
Does Posterior Cruciate Ligament Retention or Sacrifice in Total Knee Replacement Affect Proprioception? A Systematic Review

 ,
,  ,
,
Abstract
:1. Introduction
- Threshold to detection of passive motion (TTDPM): the subject is asked to indicate when he perceives the joint movement that is passively performed by a mobilization system starting from a stationary position.
- Joint position reproduction (JPR), or active joint position detection (AJPD): the subject is required to actively reproduce an established joint angle. This test allows calculation of the accuracy of the replication of the joint angle.
- Active movement extent discrimination assessment (AMEDA): the subject is asked to perform and recognize predetermined knee flexion positions.
2. Materials and Methods
2.1. Systematic Literature Search
2.2. Data Extraction
2.3. Quality Assessment
3. Results
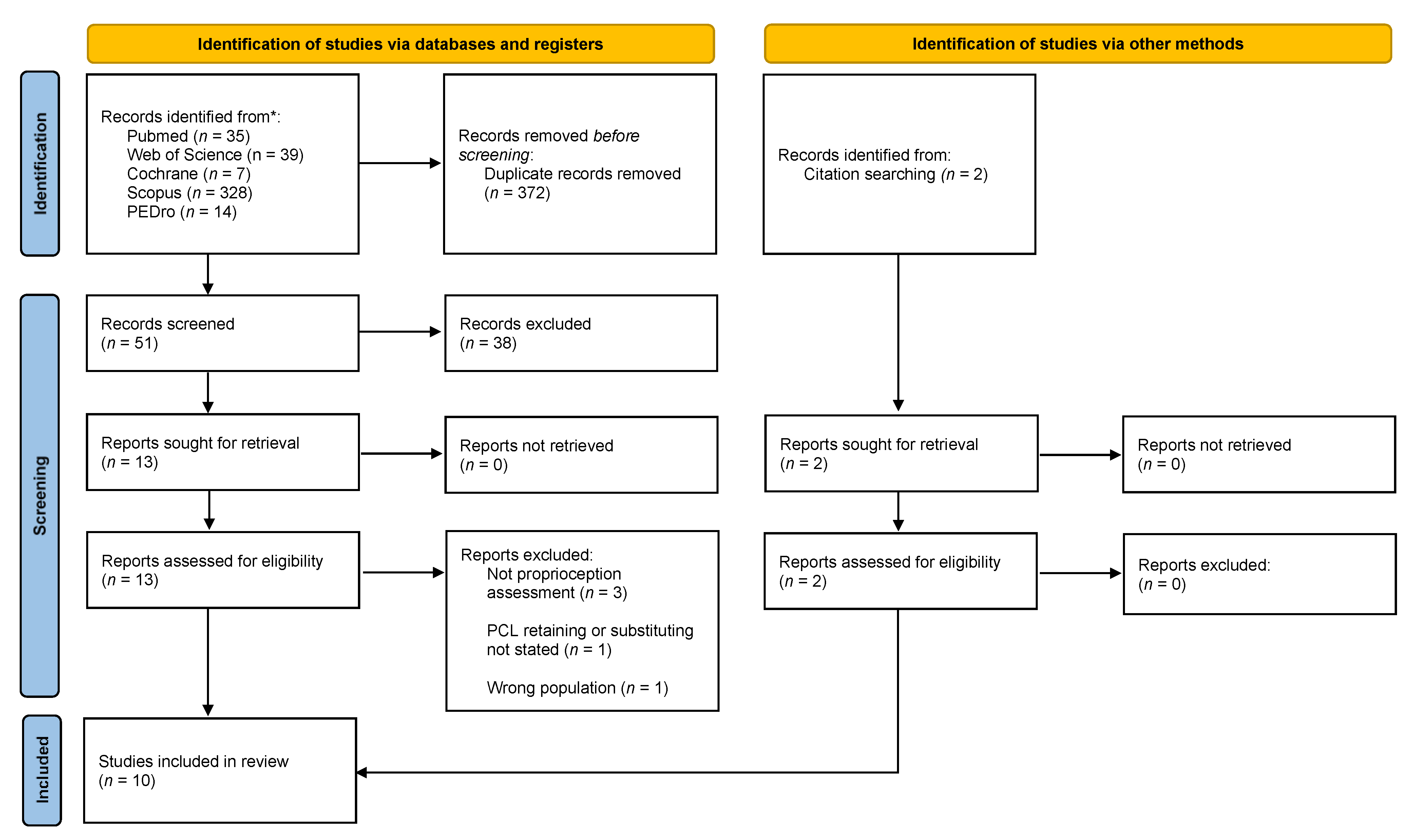
3.1. Systematic Literature Review Synthesis
3.2. Indirect Proprioception Assessment
3.3. Direct Proprioception Measurement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
| Database | Search Terms |
|---|---|
| PubMed | (“propriocept*”[All Fields] OR “Proprioception”[MeSH Terms]) AND (“total knee arthroplasty”[All Fields] OR “TKA”[All Fields] OR “TKR”[All Fields] OR “total knee replacement*”[All Fields] OR “arthroplasty, replacement, knee”[MeSH Terms]) AND (“PCL”[All Fields] OR “Posterior Cruciate Ligament”[All Fields] OR “Posterior Cruciate Ligament”[MeSH Terms]) |
| Cochrane | (Propriocept*) AND (“total knee arthroplasty” OR TKA OR TKR OR “total knee replacement*”) AND (PCL OR “posterior cruciate ligament”) |
| Scopus | ALL(propriocept*) AND (“total knee arthroplasty” OR tka OR tkr OR “total knee replacement*”) AND (pcl OR “posterior cruciate ligament”) |
| WOS | ALL = (Propriocept*) AND ALL = (“total knee arthroplasty” OR TKA OR TKR OR “total knee replacement*”) AND ALL = (PCL OR “posterior cruciate ligament”) |
| PEDro 1 | (Propriocept*) AND (“total knee arthroplasty”)(Propriocept*) AND (“total knee replacement”) |
References
- Riemann, B.L.; Lephart, S.M. The sensorimotor system, part I: The physiologic basis of functional joint stability. J. Athl. Train. 2002, 37, 71–79. [Google Scholar]
- Wodowski, A.J.; Swigler, C.W.; Liu, H.; Nord, K.M.; Toy, P.C.; Mihalko, W.M. Proprioception and Knee Arthroplasty. Orthop. Clin. N. Am. 2016, 47, 301–309. [Google Scholar] [CrossRef]
- Kvist, M. Achilles Tendon Injuries in Athletes. Sports Med. 1994, 18, 173–201. [Google Scholar] [CrossRef]
- Niessen, M.; Veeger, D.; Janssen, T. Effect of Body Orientation on Proprioception during Active and Passive Motions. Am. J. Phys. Med. Rehabil. 2009, 88, 979–985. [Google Scholar] [CrossRef]
- Han, J.; Waddington, G.; Adams, R.; Anson, J.; Liu, Y. Assessing proprioception: A critical review of methods. J. Sport Health Sci. 2016, 5, 80–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knoop, J.; Steultjens, M.; van der Leeden, M.; van der Esch, M.; Thorstensson, C.; Roorda, L.; Lems, W.; Dekker, J. Proprioception in knee osteoarthritis: A narrative review. Osteoarthr. Cartil. 2011, 19, 381–388. [Google Scholar] [CrossRef] [Green Version]
- Frattura, G.D.L.; Zaffagnini, S.; Filardo, G.; Romandini, I.; Fusco, A.; Candrian, C. Total Knee Arthroplasty in Patients With Knee Osteoarthritis: Effects on Proprioception. A Systematic Review and Best Evidence Synthesis. J. Arthroplast. 2019, 34, 2815–2822. [Google Scholar] [CrossRef]
- Hillier, S.; Immink, M.; Thewlis, D. Assessing Proprioception. Neurorehabilit. Neural Repair 2015, 29, 933–949. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.J.; Hossain, F.S.; Patel, S.; Haddad, F.S. A Cohort Study Predicts Better Functional Outcomes and Equivalent Patient Satisfaction Following UKR Compared with TKR. HSS J. 2013, 9, 21–24. [Google Scholar] [CrossRef] [Green Version]
