


Immunization as Protection Against Long COVID in the Americas: A Scoping Review

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search
2.5. Selection of Sources of Evidence
2.6. Data Charting Process
2.7. Data Items
2.8. Critical Appraisal of Individual Sources of Evidence
2.9. Synthesis of Results
3. Results
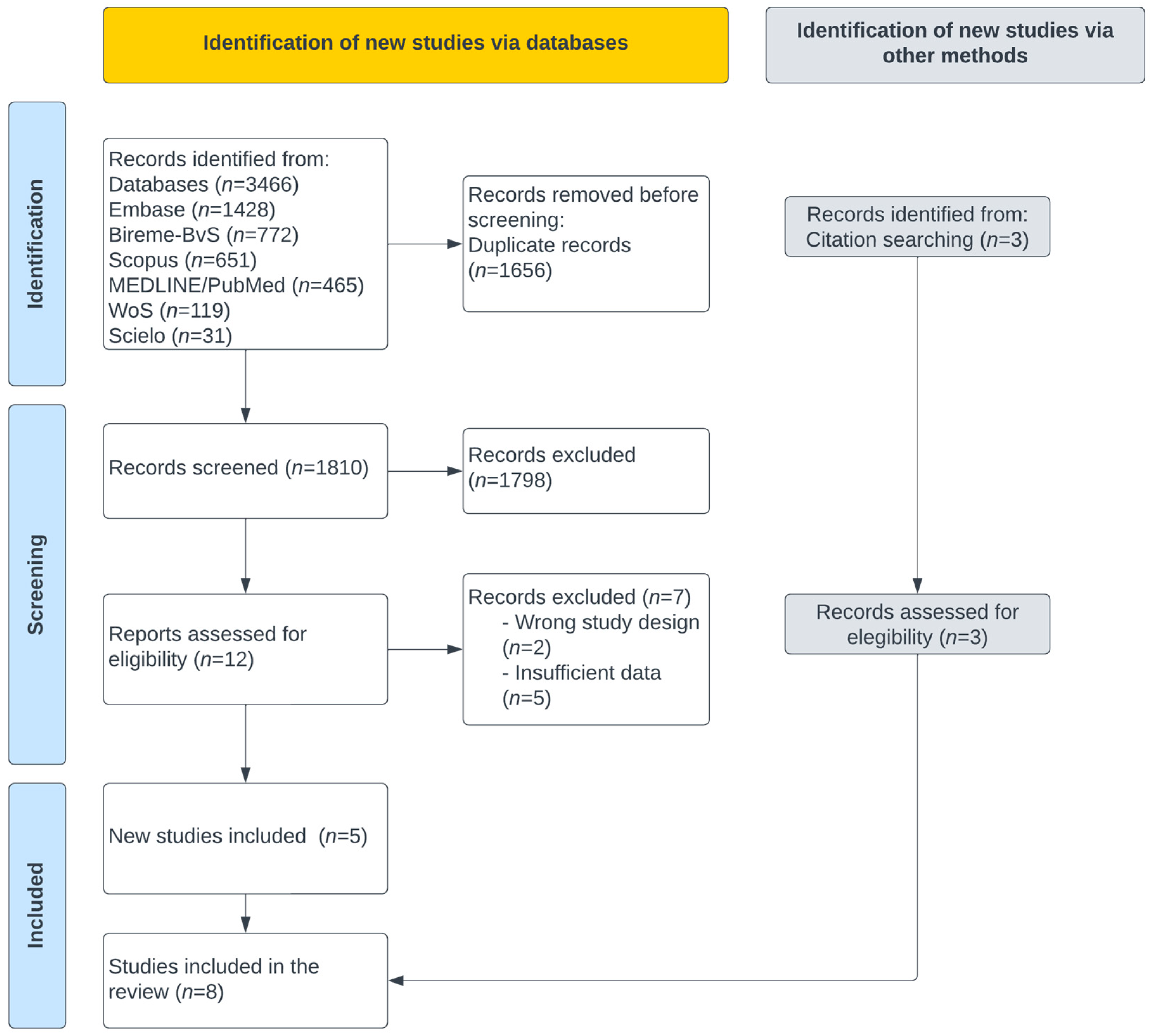
3.1. Selection of Evidence Sources
3.2. Characteristics and Results of the Sources of Evidence
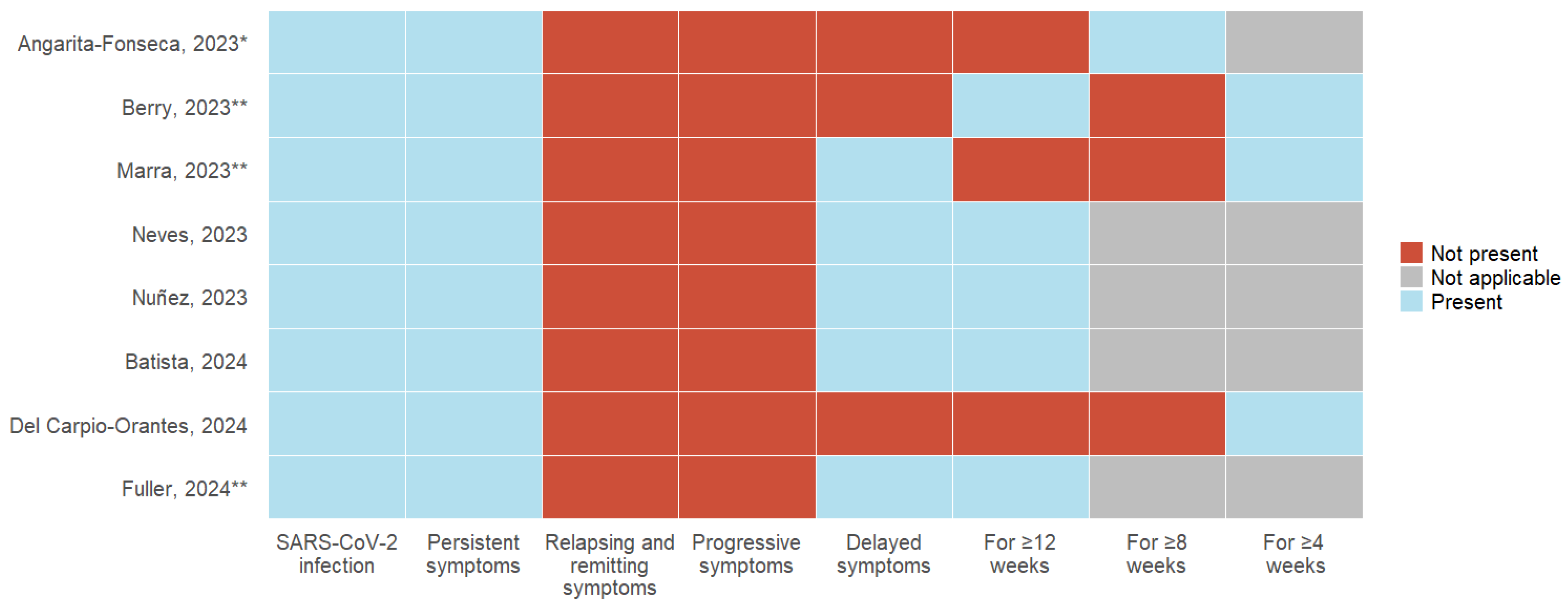
3.3. Definitions of Long COVID
- NR: Not reported, OR: Odds Ratio, HR: Hazard Ratio;
- SARS-CoV-2 infection: All eight articles, as a requirement, include a history of acute COVID-19 infection; 37.5% (3) of the studies describe the need for a positive laboratory test for SARS-CoV-2, and 12.5% (1) include suspicion and confirmation of acute infection;
- Symptoms: The persistence of symptoms from the acute stage was considered by 100% (8) of the studies; remitting and recurrent symptoms and symptom progression were not included in any definition. 62.5% (5) described developing new symptoms after the acute stage of infection;
- Time of presentation: 100% (8) of the studies describe a specific time of permanence of symptoms following acute infection. 50% (4) consider 12 weeks or more, 12.5% (1) describe 8 weeks or more, and 37.5% (3) use 4 weeks or more as a defining criterion.3.4. Vaccination Status.
