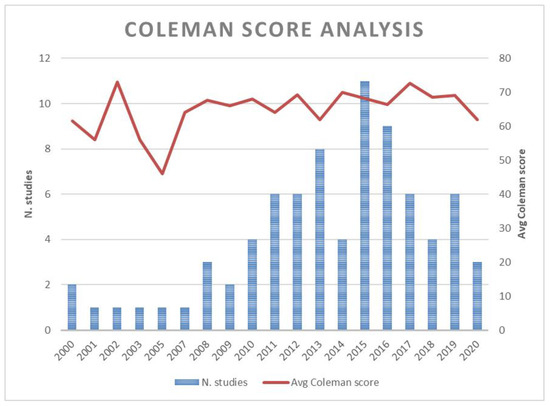
Figure 3.
Number of studies and Coleman score analysis by years.
The average MCMS across all analyzed RCTs was 66.58 (±7.57). The average MCMS during the last five years registered a score of 68.18 (±7.36), between 2010 and 2014 the average MCMS was 66 (±7.13) and between 2000 and 2009 the average MCMS was 62.75 (±8.28). A mildly significant difference in MCMS between time was found (p = 0.08). No statistically significant differences in MCMS between articles written from 2000 to 2009 and articles written from 2010 to 2014 (p = 0.21) and between articles written from 2010 to 2014 and articles written after 2015 (p = 0.25) were found. A statistically significant difference in MCMS between articles written before 2009 and articles written after 2015 was found (p = 0.03) (Table 3).
Table 3.
Mean MCMS between different years groups.
3.5. Other Methodological Factors on the CONSORT Checklist
The inter-rater reliability of the CONSORT checklist grading was 0.985. Table S1 shows the rate of missing CONSORT checklist items for each trial, computed as the ratio of the number of checklist items with missing information to total checklist items for each trial.
No correlation (Pearson correlation = 0.11, p = 0.349) between the number of checklist items for each article and the corresponding Coleman score was found.
The average number of checklist items for each article across all analyzed RCTs was 20.96 (±3.44). The 12 studies completed until the year 2009 averaged 18.25 (±3.96) number of checklist items, the studies completed between 2010 and 2014 averaged 21 (±2.95) number of checklist items, and the 39 studies done after 2015 averaged 21.77 (±3.22) number of checklist items.
There was a statistically significant difference in the number of checklist items detected over time (p = 0.007). There were statistically significant variations in the amount of checklist items between publications produced between 2000 and 2009, papers published between 2010 and 2014 (p = 0.018), and publications produced after 2015 (p = 0.002). There was no statistically significant variation in the number of checklist items between articles produced between 2010 and 2014 and those produced after 2015 (p = 0.353) (Table 4).
Table 4.
Mean number of checklist items between different years groups.
Another important quality index is the presence of a CONSORT flow diagram that outlines the inclusion and exclusion of patients for the trial as well as the follow-up rate. Of the 79 studies, 34 (43% of total studies analyzed) included a CONSORT flow diagram. Among the studies completed between 2000 and 2014, 11 included this kind of diagram and the remaining 23 studies were completed after 2015. All the analyzed studies completed until 2009, do not include the CONSORT flow diagram. A statistically significant difference in the number of checklist items between studies with and without the CONSORT flow diagram was found (p < 0.001) (Table 5).
Table 5.
Mean number of checklist items in articles with and without CONSORT flow-diagram.
4. Discussion
A total of 79 RCTs with a focus on analgesia techniques and pain management were identified in the present review. The present review reported a progressive increase of RCTs during the last six years. This data could reflect a progressive interest from the international audience on rotator cuff disease. Only RCTs were deliberately analyzed in this review to assess their quality through the analysis of several factors. The collection of RCTs present in the literature on this topic allowed better visualization of the scientific evidence on pain in patients affected by rotator cuff tears. The importance of high-quality studies in the literature is evident. RCTs could influence the trend of a specific surgical procedure. For example, in 2009, two RCTs published in the USA changed the trend of vertebroplasty worldwide [86]. Therefore, providing high-quality evidence on rotator cuff disease could help surgeons improve their skills and patient outcomes.
Many authors adopted non-surgical strategies to reduce rotator cuff tears pain. In specific nerve block and subacromial injections were the most commonly adopted and effective techniques.
RCT is one of the common disorders of the musculoskeletal system in the ageing population [75,87,88]. In fact, this type of problem is linked to the worsening of the tendons, in many cases due to microtrauma or traumatic injuries [75,89,90]. Rotator cuff tear leads to medium-severe disability and, although there are other possible causes, RCT is commonly the cause of shoulder pain [39,91]. Several factors can contribute to an increased level of pain including female gender, early work resumption post-surgery, pre-existent capsulitis or bursitis, and additional performed subacromial decompression [5]. In the current scientific literature, the appropriate treatment for rotator cuff diseases is still a source of debate. However, in the case of patients with chronic and symptomatic rotator cuff tears the best treatment to reduce pain is surgical repair and there is increasing use of arthroscopic shoulder surgery [39]. Despite these improvements, rotator cuff surgery is related to a high incidence of postoperative pain [39,43]. Therefore, close control of postoperative pain is required to reduce the duration of hospitalization, to increase patient satisfaction, and clinical outcome [39,43]. Various treatment techniques have been developed in this regard and one of the most effective of these is regional nerve blocks [43]. Several studies have analyzed these techniques. The interscalene brachial plexus blocks (ISBs) lead to a reduction in postoperative pain even if for a short time. Suprascapular nerve blocks (SSNBs) are currently the most used method in this situation. While, a new kind of block has recently been introduced, often used in association with SSNB: it is axillary nerve block (ANB) [43].