- Inacio, M.; Paxton, E.; Graves, S.; Namba, R.; Nemes, S. Projected increase in total knee arthroplasty in the United States—An alternative projection model. Osteoarthr. Cartil. 2017, 25, 1797–1803. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.W.; Kang, S.-B.; Chang, C.B.; Moon, S.-Y.; Lee, Y.-K.; Koo, K.-H. Current Trends and Projected Burden of Primary and Revision Total Knee Arthroplasty in Korea Between 2010 and 2030. J. Arthroplast. 2021, 36, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Verra, W.C.; Boom, L.G.V.D.; Jacobs, W.; Clement, D.J.; Wymenga, A.; Nelissen, R. Retention versus sacrifice of the posterior cruciate ligament in total knee arthroplasty for treating osteoarthritis. Cochrane Database Syst. Rev. 2013, 2013, CD004803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lombardi, A.V.; Mallory, T.H.; Fada, R.A.; Hartman, J.F.; Capps, S.G.; Kefauver, C.A.; Adams, J. An Algorithm for the Posterior Cruciate Ligament in Total Knee Arthroplasty. Clin. Orthop. Relat. Res. 2001, 392, 75–87. [Google Scholar] [CrossRef]
- Mihalko, W.; Krackow, K.A. Posterior Cruciate Ligament Effects on the Flexion Space in Total Knee Arthroplasty. Clin. Orthop. Relat. Res. 1999, 360, 243–250. [Google Scholar] [CrossRef]
- Nelissen, R. Retain or sacrifice the posterior cruciate ligament in total knee arthroplasty? A histopathological study of the cruciate ligament in osteoarthritic and rheumatoid disease. J. Clin. Pathol. 2001, 54, 381–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warren, P.J.; Olanlokun, T.K.; Cobb, A.G.; Bentley, G. Proprioception after knee arthroplasty. The influence of prosthetic design. Clin. Orthop. Relat. Res. 1993, 182–187. [Google Scholar]
- Bragonzoni, L.; Rovini, E.; Barone, G.; Cavallo, F.; Zaffagnini, S.; Benedetti, M.G. How proprioception changes before and after total knee arthroplasty: A systematic review. Gait Posture 2019, 72, 1–11. [Google Scholar] [CrossRef]
- Brown, D. A Review of the PubMed PICO Tool: Using Evidence-Based Practice in Health Education. Health Promot. Pract. 2019, 21, 496–498. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ma, L.-L.; Wang, X.; Yang, Z.-H.; Huang, D.; Weng, H.; Zeng, X.-T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (MINORS ): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Van Tulder, M.; Furlan, A.; Bombardier, C.; Bouter, L. Updated Method Guidelines for Systematic Reviews in the Cochrane Collaboration Back Review Group. Spine 2003, 28, 1290–1299. [Google Scholar] [CrossRef] [Green Version]
- Vandekerckhove, P.-J.T.K.; Parys, R.; Tampere, T.; Linden, P.; Daelen, L.V.D.; Verdonk, P.C. Does cruciate retention primary total knee arthroplasty affect proprioception, strength and clinical outcome? Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 1644–1652. [Google Scholar] [CrossRef]
- Swanik, C.B.; Lephart, S.M.; Rubash, H.E. Proprioception, Kinesthesia, and Balance After Total Knee Arthroplasty with Cruciate-Retaining and Posterior Stabilized Prostheses. J. Bone Jt. Surg. Am. Vol. 2004, 86, 328–334. [Google Scholar] [CrossRef]
- Simmons, S.; Lephart, S.; Rubash, H.; Borsa, P.; Barrack, R.L. Proprioception following total knee arthroplasty with and without the posterior cruciate ligament. J. Arthroplast. 1996, 11, 763–768. [Google Scholar] [CrossRef]
- Lattanzio, P.-J.; Chess, D.G.; MacDermid, J.C. Effect of the posterior cruciate ligament in knee-joint proprioception in total knee arthroplasty. J. Arthroplast. 1998, 13, 580–585. [Google Scholar] [CrossRef]
