
Thyroid Eye Disease as Initial Manifestation of Graves’ Disease Following Viral Vector SARS-CoV-2 Vaccine: Report of a Case and Review of the Literature

 ,
,  and
and
Abstract
:1. Introduction
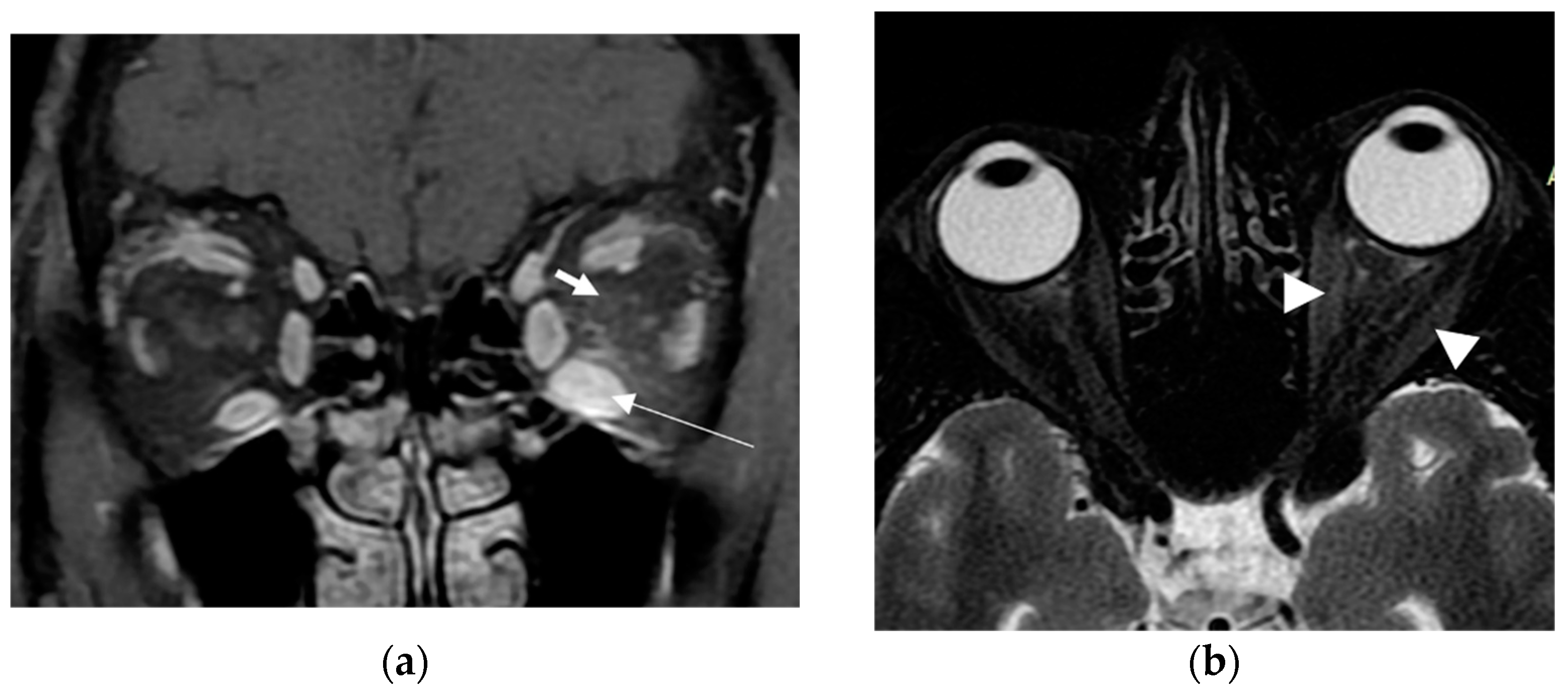
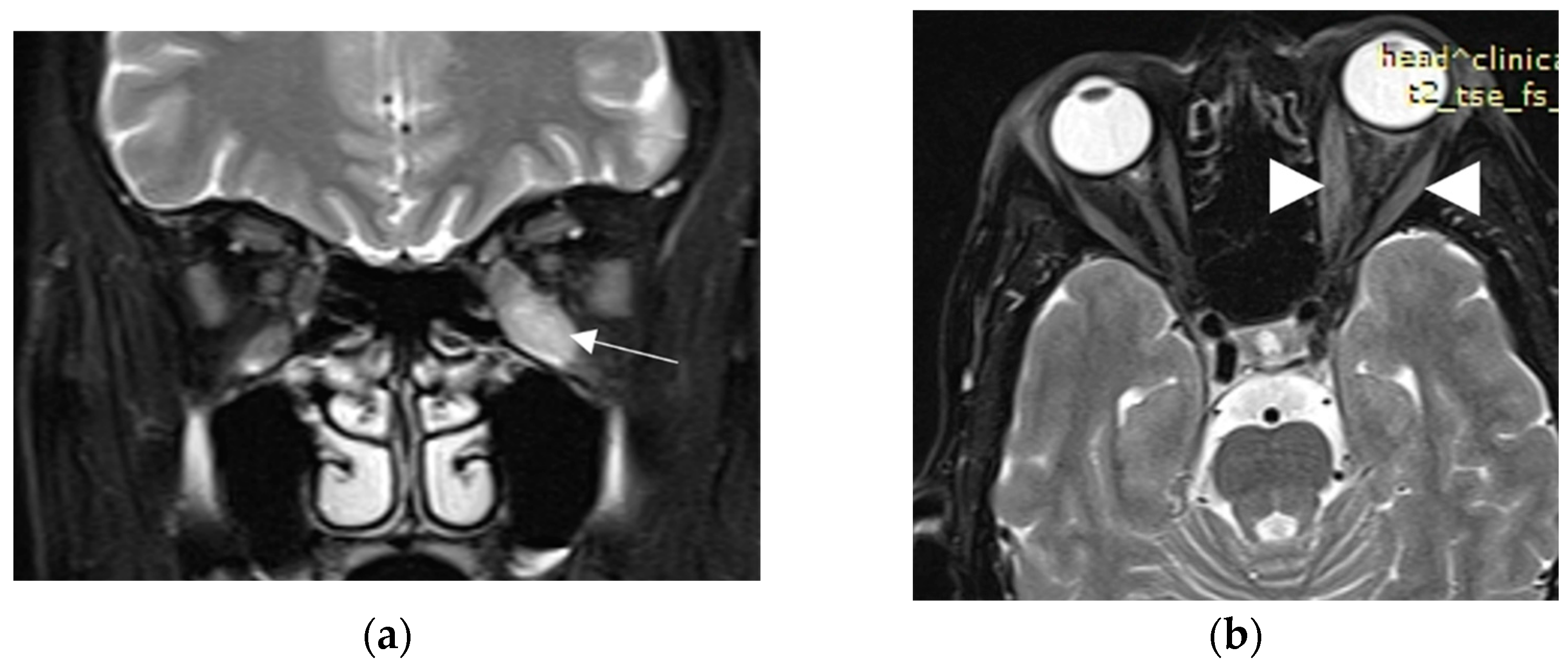
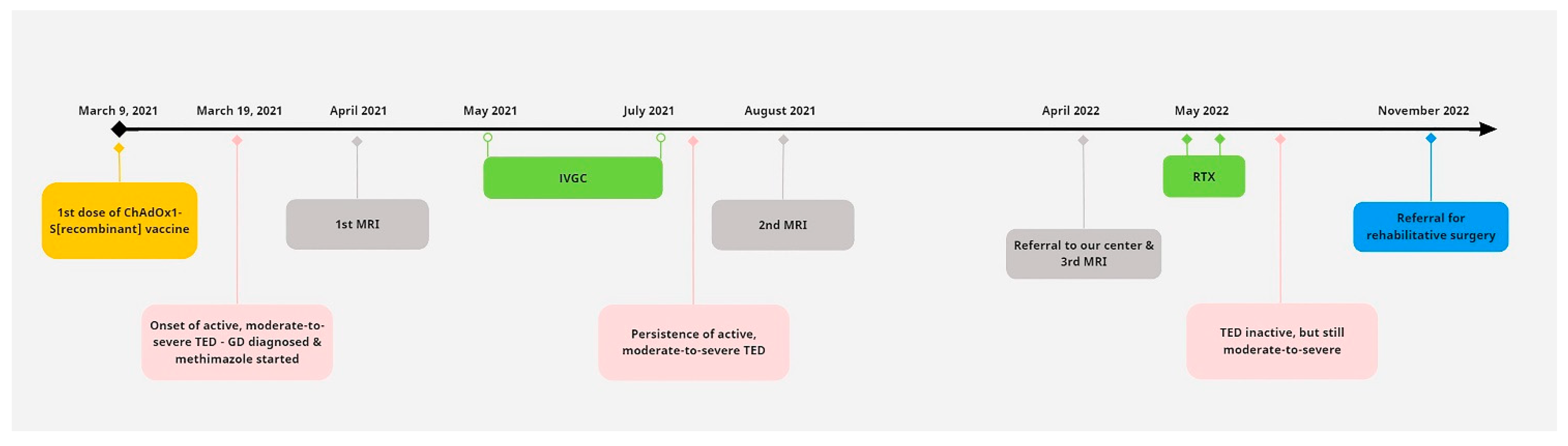
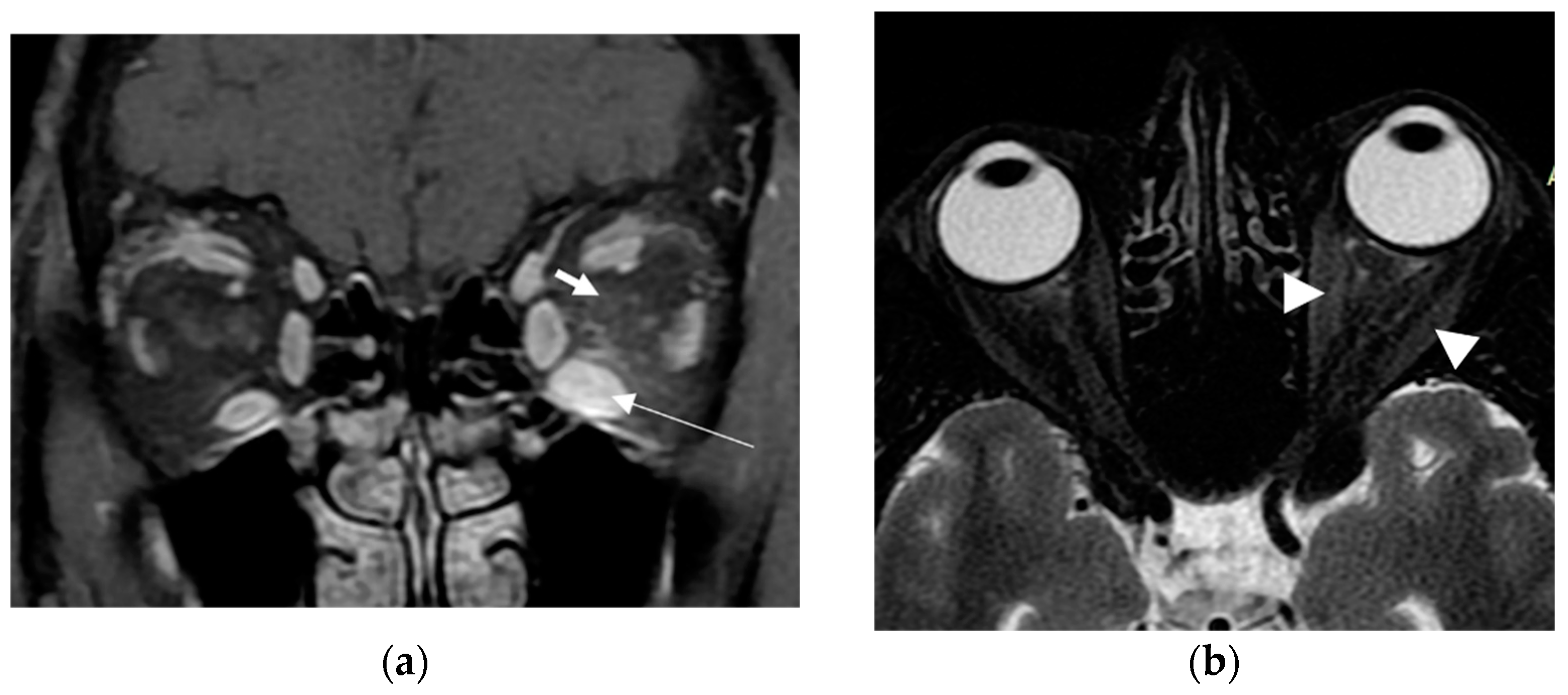
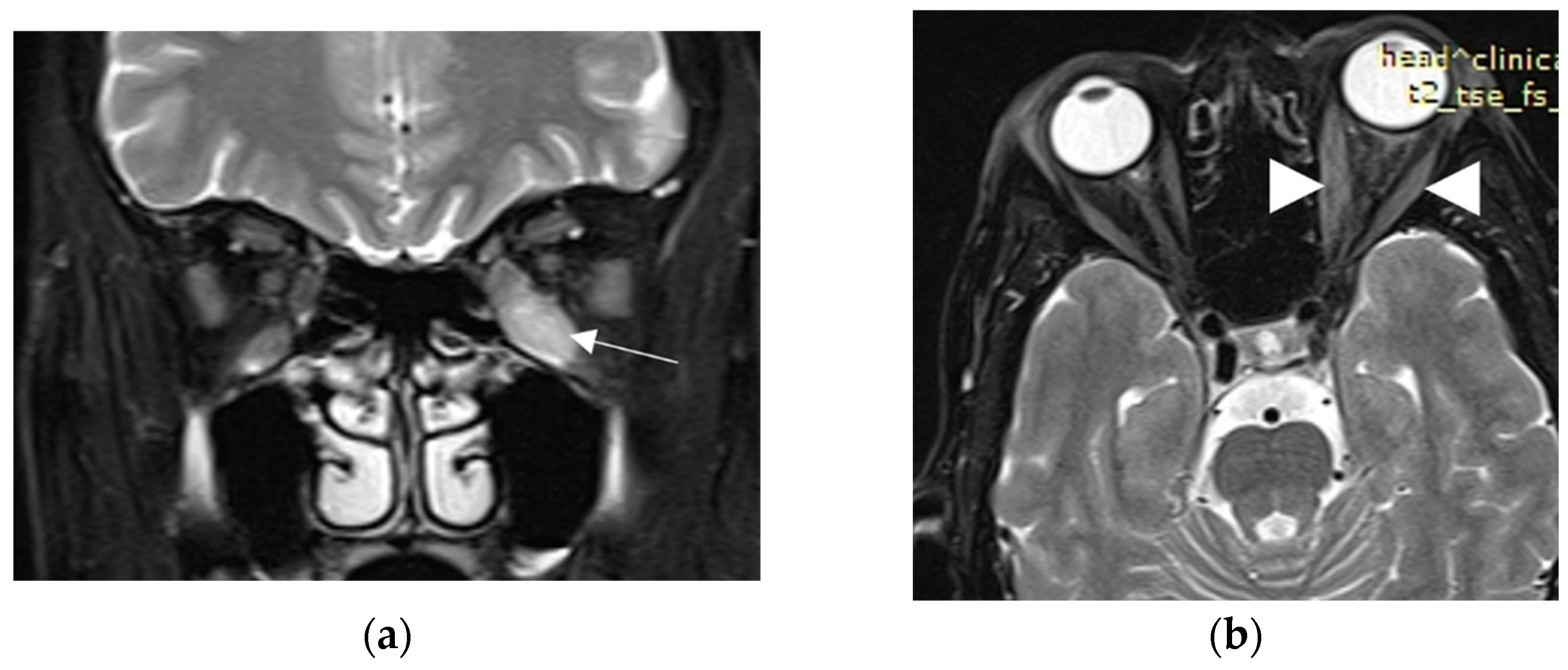
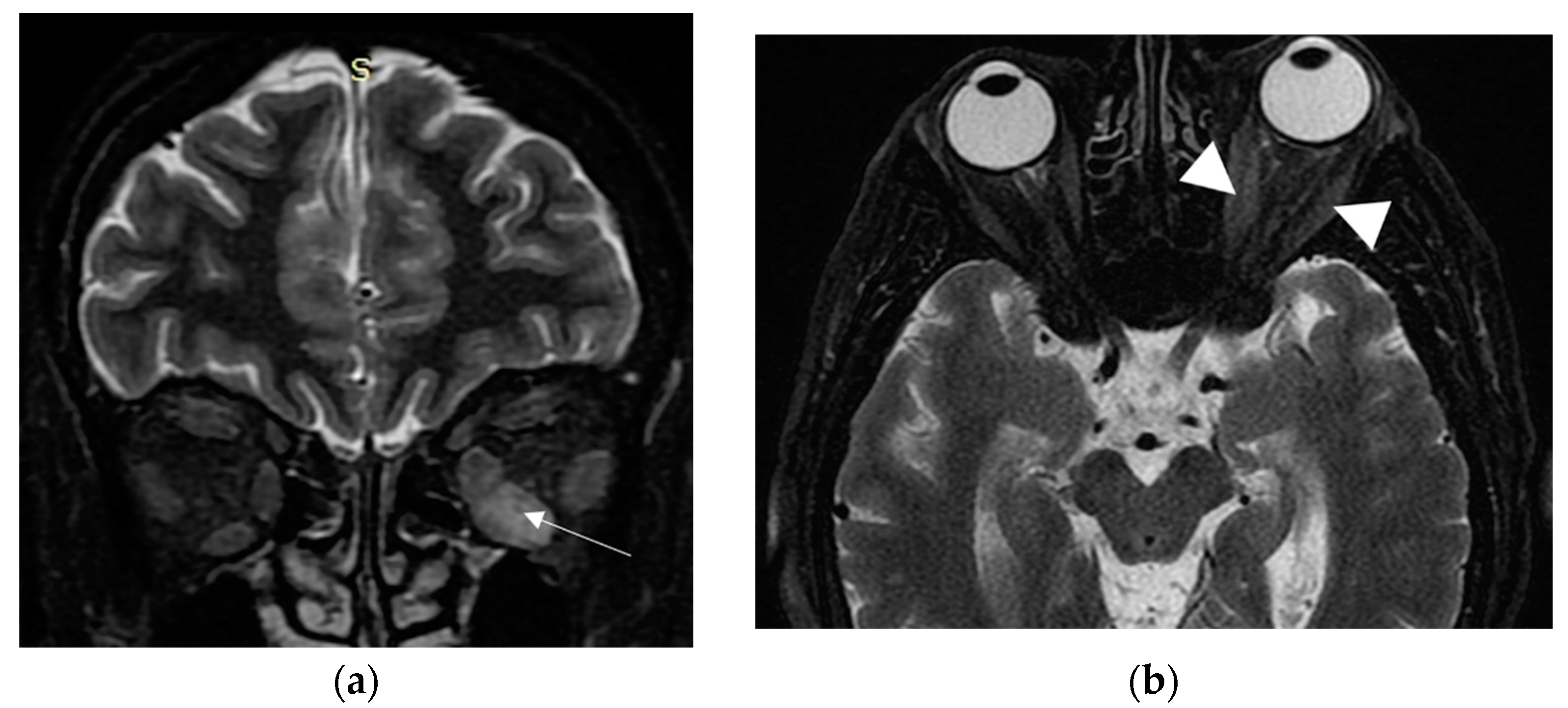
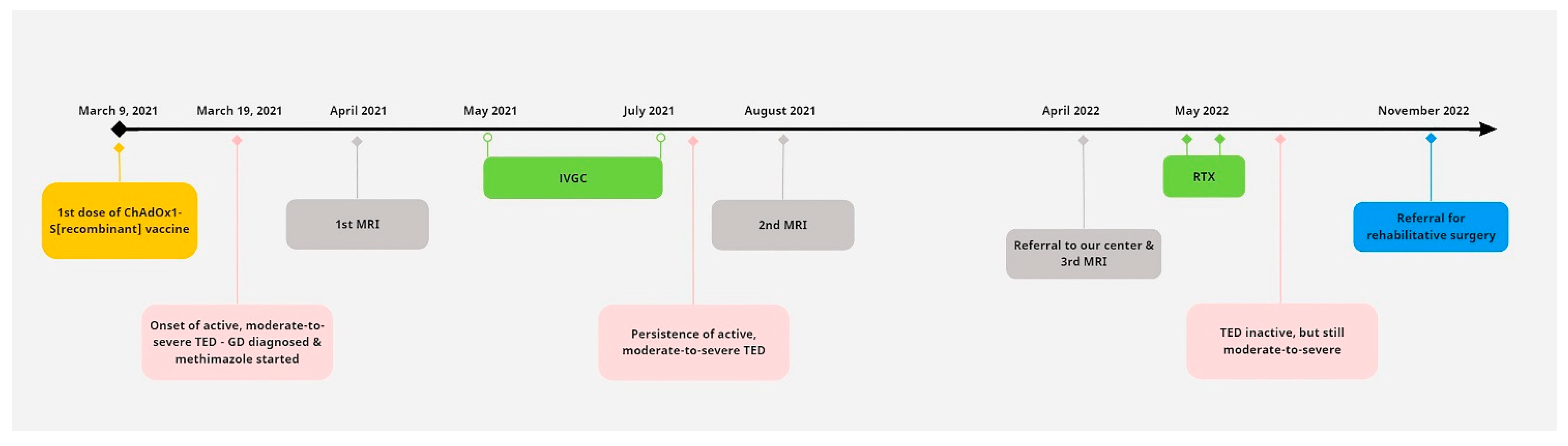
2. Case Presentation
3. Review of the Literature
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, J.M. Novel statistics predict the COVID-19 pandemic could terminate in 2022. J. Med. Virol. 2022, 94, 2845–2848. [Google Scholar] [CrossRef] [PubMed]
- Mushtaq, H.A.; Khedr, A.; Koritala, T.; Bartlett, B.N.; Jain, N.K.; Khan, S.A. A review of adverse effects of COVID-19 vaccines. Infez. Med. 2022, 30, 320. [Google Scholar] [CrossRef]
- Kim, M.A.; Lee, Y.W.; Kim, S.R.; Kim, J.H.; Min, T.K.; Park, H.S.; Shin, M.; Ye, Y.M.; Lee, S.; Lee, J.; et al. COVID-19 vaccine-associated anaphylaxis and allergic reactions: Consensus statements of the KAAACI Urticaria/Angioedema/Anaphylaxis Working Group. Allergy Asthma Immunol. Res. 2021, 13, 526. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, M.I.; Pimenta, I.; Conde, I.; Gonzalez, F.A. Vaccine-induced immune thrombocytopaenia and thrombosis (VITT) after COVID-19 vaccination. BMJ Case Rep. 2022, 15, e247346. [Google Scholar] [CrossRef] [PubMed]
- Voleti, N.; Reddy, S.P.; Ssentongo, P. Myocarditis in SARS-CoV-2 infection vs. COVID-19 vaccination: A systematic review and meta-analysis. Front. Cardiovasc. Med. 2022, 9, 951314. [Google Scholar] [CrossRef] [PubMed]
