
A Large Cluster of New Onset Autoimmune Myositis in the Yorkshire Region Following SARS-CoV-2 Vaccination

 ,
,
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Ella, R.; Vadrevu, K.M.; Jogdand, H.; Prasad, S.; Reddy, S.; Sarangi, V.; Ganneru, B.; Sapkal, G.; Yadav, P.; Abraham, P.; et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBV152: A double-blind, randomised, phase 1 trial. Lancet Infect. Dis. 2021, 21, 637–646. [Google Scholar] [CrossRef]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 2020, 396, 1979–1993. [Google Scholar] [CrossRef]
- Zhang, Y.J.; Zeng, G.; Pan, H.X.; Li, C.G.; Hu, Y.L.; Chu, K.; Han, W.; Chen, Z.; Tang, R.; Yin, W.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18–59 years: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 181–192. [Google Scholar] [CrossRef]
- Pavord, S.; Scully, M.; Hunt, B.J.; Lester, W.; Bagot, C.; Craven, B.; Rampotas, A.; Ambler, G.; Makris, M. Clinical Features of Vaccine-Induced Immune Thrombocytopenia and Thrombosis. N. Engl. J. Med. 2021, 385, 1680–1689. [Google Scholar] [CrossRef]
- Kim, H.W.; Jenista, E.R.; Wendell, D.C.; Azevedo, C.F.; Campbell, M.J.; Darty, S.N.; Parker, M.A.; Kim, R.J. Patients with Acute Myocarditis following mRNA COVID-19 Vaccination. JAMA Cardiol. 2021, 6, 1196–1201. [Google Scholar] [CrossRef]
- McGonagle, D.; McDermott, M.F. A proposed classification of the immunological diseases. PLoS Med. 2006, 3, e297. [Google Scholar] [CrossRef] [Green Version]
- Tatematsu, M.; Funami, K.; Seya, T.; Matsumoto, M. Extracellular RNA Sensing by Pattern Recognition Receptors. J. Innate Immun. 2018, 10, 398–406. [Google Scholar] [CrossRef]
- Teijaro, J.R.; Farber, D.L. COVID-19 vaccines: Modes of immune activation and future challenges. Nat. Rev. Immunol. 2021, 21, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Krug, A. Nucleic acid recognition receptors in autoimmunity. In Handbook Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 2008; pp. 129–151. [Google Scholar]
- Rodero, M.P.; Crow, Y.J. Type I interferon-mediated monogenic autoinflammation: The type I interferonopathies, a conceptual overview. J. Exp. Med. 2016, 213, 2527–2538. [Google Scholar] [CrossRef] [PubMed]
- Heine, A.; Juranek, S.; Brossart, P. Clinical and immunological effects of mRNA vaccines in malignant diseases. Mol. Cancer 2021, 20, 52. [Google Scholar] [CrossRef]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D. The CARE guidelines: Consensus-based clinical case reporting guideline development. J. Med. Case Rep. 2013, 7, 223. [Google Scholar] [CrossRef] [Green Version]
- Miller, F.W.; Waite, K.A.; Biswas, T.; Plotz, P.H. The role of an autoantigen, histidyl-tRNA synthetase, in the induction and maintenance of autoimmunity. Proc. Natl. Acad. Sci. USA 1990, 87, 9933–9937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Manual on Surveillance of Adverse Events Following Immunization, 2016 Update ed.; World Health Organization: Geneva, Switzerland, 2014.