- Ishii, Y.; Terajima, K.; Terashima, S.; Bechtold, J.E.; Laskin, R.S. Comparison of joint position sense after total knee arthroplasty. J. Arthroplast. 1997, 12, 541–545. [Google Scholar] [CrossRef]
- Götz, J.; Beckmann, J.; Sperrer, I.; Baier, C.; Dullien, S.; Grifka, J.; Koeck, F. Retrospective comparative study shows no significant difference in postural stability between cruciate-retaining (CR) and cruciate-substituting (PS) total knee implant systems. Int. Orthop. 2016, 40, 1441–1446. [Google Scholar] [CrossRef]
- Fuchs, S.; Thorwesten, L.; Niewerth, S. Proprioceptive function in knees with and without total knee arthroplasy1. Am. J. Phys. Med. Rehabil. 1999, 78, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Cash, R.M.; Gonzalez, M.H.; Garst, J.; Barmada, R.; Stern, S.H. Proprioception after arthroplasty: Role of the posterior cruciate ligament. Clin. Orthop. Relat. Res. 1996, 172–178. [Google Scholar] [CrossRef]
- Bascuas, I.; Tejero, M.; Monleón, S.; Boza, R.; Muniesa, J.M.; Belmonte, R. Balance 1 Year After TKA: Correlation With Clinical Variables. Orthopedics 2013, 36, e6–e12. [Google Scholar] [CrossRef] [Green Version]
- Baumann, F.; Bahadin, Ö.; Krutsch, W.; Zellner, J.; Nerlich, M.; Angele, P.; Tibesku, C.O. Proprioception after bicruciate-retaining total knee arthroplasty is comparable to unicompartmental knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2016, 25, 1697–1704. [Google Scholar] [CrossRef]
- Sharma, L.; Pai, Y.-C.; Holtkamp, K.; Rymer, W.Z. Is knee joint proprioception worse in the arthritic knee versus the unaffected knee in unilateral knee osteoarthritis? Arthritis Rheum. 1997, 40, 1518–1525. [Google Scholar] [CrossRef]
- Roberts, D.; Andersson, G.; Fridén, T. Knee joint proprioception in ACL-deficient knees is related to cartilage injury, laxity and ageA retrospective study of 54 patients. Acta Orthop. Scand. 2004, 75, 78–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrack, R.L.; Skinner, H.; Brunet, M.E.; Cook, S.D. Joint Laxity and Proprioception in the Knee. Physician Sportsmed. 1983, 11, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Koralewicz, L.M.; Engh, G.A. Comparison of Proprioception in Arthritic and Age-Matched Normal Knees. J. Bone Jt. Surg. Am. Vol. 2000, 82, 1582–1588. [Google Scholar] [CrossRef] [Green Version]
- Pai, Y.-C.; Rymer, W.Z.; Chang, R.W.; Sharma, L. Effect of age and osteoarthritis on knee proprioception. Arthritis Rheum. 1997, 40, 2260–2265. [Google Scholar] [CrossRef] [PubMed]
- Fujito, T.; Tomita, T.; Yamazaki, T.; Oda, K.; Yoshikawa, H.; Sugamoto, K. Influence of Posterior Tibial Slope on Kinematics After Cruciate-Retaining Total Knee Arthroplasty. J. Arthroplast. 2018, 33, 3778–3782.e1. [Google Scholar] [CrossRef]
- Migliorini, F.; Eschweiler, J.; Tingart, M.; Rath, B. Posterior-stabilized versus cruciate-retained implants for total knee arthroplasty: A meta-analysis of clinical trials. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 937–946. [Google Scholar] [CrossRef]
- Bravi, M.; Gallotta, E.; Morrone, M.; Maselli, M.; Santacaterina, F.; Toglia, R.; Foti, C.; Sterzi, S.; Bressi, F.; Miccinilli, S. Concurrent validity and inter trial reliability of a single inertial measurement unit for spatial-temporal gait parameter analysis in patients with recent total hip or total knee arthroplasty. Gait Posture 2020, 76, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Boekesteijn, R.J.; Smolders, J.M.H.; Busch, V.J.J.F.; Geurts, A.C.H.; Smulders, K. Independent and sensitive gait parameters for objective evaluation in knee and hip osteoarthritis using wearable sensors. BMC Musculoskelet. Disord. 2021, 22, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Webster, K.E.; Wittwer, J.; Feller, J.A. Validity of the GAITRite® walkway system for the measurement of averaged and individual step parameters of gait. Gait Posture 2005, 22, 317–321. [Google Scholar] [CrossRef] [PubMed]