- Jafarzadeh, A.; Nemati, M.; Jafarzadeh, S.; Nozari, P.; Mortazavi, S.M.J. Thyroid dysfunction following vaccination with COVID-19 vaccines: A basic review of the preliminary evidence. J. Endocrinol. Investig. 2022, 45, 1835–1863. [Google Scholar] [CrossRef] [PubMed]
- Abeillon-du Payrat, J.; Grunenwald, S.; Gall, E.; Ladsous, M.; Raingeard, I.; Caron, P. Graves’ orbitopathy post-SARS-CoV-2 vaccines: Report on six patients. J. Endocrinol. Investig. 2023, 46, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Rubinstein, T.J. Thyroid Eye Disease Following COVID-19 Vaccine in a Patient With a History Graves’ Disease: A Case Report. Ophthalmic Plast. Reconstr. Surg. 2021, 37, e221–e223. [Google Scholar] [CrossRef] [PubMed]
- Patrizio, A.; Ferrari, S.M.; Antonelli, A.; Fallahi, P. Worsening of Graves’ ophthalmopathy after SARS-CoV-2 mRNA vaccination. Autoimmun. Rev. 2022, 21, 103096. [Google Scholar] [CrossRef]
- Chaudhary, S.; Dogra, V.; Walia, R. Four cases of Graves’ disease following viral vector severe acute respiratory syndrome corona virus-2 (SARS-CoV-2) vaccine. Endocr. J. 2022, 69, 1431–1435. [Google Scholar] [CrossRef]
- Taylor, P.N.; Albrecht, D.; Scholz, A.; Gutierrez-Buey, G.; Lazarus, J.H.; Dayan, C.M.; Okosieme, O.E. Global epidemiology of hyperthyroidism and hypothyroidism. Nat. Rev. Endocrinol. 2018, 14, 301–316. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.J.; Hegedüs, L. Graves’ disease. N. Engl. J. Med. 2016, 375, 1552–1565. [Google Scholar] [CrossRef] [PubMed]