- Bellavite, P. Causality assessment of adverse events following immunization: The problem of multifactorial pathology. F1000Research 2020, 9, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.; Kang, H.Y.; Cho, S.; Park, S.; Kim, A.Y.; Jung, S.Y.; Seong, B.L.; Lee, Y.M. Causality Assessment Guidelines for Adverse Events Following Immunization with a Focus on Guillain-Barre Syndrome. Vaccines 2020, 8, 101. [Google Scholar] [CrossRef] [Green Version]
- Watad, A.; De Marco, G.; Mahajna, H.; Druyan, A.; Eltity, M.; Hijazi, N.; Haddad, A.; Elias, M.; Zisman, D.; Naffaa, M.E.; et al. Immune-Mediated Disease Flares or New-Onset Disease in 27 Subjects Following mRNA/DNA SARS-CoV-2 Vaccination. Vaccines 2021, 9, 435. [Google Scholar] [CrossRef]
- Meyer, A.; Meyer, N.; Schaeffer, M.; Gottenberg, J.E.; Geny, B.; Sibilia, J. Incidence and prevalence of inflammatory myopathies: A systematic review. Rheumatology 2015, 54, 50–63. [Google Scholar] [CrossRef] [Green Version]
- Lundberg, I.E.; Fujimoto, M.; Vencovsky, J.; Aggarwal, R.; Holmqvist, M.; Christopher-Stine, L.; Mammen, A.L.; Miller, F.W. Idiopathic inflammatory myopathies. Nat. Rev. Dis. Primers 2021, 7, 86. [Google Scholar] [CrossRef]
- Maramattom, B.V.; Philips, G.; Thomas, J.; Santhamma, S.G.N. Inflammatory myositis after ChAdOx1 vaccination. Lancet Rheumatol. 2021, 3, e747–e749. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, J.H.; Woo, C.G. Clinicopathological Characteristics of Inflammatory Myositis Induced by COVID-19 Vaccine (Pfizer-BioNTech BNT162b2): A Case Report. J. Korean Med. Sci. 2022, 37, e91. [Google Scholar] [CrossRef] [PubMed]
- Gouda, W.; Albasri, A.; Alsaqabi, F.; Al Sabah, H.Y.; Alkandari, M.; Abdelnaby, H.J. Dermatomyositis Following BNT162b2 mRNA COVID-19 Vaccination. Korean Med. Sci. 2022, 37, e32. [Google Scholar] [CrossRef] [PubMed]
- Lazzaro, S.; Giovani, C.; Mangiavacchi, S.; Magini, D.; Maione, D.; Baudner, B.; Geall, A.J.; De Gregorio, E.; D’Oro, U.; Buonsanti, C. CD8 T-cell priming upon mRNA vaccination is restricted to bone-marrow-derived antigen-presenting cells and may involve antigen transfer from myocytes. Immunology 2015, 146, 312–326. [Google Scholar] [CrossRef]
- Sheridan, C. First COVID-19 DNA vaccine approved, others in hot pursuit. Nat. Biotechnol. 2021, 39, 1479–1482. [Google Scholar] [CrossRef]