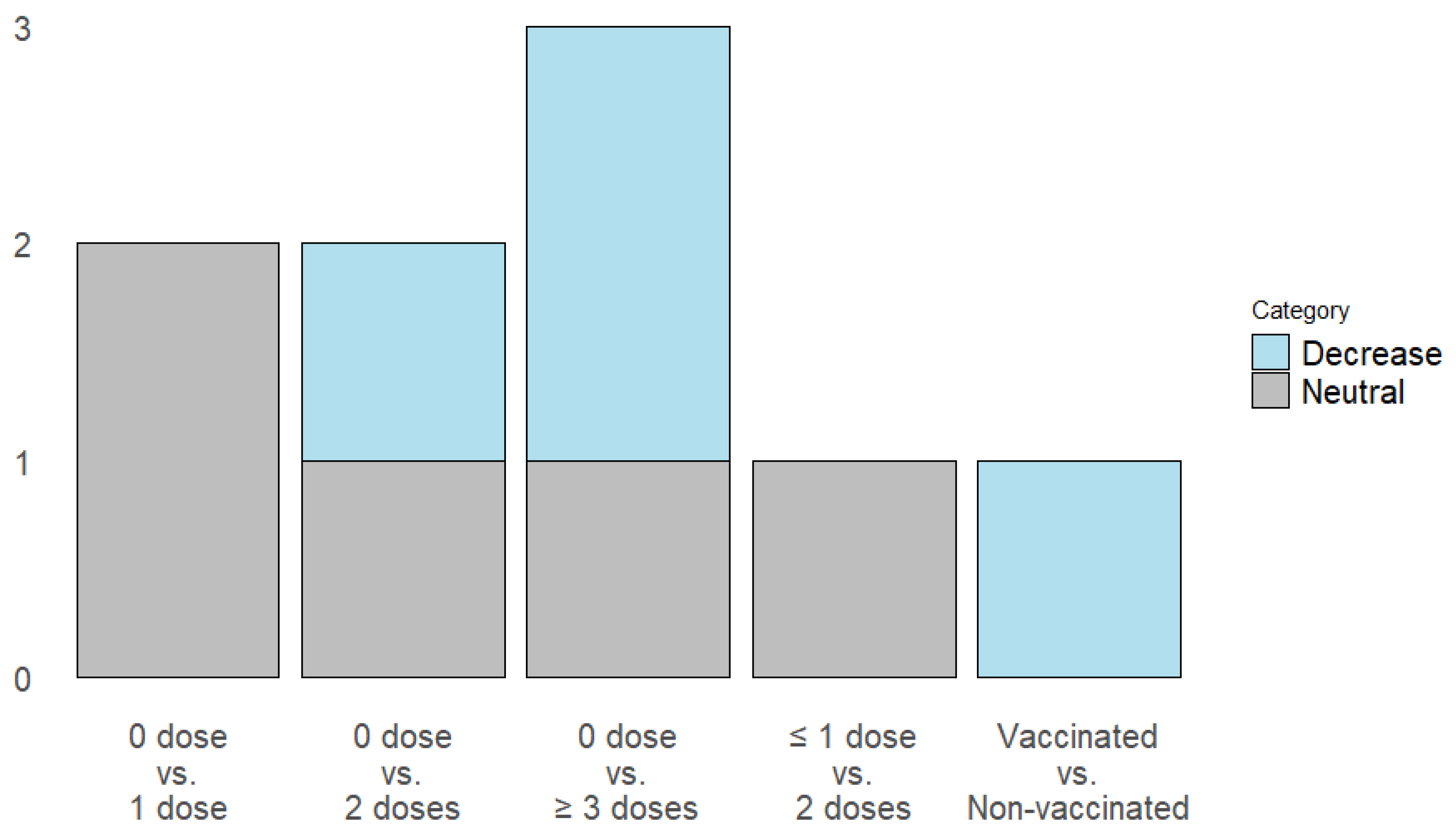
3.4. Reducing the Incidence of Long COVID
- Batista et al. evaluated the complete vaccination status, demonstrating that it decreases the risk of Long COVID [25].