- Burch, H.B.; Perros, P.; Bednarczuk, T.; Cooper, D.S.; Dolman, P.J.; Leung, A.M.; Stan, M.N. Management of thyroid eye disease: A Consensus Statement by the American Thyroid Association and the European Thyroid Association. Thyroid Off. J. Am. Thyroid Assoc. 2022, 32, 1439–1470. [Google Scholar] [CrossRef] [PubMed]
- Rundle, F.F. Management of exophthalmos and related ocular changes in Graves’ disease. Metabolism 1957, 6, 36–48. [Google Scholar] [PubMed]
- Anagnostis, P.; Boboridis, K.; Adamidou, F.; Kita, M. Natural course of mild Graves’ orbitopathy: Is it a chronic remitting or a transient disease? J. Endocrinol. Investig. 2017, 40, 257–261. [Google Scholar] [CrossRef]
- Bartalena, L.; Kahaly, G.J.; Baldeschi, L.; Dayan, C.M.; Eckstein, A.; Marcocci, C.; Marinò, M.; Vaidya, B.; Wiersinga, W.M.; EUGOGO. The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves’ orbitopathy. Eur. J. Endocrinol. 2021, 185, G43–G67. [Google Scholar] [CrossRef]
- Pierman, G.; Delgrange, E.; Jonas, C. Recurrence of Graves’ disease (a Th1-type cytokine disease) following SARS-CoV-2 mRNA vaccine administration: A simple coincidence? Eur. J. Case Rep. Intern. Med. 2021, 8, 002807. [Google Scholar] [CrossRef]
- Bostan, H.; Ucan, B.; Kizilgul, M.; Calapkulu, M.; Hepsen, S.; Gul, U.; Unsal, I.O.; Cakal, E. Relapsed and newly diagnosed Graves’ disease due to immunization against COVID-19: A case series and review of the literature. J. Autoimmun. 2022, 128, 102809. [Google Scholar] [CrossRef]
- Goblirsch, T.J.; Paulson, A.E.; Tashko, G.; Mekonnen, A.J. Graves’ disease following administration of second dose of SARS-CoV-2 vaccine. BMJ Case Rep. CP 2021, 14, e246432. [Google Scholar] [CrossRef]