- Zhu, F.C.; Li, Y.H.; Guan, X.H.; Hou, L.H.; Wang, W.J.; Li, J.X.; Wu, S.P.; Wang, B.S.; Wang, Z.; Wang, L.; et al. Safety, tolerability, and immunogenicity of a recombinant adenovirus type-5 vectored COVID-19 vaccine: A dose-escalation, open-label, non-randomised, first-in-human trial. Lancet 2020, 395, 1845–1854. [Google Scholar] [CrossRef]
- Chavda, V.P.; Hossain, M.K.; Beladiya, J.; Apostolopoulos, V. Nucleic Acid Vaccines for COVID-19: A Paradigm Shift in the Vaccine Development Arena. Biologics 2021, 1, 337–356. [Google Scholar] [CrossRef]
- Kyriakidis, N.C.; López-Cortés, A.; González, E.V.; Grimaldos, A.B.; Prado, E.O. SARS-CoV-2 vaccines strategies: A comprehensive review of phase 3 candidates. npj Vaccines 2021, 6, 28. [Google Scholar] [CrossRef]
- Kurteva, E.; Vasilev, G.; Tumangelova-Yuzeir, K.; Ivanova, I.; Ivanova-Todorova, E.; Velikova, T.; Kyurkchiev, D. Interferon-gamma release assays outcomes in healthy subjects following BNT162b2 mRNA COVID-19 vaccination. Rheumatol. Int. 2022, 42, 449–456. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Centre Gender Age (in Years, at Myositis Onset) | Past Medical History for Autoimmunity | SARS-CoV-2 Vaccine. (Time between Exposure and Myositis Onset, in Weeks) | Details Related to Myositis Including Muscle Related Autoantigen (MRA) | Non-Muscular Manifestations (Complications, if Occurred) | Treatment |
|---|---|---|---|---|---|
| Case 1 | No | AZD1222/ChAdOx1 | Asthenia, dysphonia, impaired swallowing. CK 536 U/L and CRP 55 mg/L, no biopsy. Widespread quadriceps oedema on MRI ANA +, Myoblot positive (SAE-1) | Gottron’s papules; heliotrope rash; shawl’s sign (aspiration pneumonia) | IV, then oral steroid, IvIg Methotrexate and Hydroxychloroquine |
| York | Dose 2, May 2021 | ||||
| Female, 68 | (34 weeks) | ||||
| Case 2 | No | AZD1222/ChAdOx1 | Asthenia, impaired swallowing. CK > 7000 U/L and CRP 24 mg/L, no biopsy. widespread muscle oedema in thighs on MRI ANA + Myoblot positive (Mi2) | Gottron’s papules; heliotrope rash; shawl’s sign | As above |
| York | Dose 2, May 2021 | ||||
| Female, 68 | (25 weeks) | ||||
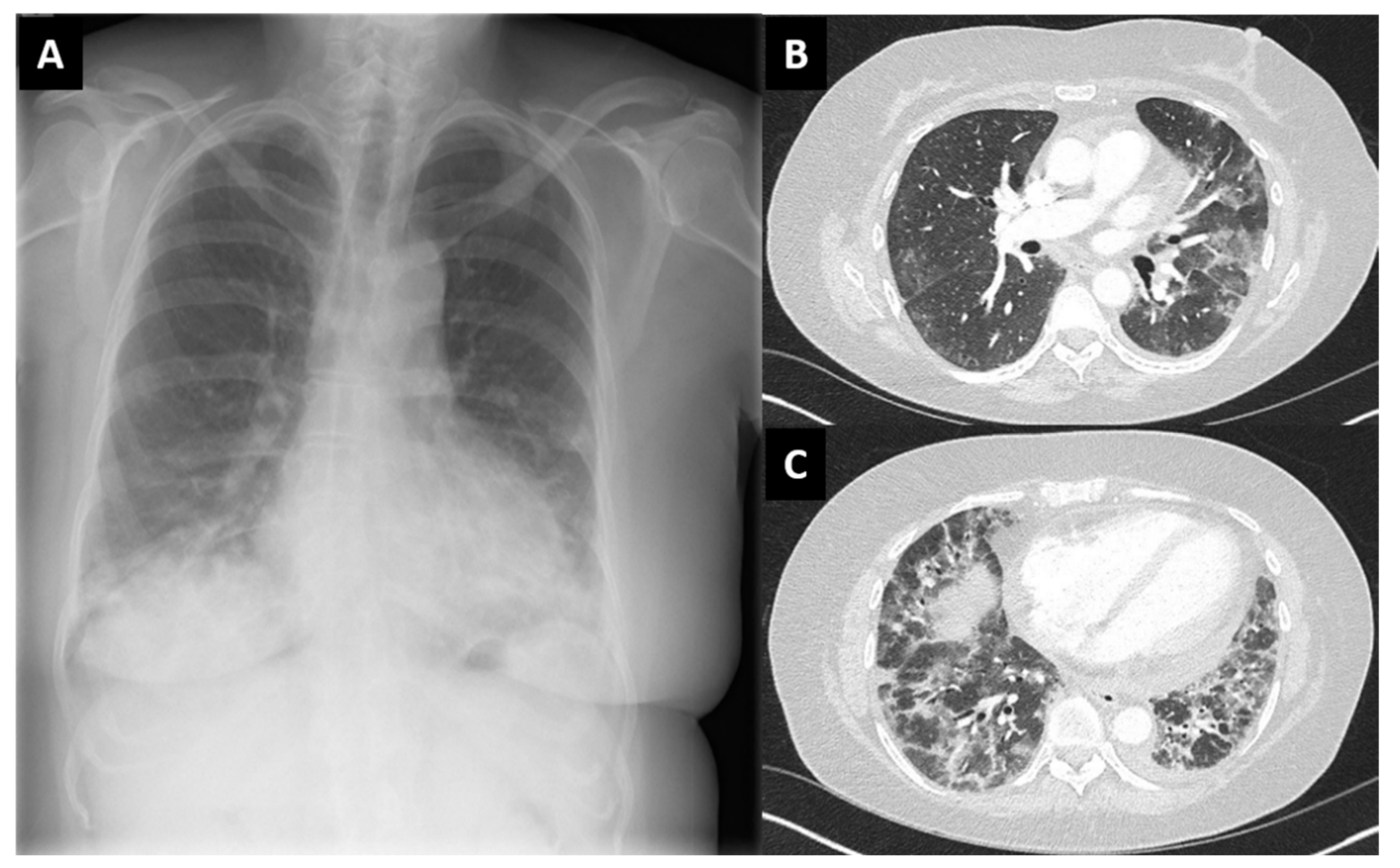
| Case 3 | No | AZD1222/ChAdOx1 | Amyopathic, sicca symptoms, shortness of breath. CRP 20 mg/L, CK normal. ANA + Myoblot + (SL 75, Ro52) | Heliotrope rash, mechanics hands. Interstitial lung disease. Pericardic effusion | Oral steroids, then IV cyclophosphamide followed by mycophenolate |
| York | dose 1, May 2021 | ||||