3.5. The Severity of Symptoms Related to Long COVID
3.6. Duration of Long COVID Symptoms
4. Discussion
4.1. What Is Already Known About This Topic
4.2. Main Findings
4.3. Implications for Public Health in the Americas. A Call to Action
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PCC | Post-COVID-19 condition |
| PASC | Post-acute sequelae of COVID-19 |
| JBI | Joanna Briggs Institute |
References
- CDC. Long COVID or Post-COVID Conditions 2023. Available online: https://stacks.cdc.gov/view/cdc/133106 (accessed on 11 November 2023).
- Ely, E.W.; Brown, L.M.; Fineberg, H.V. From the National Academy of Medicine Long Covid Defined Medicine Committee on Examining the Working Definition for Long Covid*. N. Engl. J. Med. 2024, 391, 1746–1753. [Google Scholar] [CrossRef]
- Sk Abd Razak, R.; Ismail, A.; Abdul Aziz, A.F.; Suddin, L.S.; Azzeri, A.; Sha’ari, N.I. Post-COVID syndrome prevalence: A systematic review and meta-analysis. BMC Public Health 2024, 24, 1785. [Google Scholar] [CrossRef] [PubMed]
- Woodrow, M.; Carey, C.; Ziauddeen, N.; Thomas, R.; Akrami, A.; Lutje, V.; Greenwood, D.C.; A Alwan, N. Systematic Review of the Prevalence of Long COVID. Open Forum Infect. Dis. 2023, 10, ofad233. [Google Scholar] [CrossRef] [PubMed]
- WHO Post COVID-19 Condition (Long COVID). 2022. Available online: https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-condition (accessed on 11 November 2023).
- Angarita-Fonseca, A.; Torres-Castro, R.; Benavides-Cordoba, V.; Chero, S.; Morales-Satán, M.; Hernández-López, B.; Salazar-Pérez, R.; Larrateguy, S.; Sanchez-Ramirez, D.C. Exploring long COVID condition in Latin America: Its impact on patients’ activities and associated healthcare use. Front. Med. 2023, 10, 1168628. [Google Scholar] [CrossRef] [PubMed]
- Núñez, I.; Gillard, J.; Fragoso-Saavedra, S.; Feyaerts, D.; Islas-Weinstein, L.; Gallegos-Guzmán, A.A.; Valente-García, U.; Meyerowitz, J.; Kelly, J.D.; Chen, H.; et al. Longitudinal clinical phenotyping of post COVID condition in Mexican adults recovering from severe COVID-19: A prospective cohort study. Front. Med. 2023, 10, 1236702. [Google Scholar] [CrossRef]
- Alvarez-Moreno, C.A.; Pineda, J.; Bareño, A.; Espitia, R.; Rengifo, P. Long COVID-19 in Latin America: Low prevalence, high resilience or low surveillance and difficulties accessing health care? Travel Med. Infect. Dis. 2023, 51, 102492. [Google Scholar] [CrossRef]
- Peluso, M.J.; Swank, Z.N.; Goldberg, S.A.; Lu, S.; Dalhuisen, T.; Borberg, E.; Senussi, Y.; A Luna, M.; Song, C.C.; Clark, A.; et al. Plasma-based antigen persistence in the post-acute phase of COVID-19. Lancet Infect. Dis. 2024, 24, e345–e347. [Google Scholar] [CrossRef]
- PAHO/WHO. Summary Situation and COVID-19 Cases and Deaths 2023. Available online: https://www.paho.org/en/covid-19-weekly-updates-region-americas (accessed on 11 November 2023).
- WHO. Statement on the Antigen Composition of COVID-19 Vaccines 2024. Available online: https://www.who.int/news/item/26-04-2024-statement-on-the-antigen-composition-of-covid-19-vaccines (accessed on 30 November 2024).