- Kikkawa, D.; Park, K.; Fung, S.; Ting, M.; Ozzello, D.; Yoon, J.; Liu, C.; Korn, B. Thyroid eye disease reactivation associated with COVID-19 vaccination. Taiwan J. Ophthalmol. 2022, 12, 93–96. [Google Scholar] [CrossRef]
- Chee, Y.J.; Liew, H.; Hoi, W.H.; Lee, Y.; Lim, B.; Chin, H.X.; Dalan, R. SARS-CoV-2 mRNA vaccination and Graves’ disease: A report of 12 cases and review of the literature. J. Clin. Endocrinol. Metab. 2022, 107, e2324–e2330. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, A.; Tzoulis, P.; Kossler, A.L.; Dosiou, C. New onset or deterioration of thyroid eye disease after mRNA SARS-CoV-2 vaccines: Report of 2 cases and literature review. J. Clin. Endocrinol. Metab. 2023, 108, 979–985. [Google Scholar] [CrossRef] [PubMed]
- Cheng, O.T.; Schlachter, D.M. Teprotumumab in advanced reactivated thyroid eye disease. Am. J. Ophthalmol. Case Rep. 2022, 26, 101484. [Google Scholar] [CrossRef] [PubMed]
- Barrett, L.; Glatt, H.J.; Burde, R.M.; Gado, M.H. Optic nerve dysfunction in thyroid eye disease: CT. Radiology 1988, 167, 503–507. [Google Scholar] [CrossRef]
- Draman, M.S.; Zhang, L.; Dayan, C.; Ludgate, M. Orbital signaling in Graves’ orbitopathy. Front. Endocrinol. 2021, 12, 739994. [Google Scholar] [CrossRef]
- Weetman, A.P. The Immunopathogenesis of Chronic Autoimmune Thyroiditis One Century after Hashimoto. Eur. Thyroid. J. 2013, 1, 243–250. [Google Scholar] [CrossRef]
- Bliddal, S.; Nielsen, C.H.; Feldt-Rasmussen, U. Recent advances in understanding autoimmune thyroid disease: The tallest tree in the forest of polyautoimmunity. F1000Research 2017, 6, 1776. [Google Scholar] [CrossRef]