| Population | Intervention | Comparison | Outcome |
|---|---|---|---|
| Adults with total knee replacement | PCL retaining PCL substituting | Direct and indirect proprioception assessment |
| Clearly Defined Aim | Consecutive Patients | Prospective Data Collection | Adequate Endpoint | Blind Assessment | Adequate Length of Follow-Up | Loss to Follow-Up Rate <5% | Prospective Calculation of the Study Size | Control Equivalent to Cases | Control Contemporaneous to Cases | Baseline Equivalence of Groups | Adequate Statistical Analysis | Total Score | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Götz et al. (2016) | 2 | 0 | 2 | 0 | 0 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 16/24 |
| Vandekerckhove et al. (2014) | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 20/24 |
| Bascuas et al. (2013) | 2 | 2 | 2 | 1 | 0 | 2 | 1 | 0 | 2 | 2 | 1 | 2 | 17/24 |
| Fuchs et al. (1999) | 2 | 1 | 2 | 1 | 0 | 2 | 0 | 0 | 2 | 2 | 0 | 2 | 14/24 |
| Lattanzio et al. (1998) | 2 | 1 | 2 | 1 | 1 | 2 | 0 | 0 | 1 | 2 | 2 | 2 | 16/24 |
| Ishii et al. (1997) | 1 | 1 | 2 | 1 | 0 | 2 | 1 | 0 | 1 | 2 | 1 | 2 | 14/24 |
| Cash et al. (1996) | 2 | 1 | 2 | 1 | 1 | 2 | 2 | 0 | 0 | 2 | 2 | 2 | 17/24 |
| Simmons et al. (1996) | 2 | 2 | 2 | 1 | 0 | 2 | 1 | 0 | 0 | 2 | 2 | 2 | 16/24 |
| Warren et al. (1993) | 1 | 1 | 2 | 1 | 0 | 2 | 1 | 0 | 1 | 2 | 1 | 2 | 14/24 |
| Author (Year) | Design and Aim | Participants | Instruments | Proprioception Assessment | Assessment Protocol | Results |
|---|---|---|---|---|---|---|
| Götz et al. (2016) | Observational To evaluate whether a CR TKA should be preferred over a PS TKA regarding postural stability in one-leg stance and clinical scores. | 40 patients with primary OA designated for TKA. CR group: n = 20; 4 males; mean age = 64.3 ± 7.3 y; mean BMI = 31.5 ± 5.9 kg/m2; PS group: n = 20; 5 males; mean age = 70 ± 7.9 y; mean BMI = 33.4 ± 14.1 kg/m2; Assignment to group depending on stability needs. Evaluation mean FU = 5.3 months. | Biodex Balance System® (Biodex Inc., Shirley, NY, USA). | Postural stability by means of ability to balance on both legs and on single leg. | The ability to balance on both legs was tested asking the patients to keep their centre of mass (visible as a moving black dot on a screen in front of them) in the centre of the target for 3 × 20 s. One leg stance: the ability to balance on one leg was tested asking the patients to keep the balance standing with one leg on the locked platform for 3 ×10 s starting with the non-operated leg. | One leg stance: CR operated side vs. healty side: median 1.35 vs. 1.50 (p = 0.732). PS operated side vs. healty side: 1.55 vs. 1.60 (p = 0.125). No significant differences between groups (2.37 CR, 2.89 PS; p = 0.198) of postural stability index (variance of change of platform in degrees) for the two-leg stance on the unstable platform. The difference in one-leg stance was not statistically significant between groups (1.65 CR; 2.05 PS; p = 0.314). No proof of the superiority of PCL retaining over substituting in terms of postural stability. |