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-term cardiovascular outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef]
- Gao, P.; Liu, J.; Liu, M. Effect of COVID-19 Vaccines on Reducing the Risk of Long COVID in the Real World: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 12422. [Google Scholar] [CrossRef]
- Tami, A.; van der Gun, B.T.F.; Wold, K.I.; Vincenti-González, M.F.; Veloo, A.C.M.; Knoester, M.; Harmsma, V.P.R.; de Boer, G.C.; Huckriede, A.L.W.; Pantano, D.; et al. The COVID HOME study research protocol: Prospective cohort study of non-hospitalised COVID-19 patients. PLoS ONE 2022, 17, e0273599. [Google Scholar] [CrossRef]
- Zhang, H.; Zang, C.; Xu, Z.; Zhang, Y.; Xu, J.; Bian, J.; Morozyuk, D.; Khullar, D.; Zhang, Y.; Nordvig, A.S.; et al. Data-driven identification of post-acute SARS-CoV-2 infection subphenotypes. Nat. Med. 2022, 29, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Zambrano-Sánchez, G.; Rivadeneira, J.; Manterola, C.; Fuenmayor-González, L. Immunization as protection against long COVID in the Americas: A scoping review protocol. OSF 2024. [Google Scholar] [CrossRef]
- Peters, M.D.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11: Scoping Reviews. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; JBI: North Adelaid, Australia, 2020. [Google Scholar]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Khalil, H.; Larsen, P.; Marnie, C.; Pollock, D.; Tricco, A.C.; Munn, Z. Best practice guidance and reporting items for the development of scoping review protocols. JBI Evid. Synth. 2022, 20, 953–968. [Google Scholar] [CrossRef] [PubMed]
- Moraga, J.; Manterola, C.; Cartes-Velasquez, R.A.; Me, B.; Aravena, P.; Urrutia, S. Instructions for the Use of MINCIR Scale to Assess Methodological Quality in Therapy Studies. Int. J. Morphol. 2014, 32, 294–298. [Google Scholar] [CrossRef]
- Neves Amorim, C.E.; Silveira Cazetta, G.; Pontello Cristelli, M.; Requião-Moura, L.R.; Rodrigues da Silva, E.; Pinheiro Vale, L.; Brito, M.d.M.P.; Bronzo, T.M.; Nakamura, M.R.M.; Tedesco-Silva, H.; et al. Long COVID Among Kidney Transplant Recipients Appears to Be Attenuated During the Omicron Predominance. Transplantation 2023, 108, 963–969. [Google Scholar] [CrossRef]
- Marra, A.R.; Sampaio, V.S.; Ozahata, M.C.; Lopes, R.; Brito, A.F.; Bragatte, M.; Kalil, J.; Miraglia, J.L.; Malheiro, D.T.; Guozhang, Y.; et al. Risk factors for long coronavirus disease 2019 (long COVID) among healthcare personnel, Brazil, 2020-2022. Infect. Control Hosp. Epidemiol. 2023, 44, 1972–1978. [Google Scholar] [CrossRef]
- Berry, D.S.F.; Dalhuisen, T.; Marchena, G.; Tiemessen, I.; Geubbels, E.; Jaspers, L. Association between post-infection COVID-19 vaccination and symptom severity of post COVID-19 condition among patients on Bonaire, Caribbean Netherlands: A retrospective cohort study. MedRxiv, 2023; preprint. [Google Scholar] [CrossRef]
- Del Carpio-Orantes, L.; Trelles-Hernández, D.; García-Méndez, S.; Sánchez-Díaz, J.S.; Aguilar-Silva, A.; López-Vargas, E.R. Clinical-epidemiological characterization of patients with long COVID in Mexico. Gac. Med. Mex. 2024, 160, 144–151. [Google Scholar] [CrossRef]
- Batista, K.B.C.; Fernandez, M.V.; Barberia, L.G.; da Silva, E.T.; Pedi, V.D.; Pontes, B.M.L.M.; Araujo, G.; Moreira, R.d.S.; Pedrosa, M.; Verotti, M.P.; et al. Overview of long COVID in Brazil: A preliminary analysis of a survey to think about health policies. Cad Saude Publica 2024, 40, e00094623. [Google Scholar] [CrossRef]