Considering the Coleman score, there was an improvement in the quality of the studies completed in the last five years (average MCMS of 68.18) compared to the other studies published between 2000 and 2014. A statistically significant difference in MCMS between articles written before 2009 and articles written after 2015 was found. Unfortunately, the MCMS allows evaluation of only the quality of reporting, consequently, low scores are given to high-quality studies that are poorly written.
The CONSORT statement is an evidence-based minimum set of recommendations including a checklist and flow diagram for reporting RCTs to evaluate the quality of the studies [92]. In 2008, the CONSORT group developed an extension to the original statement that addressed methodological issues specific to trials of non-pharmacologic treatments (NPTs) [93]. The factors outlined in this extension included descriptions of how such trials should outline the calculation of sample sizes, the randomization procedure used, report the blinding status, and outline the flow of participants [93].
4.1. Limitations
The main limitation associated with the use of the modified Coleman methodology score (MCMS) as a quality measure of RCTs is that it assesses the quality of trial reporting rather than the quality of the trials themselves. In reality, stronger methodological protections may have been applied in certain studies that were not disclosed in the analysis. Furthermore, certain MCMS components might only be addressed in surgical studies (e.g., appropriate description of surgical technique and description of postoperative protocol). As a result, non-surgical investigations could never achieve the maximum score of 100.
Therefore, the RCTs that involved surgery and that did not were assessed separately. Conservative studies increased after 2015, while surgical ones decreased. In fact, the conservative/surgical ratio is increasing since 2015 (Figure 4). Considering the years after 2015, the higher number of RCTs involving surgery could change the trend of MCMS.
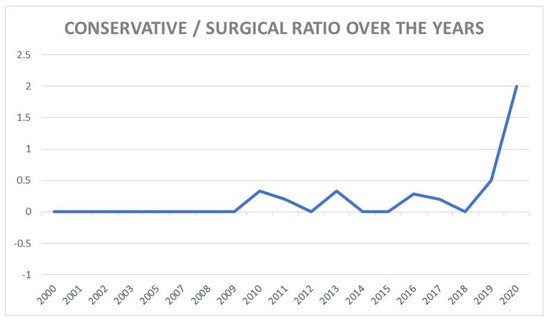
Figure 4.
Ratio of conservative and surgical studies divided by years.
This investigation only included English-language trials. Moreover, since too many variables between the studies included were present (type of treatment, sample size, follow up, baseline patient’s characteristics, initial tear size, etc.), it was not possible to perform a meta-analysis. We decided to only perform a systematic review, therefore it was not possible to test the heterogeneity between studies.
RCTs focusing on shoulder discomfort with intact rotator cuff tendons were also excluded.
4.2. Future Directions
Future studies might examine the impact that the pain in RCTs has had on clinical practices in RC surgery over time. Moreover, it would be important to assess the quality of reporting in other orthopedic areas to find the areas that require progress.
5. Conclusions
There has been a significant increase in the last years in both quantity and quality of RCT studies evaluating pain in RC tears. The number of RCT studying RC tears increased by 2010, with a peak in 2015. Concerning the quality of reporting of these RCTs has resulted in an improvement of the MCMS score registering a positive trend across the analyzed set. Papers written from 2015 had a higher average MCMS with respect to papers written between 2000 and 2009. Studies written from 2010 had a higher average number of checklist items with respect to studies written between 2000 and 2009. No correlation between the number of checklist items for each article and the respective Coleman score was found. The double-blinded articles showed higher Coleman scores with respect to the no blinded studies.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/jcm10184072/s1, Table S1: The rate of missed checklist items of CONSORT checklist for each trial.