| Female, 58 | (4 weeks) | ||||
| Case 4 | No | AZD1222/ChAdOx1 | Asthenia, general malaise, weight loss. CK 17,000 U/L, CRP normal, myositic pattern on EMG. ANA negative, Myoblot negative | No | Oral steroids and methotrexate |
| Scarborough | dose 1, March 2021 | ||||
| Male, 61 | (2 weeks) | ||||
| Case 5 | No | BNT162b2 | CK 4793 U/L, CRP 55 mg/L. Anti-Jo1 + (>8.0 U/L) Ro52 1.00 (cut-off = <0.99) | Usual interstitial pneumonia (cataract, iatrogenic) | Oral steroids |
| Harrogate | Dose 3, September 2021 | ||||
| Male, 82 | (4 weeks) | ||||
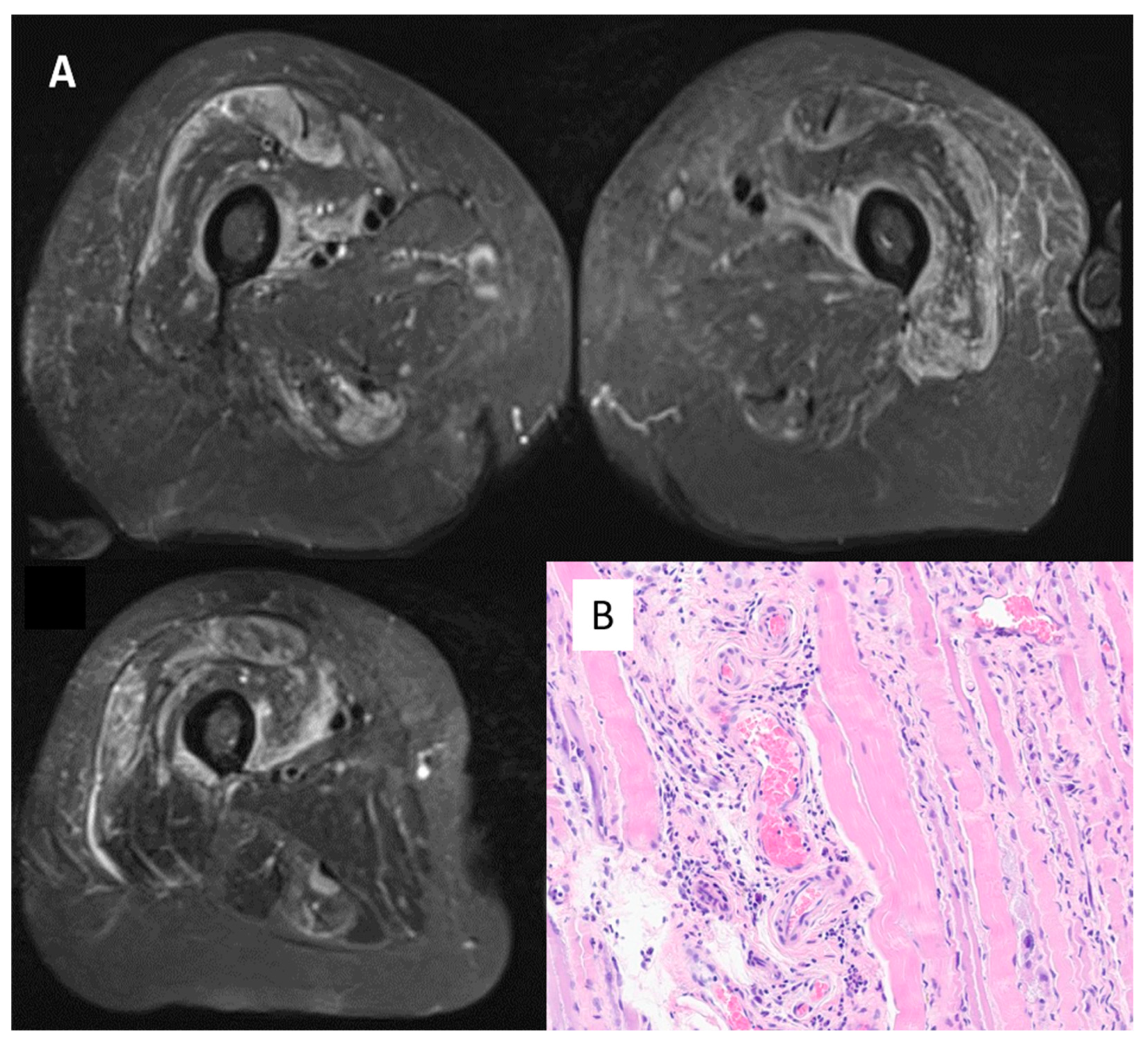
| Case 6 | No | AZD1222/ChAdOx1 | Asthenia, myalgia. CK 7598 U/L, CRP normal, myositic pattern on EMG, muscle oedema on MRI, biopsy positive ANA negative Myoblot + (Pl12 and Scl100) | No | Steroids, then azathioprine and one IV drip of immunoglobulins |
| Bradford | dose 2, February 2021 | ||||
| Female, 76 | (5 weeks) | ||||
| Case 7 | No | BNT162b2 | Asthenia, myalgia. CK 15,212 U/L, CRP 13 mg/L, muscle oedema on MRI, necrosis-related features on biopsy ANA negative, Myoblot negative Anti-HMGCR + | No | Steroids, then two IV drips of immunoglobulins |
| Bradford | dose 3, November 2021 | ||||
| Male, 64 | (5 weeks) | ||||
| Case 8 | No | BNT162b2 | Asthenia, myalgia. CK 8038 U/L, CRP normal, muscle oedema on MRI ANA negative, Myoblot negative | No | Physiotherapy |
| Bradford | dose 2, May 2021 | ||||
| Male, 70 | (24 weeks) | ||||
| Case 9 | Systemic lupus erythematosus (CK normal, no clinical myositis) | AZD1222/ChAdOx1 | Asthenia, myalgia. CK 1299 U/L, CRP normal, myositic pattern on EMG, muscle oedema on MRI, biopsy positive ANA + (Ro/RNP/Sm/ribosomal) | No (Immune thrombocytopenic purpura causing stroke) | Oral steroids and methotrexate |
| Bradford | dose 1, January 2021 | ||||
| Female, 37 | (4 weeks) | ||||
| Case 10 | No | BNT162b2 | Asthenia. CK 3581 U/L, CRP 109 mg/L, myositic pattern on EMG, muscle oedema on MRI, biopsy positive ANA negative, Myoblot negative Anti-HMGCR + | Mild interstitial changes on computed scan, asymptomatic | IV, then oral steroid Methotrexate |
| Mid-Yorkshire | Dose 3, October 2021 | ||||
| Female, 71 | (5 weeks) | ||||
| Case 11 | No | AZD1222/ChAdOx1 | Asthenia, myalgia. CK 2725 U/L, CRP 53 mg/L, muscle oedema on MRI, biopsy negative ANA + (Jo1) | Pulmonary embolism | Oral steroids and azathioprine (not tolerated), then methotrexate |