| Vandekerckhove et al. (2014) | Observational To perform a functional comparison between CR and PS TKA. | 45 patients with TKA for end-stage OA. CR group: n = 27; male/female ratio = 0.33; mean age = 70.5 ± 6.4 y; PS group: n = 18; male/female ratio = 0.55; mean age = 68.0 ± 8.4 y; Assignment to group depending on stability needs. Evaluation mean FU: CR = 2.9 ± 0.8 years; PS = 3.1 ± 0.8 years. | Balance Master system® (Neurocom, Clackamas, OR, USA) | Balance and postural control tests consisting of five subtests: WBS, mCTSIB, UST, LOS, RWS test. | WBS measures the percentage of body weight undergone by each leg consecutively while standing erect, and then squatting in three positions of knee flexion (30°, 60° and 90°). mCTSIB measures the postural sway velocity in bilateral standing position on the firm and unstable surface with eyes open and closed. UST measures the postural sway velocity on a single leg (both the operated and non-operated leg were tested). LOS quantifies the maximum distance participants can lean their bodies in a given direction without losing balance. Patients are asked to reach 8 targets distributed from a central point and displayed on a screen. RWS quantifies the subject’s ability to rhythmically move their COG from the left to the right and forward to backward at 3 different speeds: slow, moderate and fast. | UST: no significance differences between CR and PS. Comparison of both CR and PS TKA to the non-operated contralateral leg revealed no significant differences. CR group showed statistically higher speed than PS for RWS test at slow (p = 0.01) and moderate (p = 0.03) speeds. The PCL does not seem to play an important role in balance/postural control. |
| Bascuas et al. (2013) | Observational | 44 (12 male; mean age 71.4 ± 7.12 y; BMI 32.65 ± 5.02 kg/m2) patients underwent TKA for severe OA. CR group: n = 16 PS group: n = 28 Evaluation mean FU: 12 months. | Neurocom Balance Master | Balance, mCTSIB | 3 posturopgraphy test: The center of gravity movement is measured 3 times in each test, 10 s per trial. The amount of sway is expressed in degrees per sec. The test was done: on a firm surface with open eyes, on a firm surface with closed eyes, on a foam surface with open eyes, and on a foam surface with closed eyes. | No significant difference existed in posturograpy changes when comparing CR vs. PS group. |
| Swanik et al. (2004) | Randomized Controlled Trial To evaluate and compare the effects of total knee arthroplasty with cruciate-retaining and posterior stabilized prostheses by assessing proprioception, kinesthesia, and balance | 20 patients (13 male) underwent TKA for a grade-2 or 3 OA were randomly assigned to CR or PS group. CR group: n = 10; mean age = 71.1 ± 6.3 y;PS group: n = 10; mean age = 69.4 ± 5 y; Evaluation at T0 = 1.5 months preoperatively and T1 = 7.6 months postoperatively. | Non-commercial proprioception testing device. Biodex Balance System® (Biodex Inc., Shirley, NY, USA). | TTDPM; JPS; balance test | - TTDPM: the proprioception testing device passively rotated the knee into flexion or extension at a velocity of 0.5°/sec. On perceiving motion, the subject pressed a handheld switch, and the degree of rotation was recorded. Test repeated 6 times: 3 times for passive flexion and 3 time for passive extension. - JPS was measured as reproduction of passive positioning: the subject’s knee was rotated away from the starting position to a presented angle the position was held 10 s. Then, from starting position the knee was passively rotated at a constant velocity (0.5°/sec) toward the presented angle. The subject disengaged the device by pressing the handheld switch when the knee position reproduced the presented angle. The difference between the presented angle and the reproduced angle was recorded in degrees. The test was repeated a total of 4 times, with reproduction of passive positioning moving into flexion and extension measured from both 15° and 45° reference positions. - Balance was assessed asking the subject to maintain balance for 20 