Author Contributions
Conceptualization, U.G.L. and S.D.S.; methodology, M.G.D.M.; software, I.P.; validation, U.G.L., A.B. and V.D.; formal analysis, I.P.; investigation, G.S. (Gaia Sciotti); resources, G.S. (Giulia Santamaria); data curation, I.P.; writing—original draft preparation, I.P.; writing—review and editing, S.D.S.; visualization, M.G.D.M.; supervision, U.G.L.; project administration, V.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Khashan, M.; Dolkart, O.; Amar, E.; Chechik, O.; Sharfman, Z.; Mozes, G.; Maman, E.; Weinbroum, A. Effect of preemptive intra-articular morphine and ketamine on pain after arthroscopic rotator cuff repair: A prospective, double-blind, randomized controlled study. Arch. Orthop. Trauma Surg. 2016, 136, 233–239. [Google Scholar] [CrossRef]
- Seven, M.M.; Ersen, O.; Akpancar, S.; Ozkan, H.; Turkkan, S.; Yıldız, Y.; Koca, K. Effectiveness of prolotherapy in the treatment of chronic rotator cuff lesions. Orthop. Traumatol. Surg. Res. 2017, 103, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Berton, A.; Papapietro, N.; Maffulli, N.; Denaro, V. Epidemiology, genetics and biological factors of rotator cuff tears. Med. Sport Sci. 2012, 57, 1–9. [Google Scholar] [CrossRef]
- Longo, U.G.; Berton, A.; Khan, W.S.; Maffulli, N.; Denaro, V. Histopathology of rotator cuff tears. Sports Med. Arthrosc. Rev. 2011, 19, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Hollman, F.; Wolterbeek, N.; Zijl, J.A.C.; van Egeraat, S.P.M.; Wessel, R.N. Abduction Brace Versus Antirotation Sling After Arthroscopic Cuff Repair: The Effects on Pain and Function. Arthroscopy 2017, 33, 1618–1626. [Google Scholar] [CrossRef] [PubMed]
- Ikemoto, R.Y.; Murachovsky, J.; Prata Nascimento, L.G.; Bueno, R.S.; Oliveira Almeida, L.H.; Strose, E.; de Mello, S.C.; Saletti, D. Prospective Randomized Study Comparing Two Anesthetic Methods For Shoulder Surgery. Rev. Bras. Ortop. 2010, 45, 395–399. [Google Scholar] [CrossRef]
- Park, J.Y.; Bang, J.Y.; Oh, K.S. Blind suprascapular and axillary nerve block for post-operative pain in arthroscopic rotator cuff surgery. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3877–3883. [Google Scholar] [CrossRef]
- Kim, J.H.; Koh, H.J.; Kim, D.K.; Lee, H.J.; Kwon, K.H.; Lee, K.Y.; Kim, Y.S. Interscalene brachial plexus bolus block versus patient-controlled interscalene indwelling catheter analgesia for the first 48 hours after arthroscopic rotator cuff repair. J. Shoulder Elbow. Surg. 2018, 27, 1243–1250. [Google Scholar] [CrossRef]
- Shin, S.W.; Byeon, G.J.; Yoon, J.U.; Ok, Y.M.; Baek, S.H.; Kim, K.H.; Lee, S.J. Effective analgesia with ultrasound-guided interscalene brachial plexus block for postoperative pain control after arthroscopic rotator cuff repair. J. Anesth. 2014, 28, 64–69. [Google Scholar] [CrossRef]
- MacDonald, P.; McRae, S.; Leiter, J.; Mascarenhas, R.; Lapner, P. Arthroscopic rotator cuff repair with and without acromioplasty in the treatment of full-thickness rotator cuff tears: A multicenter, randomized controlled trial. J. Bone Joint Surg. Am. 2011, 93, 1953–1960. [Google Scholar] [CrossRef]
- Shin, S.J.; Oh, J.H.; Chung, S.W.; Song, M.H. The efficacy of acromioplasty in the arthroscopic repair of small- to medium-sized rotator cuff tears without acromial spur: Prospective comparative study. Arthroscopy 2012, 28, 628–635. [Google Scholar] [CrossRef]
- Cai, Y.Z.; Zhang, C.; Jin, R.L.; Shen, T.; Gu, P.C.; Lin, X.J.; Chen, J.D. Arthroscopic Rotator Cuff Repair With Graft Augmentation of 3-Dimensional Biological Collagen for Moderate to Large Tears: A Randomized Controlled Study. Am. J. Sports Med. 2018, 46, 1424–1431. [Google Scholar] [CrossRef] [PubMed]
- Watsend, A.M.; Osestad, T.M.; Jakobsen, R.B.; Jacobsen, R.B.; Engebretsen, L. Clinical studies on posterior cruciate ligament tears have weak design. Knee Surg. Sports Traumatol. Arthrosc. 2009, 17, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.S.; Pulido, P.; Adelson, W.S.; Fronek, J.; Hoenecke, H.R. The efficacy of continuous bupivacaine infiltration following arthroscopic rotator cuff repair. Arthroscopy 2008, 24, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Bang, S.R.; Yu, S.K.; Kim, T.H. Can gabapentin help reduce postoperative pain in arthroscopic rotator cuff repair? A prospective, randomized, double-blind study. Arthroscopy 2010, 26, S106–S111. [Google Scholar] [CrossRef]