| Hull | dose 1, January 2021 | ||||
| Female, 78 | (2 weeks) | ||||
| Case 12 | No | AZD1222/ChAdOx1 | Asthenia, dysphagia, respiratory arrest. CK 149,430 U/L, CRP 220 mg/L, Necrosis on biopsy ANA + (Ro/La) Myoblot negative Anti-HMGCR negative | Anuria (renal failure haemodialysis-dependant), respiratory arrest (dependent on intensive care support), suspected myocarditis. Multiple supra-infections. Ultimately death | IV steroids and IV drips of immunoglobulins and rituximab |
| Hull | dose 2, May 2021 | ||||
| Male, 67 | (6 weeks) | ||||
| Case 13 | No | BNT162b2 | Asthenia. CK 3654 U/L, normal CRP, myositic pattern on EMG, muscle oedema on MRI. Biopsy not performed (declined by patient. ANA negative, Myoblot negative Anti-HMGCR + | No | Physiotherapy |
| Mid-Yorkshire | dose 1, May 2021 | ||||
| Female, 72 | (<1 week) | ||||
| Case 14 | No | BNT162b2 | Asthenia. CK 5602 U/L, normal CRP, myositic pattern on EMG, muscle oedema on MRI. Biopsy slighty suggestive of myositis (drying artifacts). ANA + (Sm/RNP/anti-chromatin+) | Raynaud’s phenomenon | Oral steroids and methotrexate |
| Leeds | dose 2, August 2021 | ||||
| Female, 37 | (12 weeks) | ||||
| Case 15 | Giant Cell Arteritis | AZD1222/ChAdOx1 | Asthenia, general malaise, weight loss. CK 3070 U/L, CRP 19.5 mg/L, myositic pattern on EMG, muscle oedema on MRI, Necrosis on biopsy. ANA negative, Myoblot + (anti-SRP) | No | Oral steroids and methotrexate |
| Leeds | dose 2, March 2021 | ||||
| Female, 83 | (6 weeks) |
| KERRYPNX | Relevant Medications before Myositis Onset | Duration of Symptoms Severity | Amounts of Medications Administered to Treat Myositis | Duration of Myositis treatment | Interval to Recovery (If Applicable) |
|---|---|---|---|---|---|
| Case 1 | No other vaccinations preceding exposure to AZD1222/ChAdOx1 | 8 weeks | 1 IV pulse of MP (1.5 g) followed by oral prednisolone 35 mg/day; both associated with IVIG (150 g), MTX 25 mg/week and HCQ 400 mg/day | 7 months | 3 months (muscular strength recovery) Swallow unrecovered |
| Not on relevant medications (including statins) | |||||
| Case 2 | No other vaccinations preceding exposure to AZD1222/ChAdOx1 | 10 days | 1 IV pulse of MP (1.5 g) followed by oral prednisolone 40 mg/day (tapered); both associated with IVIG (90 g), MTX 20 mg/week and HCQ 200 mg/day | 4 months | 4 months |
| Not on relevant medications (including statins) | |||||