- Fuller, T.; Flores Mamani, R.; Ferreira Pinto Santos, H.; Melo Espíndola, O.; Guaraldo, L.; Lopes Melo, C.; Da Silva, M.F.B.; Calvet, G.A.; Bastos, L.S.; Carvalho, M.S.; et al. Sex, vaccination status, and comorbidities influence long COVID persistence. J. Infect. Public Health 2024, 17, 102562. [Google Scholar] [CrossRef]
- Signore, I.A.; Donoso, G.; Bocchieri, P.; Tobar-Calfucoy, E.A.; Yáñez, C.E.; Carvajal-Silva, L.; Silva, A.X.; Otth, C.; Cappelli, C.; Jorquera, H.V.; et al. The Chilean COVID-19 Genomics Network Biorepository: A Resource for Multi-Omics Studies of COVID-19 and Long COVID in a Latin American Population. Genes 2024, 15, 1352. [Google Scholar] [CrossRef]
- Watanabe, A.; Iwagami, M.; Yasuhara, J.; Takagi, H.; Kuno, T. Protective effect of COVID-19 vaccination against long COVID syndrome: A systematic review and meta-analysis. Vaccine 2023, 41, 1783–1790. [Google Scholar] [CrossRef] [PubMed]
- Brannock, M.D.; Chew, R.F.; Preiss, A.J.; Hadley, E.C.; Redfield, S.; McMurry, J.A.; Leese, P.J.; Girvin, A.T.; Crosskey, M.; Zhou, A.G.; et al. Long COVID risk and pre-COVID vaccination in an EHR-based cohort study from the RECOVER program. Nat. Commun. 2023, 14, 2914. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Morales, A.J.; Lopez-Echeverri, M.C.; Perez-Raga, M.F.; Quintero-Romero, V.; Valencia-Gallego, V.; Galindo-Herrera, N.; López-Alzate, S.; Sánchez-Vinasco, J.D.; Gutiérrez-Vargas, J.J.; Mayta-Tristan, P.; et al. The global challenges of the long COVID-19 in adults and children. Travel Med. Infect. Dis. 2023, 54, 102606. [Google Scholar] [CrossRef]
- Azambuja, P.; Bastos, L.S.L.; Batista-da-Silva, A.A.; Ramos, G.V.; Kurtz, P.; Dias, C.M.C.; da Silva, E.P.; Arouca, L.E.; Soares, J.; Sejvar, J.J.; et al. Prevalence, risk factors, and impact of long COVID in a socially vulnerable community in Brazil: A prospective cohort study. Lancet Reg. Health 2024, 37, 100839. [Google Scholar] [CrossRef] [PubMed]
- Català, M.; Mercadé-Besora, N.; Kolde, R.; Trinh, N.T.H.; Roel, E.; Burn, E.; Rathod-Mistry, T.; Kostka, K.; Yi Man, W.; Delmestri, A.; et al. The effectiveness of COVID-19 vaccines to prevent long COVID symptoms: Staggered cohort study of data from the UK, Spain, and Estonia. Lancet Respir. Med. 2024, 12, 225–236. [Google Scholar] [CrossRef]
- Iba, A.; Hosozawa, M.; Hori, M.; Muto, Y.; Kihara, T.; Muraki, I.; Masuda, R.; Tamiya, N.; Iso, H. Booster vaccination and post COVID-19 condition during the Omicron variant-dominant wave: A large population-based study. Clin. Microbiol. Infect. 2024, 31, 630–635. [Google Scholar] [CrossRef]
- Camporesi, A.; Morello, R.; La Rocca, A.; Zampino, G.; Vezzulli, F.; Munblit, D.; Raffaelli, F.; Valentini, P.; Buonsenso, D. Characteristics and predictors of Long Covid in children: A 3-year prospective cohort study. EClinicalMedicine 2024, 76, 102815. [Google Scholar] [CrossRef]
- Wu, Q.; Zhang, B.; Tong, J.; Bailey, L.C.; Bunnell, H.T.; Chen, J.; Chrischilles, E.A.; Christakis, D.A.; Downs, S.M.; Hirabayashi, K.; et al. Real-world effectiveness and causal mediation study of BNT162b2 on long COVID risks in children and adolescents. EClinicalMedicine 2025, 79, 102962. [Google Scholar] [CrossRef]
- Mercadé-Besora, N.; Li, X.; Kolde, R.; Trinh, N.T.; Sanchez-Santos, M.T.; Man, W.Y.; Roel, E.; Reyes, C.; Delmestri, A.; E Nordeng, H.M.; et al. The role of COVID-19 vaccines in preventing post-COVID-19 thromboembolic and cardiovascular complications Cardiac risk factors and prevention. Heart 2024, 110, 635–643. [Google Scholar] [CrossRef]