- Behr, A.; Freo, U.; Ori, C.; Westermann, B.; Alemanno, F. Buprenorphine added to levobupivacaine enhances postoperative analgesia of middle interscalene brachial plexus block. J. Anesth. 2012, 26, 746–751. [Google Scholar] [CrossRef] [PubMed]
- Borgeat, A.; Aguirre, J.; Marquardt, M.; Mrdjen, J.; Blumenthal, S. Continuous interscalene analgesia with ropivacaine 0.2% versus ropivacaine 0.3% after open rotator cuff repair: The effects on postoperative analgesia and motor function. Anesth. Analg. 2010, 111, 1543–1547. [Google Scholar] [CrossRef]
- Cabaton, J.; Nové-Josserand, L.; Mercadal, L.; Vaudelin, T. Analgesic efficacy of ultrasound-guided interscalene block vs. supraclavicular block for ambulatory arthroscopic rotator cuff repair: A randomised noninferiority study. Eur. J. Anaesthesiol. 2019, 36, 778–786. [Google Scholar] [CrossRef]
- Cho, C.H.; Song, K.S.; Min, B.W.; Lee, K.J.; Ha, E.; Lee, Y.C.; Lee, Y.K. Multimodal approach to postoperative pain control in patients undergoing rotator cuff repair. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 1744–1748. [Google Scholar] [CrossRef]
- Cho, C.H.; Lee, S.W.; Lee, Y.K.; Shin, H.K.; Hwang, I. Effect of a sleep aid in analgesia after arthroscopic rotator cuff repair. Yonsei Med. J. 2015, 56, 772–777. [Google Scholar] [CrossRef]
- Choi, S.; Kim, T.; Kwon, Y.S.; Kang, H. Intra-operative effect of interscalene brachial plexus block to arthroscopic rotator cuff repair surgery. Int. Orthop. 2019, 43, 2117–2124. [Google Scholar] [CrossRef]
- Choi, E.M.; Kim, E.M.; Chung, M.H.; Park, J.H.; Lee, H.K.; Choi, Y.R.; Lee, M. Effects of ultrasound-guided stellate ganglion block on acute pain after arthroscopic shoulder surgery. Pain Phys. 2015, 18, E379–E388. [Google Scholar]
- Ciccone, W.J.; Busey, T.D.; Weinstein, D.M.; Walden, D.L.; Elias, J.J. Assessment of pain relief provided by interscalene regional block and infusion pump after arthroscopic shoulder surgery. Arthroscopy 2008, 24, 14–19. [Google Scholar] [CrossRef]
- Coghlan, J.A.; Forbes, A.; McKenzie, D.; Bell, S.N.; Buchbinder, R. Efficacy of subacromial ropivacaine infusion for rotator cuff surgery. A randomized trial. J. Bone Jt. Surg. Am. 2009, 91, 1558–1567. [Google Scholar] [CrossRef]
- Conti, M.; Garofalo, R.; Castagna, A. Does a brace influence clinical outcomes after arthroscopic rotator cuff repair? Musculoskelet. Surg. 2015, 99 (Suppl. 1), S31–S35. [Google Scholar] [CrossRef]
- Coory, J.A.; Parr, A.F.; Wilkinson, M.P.; Gupta, A. Efficacy of suprascapular nerve block compared with subacromial injection: A randomized controlled trial in patients with rotator cuff tears. J. Shoulder Elbow Surg. 2019, 28, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Culebras, X.; Van Gessel, E.; Hoffmeyer, P.; Gamulin, Z. Clonidine combined with a long acting local anesthetic does not prolong postoperative analgesia after brachial plexus block but does induce hemodynamic changes. Anesth. Analg. 2001, 92, 199–204. [Google Scholar] [CrossRef]
- Delaunay, L.; Souron, V.; Lafosse, L.; Marret, E.; Toussaint, B. Analgesia after arthroscopic rotator cuff repair: Subacromial versus interscalene continuous infusion of ropivacaine. Reg. Anesth. Pain Med. 2005, 30, 117–122. [Google Scholar] [CrossRef]
- Desmet, M.; Vanneste, B.; Reynvoet, M.; Van Cauwelaert, J.; Verhelst, L.; Pottel, H.; Missant, C.; Van de Velde, M. A randomised controlled trial of intravenous dexamethasone combined with interscalene brachial plexus blockade for shoulder surgery. Anaesthesia 2015, 70, 1180–1185. [Google Scholar] [CrossRef] [PubMed]
- Desroches, A.; Klouche, S.; Schlur, C.; Bauer, T.; Waitzenegger, T.; Hardy, P. Suprascapular Nerve Block Versus Interscalene Block as Analgesia After Arthroscopic Rotator Cuff Repair: A Randomized Controlled Noninferiority Trial. Arthroscopy 2016, 32, 2203–2209. [Google Scholar] [CrossRef] [PubMed]
- Düzgün, I.; Baltacı, G.; Atay, O.A. Comparison of slow and accelerated rehabilitation protocol after arthroscopic rotator cuff repair: Pain and functional activity. Acta Orthop. Traumatol. Turc. 2011, 45, 23–33. [Google Scholar] [CrossRef]