s standing on the Biodex unstable platform. The test was repeated 3 times at 2 different levels of difficulty. | PS JPS (mean error, 1.0° ± 0.5°) was significantly more accurate (p < 0.05) than CR (mean error, 2.2° ± 1.0°) when moving into extension from 45° knee joint angle. No significant differences for all the other tested positions. TTDPM did not identify any significant differences at either of the two test angles (15° and 45°) moving into either flexion or extension. Balance test: no significant differences between PS and CR group. The results show no substantial proprioceptive or kinesthetic advantages of preserving posterior cruciate ligament. |
| Fuchs et al. (1999) | Controlled Clinical Trial To evaluate the differences in angle reproduction capability after non-constrained posterior cruciate ligament retaining total knee arthroplasty | 28 patients underwent non-constrained CR TKA for OA. CR group: n = 28; 11 male; mean age = 65.7 y; CTRL group (healthy): n = 25; 11 male; mean age 55.7 y. Evaluation mean FU: 63.9 (range, 13–89) months. | Kinemetrix motion analysis system (Orthodata Lüdenscheid, Germany) | JPS | 16 measurements (operated/nonoperated leg: 0°, 30°, 60°, 90°, 90°, 60°, 30°, 0°) were made in the sitting position, with the lower leg hanging free. Patients were blindfolded and not blindfolded. The leg was positioned by the examiner, then relaxed, and afterward, the subject was asked to reproduce the original joint position. The test was repeated 3 times before measurements were taken. The starting joint positions were assumed by the subjects before each measurement and checked by the examiner. The patients were examined starting at 90 and 0° of knee flexion to restore 60° and 30° of knee flexion. | With visual control no significant differences between CR (mean error: 6.1 ± 5.9°) and CTRL (mean error (5.6 ± 4.6°) from 0° to 30° (p = 0.734) and from 0° to 60° CR = 11 ± 7.5°; CTRL = 7.2 ± 5°; p = 0.033). Without visual control significant differences between CR (7.7 ± 5.9°) and CTRL (4.6 ± 4.7°) (p = 0.041). No significant differences between the operated and the contralateral leg. Reduced proprioceptive capabilities are present after non-constrained CR TKA in both the operated and the contralateral leg compared with healthy controls. |
| Lattanzio et al. (1998) | Observational To examine the role of the PCL in knee-joint proprioception after TKA | 20 patients underwent TKA for OA. CR group: n = 10; 4 male; mean age = 74 (range, 65–83)y; PS group: n = 10; 4 male; mean age = 69 (range, 53–82 y); Evaluation mean FU: CR = 10 (range, 6.3–16.8) months; PS = 12 (range, 6.5–16.0) | Penny and Giles electrogoniometer | JPS | The starting position was 90° of knee flexion and the testing range was 10° to 55° of knee extension from the reference position. 10 randomized test angles were evaluated for each experimental trial. Both the operated and non-operated leg was evaluated. The patient was instructed to extend the testing leg to a predetermined angle. When the test angle was reached, the patient was asked to concentrate on the test angle for 3 s. The patient then lowered the testing leg back to the starting angle and remained there for another 3 s. After the 3-s interval the patient was given 5 s to reproduce the test angle and acknowledge when he/she believed had reproduced the designated test angle. Absolute angular error was measured. | The mean error values between the operated and non-operated knee in each patient were not significantly different (p > 0.4). No significant differences between the CR and PS group (p > 0.6). Preserving the PCL in TKA may not improve knee-joint proprioception and consequently may not improve functional joint performance after total knee arthroplasty. |