- Guzman-Esquivel, J.; Mendoza-Hernandez, M.A.; Guzman-Solorzano, H.P.; Sarmiento-Hernandez, K.A.; Rodriguez-Sanchez, I.P.; Martinez-Fierro, M.L.; Paz-Michel, B.A.; Murillo-Zamora, E.; Rojas-Larios, F.; Lugo-Trampe, A.; et al. Clinical Characteristics in the Acute Phase of COVID-19 That Predict Long COVID: Tachycardia, Myalgias, Severity, and Use of Antibiotics as Main Risk Factors, While Education and Blood Group B Are Protective. Healthcare 2023, 11, 197. [Google Scholar] [CrossRef] [PubMed]
- Flores-Lastra, N.; Rivadeneira-Dueñas, J.; Fuenmayor-González, L.; Guayasamín-Tipanta, G.; Jácome-García, M.; Otzen, T.; Manterola, C. Safety Profile of Homologous and Heterologous Booster COVID-19 Vaccines in Physicians in Quito-Ecuador: A Cross-Sectional Study. Vaccines 2023, 11, 676. [Google Scholar] [CrossRef] [PubMed]
- Faksova, K.; Walsh, D.; Jiang, Y.; Griffin, J.; Phillips, A.; Gentile, A.; Kwong, J.; Macartney, K.; Naus, M.; Grange, Z.; et al. COVID-19 vaccines and adverse events of special interest: A multinational Global Vaccine Data Network (GVDN) cohort study of 99 million vaccinated individuals. Vaccine 2024, 42, 2200–2211. [Google Scholar] [CrossRef]
- Yaamika, H.; Muralidas, D.; Elumalai, K. Review of adverse events associated with COVID-19 vaccines, highlighting their frequencies and reported cases. J. Taibah. Univ. Med. Sci. 2023, 18, 1646–1661. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country | Design | Number of Participants | Methodological Quality | |
|---|---|---|---|---|---|
| Sex n, (%) | Age, Years | ||||
| Angarita-Fonseca, 2023 [6] | Latin-America | Cross-sectional study | Men: 840 (34.1); Women:1626 (65.9) | Mean (SD): 39.5 (53.3) | Inadequate or Low |
| Berry, 2023 [23] | Bonaire | Retrospective cohort study | Men: 10 (21.2); Women: 37 (78.8) | Median (range): 47 (14–89) | Adequate or High |
| Marra, 2023 [22] | Brazil | Case–control study | Men: 1950 (27.6); Women: 5101 (72.4) | Mean (SD): General: 37.5 (NR) Cases: 38.1 (8.7); Controls: 37.2 (9.0) | Inadequate or Low |
| Neves, 2023 [21] | Brazil | Prospective cohort study | Men: 338 (56.1); Women: 264 (43.9) | Mean (SD): 51 (12) | Adequate or High |
| Nuñez, 2023 [7] | Mexico | Prospective cohort study | Men: 126 (65.6); Women: 66 (34.4) | Median (range): 53 (45–64) | Inadequate or Low |
| Batista, 2024 [25] | Brazil | Cross-sectional study | Men: 59 (11.9); Women: 437 (88.1) | NR | Inadequate or Low |
| Del Carpio-Orantes, 2024 [24] | Mexico | Cross-sectional study | Men: 65 (32,0); Women: 138 (68,0%) | Mean (SD): 41.8 (11.3) | Inadequate or Low |
| Fuller, 2024 [26] | Brazil | Prospective cohort study | Men: 88 (31.8); Women: 188 (68.2) | Median (range): 45 (18–88) | Adequate or High |
| Author, Year | “Fully Vaccinated” Status | Vaccine Type | Long COVID Definition | Efficacy Measures |
|---|---|---|---|---|
| Angarita-Fonseca, 2023 [6] | Two doses | NR | Individuals with a history of probable or confirmed SARS-CoV-2 infection, usually 3 months from the onset of COVID-19 with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis. | Outcome: Risk of development of long COVID. Multivariable logistic regression. 1 dose: OR: 0.82; 95% CI 0.6–1.1 2 doses: OR: 0.75; 95% CI 0.6–0.9 3 or more doses: OR: 0.81; 95% CI 0.6–1.0. |