- Faria-Silva, R.; de Rezende, D.C.; Ribeiro, J.M.; Gomes, T.H.; Oliveira, B.A.; Pereira, F.M.; de Almeida Filho, I.A.; de Carvalho Junior, A.E. Association of clonidine and ropivacaine in brachial plexus block for shoulder arthroscopy. Braz. J. Anesthesiol. 2016, 66, 335–340. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Forsythe, B.; Agarwalla, A.; Puzzitiello, R.N.; Patel, B.H.; Lu, Y.; Verma, N.N.; Romeo, A.A.; Cole, B.J. Clinical Function Improves After Subacromial Injection of Local Anesthetic in Full-Thickness Rotator Cuff Tears: A Randomized Control Trial. Orthop. J. Sports Med. 2020, 8, 2325967119892331. [Google Scholar] [CrossRef] [PubMed]
- Fredrickson, M.J.; Abeysekera, A.; Price, D.J.; Wong, A.C. Patient-initiated mandatory boluses for ambulatory continuous interscalene analgesia: An effective strategy for optimizing analgesia and minimizing side-effects. Br. J. Anaesth. 2011, 106, 239–245. [Google Scholar] [CrossRef]
- Ghandour, T.M.; Ibrahim, A.; Abdelrahman, A.A.; Elgammal, A.; Hammad, M.H. Does The Type of Shoulder Brace Affect Postoperative Pain and Clinical Outcome After Arthroscopic Rotator Cuff Repair? Arthroscopy 2019, 35, 1016–1023. [Google Scholar] [CrossRef] [PubMed]
- Gialanella, B.; Prometti, P. Effects of corticosteroids injection in rotator cuff tears. Pain Med. 2011, 12, 1559–1565. [Google Scholar] [CrossRef] [PubMed]
- Gialanella, B.; Bertolinelli, M. Corticosteroids injection in rotator cuff tears in elderly patient: Pain outcome prediction. Geriatr Gerontol. Int. 2013, 13, 993–1001. [Google Scholar] [CrossRef]
- Gumina, S.; Passaretti, D.; Gurzì, M.D.; Candela, V. Arginine L-alpha-ketoglutarate, methylsulfonylmethane, hydrolyzed type I collagen and bromelain in rotator cuff tear repair: A prospective randomized study. Curr. Med. Res. Opin. 2012, 28, 1767–1774. [Google Scholar] [CrossRef]
- Gurger, M.; Ozer, A.B. A comparison of continuous interscalene block versus general anesthesia alone on the functional outcomes of the patients undergoing arthroscopic rotator cuff repair. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 1659–1666. [Google Scholar] [CrossRef] [PubMed]
- Han, S.S.; Lee, Y.H.; Oh, J.H.; Aminzai, S.; Kim, S.H. Randomized, controlled trial of multimodal shoulder injection or intravenous patient-controlled analgesia after arthroscopic rotator cuff repair. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 2877–2883. [Google Scholar] [CrossRef]
- Hartrick, C.T.; Tang, Y.S.; Siwek, D.; Murray, R.; Hunstad, D.; Smith, G. The effect of initial local anesthetic dose with continuous interscalene analgesia on postoperative pain and diaphragmatic function in patients undergoing arthroscopic shoulder surgery: A double-blind, randomized controlled trial. BMC Anesthesiol. 2012, 12, 6. [Google Scholar] [CrossRef] [PubMed]
- Hofmann-Kiefer, K.; Eiser, T.; Chappell, D.; Leuschner, S.; Conzen, P.; Schwender, D. Does patient-controlled continuous interscalene block improve early functional rehabilitation after open shoulder surgery? Anesth. Analg. 2008, 106, 991–996, table of contents. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.T.; Jang, J.S.; Lee, J.J.; Song, D.K.; Lee, H.N.; Kim, D.Y.; Lee, S.S.; Hwang, S.M.; Kim, Y.B.; Lee, S. Dexmedetomidine combined with interscalene brachial plexus block has a synergistic effect on relieving postoperative pain after arthroscopic rotator cuff repair. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 2343–2353. [Google Scholar] [CrossRef] [PubMed]
- Jo, C.H.; Shin, J.S.; Huh, J. Multimodal analgesia for arthroscopic rotator cuff repair: A randomized, placebo-controlled, double-blind trial. Eur. J. Orthop. Surg. Traumatol. 2014, 24, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Kasten, P.; Keil, C.; Grieser, T.; Raiss, P.; Streich, N.; Loew, M. Prospective randomised comparison of arthroscopic versus mini-open rotator cuff repair of the supraspinatus tendon. Int. Orthop. 2011, 35, 1663–1670. [Google Scholar] [CrossRef]
- Kim, J.Y.; Song, K.S.; Kim, W.J.; Park, Y.H.; Kang, H.; Woo, Y.C.; Shin, H.Y. Analgesic efficacy of two interscalene blocks and one cervical epidural block in arthroscopic rotator cuff repair. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 931–939. [Google Scholar] [CrossRef]
- Klein, S.M.; Grant, S.A.; Greengrass, R.A.; Nielsen, K.C.; Speer, K.P.; White, W.; Warner, D.S.; Steele, S.M. Interscalene brachial plexus block with a continuous catheter insertion system and a disposable infusion pump. Anesth. Analg. 2000, 91, 1473–1478. [Google Scholar] [CrossRef]