| Case 3 | No other vaccinations preceding exposure to AZD1222/ChAdOx1 | 7 days | Oral prednisolone 40 mg/day (tapered), associated with CYCLO 6 IV pulses (15 mg/kg) and MMP 2 g/day | 3 months | 3 months (partial muscular strength recovery, residual fatigue) |
| On levothyroxine 100 mcg/day | |||||
| Not on statins | |||||
| Case 4 | No other vaccinations preceding exposure to AZD1222/ChAdOx1 | 10 months | Oral prednisolone 30 mg/day (tapered to 0) MTX 20 mg/week | 6 months | 6 months (partial recovery of muscular strength) |
| Not on relevant medications (including statins) | |||||
| Case 5 | Flu vaccine was received at the same time of exposure to BNT162b2 | 2 months | Oral prednisolone 40 mg/day (tapered to 0) MMP 2 g/day | 2 months | 2 months |
| Simvastatin (stopped at the time of myositis onset) | |||||
| Case 6 | No other vaccinations preceding exposure to AZD1222/ChAdOx1 | 21 days | oral prednisolone 60 mg/day (tapered to 0); associated with both IVIG (90 g) and AZA 2.5 mg/kg | 4 months | 4 months |
| Atorvastatin (stopped at admission) | |||||
| Case 7 | No other vaccinations preceding exposure to BNT162b2 | 45 days | oral prednisolone 60 mg/day (tapered to 0); associated with both IVIG (120 g) and MTX 25 mg/week | 6.5 months | 4 months |
| Atorvastatin (stopped at admission) | |||||
| Case 8 | No other vaccinations preceding exposure to BNT162b2 | 10 days | Conservative approach and physiotherapy | 5 months | 3 months |
| Not on relevant medications (including statins) | |||||
| Case 9 | No other vaccinations preceding exposure to AZD1222/ChAdOx1 | 5 weeks | oral prednisolone 60 mg/day (initially tapered to 0); associated with MTX 25 mg/week (stopped due to ITP), then with RTX (two doses of 1 g two weeks apart) | 7 months | 2 months (transient recovery, then relapse of myositis; treatment ongoing) |
| On azathioprine for SLE | |||||
| Case 10 | No other vaccinations preceding exposure to BNT162b2 | 2 weeks | 3 IV pulses of MP (1 g) followed by oral prednisolone 60 mg/day (tapered to 0); both associated with MTX 25 mg/week | 5 months | 1.5 months |
| Atorvastatin (stopped at admission) | |||||
| Case 11 | No other vaccinations preceding exposure to AZD1222/ChAdOx1 | 6 weeks | oral prednisolone 60 mg/day (tapered to 0); associated with MTX 25 mg/week | 5.5 months | 3 months |
| Not on relevant medications (including statins) | |||||