- Kendler, D.L.; Lippa, J.; Rootman, J. The Initial Clinical Characteristics of Graves’ Orbitopathy Vary With Age and Sex. Arch. Ophthalmol. Chic Ill 1993, 111, 197–201. [Google Scholar] [CrossRef]
- Stan, M.N.; Bahn, R.S.; Perros, P.; Tumminia, A.; Frittitta, L.; Buscema, M.; Palermo, F.; Sciacca, L.; Squatrito, S.; McAlinden, C.; et al. Risk Factors for Development or Deterioration of Graves’ Ophthalmopathy. Thyroid Off. J. Am. Thyroid Assoc. 2010, 20, 777–783. [Google Scholar] [CrossRef]
- Traisk, F.; Tallstedt, L.; Abraham-Nordling, M.; Andersson, T.; Berg, G.; Calissendorff, J.; Thyroid Study Group of TT 96. Thyroid-associated ophthalmopathy after treatment for Graves’ hyperthyroidism with antithyroid drugs or iodine-131. J. Clin. Endocrinol. Metab. 2009, 94, 3700–3707. [Google Scholar] [CrossRef]
- Vestergaard, P. Smoking and thyroid disorders--a meta-analysis. Eur. J. Endocrinol. 2002, 146, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.Z.; Huang, S.S.; Liu, J.; Lu, B.; Shao, J.Q. High serum cholesterol: A novel risk factor for thyroid associated ophthalmopathy? Zhonghua Nei Ke Za Zhi 2019, 58, 823–825. [Google Scholar]
- Antonelli, A.; Ferrari, S.M.; Ragusa, F.; Elia, G.; Paparo, S.R.; Ruffilli, I.; Patrizio, A.; Giusti, C.; Gonnella, D.; Cristaudo, A.; et al. Graves’ disease: Epidemiology, genetic and environmental risk factors and viruses. Best Pract. Res. Clin. Endocrinol. Metab. 2020, 34, 101387. [Google Scholar] [CrossRef] [PubMed]
- Vojdani, A.; Kharrazian, D. Potential antigenic cross-reactivity between SARS-CoV-2 and human tissue with a possible link to an increase in autoimmune diseases. Clin. Immunol. 2020, 217, 108480. Available online: https://pubmed.ncbi.nlm.nih.gov/32461193/ (accessed on 27 July 2023). [CrossRef] [PubMed]