- Ko, S.H.; Cho, S.D.; Lee, C.C.; Choi, J.K.; Kim, H.W.; Park, S.J.; Bae, M.H.; Cha, J.R. Comparison of Arthroscopically Guided Suprascapular Nerve Block and Blinded Axillary Nerve Block vs. Blinded Suprascapular Nerve Block in Arthroscopic Rotator Cuff Repair: A Randomized Controlled Trial. Clin. Orthop. Surg. 2017, 9, 340–347. [Google Scholar] [CrossRef]
- Koh, W.U.; Kim, H.J.; Park, H.S.; Choi, W.J.; Yang, H.S.; Ro, Y.J. A randomised controlled trial comparing continuous supraclavicular and interscalene brachial plexus blockade for open rotator cuff surgery. Anaesthesia 2016, 71, 692–699. [Google Scholar] [CrossRef]
- Kraeutler, M.J.; Reynolds, K.A.; Long, C.; McCarty, E.C. Compressive cryotherapy versus ice-a prospective, randomized study on postoperative pain in patients undergoing arthroscopic rotator cuff repair or subacromial decompression. J. Shoulder Elbow Surg. 2015, 24, 854–859. [Google Scholar] [CrossRef]
- Lee, H.J.; Kim, Y.S.; Park, I.; Ha, D.H.; Lee, J.H. Administration of analgesics after rotator cuff repair: A prospective clinical trial comparing glenohumeral, subacromial, and a combination of glenohumeral and subacromial injections. J. Shoulder Elbow Surg. 2015, 24, 663–668. [Google Scholar] [CrossRef]
- Lee, J.J.; Kim, D.Y.; Hwang, J.T.; Lee, S.S.; Hwang, S.M.; Kim, G.H.; Jo, Y.G. Effect of ultrasonographically guided axillary nerve block combined with suprascapular nerve block in arthroscopic rotator cuff repair: A randomized controlled trial. Arthroscopy 2014, 30, 906–914. [Google Scholar] [CrossRef]
- Lee, J.J.; Yoo, Y.S.; Hwang, J.T.; Kim, D.Y.; Jeon, S.J.; Hwang, S.M.; Jang, J.S. Efficacy of direct arthroscopy-guided suprascapular nerve block after arthroscopic rotator cuff repair: A prospective randomized study. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 562–566. [Google Scholar] [CrossRef]
- Lee, J.J.; Hwang, J.T.; Kim, D.Y.; Lee, S.S.; Hwang, S.M.; Lee, N.R.; Kwak, B.C. Effects of arthroscopy-guided suprascapular nerve block combined with ultrasound-guided interscalene brachial plexus block for arthroscopic rotator cuff repair: A randomized controlled trial. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 2121–2128. [Google Scholar] [CrossRef]
- Liu, X.N.; Noh, Y.M.; Yang, C.J.; Kim, J.U.; Chung, M.H.; Noh, K.C. Effects of a Single-Dose Interscalene Block on Pain and Stress Biomarkers in Patients Undergoing Arthroscopic Rotator Cuff Repair: A Randomized Controlled Trial. Arthroscopy 2017, 33, 918–926. [Google Scholar] [CrossRef]
- Mahure, S.A.; Rokito, A.S.; Kwon, Y.W. Transcutaneous electrical nerve stimulation for postoperative pain relief after arthroscopic rotator cuff repair: A prospective double-blinded randomized trial. J. Shoulder Elbow Surg. 2017, 26, 1508–1513. [Google Scholar] [CrossRef] [PubMed]
- Malik, T.; Mass, D.; Cohn, S. Postoperative Analgesia in a Prolonged Continuous Interscalene Block Versus Single-Shot Block in Outpatient Arthroscopic Rotator Cuff Repair: A Prospective Randomized Study. Arthroscopy 2016, 32, 1544–1550.e1541. [Google Scholar] [CrossRef]
- Merivirta, R.; Kuusniemi, K.S.; Aantaa, R.; Hurme, S.A.; Aärimaa, V.; Leino, K.A. The analgesic effect of continuous subacromial bupivacaine infusion after arthroscopic shoulder surgery: A randomized controlled trial. Acta Anaesthesiol. Scand. 2012, 56, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Merivirta, R.; Äärimaa, V.; Aantaa, R.; Koivisto, M.; Leino, K.; Liukas, A.; Kuusniemi, K. Postoperative fentanyl patch versus subacromial bupivacaine infusion in arthroscopic shoulder surgery. Arthroscopy 2013, 29, 1129–1134. [Google Scholar] [CrossRef]
- Merolla, G.; Dellabiancia, F.; Ingardia, A.; Paladini, P.; Porcellini, G. Co-analgesic therapy for arthroscopic supraspinatus tendon repair pain using a dietary supplement containing Boswellia serrata and Curcuma longa: A prospective randomized placebo-controlled study. Musculoskelet. Surg. 2015, 99 (Suppl. 1), S43–S52. [Google Scholar] [CrossRef] [PubMed]
- Oh, C.H.; Oh, J.H.; Kim, S.H.; Cho, J.H.; Yoon, J.P.; Kim, J.Y. Effectiveness of subacromial anti-adhesive agent injection after arthroscopic rotator cuff repair: Prospective randomized comparison study. Clin. Orthop. Surg. 2011, 3, 55–61. [Google Scholar] [CrossRef]
- Osti, L.; Buono, A.D.; Maffulli, N. Pulsed electromagnetic fields after rotator cuff repair: A randomized, controlled study. Orthopedics 2015, 38, e223–e228. [Google Scholar] [CrossRef]