| Case 12 | No other vaccinations preceding exposure to AZD1222/ChAdOx1 | 2 months | 3 IV pulses of MP (1 g) followed by IV hydrocortisone 300 mg/day; both associated with IVIG (165 g) and RTX (two doses of 1 g two weeks apart) | 2 months | Not applicable (death) |
| Atorvastatin (stopped at admission) | |||||
| Case 13 | No other vaccinations preceding exposure to BNT162b2 | 2 months | None | Not applicable | 2 months |
| Atorvastatin (stopped at myositis onset) | |||||
| Case 14 | No other vaccinations preceding exposure to BNT162b2 | 6 months | Oral prednisolone 60 mg/day (tapered to 45); Associated with MTX 20 mg/week | 2 months | 2 months (full recovery not achieved) |
| Not on relevant medications (including statins) | |||||
| Case 15 | No other vaccinations preceding exposure to AZD1222/ChAdOx1 | 12 months | Oral prednisolone 40 mg/day (tapered to 15); Associated with MTX 20 mg/week | 3.5 months | 3.5 months (full recovery not achieved) |
| Not on relevant medications (including statins) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Marco, G.; Giryes, S.; Williams, K.; Alcorn, N.; Slade, M.; Fitton, J.; Nizam, S.; Smithson, G.; Iqbal, K.; Tran, G.; et al. A Large Cluster of New Onset Autoimmune Myositis in the Yorkshire Region Following SARS-CoV-2 Vaccination. Vaccines 2022, 10, 1184. https://doi.org/10.3390/vaccines10081184
De Marco G, Giryes S, Williams K, Alcorn N, Slade M, Fitton J, Nizam S, Smithson G, Iqbal K, Tran G, et al. A Large Cluster of New Onset Autoimmune Myositis in the Yorkshire Region Following SARS-CoV-2 Vaccination. Vaccines. 2022; 10(8):1184. https://doi.org/10.3390/vaccines10081184
Chicago/Turabian StyleDe Marco, Gabriele, Sami Giryes, Katie Williams, Nicola Alcorn, Maria Slade, John Fitton, Sharmin Nizam, Gayle Smithson, Khizer Iqbal, Gui Tran, and et al. 2022. "A Large Cluster of New Onset Autoimmune Myositis in the Yorkshire Region Following SARS-CoV-2 Vaccination" Vaccines 10, no. 8: 1184. https://doi.org/10.3390/vaccines10081184
APA StyleDe Marco, G., Giryes, S., Williams, K., Alcorn, N., Slade, M., Fitton, J., Nizam, S., Smithson, G., Iqbal, K., Tran, G., Pekarska, K., Keen, M. U. H., Solaiman, M., Middleton, E., Wood, S., Buss, R., Devine, K., Marzo-Ortega, H., Green, M., & McGonagle, D. (2022). A Large Cluster of New Onset Autoimmune Myositis in the Yorkshire Region Following SARS-CoV-2 Vaccination. Vaccines, 10(8), 1184. https://doi.org/10.3390/vaccines10081184