- Shoenfeld, Y.; Agmon-Levin, N. ‘ASIA’–autoimmune/inflammatory syndrome induced by adjuvants. J. Autoimmun. 2011, 36, 4–8. [Google Scholar] [CrossRef]
- Patrizio, A.; Ferrari, S.M.; Elia, G.; Ragusa, F.; Paparo, S.R.; Mazzi, V.; Fallahi, P. Graves’ disease following SARS-CoV-2 vaccination: A systematic review. Vaccines 2022, 10, 1445. [Google Scholar] [CrossRef]
- Teijaro, J.R.; Farber, D.L. COVID-19 vaccines: Modes of immune activation and future challenges. Nat. Rev. Immunol. 2021, 21, 195–197. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | Age | Family History of Autoimmunity | Personal History of Autoimmunity | Name of Vaccine | Type of Vaccine | Dose | Time of TED Onset after Vaccination (Days) | History of TED | Thyrotoxicosis | CAS | Severity of TED | Reference |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | 34 | ND | ND | Pfizer | mRNA | 1st | 10 | New | Yes | ND | Mild | [17] |
| F | 50 | ND | ND | Pfizer | mRNA | 2nd | 3 | New | No | 5/7 | Moderate-to-severe | [8] |
| F | 51 | ND | No | Pfizer | mRNA | 2nd | 4 | New | Yes | 3/7 | Mild GO | [18] |
| F | 71 | ND | No | Pfizer | mRNA | 2nd | >70 | New | Yes | ND | Moderate-to-severe / 10 weeks after treatment of Graves’ disease | [19] |
| M | 43 | ND | ND | Pfizer | mRNA | ND | 14 | TED recurrence | No | ND | Sight threatening | [9] |
| F | 58 | ND | ND | Pfizer | mRNA | 2nd | 3 | Worsening of 3-year TED | No | 6/10 | Moderate-to-severe | [9] |
| F | 53 | ND | ND | Pfizer | mRNA | 1st | 1 | New | No | ND | Moderate-to-severe | [20] |