- Perdreau, A.; Joudet, T. Efficacy of multimodal analgesia injection combined with corticosteroids after arthroscopic rotator cuff repair. Orthop. Traumatol. Surg. Res. 2015, 101, S337–S345. [Google Scholar] [CrossRef] [PubMed]
- Reynard, F.; Vuistiner, P.; Léger, B.; Konzelmann, M. Immediate and short-term effects of kinesiotaping on muscular activity, mobility, strength and pain after rotator cuff surgery: A crossover clinical trial. BMC Musculoskelet. Disord. 2018, 19, 305. [Google Scholar] [CrossRef] [PubMed]
- Rha, D.W.; Park, G.Y.; Kim, Y.K.; Kim, M.T.; Lee, S.C. Comparison of the therapeutic effects of ultrasound-guided platelet-rich plasma injection and dry needling in rotator cuff disease: A randomized controlled trial. Clin. Rehabil. 2013, 27, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Salviz, E.A.; Xu, D.; Frulla, A.; Kwofie, K.; Shastri, U.; Chen, J.; Shariat, A.N.; Littwin, S.; Lin, E.; Choi, J.; et al. Continuous interscalene block in patients having outpatient rotator cuff repair surgery: A prospective randomized trial. Anesth. Analg. 2013, 117, 1485–1492. [Google Scholar] [CrossRef]
- Schwartzberg, R.S.; Reuss, B.L.; Rust, R. Efficacy of continuous subacromial bupivacaine infusion for pain control after arthroscopic rotator cuff repair. J. Shoulder Elbow Surg. 2013, 22, 1320–1324. [Google Scholar] [CrossRef]
- Schwitzguebel, A.J.; Kolo, F.C.; Tirefort, J.; Kourhani, A.; Nowak, A.; Gremeaux, V.; Saffarini, M.; Lädermann, A. Efficacy of Platelet-Rich Plasma for the Treatment of Interstitial Supraspinatus Tears: A Double-Blinded, Randomized Controlled Trial. Am. J. Sports Med. 2019, 47, 1885–1892. [Google Scholar] [CrossRef]
- Sethi, P.M.; Brameier, D.T.; Mandava, N.K.; Miller, S.R. Liposomal bupivacaine reduces opiate consumption after rotator cuff repair in a randomized controlled trial. J. Shoulder Elbow Surg. 2019, 28, 819–827. [Google Scholar] [CrossRef]
- Shams, A.; El-Sayed, M.; Gamal, O.; Ewes, W. Subacromial injection of autologous platelet-rich plasma versus corticosteroid for the treatment of symptomatic partial rotator cuff tears. Eur. J. Orthop. Surg. Traumatol. 2016, 26, 837–842. [Google Scholar] [CrossRef]
- Syed, U.A.M.; Aleem, A.W.; Wowkanech, C.; Weekes, D.; Freedman, M.; Tjoumakaris, F.; Abboud, J.A.; Austin, L.S. Neer Award 2018: The effect of preoperative education on opioid consumption in patients undergoing arthroscopic rotator cuff repair: A prospective, randomized clinical trial. J. Shoulder Elbow Surg. 2018, 27, 962–967. [Google Scholar] [CrossRef] [PubMed]
- Takada, M.; Fukusaki, M.; Terao, Y.; Yamashita, K.; Ando, Y.; Sumikawa, K. Postoperative analgesic effect of preoperative intravenous flurbiprofen in arthroscopic rotator cuff repair. J. Anesth. 2009, 23, 500–503. [Google Scholar] [CrossRef] [PubMed]
- Tetzlaff, J.E.; Brems, J.; Dilger, J. Intraarticular morphine and bupivacaine reduces postoperative pain after rotator cuff repair. Reg. Anesth. Pain Med. 2000, 25, 611–614. [Google Scholar] [CrossRef] [PubMed]
- Thackeray, E.M.; Swenson, J.D.; Gertsch, M.C.; Phillips, K.M.; Steele, J.W.; Burks, R.T.; Tashjian, R.Z.; Greis, P.E. Diaphragm function after interscalene brachial plexus block: A double-blind, randomized comparison of 0.25% and 0.125% bupivacaine. J. Shoulder Elbow Surg. 2013, 22, 381–386. [Google Scholar] [CrossRef]
- Türkmen, E.; Analay Akbaba, Y.; Altun, S. Effectiveness of video-based rehabilitation program on pain, functionality, and quality of life in the treatment of rotator cuff tears: A randomized controlled trial. J. Hand Ther. 2020, 33, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Tokumine, J.; Yorozu, T.; Moriyama, K.; Sakamoto, H.; Inoue, T. Particulate-steroid betamethasone added to ropivacaine in interscalene brachial plexus block for arthroscopic rotator cuff repair improves postoperative analgesia. BMC Anesthesiol. 2016, 16, 84. [Google Scholar] [CrossRef]
- Wong, A.K.; Keeney, L.G.; Chen, L.; Williams, R.; Liu, J.; Elkassabany, N.M. Effect of Local Anesthetic Concentration (0.2% vs. 0.1% Ropivacaine) on Pulmonary Function, and Analgesia After Ultrasound-Guided Interscalene Brachial Plexus Block: A Randomized Controlled Study. Pain Med. 2016, 17, 2397–2403. [Google Scholar] [CrossRef]
- Yamakado, K. Efficacy of arthroscopically placed pain catheter adjacent to the suprascapular nerve (continuous arthroscopically assisted suprascapular nerve block) following arthroscopic rotator-cuff repair. Open Access J. Sports Med. 2014, 5, 129–136. [Google Scholar] [CrossRef]