| Ishii et al. (1997) | Controlled Clinical Trial | 48 OA patients undergoing a TKA. 4 male; mean age = 70 (range, 54–82) y. The patients were divided into five study groups. Groups 1–4 included patients with a cemented TKA. Group l: CR and patella not resurfaced. Group 2: CR and patella resurfaced. Groups 3: PS and patella not resurfaced. Group 4: PS and patella resurfaced. Group 5: non-cemented CR TKA and patella notresurfaced. Group 6: age-matched non-arthroplasty mild osteoarthritis patients. Evaluation mean FU: 24 (range, 12–48) months. | A 6-degree-of-freedom electrogoniometer or instrumented spatial linkage. | JPS | The subject actively sets both the initial and repeat angles. The tests were conducted on one leg at a time in randomized order, with the tested leg hanging freely and the patient standing upright on the opposite leg. The resulting error terms were based on the averages of 6 trials, 3 made at 30° and 3 made at 70° of flexion. | Groups 1 and 3 did not have significant difference in either reproducibility of index angle (group 1, 5.6° ± 2.4°; group 3, 5.4° ± 1.6°) or reproducibility of change of angles (group l, 4.6° ± 3.1°; group 3, 5.7° ± 3.7°). For groups 2 and 4, no significant differences in either reproducibility of the index angles (group 2, 6.1° ± 3.1°; group 4, 3.7° ± 1.6°) or reproducibility of the change of angles (group 2, 4.2° ± 3.0°; group 4, 5.1° ± 1.9°). No significant difference among any of the 6 groups for any test at p = 0.05. Retaining the PCL does not appear to impart the advantage of improved proprioception. |
| Cash et al. (1996) | Observational To test the hypothesis that retaining the posterior cruciate ligament during total knee arthroplasty helps preserve the threshold of proprioceptive sensation | 60 patients undergone unilateral TKA for OA. CR group: n = 30; 13 male; mean age = 69 (range, 69–91) y. PS group: n = 30; 9 male; mean age = 65 (range, 41–84) y. Evaluation mean FU: CR = 34 (range, 12–87) months; PS = 39 (range, 12–156) months. | Non-commercial device which passively extended either leg at a constant rate of 0.5° per second. | TTDPM | Patients were seated in a relaxed position with both legs hooked up to the apparatus. Patients were given a right and left sided button and told to hit the button on the side that they perceived motion. Patients were blindfolded not informed as to which leg was being tested. Auditory clues were removed by random initiation of motion by a clutch 5 to 30 s after starting the pulley motors. The knee was tested between 45° and 90° flexion. Each lower extremity was tested 3 times in an independent and random fashion. The recorded angular deflection for each lower extremity was averaged to give a mean angular deflection at the threshold for the operative and nonoperative lower extremities. The patients were asked to indicate their perception of motion by pushing the button for the appropriate extremity. | No difference between CR (2.4 ± 1.0°) and PS (2.4 ± 1.5°) angular deflection. The average difference in angular deflection at threshold between operated and non-operated knees was not significant in both group (p = 0.05). The decision to retain the posterior cruciate ligament should not be made based on the premise of improved proprioceptive function. |