| F | 66 | ND | ND | Moderna | mRNA | 2nd | 21 | TED recurrence after 15 years | No | 6/10 | Moderate-to-severe | [20] |
| F | 37 | ND | ND | ND | mRNA | 2nd | 21 | New | Yes | ND | Mild-to-moderate | [21] |
| F | 45 | ND | ND | Moderna | mRNA | 1st | 21 | TED recurrence after 5 years | ND | ND | Mild-to-moderate | [20] |
| M | 59 | ND | ND | ND | mRNA | 1st | 21 | New | Yes | ND | Mild-to-moderate | [21] |
| F | 34 | ND | ND | ND | mRNA | 1st | 26 | New | Yes | ND | Mild-to-moderate | [21] |
| F | 70 | ND | Graves’ disease (total thyroidectomy) | ND | mRNA | 2nd | 6 | TED recurrence after 18 weeks | No | 4/7 | Moderate-to-severe | [7] |
| M | 43 | ND | Type-1 diabetes mellitus, psoriasis, Graves’ disease | Moderna | mRNA | 1st | 1 | TED recurrence after 45 weeks | No | 7/7 | Sight threatening | [7] |
| M | 73 | ND | Graves’ disease | Pfizer | mRNA | 1st | 21 | New | No | 3/7 | Mild | [7] |
| F | 45 | ND | Graves’ disease (total thyroidectomy) | Moderna | mRNA | 2nd | 7 | TED recurrence | No | 4/7 | Moderate-to-severe | [7] |
| M | 48 | ND | Graves’ disease (total thyroidectomy) | Moderna | mRNA | 2nd | 30 | TED recurrence after 11 months | Yes | 5/7 | Sight threatening | [7] |
| F | 39 | Thyroid disease | ND | Pfizer | mRNA | 1st | 7 | New | No | 2/7 | Mild | [7] |
| M | 20 | No | No | COVISHIELD | viral vector | 1st | 14 | New | Yes | 2/7 | Mild | [10] |
| F | 46 | Hypothyroidism | No | COVISHIELD | viral vector | 1st | 10 | New | Yes | 2/7 | Mild | [10] |
| M | 50 | ND | Psoriasis, vitiligo, atrophic gastritis, Graves’ disease | Pfizer | mRNA | 2nd | 21 | Worsening of 9-months TED | No | 7/10 | Moderate-to-severe | [22] |