- Yamamoto, S.; Yamaguchi, H.; Sakaguchi, M.; Yamashita, S.; Satsumae, T. Preoperative droperidol improved postoperative pain relief in patients undergoing rotator-cuff repair during general anesthesia using intravenous morphine. J. Clin. Anesth. 2003, 15, 525–529. [Google Scholar] [CrossRef]
- Yun, M.J.; Oh, J.H.; Yoon, J.P.; Park, S.H.; Hwang, J.W.; Kil, H.Y. Subacromial patient-controlled analgesia with ropivacaine provides effective pain control after arthroscopic rotator cuff repair. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 1971–1977. [Google Scholar] [CrossRef]
- Chou, W.Y.; Ko, J.Y.; Wang, F.S.; Huang, C.C.; Wong, T.; Wang, C.J.; Chang, H.E. Effect of sodium hyaluronate treatment on rotator cuff lesions without complete tears: A randomized, double-blind, placebo-controlled study. J. Shoulder Elbow Surg. 2010, 19, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Alemanno, F.; Ghisi, D.; Fanelli, A.; Faliva, A.; Pergolotti, B.; Bizzarri, F.; Fanelli, G. Tramadol and 0.5% levobupivacaine for single-shot interscalene block: Effects on postoperative analgesia in patients undergoing shoulder arthroplasty. Minerva Anestesiol. 2012, 78, 291–296. [Google Scholar] [PubMed]
- Barber, F.A.; Herbert, M.A. The effectiveness of an anesthetic continuous-infusion device on postoperative pain control. Arthroscopy 2002, 18, 76–81. [Google Scholar] [CrossRef]
- Cho, N.S.; Ha, J.H.; Rhee, Y.G. Patient-controlled analgesia after arthroscopic rotator cuff repair: Subacromial catheter versus intravenous injection. Am. J. Sports Med. 2007, 35, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Arias-Buría, J.L.; Valero-Alcaide, R.; Cleland, J.A.; Salom-Moreno, J.; Ortega-Santiago, R.; Atín-Arratibel, M.A.; Fernández-de-las-Peñas, C. Inclusion of trigger point dry needling in a multimodal physical therapy program for postoperative shoulder pain: A randomized clinical trial. J. Manip. Physiol. Ther. 2015, 38, 179–187. [Google Scholar] [CrossRef]
- Denaro, L.; Longo, U.G.; Papalia, R.; De Salvatore, S.; Ruzzini, L.; Piergentili, I.; Denaro, V. The burden of percutaneous vertebroplasty: An epidemiological nationwide study in Italy from 2009 to 2015. Eur. Spine J. 2021, 1–8. [Google Scholar] [CrossRef]
- Alessandra, B. Delayed Rehabilitation Protocol after Rotator Cuff Repair. Osteology 2021, 1, 29–38. [Google Scholar] [CrossRef]
- Longo, U.G.; Candela, V.; De Salvatore, S.; Piergentili, I.; Panattoni, N.; Casciani, E.; Faldetta, A.; Marchetti, A.; De Marinis, M.G.; Denaro, V. Arthroscopic Rotator Cuff Repair Improves Sleep Disturbance and Quality of Life: A Prospective Study. Int. J. Environ. Res. Public Health 2021, 18, 3739. [Google Scholar] [CrossRef]
- Panattoni, N.; Longo, U.G.; De Salvatore, S.; Castaneda, N.S.C.; Risi Ambrogioni, L.; Piredda, M.; De Marinis, M.G.; Denaro, V. The influence of psychosocial factors on patient-reported outcome measures in rotator cuff tears pre- and post-surgery: A systematic review. Qual. Life Res. 2021, 1–26. [Google Scholar] [CrossRef]
- Longo, U.G.; Forriol, F.; Candela, V.; Tecce, S.M.; De Salvatore, S.; Altonaga, J.R.; Wallace, A.L.; Denaro, V. Arthroscopic Tenotomy of the Long Head of the Biceps Tendon and Section of the Anterior Joint Capsule Produce Moderate Osteoarthritic Changes in an Experimental Sheep Model. Int. J. Environ. Res. Public Health 2021, 18, 7471. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Berton, A.; De Salvatore, S.; Piergentili, I.; Casciani, E.; Faldetta, A.; De Marinis, M.G.; Denaro, V. Minimal Clinically Important Difference and Patient Acceptable Symptom State for the Pittsburgh Sleep Quality Index in Patients Who Underwent Rotator Cuff Tear Repair. Int. J. Environ. Res. Public Health 2021, 18, 8666. [Google Scholar] [CrossRef] [PubMed]
- Turner, L.; Shamseer, L.; Altman, D.G.; Schulz, K.F.; Moher, D. Does use of the CONSORT Statement impact the completeness of reporting of randomised controlled trials published in medical journals? A Cochrane review. Syst. Rev. 2012, 1, 60. [Google Scholar] [CrossRef] [PubMed]
- Boutron, I.; Altman, D.G.; Moher, D.; Schulz, K.F.; Ravaud, P.; Group, C.N. CONSORT Statement for Randomized Trials of Nonpharmacologic Treatments: A 2017 Update and a CONSORT Extension for Nonpharmacologic Trial Abstracts. Ann. Intern. Med. 2017, 167, 40–47. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).