| Berry, 2023 [23] | At least one dose of the Pfizer vaccine at least 8 weeks after SARS-CoV-2 infection | mRNA: 36, Unvaccinated: 11 | Individuals with a laboratory-confirmed SARS-CoV-2 positive test result, for whom at least one symptom self-attributed to the experienced SARS-CoV-2 infection lasted longer than four weeks. | Outcome: Self-reported change in symptom severity. Multiple covariate adjusted linear regression model. Regression coefficients and 95% CI: Cough: −0.36; 95% CI −1.11–0.39; Heart palpitations: 0.60; 95% CI 0.18–1.02 |
| Marra, 2023 [22] | Analysis were performed whether 1, 2, 3, or 4 doses were administered. | Inactivated virus= 3259; Viral vector= 3255; mRNA = 148 | Signs and symptoms that developed during or following a SARS-CoV-2 RT-PCR confirmed infection, continued for >4 weeks, and could not explained by an alternative diagnosis. | Outcome: Risk of development of long COVID. Logistic Regression multivariable analysis. 0 vs. 1 doses: OR:0.91; 95%CI: 0.60–1.39; 0 vs. 2 doses: OR: 1.17; 95%CI: 0.79–1.76; 0 vs. 3 doses: OR: 0.63; 95%CI: 0.39–1.02; 0 vs. 4 doses: OR: 0.05; 95%CI: 0.01–0.19. |
| Neves, 2023 [21] | Two doses | Homologous regimens: Inactivated Whole-virion vaccine: 189; mRNA vaccine: 24; Viral-vector vaccine:96 | Physical complaints newly developed during or after the acute phase, persisting for >12 weeks, and not explained by an alternative diagnosis. | Outcome: risk of long COVID. HR: 0.89; 95% CI: 0.57–1.41 |
| Nuñez, 2023 [7] | At least one dose of any SARS-CoV-2 vaccine at least 14 days before the date on which symptoms of acute infection began | NR | Patients experiencing any symptoms not present before acute COVID-19 onset, and that persisted for longer than 90 days after acute COVID-19 onset. | Outcome: probability to experience a shorter time to long COVID resolution. HR: 3.16; 95%CI 1.21–8.26 |
| Batista, 2024 [25] | NR | NR | Symptoms that remain or appear for the first time within three months of SARS-CoV-2 infection. | NR |
| Del Carpio-Orantes, 2024 [24] | One dose or more | NR | Persistence of COVID-19 symptoms four weeks after the acute episode. | Outcome: probability to experience: Neurological symptoms: OR: 3.768 (CI 0.684–20.766); Cardiac symptoms: OR: 0.213 (CI 0.028–1.640); Pulmonary symptoms: OR: 1.649 (CI 0.645–1.640); Gastrointestinal symptoms: OR: 0.391 (CI 0.087–1.753); Musculoskeletal symptoms: OR: 0.422 (CI 0.138–1.286) |
| Fuller, 2024 [26] | Two or more doses | NR | Symptoms that began within three months of the positive SARS-CoV-2 test. | Outcome: Persistence of Long COVID in not fully vaccinated people. HR: 1·96, 95 % CI: 1·03–3·7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zambrano-Sánchez, G.; Rivadeneira, J.; Manterola, C.; Otzen, T.; Fuenmayor-González, L. Immunization as Protection Against Long COVID in the Americas: A Scoping Review. Vaccines 2025, 13, 822. https://doi.org/10.3390/vaccines13080822
Zambrano-Sánchez G, Rivadeneira J, Manterola C, Otzen T, Fuenmayor-González L. Immunization as Protection Against Long COVID in the Americas: A Scoping Review. Vaccines. 2025; 13(8):822. https://doi.org/10.3390/vaccines13080822
Chicago/Turabian StyleZambrano-Sánchez, Gabriela, Josue Rivadeneira, Carlos Manterola, Tamara Otzen, and Luis Fuenmayor-González. 2025. "Immunization as Protection Against Long COVID in the Americas: A Scoping Review" Vaccines 13, no. 8: 822. https://doi.org/10.3390/vaccines13080822
APA StyleZambrano-Sánchez, G., Rivadeneira, J., Manterola, C., Otzen, T., & Fuenmayor-González, L. (2025). Immunization as Protection Against Long COVID in the Americas: A Scoping Review. Vaccines, 13(8), 822. https://doi.org/10.3390/vaccines13080822