| Simmons et al. (1996) | Observational to quantify whether a difference in proprioceptive ability could be detected between CR TKA and PS TKA. | 28 patients (10 male; mean age 69 y) undergone unilateral CR or PS TKA for OA. CR group: n = 15; PS group: n = 13; Evaluation mean FU: 23 (range, 6–47) months. | A non-commercial proprioception testing device which rotated the knee at a constant angular velocity (0.5°/s), and an optical encoder, which measured angular displacement of the knee in degrees. | TTDPM | The TTDPM was tested from starting positions of 15° knee flexion and 45° knee. The testing device moved the knee randomly into flexion or extension at a constant angular velocity from the two starting positions. The subject signified the detection of passive motion by pressing a remote switch. After 2 practice trials, 3 randomized runs of the TTDPM were subsequently recorded with both flexion and extension from the two starting positions. | No significant difference between mean TTDPM for CR (2.24) and PS groups (2.36). No significant differences between the operated and non-operated knee except for testing condition on 15° moving into flexion (2.44° ± 0.34° vs. 2.01° ± 0.27°, p = 0.04). Patients with grade 2 OA: no differences between CR and PS group in TTDPM (p > 0.04) Patients with grade 3 OA: PS group performed significantly better than CR at all tests. Retaining the PCL in TKA did not result in improved performance in proprioception testing. Attempting to retain the PCL may be counterproductive in the severely degenerative knee. |
| Warren et al. (1993) | Controlled clinical trial To test if CR TKA confer better proprioception than PS TKA. | 9 healthy subjects (6 male; age range = 26–61 y) and 50 patients undergone TKA for OA (13 male; age range = 56–85 y). A total of 118 knees assessed. CR group: n = 25 | Electrogoniometer (Penny & Giles Blackwood, Blackwood, Gwent) and a non-commercial apparatus consisting in a well-padded leg supporting jig | JPS | The test involved the passive movemente of the leg to a predetermined sequence of ten positions of knee flexion (0° to 60°). The subject indicated his perception of the position of his knee using a hand-held model of a leg, incorporating another electrogoniometer. Measurements of joint position awareness was performed to measures the inaccuracy in estimating the change of one position to another (mean difference Ω). | Knees with CR TKA showed significantly better (p = 0.042) joint position appreciation (mean diff 10.3; range, 4.33–23.67) than PS TKA (mean diff 12.27; range, 4.56–30.1)Irrespective of its precise mechanism, the finding of improved joint position awareness may support the PCL retention in TKA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bravi, M.; Santacaterina, F.; Bressi, F.; Papalia, R.; Campi, S.; Sterzi, S.; Miccinilli, S. Does Posterior Cruciate Ligament Retention or Sacrifice in Total Knee Replacement Affect Proprioception? A Systematic Review. J. Clin. Med. 2021, 10, 3470. https://doi.org/10.3390/jcm10163470
Bravi M, Santacaterina F, Bressi F, Papalia R, Campi S, Sterzi S, Miccinilli S. Does Posterior Cruciate Ligament Retention or Sacrifice in Total Knee Replacement Affect Proprioception? A Systematic Review. Journal of Clinical Medicine. 2021; 10(16):3470. https://doi.org/10.3390/jcm10163470
Chicago/Turabian StyleBravi, Marco, Fabio Santacaterina, Federica Bressi, Rocco Papalia, Stefano Campi, Silvia Sterzi, and Sandra Miccinilli. 2021. "Does Posterior Cruciate Ligament Retention or Sacrifice in Total Knee Replacement Affect Proprioception? A Systematic Review" Journal of Clinical Medicine 10, no. 16: 3470. https://doi.org/10.3390/jcm10163470
APA StyleBravi, M., Santacaterina, F., Bressi, F., Papalia, R., Campi, S., Sterzi, S., & Miccinilli, S. (2021). Does Posterior Cruciate Ligament Retention or Sacrifice in Total Knee Replacement Affect Proprioception? A Systematic Review. Journal of Clinical Medicine, 10(16), 3470. https://doi.org/10.3390/jcm10163470