| F | 71 | ND | Hypothyroidism | Moderna | mRNA | 2nd | 3 | New | Yes | 4/7 | Sight threatening | [22] |
| F | 51 | ND | Graves’ disease | Moderna | mRNA | 2nd | 15 | TED recurrence after 30 weeks | No | 9/10 | Severe | [23] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Armeni, A.K.; Markantes, G.Κ.; Stathopoulou, A.; Saltiki, K.; Zampakis, P.; Assimakopoulos, S.F.; Michalaki, M.A. Thyroid Eye Disease as Initial Manifestation of Graves’ Disease Following Viral Vector SARS-CoV-2 Vaccine: Report of a Case and Review of the Literature. Vaccines 2023, 11, 1574. https://doi.org/10.3390/vaccines11101574
Armeni AK, Markantes GΚ, Stathopoulou A, Saltiki K, Zampakis P, Assimakopoulos SF, Michalaki MA. Thyroid Eye Disease as Initial Manifestation of Graves’ Disease Following Viral Vector SARS-CoV-2 Vaccine: Report of a Case and Review of the Literature. Vaccines. 2023; 11(10):1574. https://doi.org/10.3390/vaccines11101574
Chicago/Turabian StyleArmeni, Anastasia K., Georgios Κ. Markantes, Alexandra Stathopoulou, Katerina Saltiki, Petros Zampakis, Stelios F. Assimakopoulos, and Marina A. Michalaki. 2023. "Thyroid Eye Disease as Initial Manifestation of Graves’ Disease Following Viral Vector SARS-CoV-2 Vaccine: Report of a Case and Review of the Literature" Vaccines 11, no. 10: 1574. https://doi.org/10.3390/vaccines11101574
APA StyleArmeni, A. K., Markantes, G. Κ., Stathopoulou, A., Saltiki, K., Zampakis, P., Assimakopoulos, S. F., & Michalaki, M. A. (2023). Thyroid Eye Disease as Initial Manifestation of Graves’ Disease Following Viral Vector SARS-CoV-2 Vaccine: Report of a Case and Review of the Literature. Vaccines, 11(10), 1574. https://doi.org/10.3390/vaccines11101574